118
Cerebral Physiology and the Effects of Anesthetics and Techniques دا ام خ ه ن ب1
| Date post: | 01-Jan-2016 |
| Category: |
Documents |
| Upload: | ashley-daniel |
| View: | 213 times |
| Download: | 0 times |

Cerebral Physiologyand the Effects ofAnesthetics and
Techniques
به نام خدا
1

• At rest, the brain consumes oxygen at an average rate of approximately 3.5 mL of oxygen
per 100 g of brain tissue per minute.
• Whole-brain o2 consumption(13.5 x 3.5 =47 mL/min) represents about 20% of total-body oxygen utilization.
2

• CBF is tightly coupled to Local cerebral metabolism.
• If one increase another will increase too,
• And conversely
• Suppression of cerebral metabolism leads to reduction in blood flow.
3

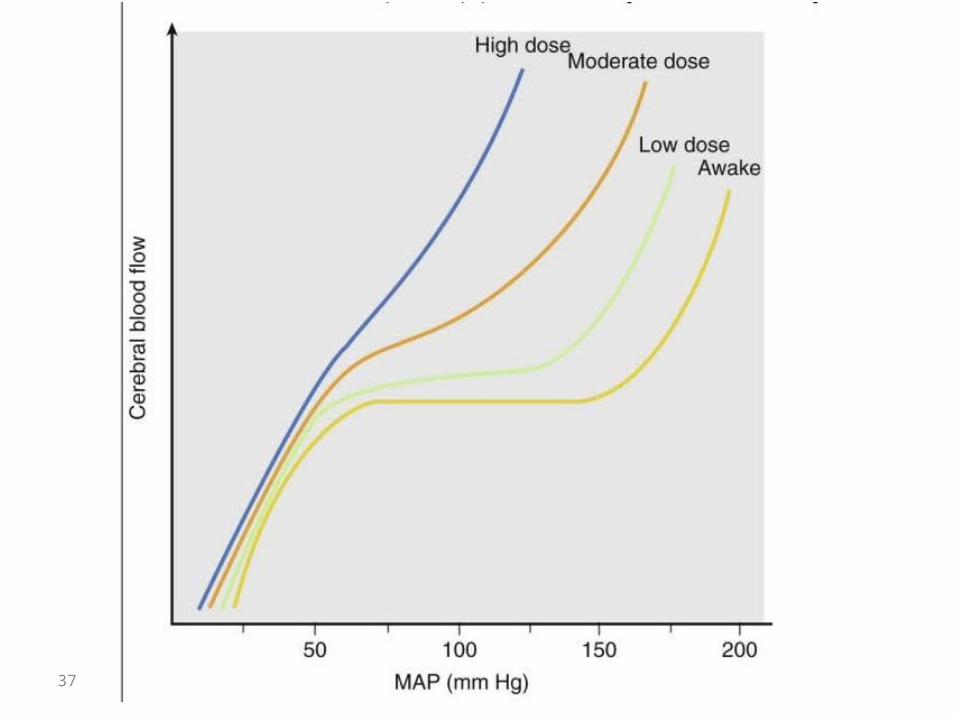
• Brain is autoregulated over a mean arterial pressure rang between 65-150 mm Hg.
• CBF becomes pressure passive when mean arterial pressure is either below the lower limit or above the upper limit of autoregulation.
4

important• The autoregulation mechanism is fragile,
and in many pathologic states CBF is regionally pressure passive.
5
• CBF is also under chemical regulation.• It varies directly with arterial carbon dioxide tension
in the PaCO2 range of 25 to 70 mm Hg.
• With a reduction in PaO2 to below 60 mm Hg, CBF increases dramatically.
• Changes in temperature affect CBF primarily by suppression of cerebral metabolism.
6

• Systemic vasodilators (nitroglycerin, nitroprusside, hydralazine, calcium channel blockers) vasodilate the cerebral circulation and can, depending on mean arterial pressure, increase CBF.
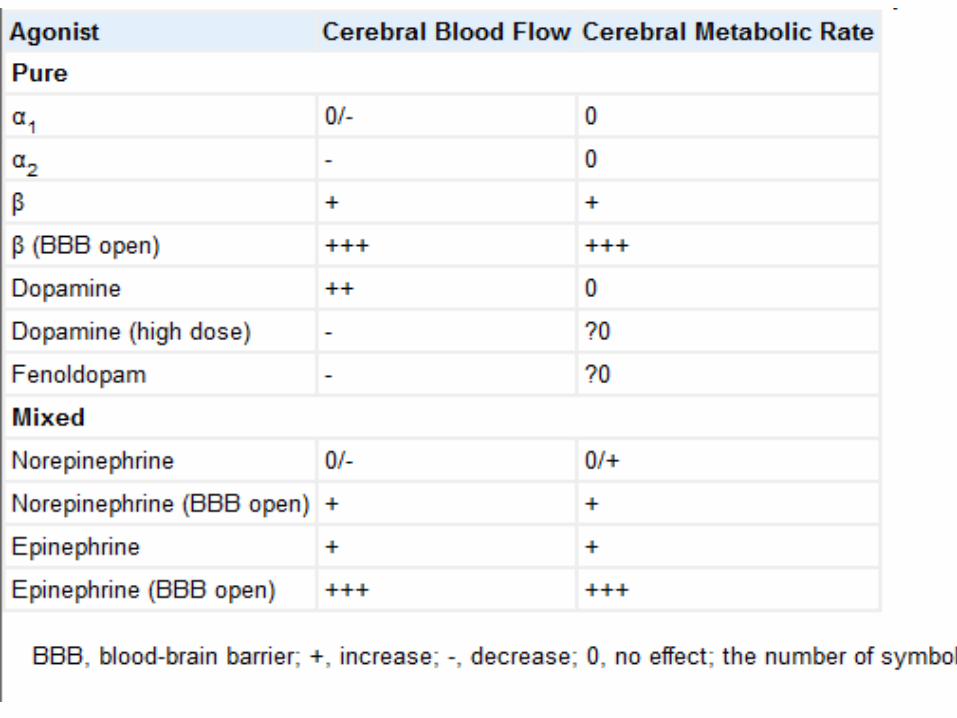
• Vasopressors such as phenylephrine, norepinephrine, ephedrine, and dopamine do not have significant direct effects on the cerebral circulation. Their effect on CBF is dependent on their effect on systemic blood pressure.
7

