6/8/2017 1 Cesarean Scar Pregnancy: Know what you are doing Cesarean Scar Pregnancy: Know what you are doing Ilan Timor-Tritsch MD Ilan Timor-Tritsch Ilan Timor-Tritsch C-section rate within 22 developed countries between 1997 and 2008 Slide Courtesy of Prof.Stanojevic Cesarean Rates (per 1,000 births), Industrialized Countries,1990-2004 50 100 150 200 250 300 350 400 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 Italy U.S. Germany Netherlands Denmark UK Source: OECD Health Data 2006 Morbidly adherent placentae 1994-2002: 1 in 2000-2500 1994-2002: 1 in 2000-2500 Cesarean scar pregnancy 2010: 1 in 2000-2500
Transcript
6/8/2017
1
Cesarean Scar Pregnancy: Know what you are doing
Cesarean Scar Pregnancy: Know what you are doing
Ilan Timor-Tritsch MD
Ilan Timor-TritschIlan Timor-Tritsch
C-section rate within 22 developed countries between 1997 and 2008
Slide Courtesy of Prof.Stanojevic
Cesarean Rates (per 1,000 births),
Industrialized Countries,1990-2004
50
100
150
200
250
300
350
400
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
Italy
U.S.
Germany
Netherlands
Denmark
UK
Source: OECD Health Data 2006
Morbidly adherent placentae
1994-2002: 1 in 2000-25001994-2002: 1 in 2000-2500
Cesarean scar
pregnancy2010: 1 in 2000-2500
6/8/2017
2
Background
• The increasing incidence of cesarean scar pregnancy (CSP) is directly related to the increase in the rate of cesarean deliveries.
• I base this talk upon some of our previous work on the subject
Timor-Tritsch IE, Monteagudo A, Santos R, Tsymbal T, Pineda G, Arslan AA. The diagnosis, treatment, and follow-up of cesarean scar pregnancy. 6. Timor-Tritsch IE, Monteagudo A. Unforeseen consequences of the increasing rate of cesarean deliveries: early placenta accreta andTimor-Tritsch IE, Monteagudo A, Santos R, Tsymbal T, Pineda G, Arslan AA. The diagnosis, treatment, and follow-up of cesarean scar pregnancy. 6. Timor-Tritsch IE, Monteagudo A. Unforeseen consequences of the increasing rate of cesarean deliveries: early placenta accreta andTimor-Tritsch IE, Monteagudo A, Santos R, Tsymbal T, Pineda G, Arslan AA. The diagnosis, treatment, and follow-up of cesarean scar pregnancy. 6. Timor-Tritsch IE, Monteagudo A. Unforeseen consequences of the increasing rate of cesarean deliveries: early placenta accreta and
Timor-Tritsch IE, Monteagudo A, Santos R, Tsymbal T, Pineda G, Arslan AA. The diagnosis, treatment, and follow-up of cesarean scar pregnancy. Am J Obstet Gynecol 2012;207:44 Timor-Tritsch IE, Monteagudo A. Unforeseen consequences of the increasing rate of cesarean deliveries: early placenta accreta and cesarean scar pregnancy. A review. Am J Obstet Gynecol2012;207:14-29.
Objectives• 1. Teach practicing clinicians to Diagnose a
cesarean scar pregnancy (CSP), using diagnostic criteria and RELIABLYdifferentiate it from an intrauterine and a cervical pregnancy.
• 2. Realize that there is a common histologic basis of CSP and morbidly adherent placenta (MAP) such as accreta, increta and percreta, and that CSP is its main precursor.
• 3. Construct an evidence based counseling and management plan taking into consideration patients' obstetrical goals.
Outline1. What is a cesarean scar pregnancyIncidence1. Diagnosis2. Natural history if left untreated3. Treatment
1. Choices in the literature2. Management complications3. Best treatment: Is there any single one?
4. Conclusions
6/8/2017
3
Outline1. What is a cesarean scar pregnancy
2. Pathogenesis3. Incidence4. Diagnosis5. Natural history if left untreated6. Treatment
1. Choices in the literature2. Management complications3. Best treatment: Is there any single one?
7. Conclusions
1. What is a cesarean scar pregnancy (CSP)
Synonyms in the literature: Scar pregnancy, Cesarean section scar
ectopic, Section scar ectopic
• CSP is a iatrogenic entity
• A blastocyst implants in a microscopic or macroscopic
tract on the uterine scar or in the “niche” left
by the incision, in the anterior uterine wall
• The mechanism is similar to implantations after uterine
surgery (myomectomy, curettage, endometrial ablation,
manual removal of placenta etc)
The general knowledge in the community
6/8/2017
4
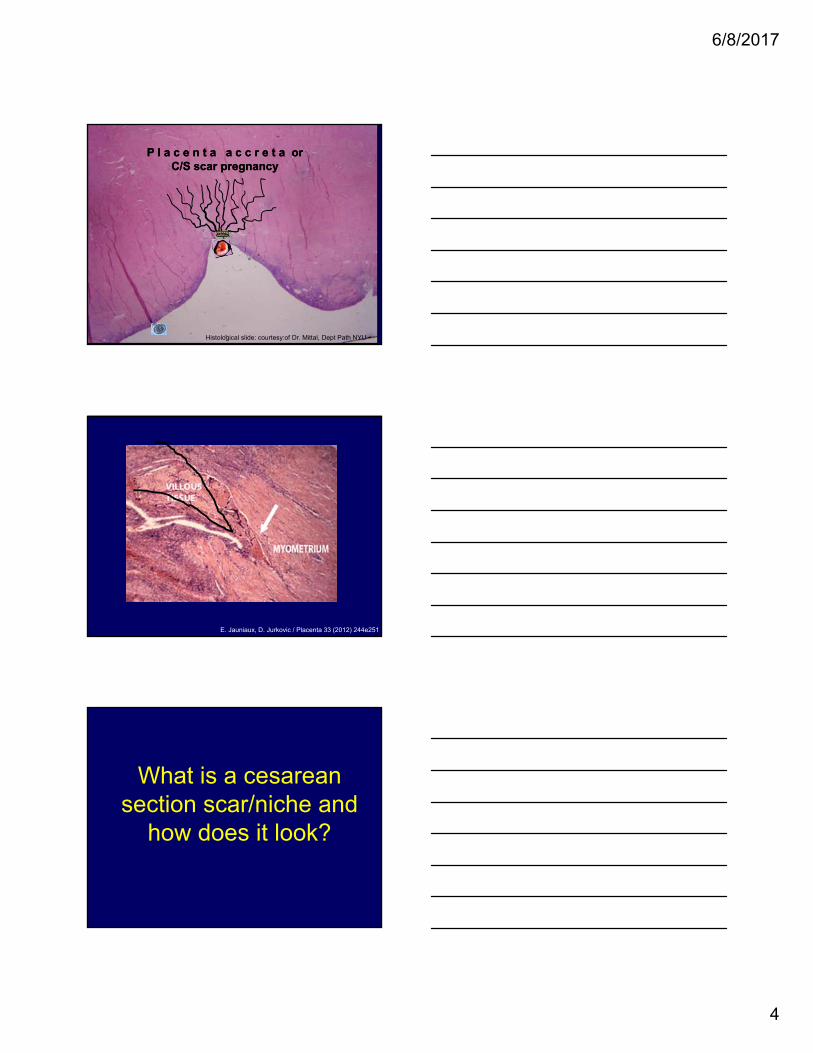
P l a c e n t a a c c r e t a or C/S scar pregnancy
P l a c e n t a a c c r e t a or C/S scar pregnancy
Histological slide: courtesy:of Dr. Mittal, Dept Path NYU
E. Jauniaux, D. Jurkovic / Placenta 33 (2012) 244e251
What is a cesarean section scar/niche and
how does it look?
