53
CERVICAL CANCER FAHAD ZAKWAN
| Date post: | 22-Jul-2015 |
| Category: |
Documents |
| Upload: | fahad-zakwan |
| View: | 39 times |
| Download: | 0 times |

CERVICAL CANCER
FAHAD ZAKWAN

Review of anatomy

Epidemiology• Cancer of the cervix uteri is the second most
common cancer among women worldwide
BUT
• for Tanzania is the leading type of cancer in women and the commonest cause of cancer related deaths in this country.

Burden in Tanzania• Tanzania has a population of 10.97 millions women ages 15
years and older who are at risk of developing cervical cancer.
• Current estimates indicate that every year 6241 women are diagnosed with cervical cancer and 4355 die from the disease.
• Cervical cancer ranks as the 1st most frequent cancer among women in Tanzania, and the 1st most frequent cancer among women between 15 and 44 years of age

Projections• Projected number of new cervical cancer cases in
2025* is estimated to increases to 10257
• Projected number of cervical cancer deaths in 2025* is estimated to increase to 7173
Cervical cancer is on the increase

PathogenesisCancer of the cervix has been regarded as a preventable
cancer because;
1. Known etiology. (HPV)
2. It has a long pre-invasive state.
3. Cervical cytological screening programs are available
4. Treatment of pre-invasive lesions is effective.
• Invasive cervical cancers are usually preceded by a long phase of preinvasive disease.
• This is characterized microscopically as a spectrum of events progressing from cellular atypia to various grades of dysplasia or cervical intraepithelial neoplasia (CIN) before progression to invasive carcinoma

A good knowledge of the etiology, pathophysiology and natural history of these pre-invasive conditions provides a strong basis both for visual testing and for colposcopic diagnosis and understanding the
principles of treatment of these lesions.
• CIN and cancer of cervix is a single, continuous disease process by which normal epithelium evolves into epithelial precursor lesions and on to invasive cancer.
• Precancerous lesions are usually discovered by a screening test, the Papanicolaou or "pap" smear


Grades of CIN (pre-invasive cancer)
CIN1 (Grade I)• The least risky type, represents only mild dysplasia, or
abnormal cell growth and corresponds to a low grade squamous intraepithelial lesion (LGSIL)..
• It is confined to the basal 1/3 of the epithelium. • This corresponds to infection with HPV, and mostly will
be cleared by immune response in a year or so, though can take several years to clear.

• as well as CIN III, correspond to high grade squamous intraepithelial lesions (HGSIL). CIN2 represents moderate dysplasia, and is confined to the basal 2/3 of the epithelium.
CIN2 (Grade II)

CIN3 (Grade III):
In this lesion, severe dysplasia spans greater than 2/3 of the entire epithelium, and may involve the full thickness. This
lesion may sometimes also be referred to as cervical carcinoma in situ.

Disease ProgressionThe course of a specific lesion is influenced by;
1. Inciting HPV type.
2. Patients immune status
3. Smoking habits.
4. Time/duration

Disease ProgressionCIN I CIN II CIN III
Regression to normal 60% 40% 30%
Persistence 30% 35% 48%
Progression to CIN III 10% 20% -
Progression to cancer <1% 5% 22%

Disease Progression• However most CIN spontaneously regress.
• Progression to cancer typically takes 15 (3 to 40) years
• Also, evidence suggests that cancer can occur without first detectably progressing through these stages and that a high grade intraepithelial neoplasia can occur without first existing as a lower grade.

EtiologyEpidemiological studies have identified a number of risk factors
that contribute to the development of cervical cancer precursors and cervical cancer
• infection with certain oncogenic types of human papillomaviruses (HPV),
• sexual intercourse at an early age,
• multiple sexual partners

• long-term oral contraceptive use,
• tobacco smoking
• low socioeconomic status
• multiparity
• micronutrient deficiency
• diet deficient in vegetables and fruits.
• Persistent infection with one or more of the oncogenic types of HPV is considered to be a
necessary cause for cervical neoplasia.
• HPV infection is transmitted through sexual contact and the risk factors therefore are closely related to sexual behaviour (e.g., lifetime number of sexual partners, sexual intercourse at an early age).

• HPV infection is believed to start in the basal cells or parabasal cells of the metaplastic epithelium
• Typically the disease starts at the squamo-columna junction or transformation zone
• If the infection persists, integration of viral genome into the host cellular genome occur.