• All modern volatile anesthetics suppress the cerebral metabolic rate (CMR) and, with the exception of halothane, can produce burst suppression of the electroencephalogram.
• At that level, CMR is reduced by about 60%.• Volatile anesthetics have dose-dependent effects on
CBF.• In doses lower than the minimal alveolar concentration
(MAC), CBF is not significantly altered.• Beyond doses of 1 MAC, direct cerebral vasodilation
results in an increase in CBF and cerebral blood volume.
8

• Barbiturates, etomidate, and propofol decrease CMR and can produce burst suppression of the electroencephalogram.
• Opiates and benzodiazepines effect minor decreases in CBF and CMR.
• whereas ketamine can increase CMR (with a corresponding increase in blood flow) significantly.
9

• Brain stores of oxygen and substrates are limited and the brain is exquisitely sensitive to reductions in CBF.
• Severe reductions in CBF (less than 10 mL/100 g/min) lead to rapid neuronal death. Ischemic injury is characterized by early excitotoxicity and delayed apoptosis.
10

• Barbiturates, propofol, ketamine, volatile anesthetics, and xenon have neuroprotective efficacy and can reduce ischemic cerebral injury.
• Anesthetic neuroprotection is sustained only when the severity of the ischemic insult is mild.
• Administration of etomidate is associated with regional reductions in blood flow, and this can exacerbate ischemic brain injury.
11

• This chapter reviews: the effects of anesthetic drugs and techniques
on cerebral physiology, in particular, their effects on cerebral blood flow (CBF) and metabolism.
12

• Anesthetic drugs cause dose-related and reversible alterations in many aspects of cerebral physiology, including CBF, cerebral metabolic rate (CMR), and electrophysiologic function (EEG, evoked responses)
13

• brain weighs 1350 g (about 2%of total-body weight )
• it receives approximately 12-15% of cardiac output.
• brain's high metabolic rate. • Cerebral blood flow (CBF)= 50 mL/100 g/min– Gray matter receives 80% white matter 20%
• Brain’s energy consumption– 60% support electro physiologic function.– 40% cellular homeostatic activity ,
14

15

• Local CBF and CMR within the brain are very heterogeneous, and both are approximately four times greater in gray matter than in white matter.
16

• The cell population of the brain is also heterogeneous in its oxygen requirements.
• Glial cells make up about half the brain's volume and require less energy than neurons do.
• Besides providing a physically supportive latticework for the brain, glial cells are important in reuptake of neurotransmitters, in delivery and removal of metabolic substrates and wastes, and in blood-brain barrier (BBB) function.
17

• Cerebral metabolic rate:Strict local coupling of CMR and CBF (neurovascular
coupling) the precise mechanisms uncertain
K+,H+, Lactate Adenosine glutamate and NO, Gelia) neurotransmitters such as vasoactive intestinal
peptid (VIP), substance p, calcitonin gene related peptide.
18

In the neurosurgical state CMR affected by:
(1) Functional state:
• Decrease: during sleep , in coma
• Increases: during sensory stimulation, mental tasks, or arousal of any cause , During epileptic activity CMR increases may be extreme,
• whereas regionally after brain injury and globally with coma, CMR may be substantially reduced.
19

• (2)ANESTHETICS : anesthetics suppress CMR (exeptions: ketamine, N2O)
• (1) Electro physiologic Function
(2)The component of CMR required for maintenance of cellular integrity, the "house keeping“ component, is apparently unaltered by intravenous anesthetics.
20

