January 1, 2010 ◆ Volume 81, Number 1 www.aap.org/ap American Family Physician 33
Cervical Radiculopathy:
Nonoperative Managemento Neck Pain and Radicular SymptomsJASONDAVIDEUBANKS,MD,Case Western Reserve University School of Medicine, Cleveland, Ohio
Cervical radiculopathy leads toneck and radiating armpain ornumbness in the distribution oaspecicnerveroot.Oten,this
radicularpain isaccompaniedbymotororsensory disturbances. Although the causesoradiculopathyarevaried(e.g.,acutediskherniations,cervicalspondylosis,oraminal
Anepidemiologicsurveyshowedtheannualage-adjustedincidenceoradiculopathytobe83 per 100,000 persons.1 Persons reportingradiculopathywerebetween13and91yearsoage,andmenwereaectedslightlymorethanwomen. In this study, 14.8 percent opersons with radiculopathy reported ante-cedentphysicalexertionortrauma,andonly
A variety o conditions can lead to nerverootcompressioninthecervicalspine.Eachmotion segment in the subaxial spine (C3
through C7) consists o ve articulations,includingtheintervertebraldisk,twoacet joints,andtwoneurocentral(uncovertebral) joints.Boundedbytheseelements,thenerverootsexitlaterally.Unlike the lumbar spine, the cervical
spinehascervicalnerverootsthatexitabovethe level o the corresponding pedicle. Forinstance,theC5nerverootexitsattheC4-C5diskspace,andaC4-C5diskherniationtypicallyleadstoC5radiculopathy.Thereareseven cervical vertebrae and eight cervical
nerveroots. Inthe lumbarspine,thenerve
Cervical radiculopathy is a disease process marked by nerve com-pression rom herniated disk material or arthritic bone spurs. Thisimpingement typically produces neck and radiating arm pain ornumbness, sensory defcits, or motor dysunction in the neck andupper extremities. Magnetic resonance imaging or computed tomo-
graphic myelography can confrm neurologic compression. Theoverall prognosis o persons with cervical radiculopathy is avor-able. Most patients improve over time with a ocused, nonoperativetreatment course. There is little high-quality evidence on the bestnonoperative therapy or cervical radiculopathy. Cervical collarsmay be used or a short period o immobilization, and traction maytemporarily decompress nerve impingement. Medications may helpalleviate pain and neuropathic symptoms. Physical therapy andmanipulation may improve neck discomort, and selective nerve