6/8/2017
5
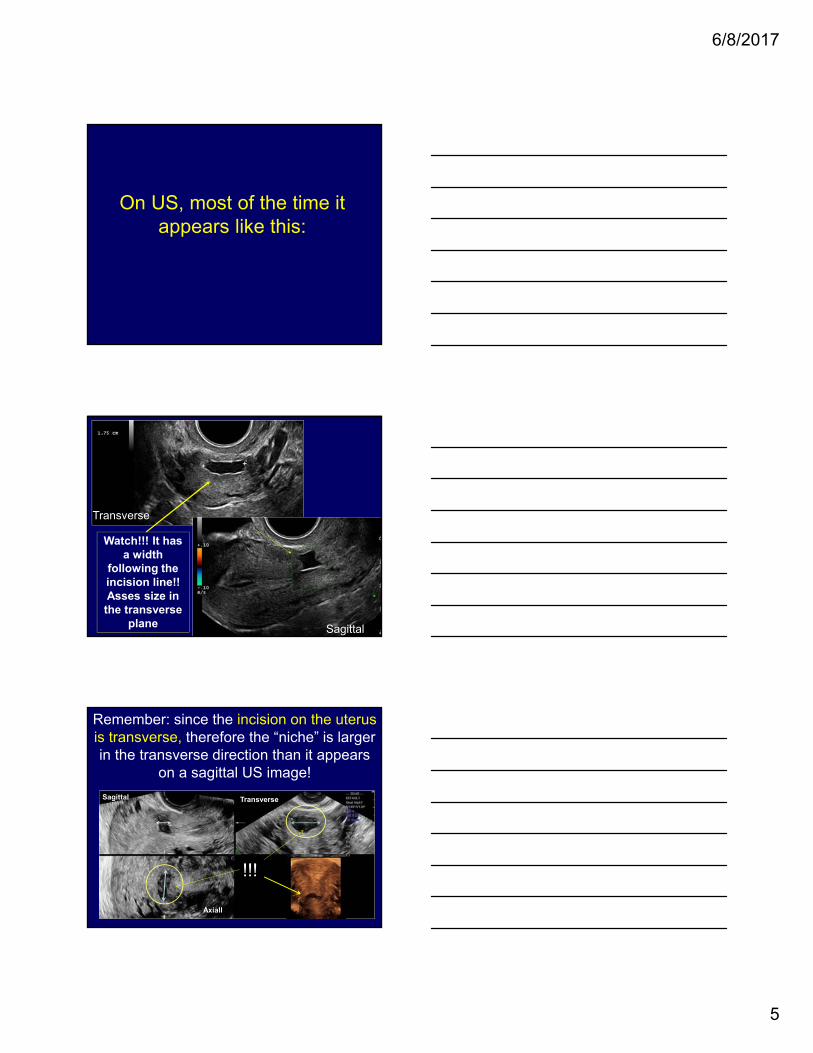
On US, most of the time it appears like this:
Transverse
Sagittal
Watch!!! It has a width
following the incision line!!Asses size in the transverse
plane
Remember: since the incision on the uterus is transverse, therefore the “niche” is larger in the transverse direction than it appears
on a sagittal US image!
Sagittal
Axiall
Transverse
!!!
6/8/2017
6
Sagittalmidline
Transverse
Horizontal along the incision line
3D US angiography of the vessels along the incision line
2. Pathogenesis
Sequence of events after fertilization
6/8/2017
7
• Normal implantation involves invasion of the uterine wall by two subgroups of extravilloustrophoblast: - the interstitial trophoblast invades through the endometrium and the superficial one-third of the myometrium.
- the endovascular trophoblast invades and remodels the maternal spiral arterioles *.
The Extravillous Trophoblasts appear, differentiate and start invading the
decidua
*Tantbirojn et al, Placenta 2008; 29:639
In early pregnancy, trophoblast cells invade the the uterus, where they transform spiral arteries to ensure the enhanced delivery of blood to the developing fetus at a low pressure
In a normal pregnancy there is a mechanism that stops the trophoblastic invasion:
The Fibrinoid Layers between the decidua and the
myometrium
6/8/2017
8
Fetomaternal immune cross-talk and its consequences for maternal and offspring's healthPetra C Arck & Kurt Hecher Nature Medicine 2013
N I t a b u c h’s F i b r I n o I d L a y e r N I t a b u c h’s F i b r I n o I d L a y e r
By far, the biggest insult on the uterus is a cesarean
section resulting in not only scaring but also leaves a
dehiscence (“niche”) at the incision area
• Propose that the extent of uterine wall ‘‘invasion’’ by placental villi (and resulting accreta vs. increta and percreta) may be dependent on the depth of the scar.