21

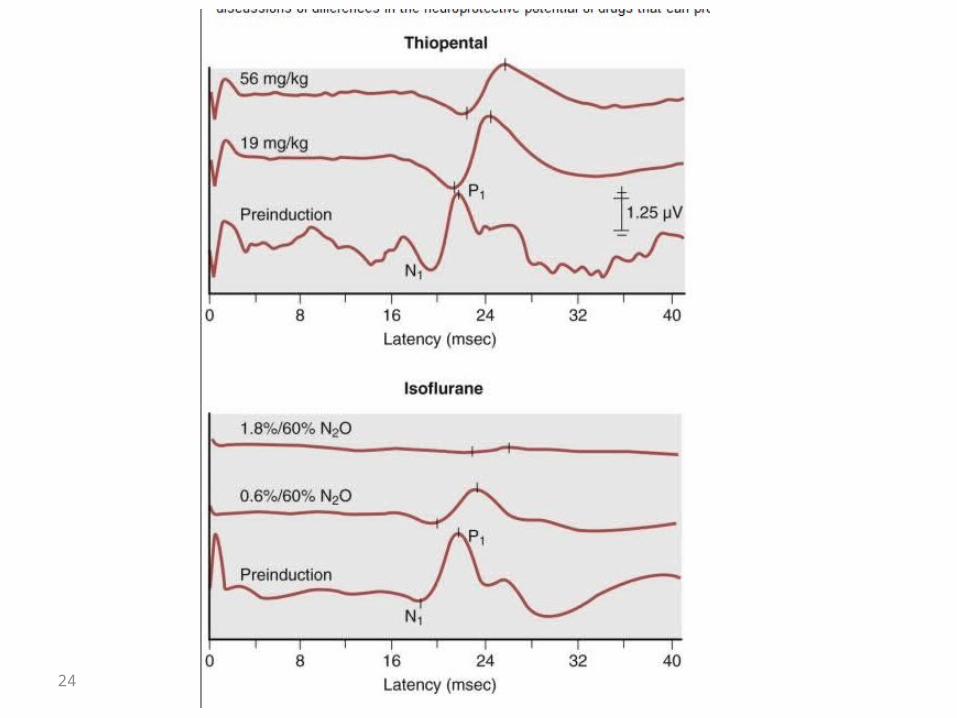
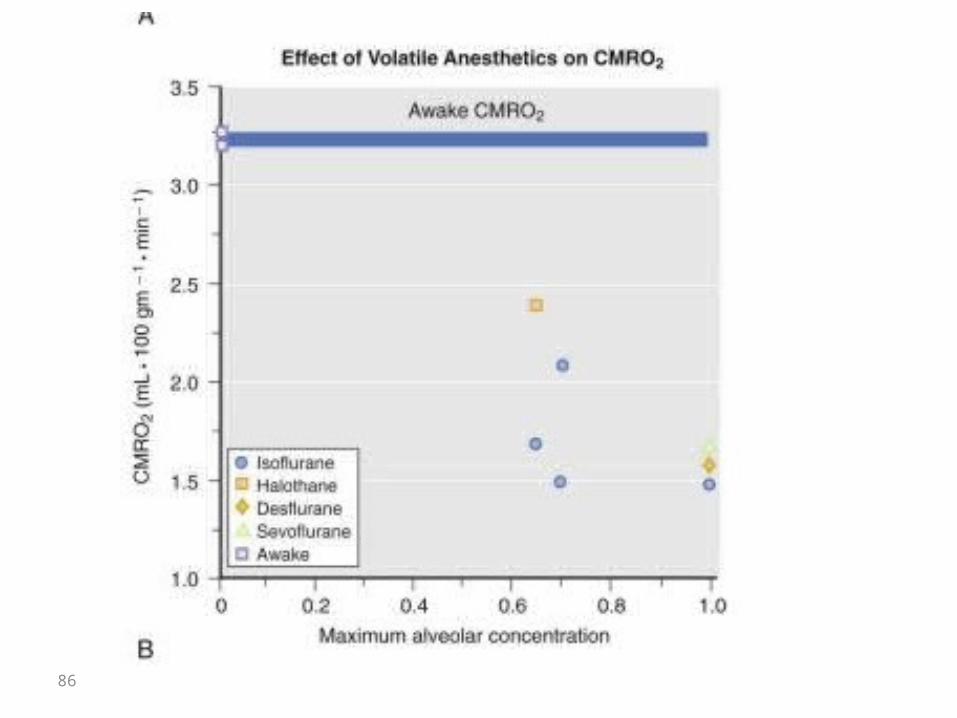
• The cerebral metabolic rate of oxygen (CMRO2) observed when complete suppression of the EEG is achieved with different anesthetic drugs is very similar.
22

• When barbiturates are administered to the point of EEG suppression, a uniform depression in CBF and CMR occurs throughout the brain.
• When suppression occurs during administration of isoflurane, the relative reductions in CMR and CBF are greater in the neocortex than in other portions of the cerebrum
23
24

• (3)Temperature:
• The effects of hypothermia on the brain have been reviewed in detail
• CMR decreases by 6 to7%/1˚c
• hypothermia can also cause complete suppression of the EEG (at about 18°C to 20°C).
• However, in contrast with anesthetic drugs, temperature reduction beyond that at which EEG suppression first occurs does produce a further decrease in CMR ( Fig. 13-3 ).
25

26

• Hyperthermia has an opposite influence on cerebral physiology. Between 37°C and 42°C, CBF and CMR increase.
• However, above 42°C, a dramatic reduction in cerebral oxygen consumption occurs, an indication of a threshold for a toxic effect of hyperthermia that may occur as a result of protein (enzyme) denaturation.
27

PCO2
• CBF varies directly with PCO2• The effect is greatest within the range of physiologic
Paco2 variation• CBF changes 1 to 2 mL/100 g/min for each l mm Hg
change in Paco2.
• Resting cerebral blood flow correlate with ∆CBF/ ∆ Paco2 The magnitude of the reduction in CBF caused by
hypocapnia is greater when resting CBF is high.
Conversely, when resting CBF is low, the magnitude of the hypocapnia-induced reduction in CBF is decreased.
28

PCO2 (continue)
• NO & PGs • The changes in extracellular pH and CBF occur rapidly
after Paco2 adjustments because CO2 diffuses freely across the cerebrovascular endothelium.
• acute systemic metabolic acidosis has little immediate effect on CBF because the BBB excludes hydrogen ion (H+) from the perivascular space
29

PCO2 (continue)• CBF changes is rapid but not sustained.(6-8h)
• Acute normalization of Paco2 will result in significant CSF acidosis (after hypocapnia) or alkalosis (after hypercapnia)
30

31
Pao2
• Below a Pao2 of 60 mm Hg, CBF increases rapidly
• peripheral or neuraxial chemoreceptor, local humoral influences.
• NO of neuronal origin.
• (ATP)-dependent K+ channels
32

• RVM (rostral ventrolateral medulla) serves as an oxygen sensor within the brain.
• Stimulation of the RVM by hypoxia results in an increase in CBF (but not CMR).
• lesions of the RVM suppress the magnitude of the CBF response to hypoxia.
33