blocks target nerve root pain. Although the eectiveness o individ-ual treatments is controversial, a multimodal approach may beneftpatients with cervical radiculopathy and associated neck pain. ( Am
34 American Family Physician www.aap.org/ap Volume 81, Number 1 ◆ January 1, 2010
exitsbelowthecorrespondingpedicle.There-ore, an analogous lumbar disk herniation(L4-L5)wouldcompressthetraversingnerveroot(L5),nottheexitingroot(L4).Whetherin the cervical spine or the lumbar spine,the nerve impingement typically occurs inthenervenumericallycorrespondingtothelowerothetwovertebrallevels.Theexitingnerverootcanbecompressed
by herniated disk material (sot disk her-niation) or through encroachment by sur-rounding degenerative or hypertrophicbony elements (hard disk pathology). Ineither case, a combination o actors, suchas infammatorymediators (e.g., substanceP),changesinvascularresponse,andintra-neuraledema,contributetothedevelopmentoradicularpain.2
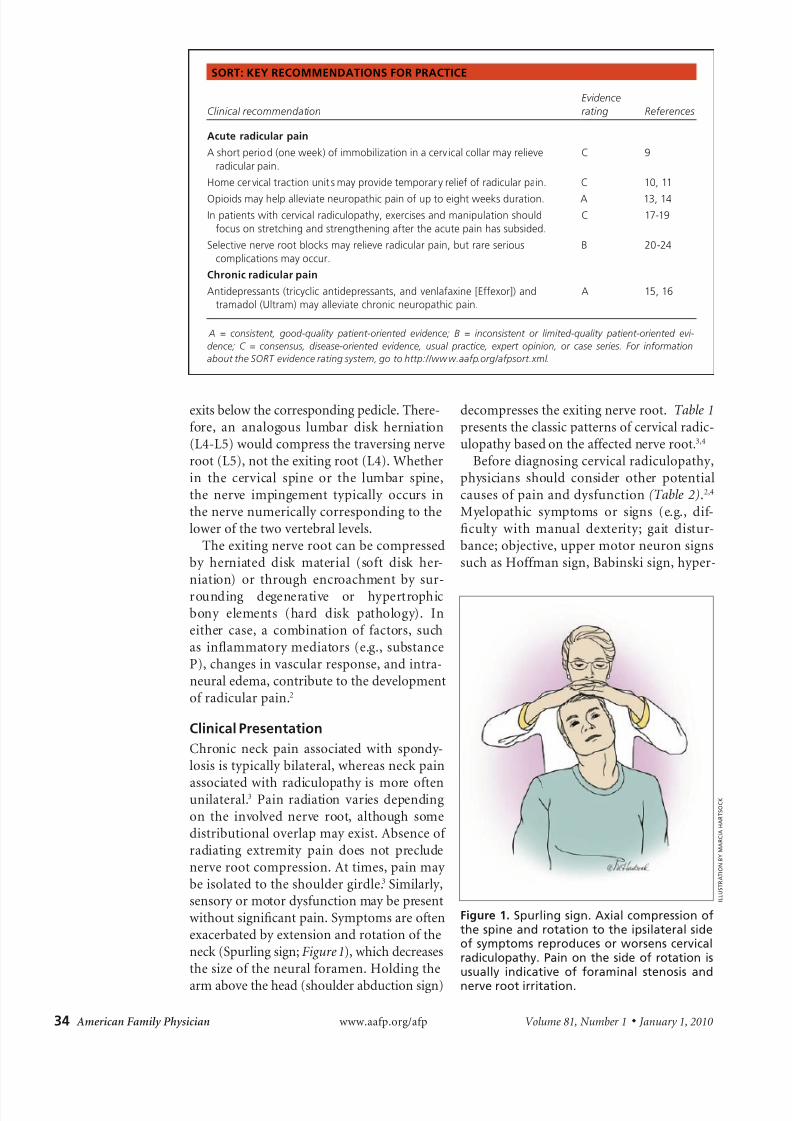
associatedwithradiculopathyismoreotenunilateral.3 Pain radiation variesdependingon the involved nerve root, although somedistributionaloverlapmayexist.Absenceoradiating extremity pain does not precludenerverootcompression.Attimes,painmaybeisolatedtotheshouldergirdle.3Similarly,sensoryormotordysunctionmaybepresentwithoutsignicantpain.Symptomsareotenexacerbatedbyextensionandrotationotheneck(Spurlingsign;Figure 1),whichdecreasesthesizeotheneuraloramen.Holdingthe
Beorediagnosingcervicalradiculopathy,physicians should consider other potentialcausesopainanddysunction(Table 2).2,4Myelopathic symptoms or signs (e.g., di-culty with manual dexterity; gait distur-bance;objective,uppermotorneuronsignssuchasHomansign,Babinskisign,hyper-
SORT: KEY RECOMMENDATIONS FOR PRACTICE
Clinical recommendation
Evidence
rating Reerences
Acute radicular pain
A short period (one week) o immobilization in a cervical collar may relieve
radicular pain.
C 9
Home cervical traction units may provide temporary relie o radicular pain. C 10, 11
Opioids may help alleviate neuropathic pain o up to eight weeks duration. A 13, 14
In patients with cervical radiculopathy, exercises and manipulation should
ocus on stretching and strengthening ater the acute pain has subsided.
C 17-19
Selective nerve root blocks may relieve radicular pain, but rare serious
complications may occur.
B 20-24
Chronic radicular pain
Antidepressants (tricyclic antidepressants, and venlaaxine [Eexor]) and
tramadol (Ultram) may alleviate chronic neuropathic pain.