And that “placenta increta and percreta are not due to a further invasion of extravillous trophoblast in the uterine wall, rather they likely arise
secondary to dehiscence of a scar, leading to the presence of chorionic villi deep within the uterine wall, and thus give extravillous trophoblast greater access to the deep myometrium”.
6/8/2017
9
• ExaminedUS features of CS scars in non-pregnant, women to identify factors associated with scar deficiency.
Deficiency ratio =c/d
The loss of more than 50% of myometrial mantle at the scar level was classified as severe deficiency.
• Conclusion Deficient uterine scars are a frequent finding in women with a Hx of PrC/S.
• The risk of scar deficiency is increased in women with a retroflexed uterus and in those who have undergone multiple C/Ss
Other theories of pathogenesis of CSP:
IVF centers use artificially “denuding” small area of the cavity to cause “inflammatory response” to increase implantation***
***Barash A et al, Fertil Steril 2003;79:1317-2***Gnainsky Y et al, Fertil Steril 94:2003-36
*Glenbacev et al Regulation of human placental development by oxigen tension. SCIENCE 1997; 277
The theory of “low oxygen tension” in the scar that facilitates oocyte implantation*
Kleiman HJ et al, Placenta 1990; 11:349-367
The “exposed cellular matrix “ attracting the throphoblast**
Theories of the pathogenesis.Uterine interventions lead to the thinning or missing Nitabuch fibrinoid layer. The placenta will attach itself deeply into the uterine wall
•
Rosen T. Placenta accreta and cesarean scar pregnancy: overlooked costs of the rising cesarean section rate. Clin Perinatol 2008;35:519-29,
??
6/8/2017
10
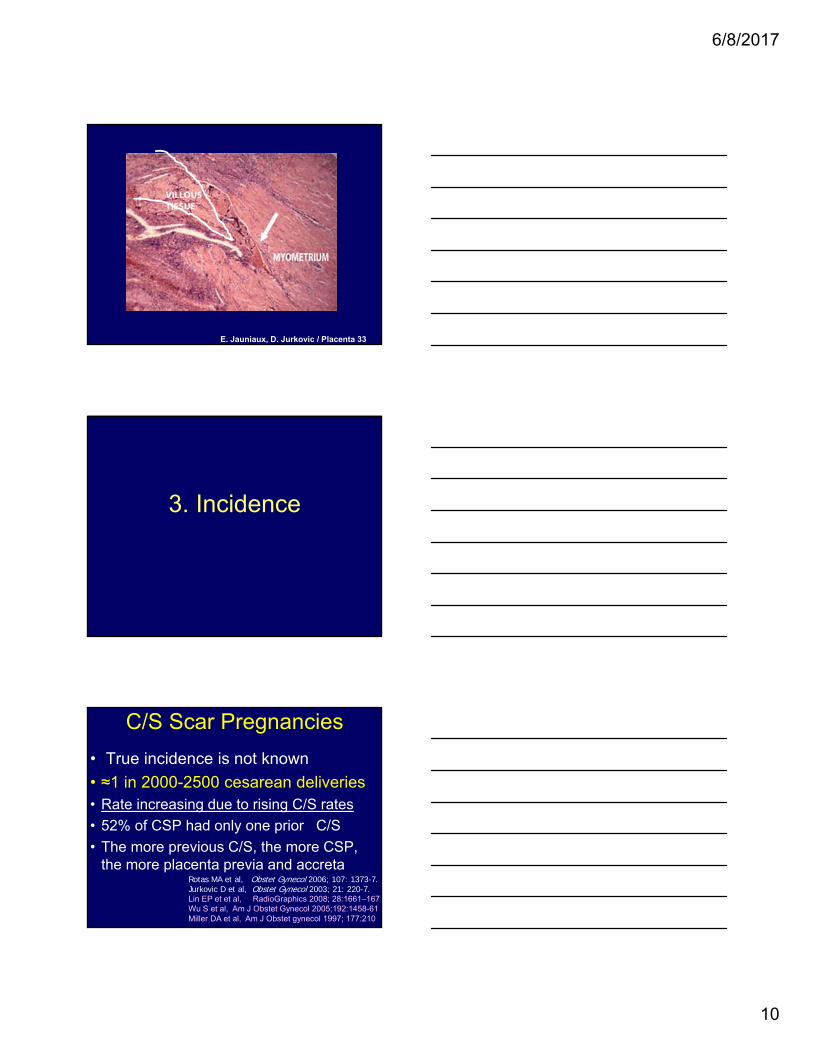
E. Jauniaux, D. Jurkovic / Placenta 33
3. Incidence
C/S Scar Pregnancies
• True incidence is not known
• ≈1 in 2000-2500 cesarean deliveries• Rate increasing due to rising C/S rates
• 52% of CSP had only one prior C/S
• The more previous C/S, the more CSP, the more placenta previa and accreta
Rotas MA et al, Obstet Gynecol 2006; 107: 1373-7.Jurkovic D et al, Obstet Gynecol 2003; 21: 220-7. Lin EP et et al, RadioGraphics 2008; 28:1661–1671Wu S et al, Am J Obstet Gynecol 2005;192:1458-61Miller DA et al, Am J Obstet gynecol 1997; 177:210
6/8/2017
11
The inevitable consequences
Morbidly adherent placentae (“accreta”)
and CSP rates parallel the increasing CD rates
4. How do we make the diagnosis and which are the differential
diagnoses?