Myogenic Regulation (Autoregulation)
• The studies about autoregulation about nomral human is limited
• CPP = MAP- ICP • normal ICP in 10 to 15 mm Hg, an LLA( lower limit of
autoregulation) of 70 expressed as MAP corresponds to an LLA of 55 to 60 mm Hg expressed as CPP
• Above and below the autoregulatory plateau, CBF is pressure dependent (pressure passive).
• a rapid change in arterial pressure will result in a transient (3 to 4 minutes) alteration in CBF.
34
• The cerebral vasculature is extensively innervated• The greatest neurogenic influence appears to be
exerted on larger cerebral arteries.• This innervation include Innervations includes
cholinergic and adrenergic and serotonergic and VlP ergic systems
35

Neurogenic Regulation• Evidence of the functional significance of neurogenic
influences has been derived from studies of CBF autoregulation and ischemic injury.
• Hemorrhagic shock, a state of high sympathetic tone.
• Activation of cerebral sympathetic innervation also shifts the upper limit of autoregulation to the right and offers some protection against hypertensive breakthrough of the BBB.
36
37

Viscosity Effects on Cerebral Blood Flow
• Blood viscosity can influence CBF.
• Hematocrit is the single most important determinant of blood viscosity.
• In healthy subjects, variation of the hematocrit within the normal range (33% to 45%) probably results in only modest alterations in CBF.
• Beyond this range, changes are more substantial.
38
In anemia: cerebral vascular resistance is reduced and CBF increases.
• The effect of a reduction in viscosity on CBF is more obvious in the setting of focal cerebral ischemia, a condition in which vasodilation in response to impaired oxygen delivery is probably already maximal.
39

• The best available information suggests that in the setting of focal cerebral ischemia, a hematocrit of 30% to 34% will result in optimal oxygen delivery.
• viscosity is not a target of manipulation in patients at risk from cerebral ischemia, with the possible exception being those with hematocrit values in excess of 55%
40
Vasoactive Drugs
1:Systemic Vasodilators• drugs used to induce hypotension(including sodium
nitroprusside, nitroglycerin, hydralazine, adenosine, and calcium
channel blockers) cause cerebral vasodilatation.
• CBF either increases or is maintained at prehypotensive levels.
• The ICP effects of these drugs are empirically less dramatic when hypotension is induced slowly.
41

Catecholamine Agonists/ Antagonists
• The effects of these drugs on cerebral physiology are dependent on :
• basal blood pressure
• the magnitude of the systemic blood pressure changes
• the status of the autoregulation mechanism.
• the status of the BBB
42
• When autoregulation is preserved, increases in systemic pressure would be expected to increase CBF if basal blood pressure is either below or above the lower and upper limits of autoregulation.
43
44
Alpha 1 Agonists• α1-agonists (phenylephrine, norepinephrine) have little direct
influence on CBF in humans, with the exception that norepinephrine may cause vasodilatation when the BBB is defective.
• Intracarotid infusion of norepinephrine in doses that significantly increase MAP result in no change in CBF.
• β-mimetic drugs (norepinephrine has β1 activity) cause activation of cerebral metabolism with a coupled increase in CBF, and this effect is likely to be most apparent when these drugs can gain greater access to the brain parenchyma via a defective BBB .
45

• In summary, it seems likely that circulating α1-agonists will have little direct influence on CBF in humans with the exception that norepinephrine may cause vasodilation when the BBB is defective.
46

Β Agonists• in small & large doses• in low doses, have little direct effect on the cerebral
vasculature• In larger doses and in association with physiologic
stress, they can cause an increase in CMR with an accompanying increase in CBF. (CMRO2 can increase by about 20%.)
• BBB defect enhances the effect of β-agonists.• it does not appear that BBB injury is a necessary condition in
humans for the occurrence of β-mediated increases in CBF and CMR, although it will probably exaggerate the phenomenon.

β-Adrenergic Blockers
• β-Blockers reduce or have no effect on CBF and CMR
• β-blockers are unlikely to have adverse effects on patients with intracranial pathology, other than effects secondary to changes in perfusion pressure.
48

Dopamine
• Dopamin is used when an elevation in MAP is desired as an adjunct to the treatment of focal cerebral ischemia, especially in the setting of vasospasm.
• its effects on CBF and CMR have not been defined with certainty.
• in low doses, is probably slight vasodilatation with minimal CMR change.
• Vasoconstriction of the cerebral circulation is not observed even when dopamine is administered in doses up to100 µ/kg/min.
49

α2 agonists
• There is considerable current interest in α2-agonists because of their analgesic and sedative effects.
• dexmedetomidine and clonidine (vasoconstriction)
• dexmedetomidine decreases CBF with no effect on CMRO2(different studies, different results).
• dexmedetomidine reduced MAP modestly.
• caution should be exercised in its use in patients in whom CBF is compromised.
50

Age• Aging, is associated with a progressive reduction in CBF
and CMRO2.
This reduction may reflect the progressive neuronal loss that occurs with age .
51
EFFECTS OF ANESTHETICS ON CBF & CMR
• anesthetic drugs and technique influence CBF
• control and manipulation of CBF are central to the management of ICP
• CBV is very important in amount of ICP approximately 5 mL/100 g
over a Paco2 range of approximately 25 to 70 mm Hg, CBV changes by about 0.049 mL/100 g for each 1–mm Hg change in Paco2.
• Although CBV and CBF usually vary in parallel, exceptions do occur.
when MAP is the manipulated variable. Auto regulation normally serves to prevent MAP-related increases in CBV
52
• When auto regulation is impaired or its upper limit (150mm Hg) is exceeded, CBF and CBV then increase in parallel as arterial pressure rises
• Declining MAP results in a progressive increase in CBV as the cerebral circulation dilates to maintain constant flow, and exaggerated increases in CBV occur as MAP falls below the LLA.
53

54

• In normal subjects, the initial increases in CBV do not result in significant elevation of ICP (compensatory adjustments by other intracranial compartments)
• When intracranial compliance is reduced, an increase in CBV can cause herniation or reduce CPP sufficiently to cause ischemia
55