A 15, 16
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evi-
dence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For inormation
about the SORT evidence rating system, go to http://www.aap.org/apsort.xml.
I L L U S T R A T I O N B Y m A R c I A h A R T S O c k
Figure 1. Surling sign. Axial oression ofthe sine and rotation to the isilateral sideof sytos rerodues or worsens ervialradiuloathy. pain on the side of rotation isusually indiative of forainal stenosis and
nerve root irritation.
8/6/2019 Cervical Radiculopathy Nonoperative Management of Neck Pain and Radicular Symptoms
January 1, 2010 ◆ Volume 81, Number 1 www.aap.org/ap American Family Physician 35
refexia,andclonus)maysuggestcompres-sionothespinalcordratherthannerveroot.Spinal cord compression typically requiressurgical decompression because myelopa-thyisprogressiveanddoesnotimprovewithnonoperativemeasures. The ollowing ac-torsmayalsoindicateanalternatediagno-sis:ageyoungerthan20yearsorolderthan50years, especially i thepatient has signs
orsymptomsosystemicdisease;unrelent-ing pain at rest; constant or progressivesigns or symptoms; neck rigidity withouttrauma;dysphasia;impairedconsciousness;central nervous system signs and symp-toms; increased risk o ligament laxity oratlantoaxial instability, such as in patientswithDown syndromeor heritable connec-tive tissuedisorders; suddenonset oacute
Table 1. Classic Patterns of Cervical Radiculopathy
Nerve
root Interspace Pain distribution
Abnormalities
Motor Sensory Refex
C4 C3-C4 Lower neck, trapezius NA Cape distribution
(i.e., lower
neck and upper
shoulder girdle)
NA
C5 C4-C5 Neck, shoulder, lateral
arm
Deltoid, elbow
exion
Lateral arm Biceps
C6 C5-C6 Neck, dorsal lateral
(radial) arm, thumb
Biceps, wrist
extension
Lateral orearm,
thumb
Brachioradialis
C7 C6-C7 Neck, dorsal lateral
orearm, middle
fnger
Triceps, wrist
exion
Dorsal orearm,
long fnger
Triceps
C8 C7-C8 Neck, medial orearm,
ulnar digits
Finger exors Medial orearm,
ulnar digits
NA
T1 C8-T1 Ulnar orearm Finger intrinsics Ulnar orearm NA
NA = not applicable.
Inormation rom reerences 3 and 4.
Table 2. Differential Diagnosis of Cervical Radiculopathy
Condition Characteristics
Cardiac pain Radiating upper extremity pain, particular ly in the let shoulder and arm, that has possible cardiac origin
Cervical spondylotic
myelopathy
Changes in gait, requent alls, bowel or bladder dysunction, difculty using the hands, stiness o the
extremities, sexual dysunction accompanied by upper motor neuron fndings
Complex regional pain
syndrome (reex
sympathetic dystrophy)
Pain and tenderness o the extremity, oten out o proportion with examination fndings, accompanied by
skin changes, vasomotor uctuations, or dysthermia; symptoms oten occur ater a precipitating event
Entrapment syndromes For example, carpal tunnel syndrome (median nerve) and cubital tunnel syndrome (ulnar nerve)
Herpes zoster (shingles) Acute inammation o dorsal root ganglion creates a painul, dermatomal radiculopathy
Intra- and extraspinal tumors Schwannomas, osteochondromas, Pancoast tumors, thyroid or esophageal tumors, lymphomas,
carcinomatous meningitis
Parsonage-Turner syndrome
(neuralgic amyotrophy)
Acute onset o proximal upper extremity pain, usually ollowed by weakness and sensory disturbances;
typically involves upper brachial plexus
Postmedian sternotomy lesion Occurs ater cardiac surgery; C8 radiculopathy may develop secondary to an occult racture o the frst
thoracic rib
Rotator cu pathology Shoulder and lateral arm pain
Thoracic outlet syndrome Median and ulnar nerve (lower brachial plexus nerve roots, C8 and T1) dysunction rom compression
by vascular or neurogenic causes, oten a tight band o tissue extending rom frst thoracic rib to C7
transverse process
Inormation rom reerences 2 and 4.