6/8/2017
12
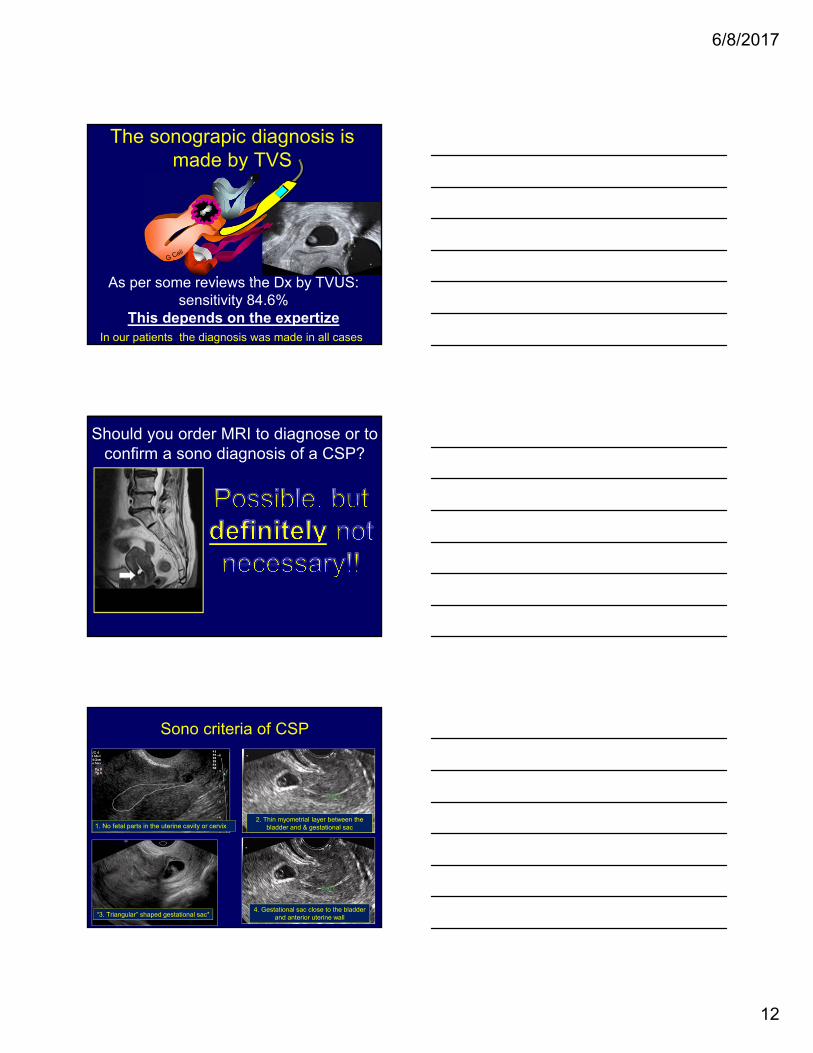
The sonograpic diagnosis is made by TVS
As per some reviews the Dx by TVUS: sensitivity 84.6%
This depends on the expertizeIn our patients the diagnosis was made in all cases
Should you order MRI to diagnose or to confirm a sono diagnosis of a CSP?
Sono criteria of CSP
“3. Triangular” shaped gestational sac*
1. No fetal parts in the uterine cavity or cervix 2. Thin myometrial layer between the
bladder and & gestational sac
4. Gestational sac close to the bladder and anterior uterine wall
6/8/2017
13
5. Rarely: A-V malformation at the site of a CS
High peak systolic velocity
The differential diagnosis1. Cervical Pregnancy – however – remember:
Cx pregnancy is EXTREMELY rare & occur in intact uteri
2. IUP in the process of abortion – however –they very rarely have a beating heart!
Therefore:
If the chorionic sac is low, close to the cervix and the patient had a previous
cesarean delivery: IT IS A CSP!!!!
If the gestational sac is below it: suspect a CSP or a cervical
pregnancy. Counsel accordingly
If the gestational sac is above it: it is mostly a normal implantation
Sensitivity = 93.0%, Specificity = 98.9%,
PPV = 96.4%, NPV = 97.9%.
On a panoramic, longitudinal, sagittal scan determine the location of the gestational sac by dividing the uterus in half by
an imaginary line
Am J Obstet Gynecol February 2016
6/8/2017
14
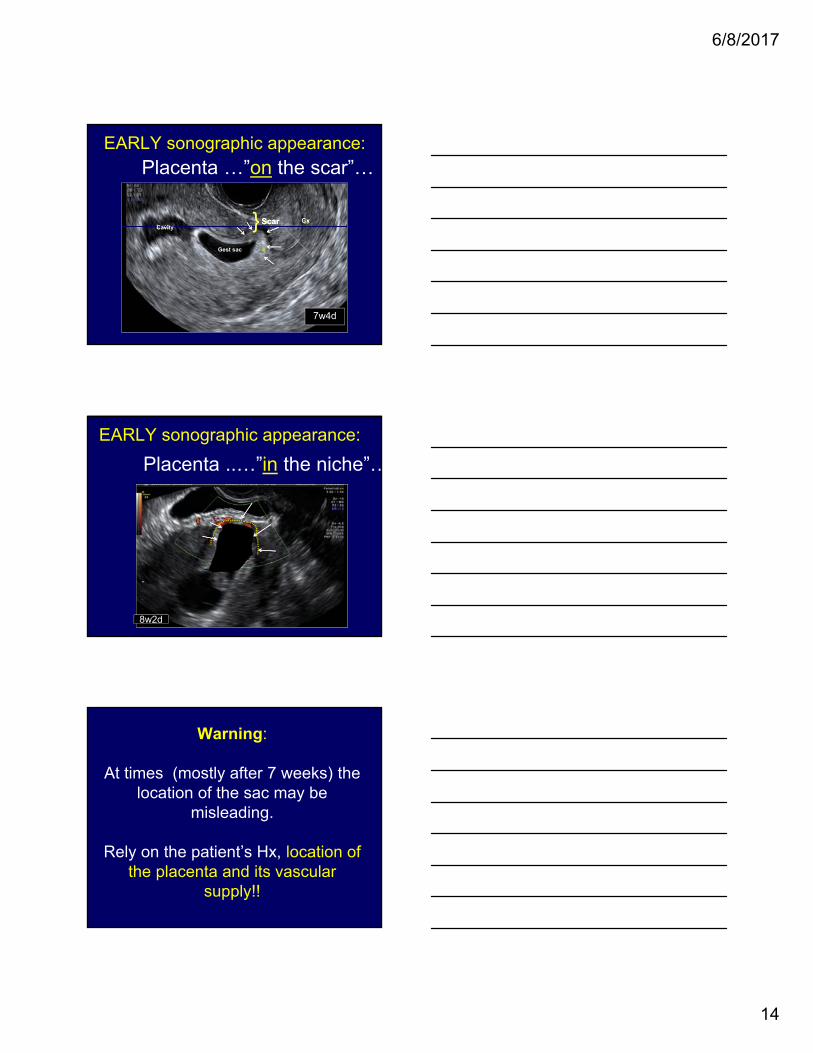
EARLY sonographic appearance:
7w4d
} ScarScar CxCavity
Gest sac
Placenta …”on the scar”…
EARLY sonographic appearance:
Placenta ..…”in the niche”…
8w2d
Warning:
At times (mostly after 7 weeks) the location of the sac may be
misleading.