• The normal differentiation and maturation of the immature squamous metaplastic into the mature squamous metaplastic epithelium may be disrupted as a result of expression of E6/E7 viral oncoproteins and the loss of normal growth control
• E6 and E7 have the ability to complex with the tumor suppressor genes p53 and Rb, respectively
• This may then lead to development of abnormal dysplastic epithelium
• If the neoplastic process continues uninterrupted, the early low-grade lesions may eventually involve the full thickness of the epithelium.
• Subsequently the disease may traverse the basement membrane and become invasive cancer, extending to surrounding tissues and organs

• Despite women’s frequent exposure to HPV, development of cervical neoplasia is uncommon
• Most cervical abnormalities caused by HPV infection are unlikely to progress to high-grade CIN or cervical cancer, as most of them regress by themselves

Cell cycle

EtiologyThe long time frame between initial infection and overt
disease indicates that several cofactors (e.g., genetic differences, hormonal effects, micronutrient deficiencies, smoking, or chronic inflammation) may be necessary for
disease progression.
• Immune system?
There are > 70 HPV subtypes, half of which infect the ano-genital epithelium based on their malignant potential, HPV subtypes are classified as
• high risk,
• intermediate risk and
• low risk subtypes

• Low risk HPV (6,11,42,43,55) are associated with condylomata and low grade pre-malignant lesions of the cervix
• Intermediate risk HPV (33,35,51,520 are associated with high grade lesion of the cervix.
• High risk HPV (16,18,31,39,45,57,58,59,68) are associated with high grade lesions and invasive cancer of the cervix.

• Cigarette smoking and HPV act synergistically on the development of CIN.
• Cigarette smoking is associated with two to four fold increase in relative risk for development of cervical
Cancer.
• Cigarette smoke carcinogens have been found to accumulate locally in the cervical mucus and cumulative exposure as measured by pack-year smoked is related to the risk of developing CIN or carcinoma insitu.
• Incidence of cervical neoplasia is increased in HIV infected women

Treatment of pre-invasive lesions (CIN)
• Cryotherapy
Nitrous oxide or carbon dioxide is used as the refrigerant for a super-cooled probe
The cryoprobe is positioned on the ectocervix where it must cover the entire lesion, which at times is not easily achieved. It is then activated until blanching of the cervix extends at least 7 mm beyond the probe in all directions in order to assure that freezing extends beyond the depth of the crypts of the glands into which the dysplasia might be extending.

Carbon Dioxide Laser
The laser destroys tissue with a very narrow zone of injury around the treated tissue, and is therefore both precise and flexible.
The tissue is vaporized to a depth of at least 7 mm to assure that the bases of the deepest glands are destroyed

• Loop Electrosurgical Excision Procedure (LEEP)
LEEP uses a small, fine, wire loop attached to an electrosurgical generator to excise the tissue of interest. Various sizes of wire loop are available
Following LEEP excision of the transformation zone, frequently an additional narrow endocervical specimen is removed to allow for histologic evaluation while avoiding excessive damage to the cervical stroma

• Cold Knife Conization
Cold knife conization of the cervix refers to the excision of a cone-shaped portion of the cervix using a scalpel. This technique can be individualized to accommodate the cervical anatomy and the size and shape of the lesion
Cervical cone biopsy is generally done in the operating room under local or general anesthesia. Complications include bleeding, infection, cervical stenosis, and cervical incompetence

• Hysterectomy
Removal of the whole uterus with or without pelvic lymph node dissection
CERVICAL CANCER: Invasive cancer
• Age of incidence: Used to be a disease of old women but nowadays the age of onset has decreased significantly.
• The average age at diagnosis of patients with cervical cancer is 51 years. However, the disease can occur in the second decade of life
• 75% decrease in the incidence of cervical cancer in developed countries following the implementation of population-based screening programs and treatment of preinvasive disease
• But the disease is on the increase in developing countries
No active screening programs
Few treatment option
• Most patients In sub-Saharan Countries and Tanzania is number 2 after Zambia

Histological types• 70–75% of cervical carcinomas are squamous
cell (squamous cell carcinoma-SCC)
• adenocarcinomas (20–25%),
• adenosquamous carcinomas (3–5%),

Symptoms and Signs• Abnormal vaginal bleeding is the most common symptom of
invasive cancer and may take the form of a blood-stained leukorrheal discharge, scant spotting, or frank bleeding. Leukorrhea, usually sanguineous or purulent, odorous, and nonpruritic, is frequently present.
• A history of postcoital/contact bleeding may be elicited on specific questioning.