8/6/2019 Cervical Radiculopathy Nonoperative Management of Neck Pain and Radicular Symptoms
attack, which may indicate vertebrobasilarinsuciency or carotid artery ischemia orstroke;suspectedneoplasia;suspectedinec-tion,suchasdiskitis,osteomyelitis,ortuber-culosis; ailed surgical usion; progressiveor painul structural deormity; abnormallaboratoryexaminationresults.5
Diagnostic Evaluation
Adults who have persistent neck pain andradicular symptoms should receive antero-posterioropen-mouth,anteroposteriorlower
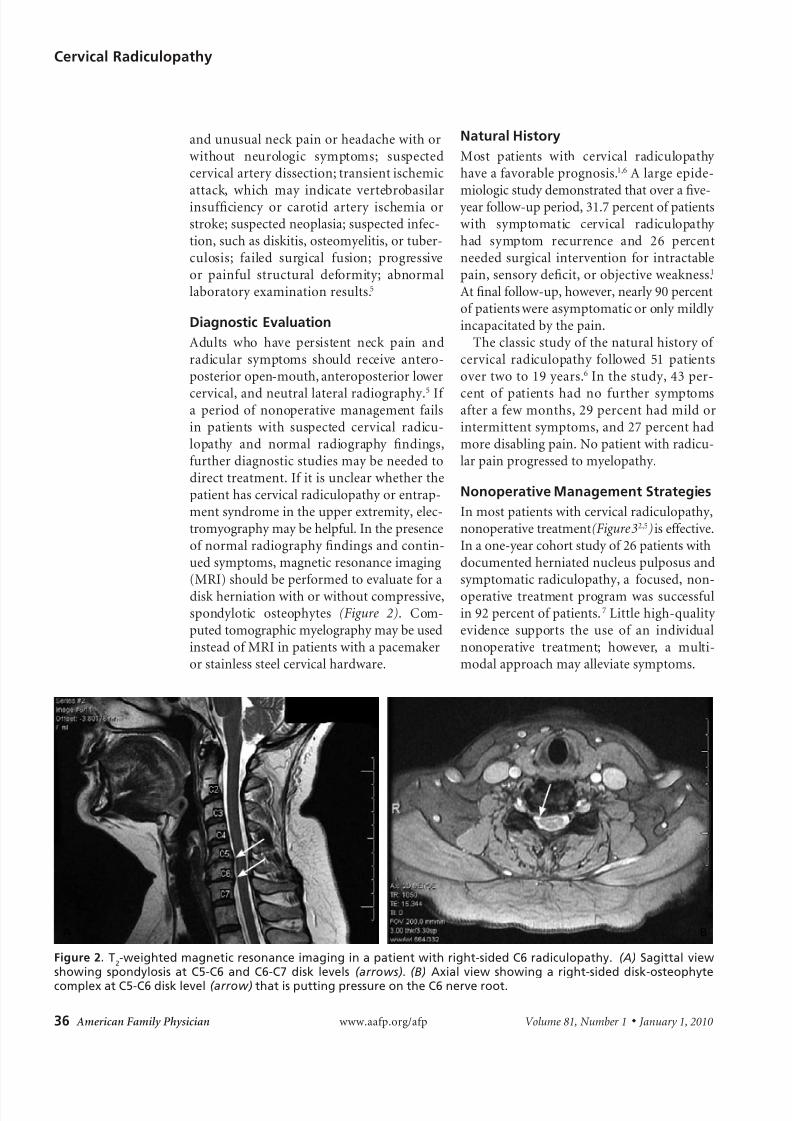
cervical,andneutrallateralradiography.5Ia period ononoperativemanagement ailsin patients with suspected cervical radicu-lopathy and normal radiography ndings,urtherdiagnosticstudiesmaybeneededtodirecttreatment.Iitisunclearwhetherthepatienthascervicalradiculopathyorentrap-mentsyndromeintheupperextremity,elec-tromyographymaybehelpul.Inthepresenceonormalradiographyndingsandcontin-uedsymptoms,magneticresonanceimaging(MRI)shouldbeperormedtoevaluateoradiskherniationwithorwithoutcompressive,spondylotic osteophytes (Figure 2). Com-putedtomographicmyelographymaybeusedinsteadoMRIinpatientswithapacemakerorstainlesssteelcervicalhardware.