Rely on the patient’s Hx, location of the placenta and its vascular
supply!!
6/8/2017
15
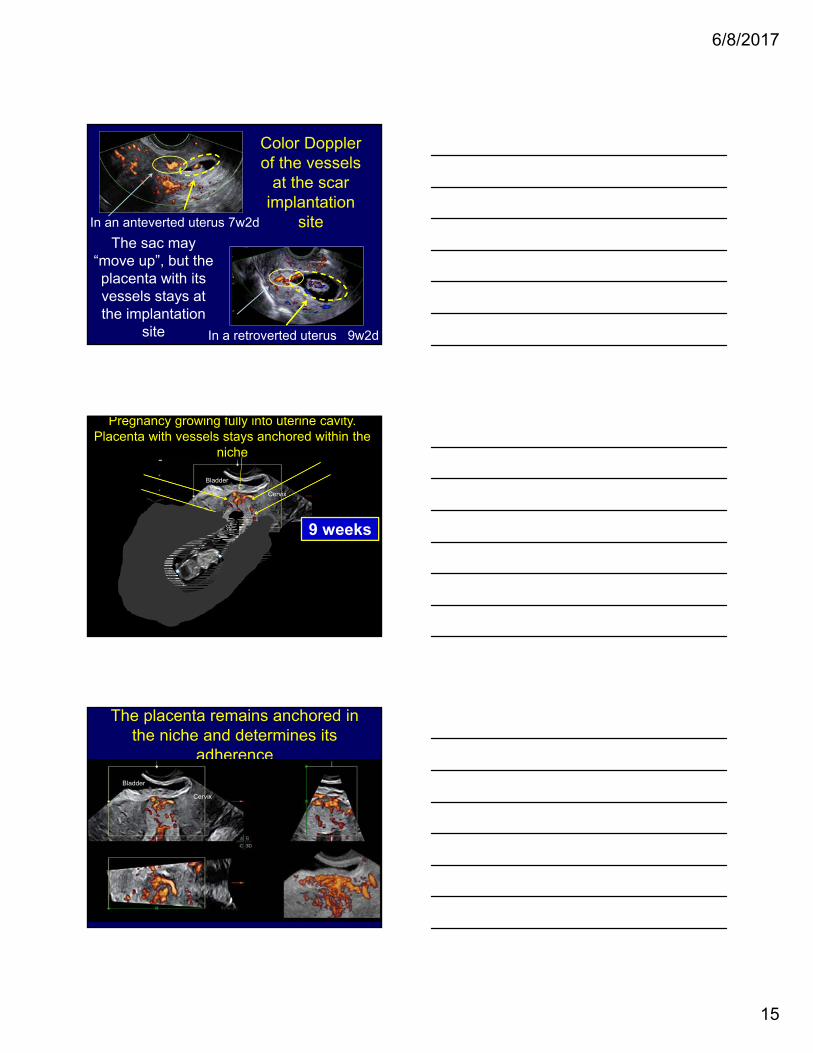
In an anteverted uterus 7w2d
Color Doppler of the vessels
at the scar implantation
site
In a retroverted uterus 9w2d
The sac may “move up”, but the placenta with its vessels stays at the implantation
site
Pregnancy with placenta implanted in the niche of the previous C/S
Bladder
6 weeks7 weeks9 weeks
Cervix
Pregnancy growing with sac moving towards the uterine cavity
Pregnancy growing fully into uterine cavity. Placenta with vessels stays anchored within the
niche
The placenta remains anchored in the niche and determines its
adherence
Bladder
Cervix
6/8/2017
16
5. What is the natural history of CSP?
First question:Are scar pregnancy and morbidly
adherent placenta the same disease?
If they are the same disease they have to share the same histology
2 Pathologists independantly examined the microscopic images
1 ?? 2 ?? 5 ??3 ?? 4 ??
Copyright releases obtained
for all pictures
They could not identified which were CSP and which were MAP
by histology
6/8/2017
17
• Conclusions:
• This study supports our hypothesis, that Cesarean Scar Pregnancy and Early Placenta Accreta are one and the same histopathologic entity and are an early manifestation of the morbidly adherent placenta.
5. What is the natural history of CSP?
The second question is if scar pregnancy is precursor of
morbidly adherent placenta?
Our Hypothesis: In the 1st trimester CSP is the clinical expression of placenta
accreta and percreta
6/8/2017
18
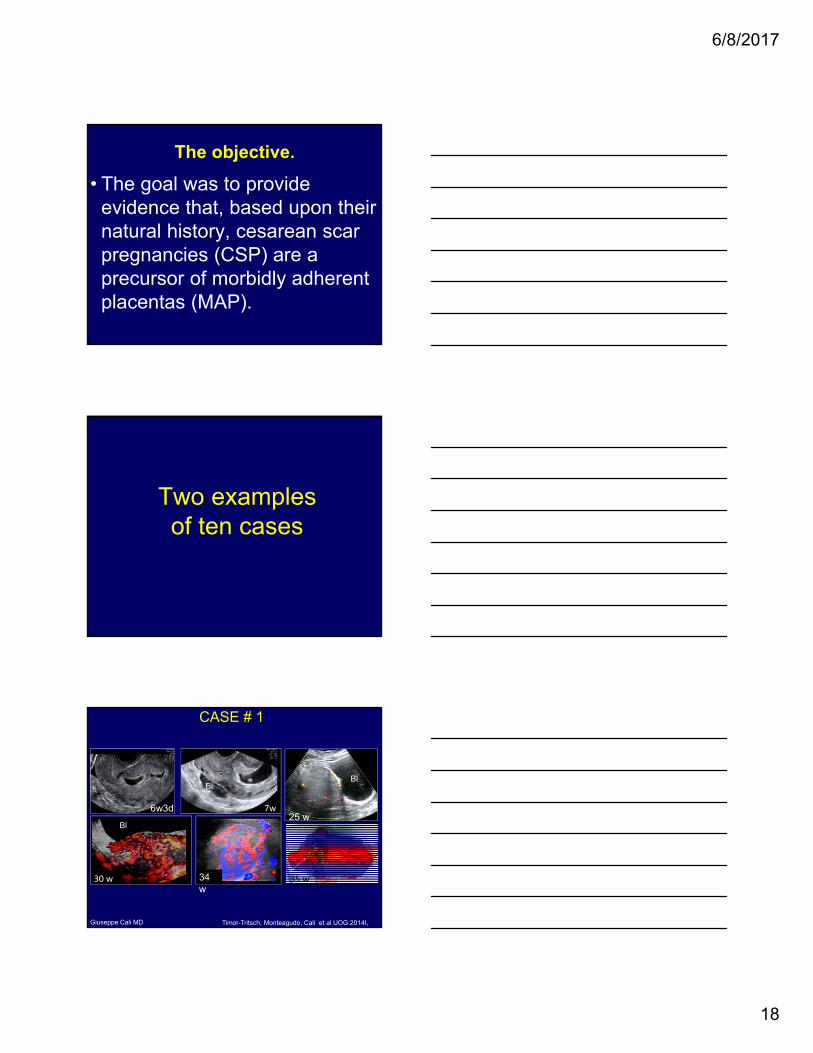
The objective.