• Pelvic pain, often unilateral and radiating to the hip or thigh, is a manifestation of advanced disease.
• Also, as is the involuntary loss of urine or feces through the vagina, a sign of fistula formation.
• Weakness, weight loss, and anemia are characteristic of the late stages of the disease, although acute blood loss and anemia may occur in an ulcerating stage I lesion.
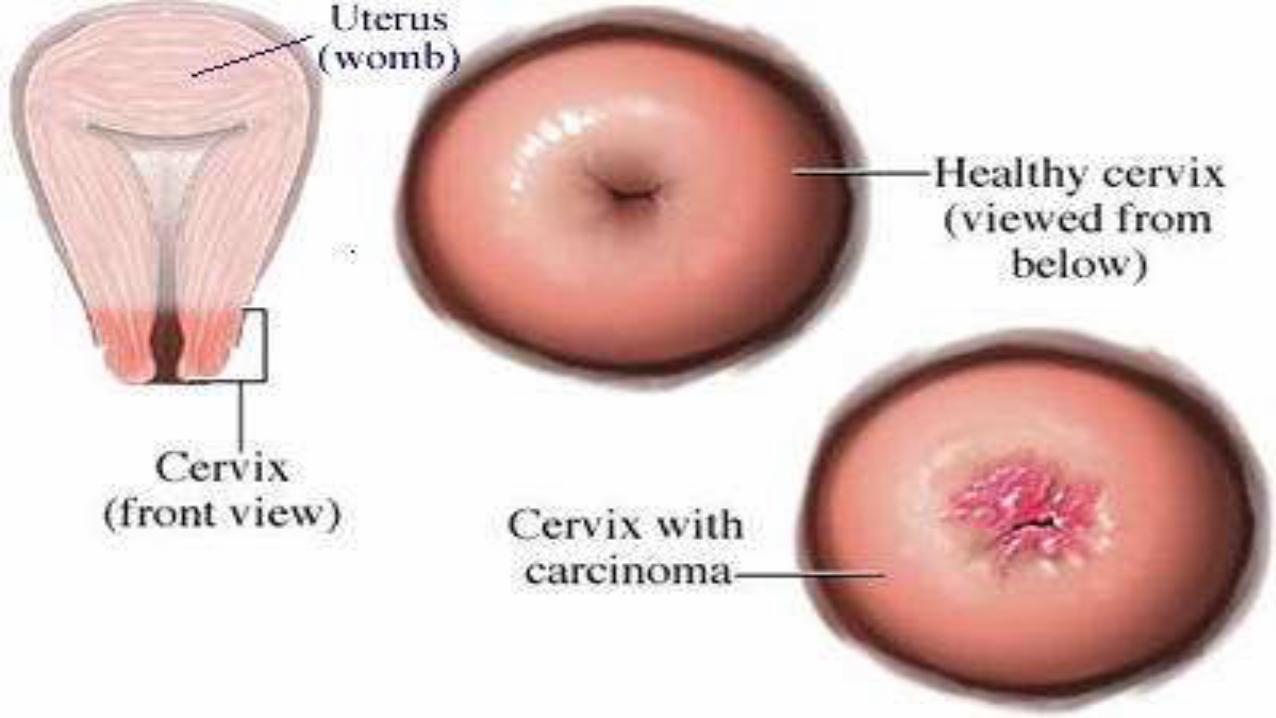
Physical examination
• Speculum examination: Infiltrative cancer produces enlargement, irregularity, and a firm consistency of the cervix and eventually of the adjacent parametria.
• The growth pattern can be endophytic, leading to a barrel-shaped enlargement of the cervix, or exophytic, where the lesion generally appears as a friable, bleeding, cauliflower like lesion of the portio vaginalis.
• Ulceration on the cervix may be the primary manifestation of invasive carcinoma;
• With further progression of the disease, the ulcer becomes deeper and necrotic
• The adjacent vaginal fornices may become involved next. Eventually, extensive parametrial involvement by the infiltrative process may produce a nodular thickening of the uterosacral and cardinal ligaments with resultant loss of mobility and fixation of the cervix.
Definitive diagnosis
Biopsy for histological
examination

Radiological exams
•Ultrasound
•IVU
•CXR

Laboratory tests• Blood test
CBC
RFT
• Urine tests
urinalysis
Cervical cancer staging• Stage 0 (CIN III) = carcinoma in situ
• Stage 1A = Microinvasive carcinoma
• Stage 1B = cancer confined to the cervix
• Stage 2A = cancer extend to the upper third of the vagina
• Stage 2B = cancer extend to the parametrium but not to the pelvic side walls


• Stage 3A = cancer involving the lower third of the vagina
• Stage 3B = cancer extends to the pelvic side walls (often obstructing the ureter)
• Stage 4A = cancer involving the bladder and/or rectum
• Stage 4B = Distant metastasis

Treatment of cervical cancer
• Surgical approach: For very early cervical cancer (1A)
Hysterectomy plus lymph node dissection
• Main stay is Radiotherapy with chemotherapy (Cisplatin IV)
External beam followed by intracavitary

PREVENTION OF CERVICAL CANCER
1. Cervical cancer screening to detect premalignant conditions
Visual inspection of the cervix (Speculum) with acetic acid or Iodine = Acetowhite changes
Pap smears
Colposcopy and Biopsy
2. Vaccine for HPV to all women before they are infected (Before they start sexual activity)
Young girls are the major target but any woman 10-50 can receive the vaccine
3. Sexual behavior
Late onset of sex
Number and behavior of sexual partners
Male circumscion

4. Using barrier methods
Male condoms
Female condom


