Natural History
Most patients with cervical radiculopathyhaveaavorableprognosis.1,6Alargeepide-
miologicstudydemonstratedthatoverave- yearollow-upperiod,31.7percentopatientswith symptomatic cervical radiculopathyhad symptom recurrence and 26 percentneeded surgical intervention or intractablepain,sensorydecit,orobjectiveweakness.1Atnalollow-up,however,nearly90percentopatientswereasymptomaticoronlymildlyincapacitatedbythepain.Theclassicstudyothenaturalhistoryo
cent o patients had no urther symptomsateraewmonths,29percenthadmildorintermittentsymptoms,and27percenthadmoredisablingpain.Nopatientwithradicu-larpainprogressedtomyelopathy.
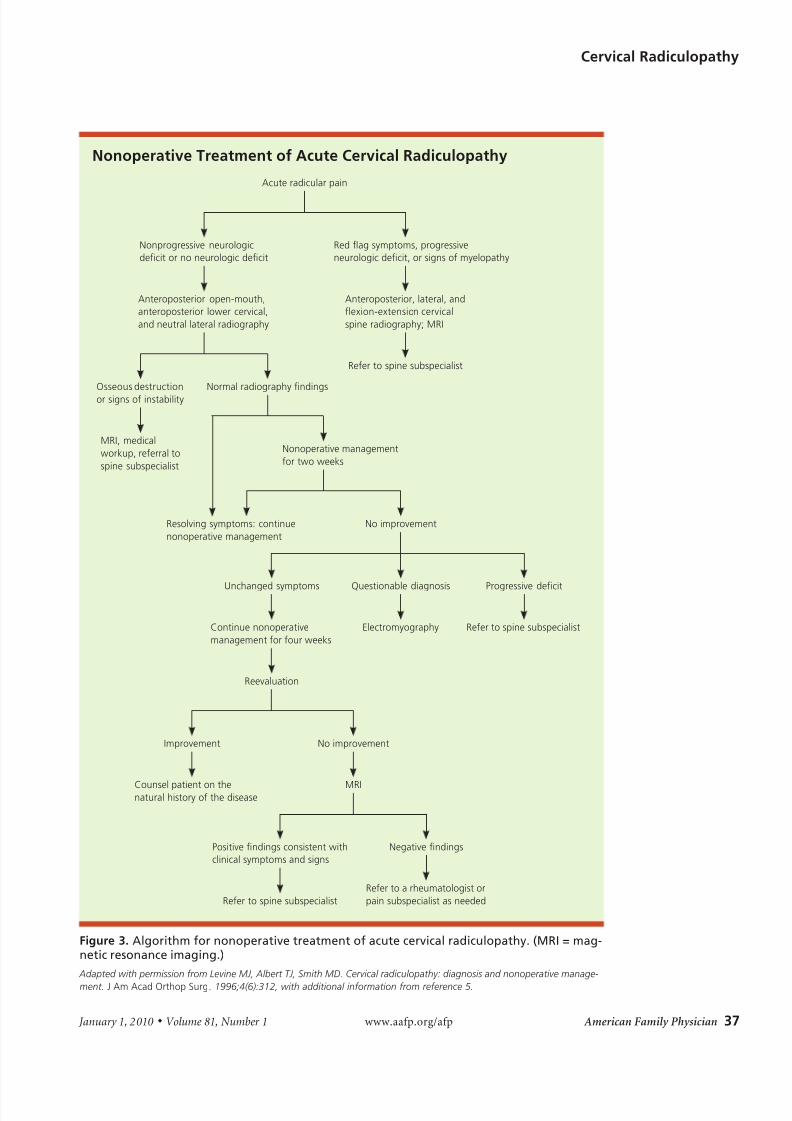
Nonoperative Management Strategies
Inmostpatientswithcervicalradiculopathy,nonoperativetreatment(Figure 32,5)iseective.Inaone-yearcohortstudyo26patientswithdocumentedherniatednucleuspulposusandsymptomaticradiculopathy,a ocused,non-operative treatment programwas successulin92percentopatients.7Littlehigh-qualityevidence supports the use o an individualnonoperative treatment; however, a multi-modalapproachmayalleviatesymptoms.