• with anestheitics: parallel relationship between CBF and CBV.
• CBF-independent influences on CBV may occur.
• It is also an unexplored possibility that anesthetics may influence
the venous side of the cerebral circulation.
• Although the intracranial veins are a largely passive compartment, some evidence indicates that in certain species, there is some active control of venous caliber by either neurogenic or humoral mechanisms.
56

• the importance of blood volume on the venous side of the cerebral circulation should not be overlooked.
• Passive engorgement of these vessels as a result of
the head-down posture, compression of the jugular venous system, or high intrathoracic pressure can have dramatic effects on ICP.
57

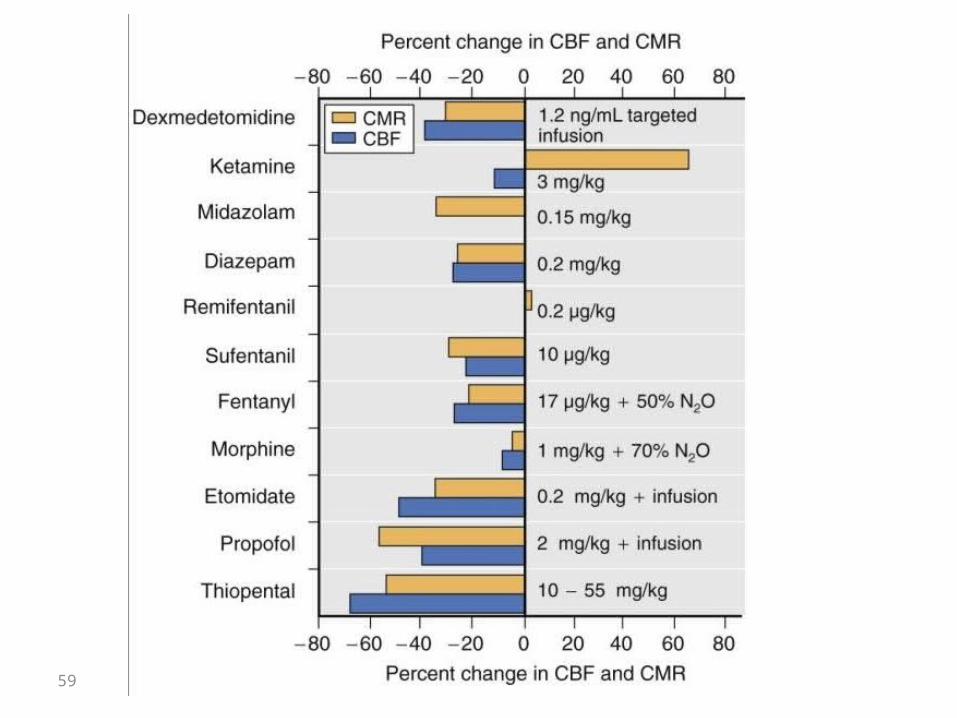
Intravenous Anesthetics• The general pattern of the effect of intravenous
anesthetics is one of parallel alterations in CMR and CBF.• The vast majority of intravenous anesthetics cause a
reduction in both. • Ketamine, which causes an increase in CMR and CBF, is
the exception. • in general, autoregulation and CO2 responsiveness are
preserved during administration of intravenous anesthetic drugs.
58
59

Barbiturates• A dose-dependent reduction in CBF and CMR. • onset of anesthesia, CBF and CMRO2 are reduced by about 30% • complete EEG suppression, CBF and CMR are reduced by about
50%. • Further increases in the dose of barbiturate have no additional
effect on CMR
electrical brain function (neurophysiologic activity), with only minimal effects on the second component, cellular homeostasis
60

Tolerance to the CBF/CMR effects of barbiturates may develop quickly(24h)
autoregulation is maintained to arterial pressures as low as 60 mm Hg.
CO2 responsiveness also persists.
61

propofol• similar to barbiturates.
• reductions in both CBF , CMR,CBV, ICP.• In one study Tolerance to the CBF/CMR effects
of barbiturates may develop quickly.• The whole-brain metabolic rate decreased by
48% to 58%.• decreased the arteriovenous oxygen saturation
difference (AVDO2).
62

Propofol• Both CO2 responsiveness and autoregulation (even
when administered in doses that produce burst suppression of the EEG).
• Seizures and opisthotonos have been reported.
• dystonic and choreiform movements,
63

Etomidate Similar to barbiturates. Induction of anesthesia with either thiopental or etomidate
resulted in a similar reduction in MCA flow velocity of about 27%.
Administration of 0.2 mg/kg of etomidate to adults and observed mean reductions in CBF and CMR of 34% and 45%, respectively.
Like barbiturates no more reduction, when we have burst suppression.
64

the CMR suppression caused by etomidate is regionally variable and occurs predominantly in forebrain structures.
However, etomidate result in an exacerbation of brain tissue hypoxia and acidosis in patients in whom the MCA was temporarily occluded during surgery.
Additional concerns regarding the occurrence of adrenocortical suppression and renal injury caused by the propylene glycol vehicle will probably preclude more than episodic use.
65

re Opioids
Narcotics have relatively little effect on CBF and CMR in the normal, unstimulated nervous system.
• they should be viewed as nonspecific effects of sedation or pain control, or both, rather than specific properties of narcotics.
66
MORPHINE• When morphine (1 mg/kg) was administered as the sole agent in
humans, no effect on global CBF and a 41% decrease in CMRO2.
• Jobes and coworkers gave morphine (1 and 3 mg/kg) with 70%N2O to patients and observed no significant change in CBF or CMR
• substantial histamine release.
• Autoregulation was observed to be intact between MAP values of 60 and 120 mm Hg in human volunteers anesthetized with morphine, 2 mg/kg, and 70% N2O.
67