• The goal was to provide evidence that, based upon their natural history, cesarean scar pregnancies (CSP) are a precursor of morbidly adherent placentas (MAP).
Two examplesof ten cases
6w3d 7w
30 w 34 w
25 w
35 w
BlBl
Bl
Giuseppe Cali MD
CASE # 1
Timor-Tritsch, Monteagudo, Cali et al UOG 2014I,
6/8/2017
19
Bl
Bl
15w2d
Bl
17w 2d 20 w
9w2d
Bl
Ilan Timor-Tritsch and Anthony Vintzileos MD
CASE # 6
Timor-Tritsch, Monteagudo, Cali et al UOG 2014I,
Results• Nine out of 10 patients diagnosed with 1st
∆ CSP delivered preterm or near term viable offspring
• One patient had a fetal loss and hysterectomy at 20 weeks
• Nine patients had cesarean deliveries and hysterectomies & 7 had significant bleeding
• All 10 patients had placenta percretaTimor-Tritsch, Monteagudo, Cali et al UOG 2014I,
• The cases in this series validate the hypothesis that CSP is a precursor of MAP, both sharing the same histopathology.
• Our findings provide evidence that can beused to counsel patients with CSP, to enable them to make an informed choice between 1st∆ TOP and continuation of the pregnancy, with its risk of premature delivery and loss of uterus and fertility.
Conclusion
6/8/2017
20
It is clear that there is no uniform and agreed upon
definition of the type and depth of implantation placental and its
correlation to outcome
Importance of measureing bladder-to-sac distance
• Rarely is there information about bladder-to-sac distance or overlying myometrial thickness
• The literature is not only confusing as to the sac location, but…..
• Furthermore , usually there is no distinction between “gestational sac” and “placenta”
• Lastly, there is rarely any mention about location of placental vascularization
To correctly measure the sac-to-bladder distance, we need a precise definition of implantation, since
it may determine outcome
Sporadically, but increasingly, le literature makes a distinction
between implantation “on the scar tissue” and “in the niche
(dehiscence)”
6/8/2017
21
No concensus (yet) on the scac location
• Comstock: “Low lying: versus--surrounded by myometrium”
-- Comstock CH, Bronsteen RA. The antenatal diagnosis of placenta accreta. BJOG 2014;121:171–182-- Twickler DM, Lucas MJ, Balis AB, et al. Color flow mapping for myometrial invasion in women with a prior cesarean delivery. J Matern Fetal Med2000; 9:330–335.Does the presence of a Caesarean section scar affect implantation site and early pregnancy outcome in women attending an early pregnancy assessment unit?--Naji O, Wynants L, Smith A, Abdallah Y, Saso S, Stalder C, Van Huffel S, Ghaem-Maghami S, Van Calster B, Timmerman D, Bourne T.Hum Reprod. 2013 Jun;28(6):1489-96.Sonographic Findings of Morbidly Adherent Placenta in the First Trimester--Rac MW, Moschos E, Wells CE, McIntire DD, Dashe JS, Twickler DM.J Ultrasound Med. 2016 Feb;35(2):263-9
• Twickler: < 1mm predicted MAP
• Naji: away from scar, close to scar, crossing the scar, inside the scar (CSP)
• Rac: smallest anterior myometrial thickness on 1st ∆ sonography significantly improved detection of morbidly adherent placenta.
KAELIN AGTEN A., CALI G., MONTEAGUDO A., OVIEDO J. TIMOR-TITSCH I.E. he clinical outcome of cesarean scar pregnancies implanted “on the scar” versus “in the niche. AJOG 2016
According to our 2016 study of 17 CSP cases who continued their pregnancy:
• 6 patients with CSP implanted “on the scar” had a substantial better outcome (1 hysterectomy for accreta), compared to 11 patients with CSP implanted “in the niche” (all had hysterectomy for percreta)
• Myometrial thickness below 2mm in the 1st trimester US was associated with Morbidly Adherent Placenta at delivery.