A B
8/6/2019 Cervical Radiculopathy Nonoperative Management of Neck Pain and Radicular Symptoms
38 American Family Physician www.aap.org/ap Volume 81, Number 1 ◆ January 1, 2010
When approaching the nonoperativemanagementoneckandradicularpain,itisimportanttodistinguishtheacuityothe
process. Pain emanating rom nerve com-pressionbyasotdiskherniationtypicallyhasamoreacutepresentation,withorwith-outradiatingextremitysymptoms.Chronic,bilateralaxialneckandradiatingarmpainis usually caused by cervical spondylosisandmayemanateromavarietyosources,includingthedegenerativediskortheacet joints.Althougheducationabouttheseandother components o cervical radiculopa-thymaybenetsomepatients,asystematicreviewdidnotshowthatpatienteducation
(i.e.,adviceocusingonactivationandcop-ing skills, and traditional neck school) isbenecialinthetreatmentoneckpainandradiculararmpain.8
IMMOBILIZATION
Forpatientswithacuteneckpainsecondarytoradiculopathy,ashortcourse(oneweek)oneckimmobilizationmayreducesymptomsin the infammatory phase.2 Although theeectivenessoimmobilizationwithacer-vicalcollarhasnotbeenproventoalterthecourseorintensityothediseaseprocess,2,3,9itmaybebenecialinsomepatients.
TRACTION
Homecervicaltractionunitsmaydecreaseradicularsymptoms.2,3,10Intheory,tractiondistracts the neural oramen and decom-presses the aected nerve root. Typically,eightto12lbotractionisappliedatanangleo approximately 24 degrees o fexion or15-to20-minuteintervals. 2Tractionismost
benecial when acute muscular pain hassubsidedandshouldnotbeusedinpatientswhohavesignsomyelopathy.2Arecentsys-tematic review o mechanical traction orneckpainomorethanthreemonthsdura-tion,withorwithout radicular symptoms,ound insucient evidence to recommendororagainstitsuseinthemanagementochronicsymptoms.11
PHARMACOTHERAPY
Pharmacotherapymaybebenecialinalle-
viating acute pain associated with cervical
radiculopathy. Although medications havenoprovenbenetorcervicalradiculopathy,positive resultswith their use in the treat-
mentolumbarradiculopathyandlowbackpain suggest a potential role.Nonsteroidalanti-infammatory drugs have been shownto be eective in treating acute low backpain,3,12andmanyphysiciansconsiderthemrst-line agents in the treatment o neckandradiatingarmpain.Somepatientsmaybenetromtheadditiononarcoticanal-gesics,musclerelaxants,antidepressants,oranticonvulsants. Although not specic tocervical radiculopathy, a systematic reviewandameta-analysissuggestthatopioidsmay
Medicationsmaybeeectiveorpatientswithchronicradicularpainwhodeclinesur-gery orhave continued pain ater surgery.A systematic review suggests that tricyclicantidepressants and venlaaxine (Eexor)may produce at least moderate relie inpatients with chronic neuropathic pain.15Similarly, another systematic review sug-gests that tramadol (Ultram) may providesignicantrelieoneuropathicpain. 16
Althoughoralsteroidsarewidelyusedtotreat acute radicular pain via dose packs,no high-quality evidence has shown thatoralsteroidsalterthediseasecourse.3Long-term use o steroids should be avoidedbecauseothepotentialorrare,butserious,
complications.3,12
PHYSICAL THERAPY AND MANIPULATION
Agraduatedphysicaltherapyprogrammaybe benecial in restoring range o motionandoverall conditioningo theneckmus-culature.Intherstsixweeksateronsetopain, gentle range-o-motion and stretch-ingexercisessupplementedbymassageandmodalities such as heat, ice, and electri-calstimulationmaybeused,althoughthisapproachhasnoproven long-term benet.