FENTANYL• Limited human data are available.• fentanyl will cause a moderate global reduction in CBF and CMR
in the normal quiescent brain and will, like morphine cause larger reductions when administered during arousal.
• CO2 responsiveness an auto regulation were unaffected, and the hyperemic CBF response to hypoxia also remained intact.
68

ALFENTANIL-CBF EFFECT
• No studies of the CMR effects of alfentanil in humans have been performed.
69

SUFENTANIL• most investigations in both animals and humans indicate that
sufentanil causes, depending on the dose, either no change or reductions in CBF and CMR and ICP.
in some investigations in humans, sufentanil was associated with modest increases in neuraxis pressure.
• four investigations, that compared conditions in the surgical field, including pressure under brain retractors, identified no adverse influences attributable to sufentanil.
70

Remifentanil• In aggregate, the available human data indicate that in low
sedative doses, administration of remifentanil alone can effect minor increases in CBF. With higher doses or with the concomitant administration of anesthetic adjuvants, CBF is either unaltered or modestly reduced.
• The underlying mechanisms for the increases in CBF are not clear.
71

Benzodiazepines• parallel reductions in CBF and CMR in human.
• CBF and CMR02 decreased by 25% (15 mg diazepam)
• The effects of midazolam on CBF (30-34% reduction)
especially in brain regions contribute with Memory-attention-arousal.
• CO2 responsiveness is preserved.• The extent of the maximal CBF/CMR reduction probably
intermediate between the narcotics (modest) and barbiturates (substantial).
72

Flumazenil• Flumazenil is a highly specific, competitive benzodiazepine
receptor antagonist.• no effect on CBF in unanesthetized human volunteers.
• flumazenil not only reversed the CBF and CMR effects of midazolam but also caused a substantial, though short-lived, overshoot above premidazolam levels in both CBF (by 44% to 56%)and ICP (by 180% to217%).
• Flumazenil should probably be avoided or used very cautiously to reverse benzodiazepine sedation in patients with impaired intracranial compliance.
73

Droperidol
• No human investigation.• droperidol is not a cerebral vasodilator and probably has little
effect on CBF and CMR in humans.
The occasional increases in ICP that have been observed probably reflect normal autoregulation-mediated vasodilation in response to an abrupt fall in MAP.
74
Ketamine• Among intravenous anesthetics unique in increasing CBF and
CMR.( even with sub anesthetic doses )• More increase is in limbic system and less in cortical structures.
• sub anesthetic doses of ketamine increase global CMR by about 25%
• changes in CMR are regionally variable
• Auto regulation and CO2 responsiveness are preserved.
75

Ketamine ( continue)
• Increase ICP
• diazepam, midazolam, isoflurane/N20,propofol blunt or eliminate the ICP or CBF increases
• probably best avoided as the sole anesthetic in patients with impaired intracranial compliance.
76
Lidocaine• a dose-related reduction in CMR02 in experimental animals.
• the membrane-stabilizing effect( reduces the energy for membrane integrity).
• compared the effectiveness of bolus doses of thiopental (Pentothal), 3 mg/kg, and lidocaine, 1.5 mg/kg was equally effective in causing a reduction ICP. (after pin holder or incision for craniotomy). Decrease in MAP was more in thiopental.
77

• Lidocaine-induced seizures have not been reported in anesthetized humans.
• has been recommended for preventing increases in ICP associated with endotracheal suctioning.
• Bolus doses of 1.5 to 2.0 mg/kg therefore seem appropriate.
78

Inhaled Anesthetics• cause parallel reductions in CMR and CBF.• suppress cerebral metabolism in a dose-related manner.
• The net effect of volatile anesthetics on CBF is therefore a balance between a reduction in CBF caused by CMR suppression and augmentation of CBF caused by the direct cerebral vasodilation.
• 0.5 MAC, CMR suppression–induced reduction in CBF predominates.
• At 1.0 MAC, CBF remains unchanged
• Beyond 1.0 MAC, CBF increases significantly (no coupling)
79

• there is a positive correlation between MAC multiples and the CBF/CMR02 ratio; that is, higher MAC levels cause greater "luxury" perfusion.
• increases in CBF and CBV and, consequently, ICP.
• the order of vasodilating potency halothane» enflurane >desflurane =isoflurane >
sevoflurane
80

• Vasodilatory effect of VA :• modified cerebral auto regulation
• administration of 1 MAC halothane significantly increased CBF in comparison when systemic blood pressure was substantially reduced.
• 1.1 MAC levels of halothane increased CBF by as much as 191% and decreased CMR by about 1O%.
• The dramatic increases in CBF( halothane and enflurane).
• Isoflurane, by contrast, does not increase CBF as much as halothane or enflurane does.
81

• 1.1 MAC isoflurane increase CBF by about 19% & CMR is reduced by about 45%
• 1.0 MAC concentrations sevoflurane and desflurane decreased CBF by 38%and 22% and CMR by 39% and 35%, respectively.
82

83

• More recent investigations have shown that both sevoflurane and desflurane can significantly reduce CBF in humans when compared with CBF in awake.
• At 1.0 MAC concentrations, sevoflurane and desflurane decreased CBF by 38% and 22% and CMR by 39% and 35%, respectively.
84

85
86

CMR EFFECTS• All volatiles, DOSE dependent reductions in CMR.
(halothane is less). (sevoflurane= isoflurane).
• from a number of investigations has shown that at doses of 1.0 MAC, isoflurane, sevoflurane, and desflurane reduce CMRO2 (AVDO2 in arterial and jugular bulb blood samples) by 25%.
87