6. Treatment of CSP
6/8/2017
22
1. First trimester treatment choices, if continuing the
pregnancy is NOT an option
The major treatment modalities• Surgical requiring general anesthesia
– Major: laparotomy
– Minor: Laparoscopy, Hysteroscopy; D&C
• Minimally invasive: Local injection (MTX/KCl)
• Systemic– Major: UAE
– Minor: IM Methotrexate (single/multiple
• Different combinations of the above– Simultaneously
– Sequentially
Volume 207, Issue 1, July 2012, Pages 14–29
6/8/2017
23
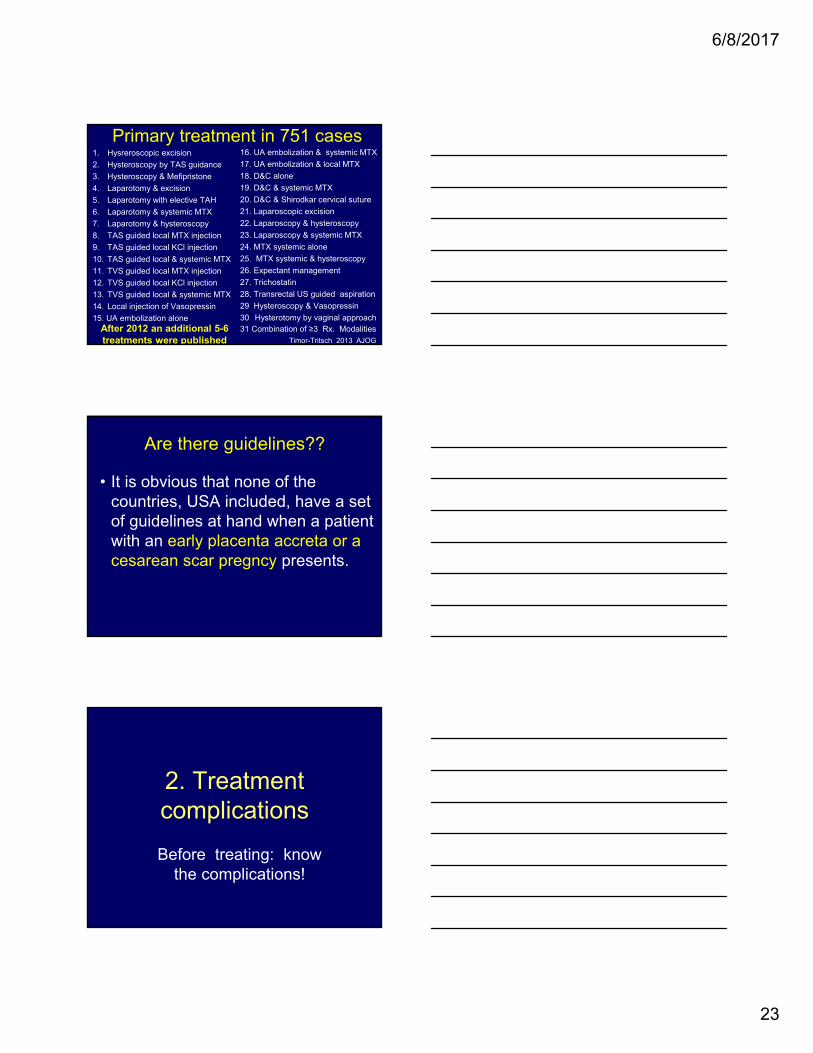
Primary treatment in 751 cases16. UA embolization & systemic MTX
17. UA embolization & local MTX
18. D&C alone
19. D&C & systemic MTX
20. D&C & Shirodkar cervical suture
21. Laparoscopic excision
22. Laparoscopy & hysteroscopy
23. Laparoscopy & systemic MTX
24. MTX systemic alone
25. MTX systemic & hysteroscopy
26. Expectant management
27. Trichostatin
28. Transrectal US guided aspiration
29 Hysteroscopy & Vasopressin
30 Hysterotomy by vaginal approach31 Combination of ≥3 Rx. Modalities
1. Hysreroscopic excision
2. Hysteroscopy by TAS guidance
3. Hysteroscopy & Mefipristone
4. Laparotomy & excision
5. Laparotomy with elective TAH
6. Laparotomy & systemic MTX
7. Laparotomy & hysteroscopy
8. TAS guided local MTX injection
9. TAS guided local KCl injection
10. TAS guided local & systemic MTX
11. TVS guided local MTX injection
12. TVS guided local KCl injection
13. TVS guided local & systemic MTX
14. Local injection of Vasopressin
15. UA embolization alone
Timor-Tritsch 2013 AJOG
After 2012 an additional 5-6 treatments were published
Are there guidelines??
• It is obvious that none of the countries, USA included, have a set of guidelines at hand when a patient with an early placenta accreta or a cesarean scar pregncy presents.
2. Treatment complications
Before treating: know the complications!
6/8/2017
24
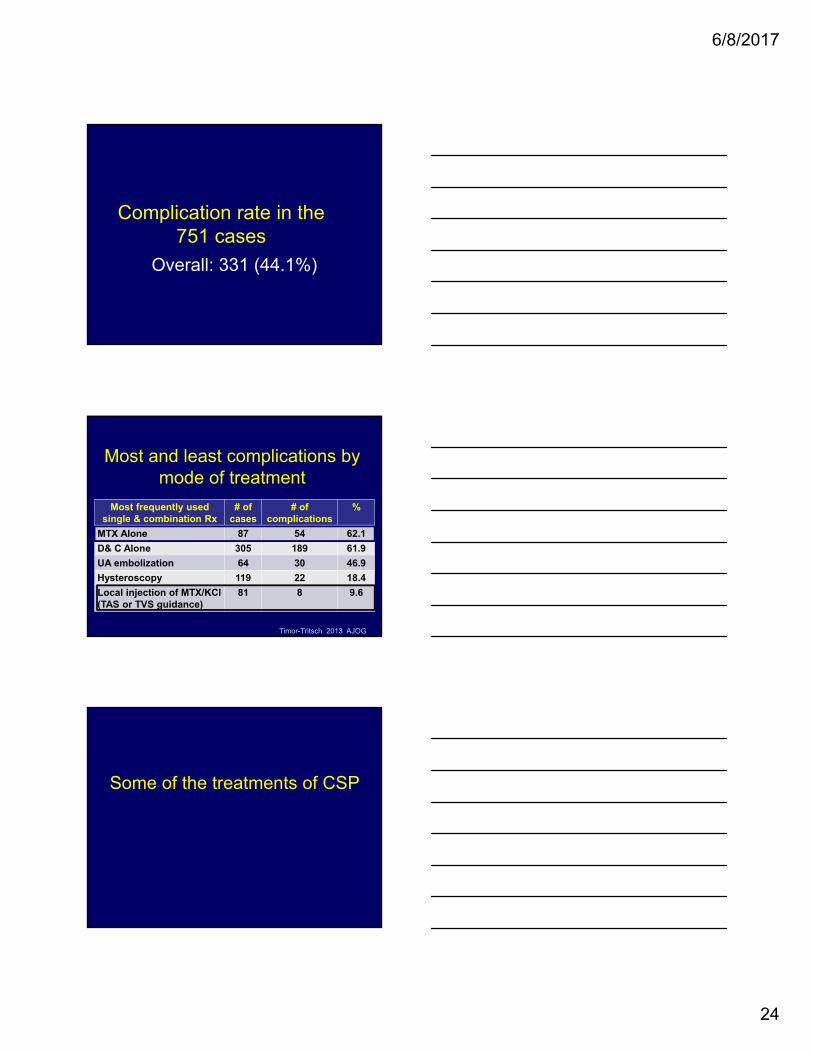
Complication rate in the 751 cases
Overall: 331 (44.1%)
Most frequently used single & combination Rx
# of cases
# of complications
%
MTX Alone 87 54 62.1
D& C Alone 305 189 61.9
UA embolization 64 30 46.9
Hysteroscopy 119 22 18.4
Local injection of MTX/KCl(TAS or TVS guidance)