As thepainimproves, a gradual,isometric
8/6/2019 Cervical Radiculopathy Nonoperative Management of Neck Pain and Radicular Symptoms
January 1, 2010 ◆ Volume 81, Number 1 www.aap.org/ap American Family Physician 39
strengthening program may be initiatedwithprogressiontoactiverange-o-motionandresistiveexercisesastolerated. 3
Nohigh-qualityevidencehasprovedtheeectivenessomanipulativetherapyinthetreatment o cervical radiculopathy. How-ever,limitedevidencesuggeststhatmanipu-lationmayprovideshort-termbenetinthetreatmentoneckpain,cervicogenichead-aches,3,17 and radicular symptoms.18 Rarecomplications, such as worsening radicu-lopathy,myelopathy,andspinalcordinjury,mayoccur.3,19Becauseotheserisksandthelackohigh-qualityevidencetosupportitseectiveness,manipulative therapy cannot
Cervical steroid injectionsmay be consid-ered in the treatment o radicular pain.Cervical perineural injections (e.g., trans-laminarandtransoraminalepidurals,selec-tivenerverootblocks)shouldbeperormedunderradiographicguidanceandonlyaterconrmationopathologyviaMRIorcom-putedtomography.Theseblocksattempttobathetheaectednerverootinsteroids.Onestudydemonstratedsignicantpainrelieat14daysandsixmonthsateraseriesoselec-tivenerverootblocks.20Inanotherprospec-tive cohort series o 21 patients awaitingsurgeryorsymptomaticradiculopathy,cer-vicalinjectionsimprovedpainandreducedtheneedoroperative intervention.21Morerecently, however, a prospective, random-izedstudyo40patientsshowednodier-enceaterthreeweeksbetweenpatientswho
received a steroid injection and those whowereinthecontrolgroups.22Complicationsassociatedwithcervicalinjectionsarerare.One study o a series o more than 1,000blocksshowedaminorcomplicationrateo1.66percentandamajoradverseeventsrateo less than 1 percent.23 However, patientsshould be advised that these rare eventsmaybesevere(e.g.,spinalcordorbrainstemdamage).A recent review o the literaturesuggests that epidural corticosteroids maylead to short-term, symptomatic improve-
Patientsshouldbereerredtoaspinesubspecialistorconsiderationosurgicalinterventionithereisintractableradicularsymptomsunrespon-sivetononoperativemanagementoverasix-week period, motor weaknesspersisting or more than sixweeks, progressive neurologicdecitatanypointatersymp-tomonset, signs or symptomsomyelopathy,orinstabilityordeormity o the spine.25 The
Washington State DepartmentoLaborandIndustries’criteriaor initiating surgicalmanage-mentaresixtoeightweeksoconservativecare (i.e.,physical therapy,medications, ortraction); subjective sensory symptoms orSpurlingsign,objectivemotor,refex,orelec-tromyographyndings;andabnormalimag-ingndingsthatcorrelatewiththepatient’ssymptoms.26Alternatively,intherarepatientwho has radicular pain without objectivephysical examination or electromyographyndings,aselectivenerverootblockmaybeused.Ithenerveblockis“positive,”oreec-tiveinpartiallyalleviatingsymptoms,thensurgerymaybeconsidered.
The Author
JASON DAVID EUBANKS, MD, is an assistant professor inthe Department of Orthopaedic Surgery, Division of SpineSurgery, at Case Western Reserve University School of Medicine in Cleveland, Ohio. At the time this manuscriptwas written, Dr. Eubanks was a spine fellow at the Univer-sity of Pittsburgh ( Pa.) Medical Center.
Address correspondence to Jason David Eubanks, MD,Dept. of Orthopaedics, University Hospitals Case Medi-cal Center, 11100 Euclid Ave., Cleveland, OH 44106.Reprints are not available from the author.