• With isoflurane desflurane and sevoflurane maximal reduction is attained simultaneously with the occurrence of EEG suppression. (1.5 to 2.0 MAC)
• Halothane concentrations in excess of 4.0 MAC are required to achieve EEG isoelectricity.
88
• volatile anesthetics will have minimal effects on cerebral homodynamic in patients with normal intracranial compliance.
• in patients with abnormal intracranial compliance, the potential for volatile anesthetic-induced increases in CBV and ICP exists
89

• Although there is a direct correlation between CBF and CBV.
• as noted earlier, the relationship is not strictly 1 : 1.
• The magnitude of the changes in CBV is significantly less than the magnitude of the changes in CBF.
• modest reduction in CBF may not necessarily be accompanied by reductions in CBV.
90

• large mass lesions, unstable ICP, or sufficient derangement of cerebral physiology that CO2 responsiveness and flow-metabolism coupling may be impaired in some or all of the brain.
• (somnolent, vomiting patient with papilledema, a large mass, and compressed basal cisterns), the clinician may be well advised to use a predominantly intravenous technique until such time as the cranium and dura are open and the effect of the anesthetic technique can be directly assessed.
91

isoflurane is a significant cerebral vasodilator:
near-maximal CMR suppression 0r EEG isoelectric
• The net vasodilating effect of equi -MAC concentrations of isoflurane, desflurane, and sevoflurane is less in humans than that of halothane
92

TIME DEPENDENCEOF CBF EFFECTS.
• After an initial increase, CBF falls substantially, with a steady state near pre-volatile anesthetic levels reached between 2.5 and 5 hours after exposure in animal study but no in human. (the mechanism not understood)
93

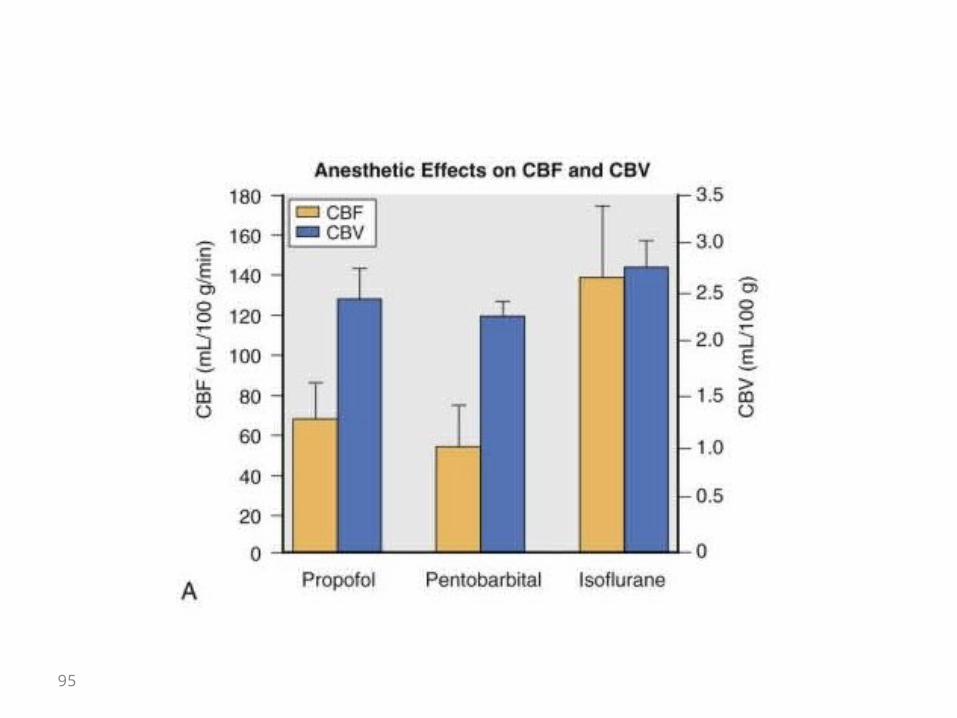
CEREBRAL BLOOD VOLUME.• CBV and not CBF per se that influences ICP• vast majority of intracranial blood is within the cerebral
venous circulation.• the magnitude of changes in CBF is considerably greater than
that in CBV• changes in CBF do not reliably predict changes in CBV and, by
extension, in ICP.• CBV is considerably greater during isoflurane anesthesia than
during propofol or pentobarbital anesthesia.• CBV responds to changes in Paco2 by a reduction in CBV with
hypocapnia and an increase in CBV with hypercapnia.
94
95

96

CO2 RESPONSIVENESS AND AUTOREGULATION. (in VA)• CO2 responsiveness is well maintained during
anesthesia with all of the volatile anesthetics.• by contrast, auto regulation of CBF in response to rising
arterial pressure is impaired.
• this impairment is dose related and greatest with potent vasodilator
• Sevofluran may cause less impairment in auto regulation than other volatile anesthetics
97

• The auto regulatory response to rising pressure is, however, rarely of significance in clinical neuroanesthesia.
• it is the CBF response to falling pressure that is important, and as with all vasodilators, CBF is preserved to lower MAP during administration of volatile anesthetics with no evidence of differences among the various agents.
98

Nitrous Oxide• The available data indicate that N2O can cause increases in CBF, CMR , and
ICP.
• At least a portion of the increases in CBF and CMR may be the result of a sympathoadrenal-stimulating effect of N2O.
• N2O alone, very substantial increases in CBF and lCP can occur.• N2O is administered in combination with IV drugs its cerebral
vasodilating effect is attenuated or even completely inhibited.• The addition of N2O to anesthesia induced with a volatile anesthetic will result in moderate CBF increases.
99

N2O ADMINISTERED ALONE.
• The most dramatic reported increases in ICP or CBF in humans and experimental animals.
• Mean ICP rose from 13 to 40 mm Hg.
100

N2O ADMINISTERED WITH INTRAVENOUS ANESTHETICS.
• N2O + intravenous anesthetics, its CBF effect may be considerably reduced.
• previous use of pentothal and diazepam
• 1 mg/kg of morphine plus 70% N2O resulted in no change in CBF from awake control values.
101

102

N2O ADMINISTEREDWITH VOLATILE ANESTHET
In the majority of investigations, including several in humans, in which N2O has been added to an anesthetic of 1.0 MAC or greater, substantial increases in CBF have been recorded
• vasodilating effect of N2O maybe positively correlated with the concentration of inhaled anesthetic
103

N2O EFFECTS ON CMR• No uniform agreement regarding the effect of
N2O on CMR has not reached. • Some studies: Parallel changes in CBF and
CMR,• Another studies: CBF increases without an
alteration in CMR • Another: CMR alteration occurring without
changes in CBF
104

CLINICAL IMPLICATION• vasodilator action of N2O (clinical significant) in patient with
reduced intracranial compliance.
• N2o + IV anesthesia = can be considerably blunted
• in circumstances where in ICP is persistently elevated or the surgical field is persistently tight, N2O should be viewed as a potential contributing factor.
• the ability of N20 to rapidly enter a closed gas space should be recalled, and it should be avoided or omitted when a closed intracranial gas space may exist.
105

Muscle Relaxants• The only recognized effect of nondepolarizing relaxants on
the cerebral vasculature occurs via the release of histamine
• Histamine can result in a reduction in CPP because of the simultaneous increase in lCP (caused by cerebral vasodilation) and decrease in MAP.
• d- Tubocurarine > Metocurine, atracurium, and mivacurium
• cisatracurium has the least histamine-releasing effect.• No evidence of histamine release was seen after the administration
of 0.15 mg/kg (three times the ED95 for twitch depression) of cisatracurium to neurosurgical ICU patients.
• Vecuronium, Pipecuronium and rocuronium 106
• Pancuronium given as a large bolus dose can cause an abrupt increase in arterial pressure.
• This increased arterial pressure might elevate ICP in the setting of impaired intracranial compliance and defective auto regulation
• Vecuronium, in relatively large doses of 0.1 to 0.14 mg/kg, had no significant effect on cerebral physiology in patients with brain tumors
• Muscle relaxation may reduce ICP, because coughing and straining are prevented, and this results in lowering of central venous pressure with a concomitant reduction in cerebral venous outflow impedance.
• laudanosine, metabolite of Atracurium may be epileptogenic.107

all MR are all reasonable drugs for use patients with or at risk for intracranial hypertension if: sudden change in BP is prevented
108

Succinylcholine Increase in ICP (light anesthesia)(5 mm Hg)
Correlation between the occurrence of visible muscle fasciculation and an increase in lCP is poor.
deep anesthesia has been observed to prevent succinylcholine-induced increases in ICP in the dog.
ICP is Blocked by paralysis with vecuronium and by "defasciculation" with metourin, 0.03 mg/kg.
However, defascicuIation with pancuronium did not prevent
increases in ICP in the dog.
Although succinylcholine increases in ICP, it is no contraindicated in ……….. rapid attainment of paralysis
.
109

Cerebrospinal Fluid Dynamics
• 150 mL of CSF in adult human. Half in cranium half in spinal space.
• CSF, as a cushion for the CNS and as an excretory pathway is
• Is replaced about three or four times per day.
• Anesthetics have been shown to influence both the rate of formation and the rate of reabsorption of CSF.
• halothane decreases secretion of CSF, isoflurane has no effect, and enflurane and desflurane increase secretion.
• Absorption of CSF is reduced by halothane and enflurane, unchanged by desflurane, and increased by isoflurane.
110
• They may be of relevance when a prolonged closed-cranium procedure is to be performed in a patient with poor intracranial compliance.
• Increased CSF production and decreased reabsorption. (enflurane,)
111
112
Blood-Brain Barrier• In most of the body's capillary beds, fenestrations 65 A between endothelial
cells.• In the brain, 8 A.
• There is little evidence that anesthetics alter the function of this "blood-brain
barrier" in most circumstances.
• acute hypertension can breach the barrier and that certain anesthetics facilitate this phenomenon.
• anesthetics may influence the leakiness of an abnormal BBB at normotension.
113

EPILEPTOGENESIS
• seizure activity may go unrecognized in an anesthetized and paralyzed patient and result in neuronal injury if substrate demand (CMR) exceeds supply for a prolonged period.
• A second concern is that the epileptogenic effect will persist in the postanesthesia period when seizures may occur in less well controlled circumstances than exist in the operating room.
• spontaneous seizures during or after anesthesia have been extremely rare events
114

Seizure and volatiles
• Enflurane is potentially epileptogenic• hypocapnia potentate it
• should probably be avoided in patients who are predisposed to seizures or have occlusive cerebrovascular disease.
• EEG-activating property of enflurane for intraoperatively to activate and identify seizure foci
115

ketamine e can elicit seizures in patients with an epileptic diathesis.
Depth electrode recordings (in epileptic patients)sub cortical seizure activity originating in the limbic and thalamic
areas.
The occurrence of seizures after ketamine anesthesia in neurologically normal subjects has also been reported (2 occasions).
in one of these instances seizure thresholds may have been lowered by aminophylline.
116

CEREBRAL PHYSIOLOGY INPATHOLOGIC STATES
• Cerebral Ischemia- Pathophysiology :• The brain has a high rate of energy utilization and very limited energy storage
capacity.
• vulnerable in the event of interruption of substrate (oxygen, glucose) supply.• global CBF at 50 mL/lOO g/min • it is not until CBF has fallen to approximately 20 mL/100 g/min that EEG
evidence of ischemia begins to appear• 15 mL/100 g/min EEG isoelectric
• 6 mL/1 00 g/ min membrane failure
• 10 and 15 mL/100 g/ min (time course that may last hours rather than minutes), to membrane failure and neuronal death .

118

