81 8 9.6
Most and least complications by mode of treatment
Timor-Tritsch 2013 AJOG
Some of the treatments of CSP
6/8/2017
25
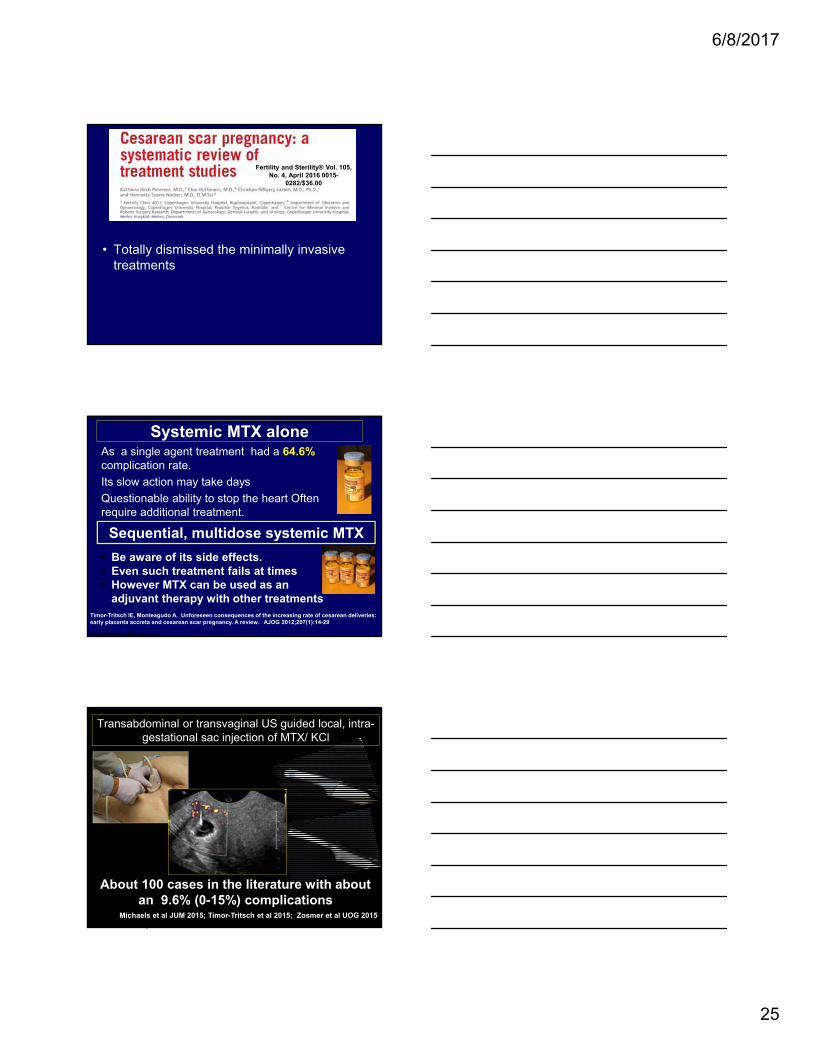
Fertility and Sterility® Vol. 105, No. 4, April 2016 0015-
0282/$36.00
• Totally dismissed the minimally invasive treatments
Systemic MTX alone• As a single agent treatment had a 64.6%
complication rate.
• Its slow action may take days
• Questionable ability to stop the heart Often require additional treatment.
Timor-Tritsch IE, Monteagudo A. Unforeseen consequences of the increasing rate of cesarean deliveries: early placenta accreta and cesarean scar pregnancy. A review. AJOG 2012;207(1):14-29
Timor-Tritsch & Monteagudo
Sequential, multidose systemic MTX
Be aware of its side effects. Even such treatment fails at times However MTX can be used as an
adjuvant therapy with other treatments
Transabdominal or transvaginal US guided local, intra-gestational sac injection of MTX/ KCl
About 100 cases in the literature with about an 9.6% (0-15%) complications
Michaels et al JUM 2015; Timor-Tritsch et al 2015; Zosmer et al UOG 2015 Timor-Tritsch & Monteagudo
6/8/2017
26
Operative hysteroscopy alone or in combination
About 119 cases reviewed in the literature with the second lowest (about 18%) complication rate (mostly bleeding)
Timor-Tritsch 2012 AJOGTimor-Tritsch & Monteagudo
Suction aspiration and/or SHARP D&C alone or in combined with inflation of Foley balloon
Larger balloon Foley (50cc)
Timor-Tritsch & Monteagudo
3D US display of rich vascular
supply surrounding the
chorionic sac of a scar pregnancy
This explains the possible bleeding complication of a
D&C when the scar pregnancy is subjected to
curettage
The use of a single balloon Foley catheter as andjuvant to local, intragestational injection
of MTX
Timor-Tritsch & Monteagudo
6/8/2017
27
Our treatment approach for CSP in
the last 3-4 years
Inject locally & place balloon
Place single balloon as single treatment OR
New treatment for CSP and Cervical pregnancy
Timor-Tritsch, Monteagudo, Bennett, Foley,,Kaelin Agten. A new minimally invasive treatment for cesarean scar and cervical pregnancy. AJOG 2016
6/8/2017
28
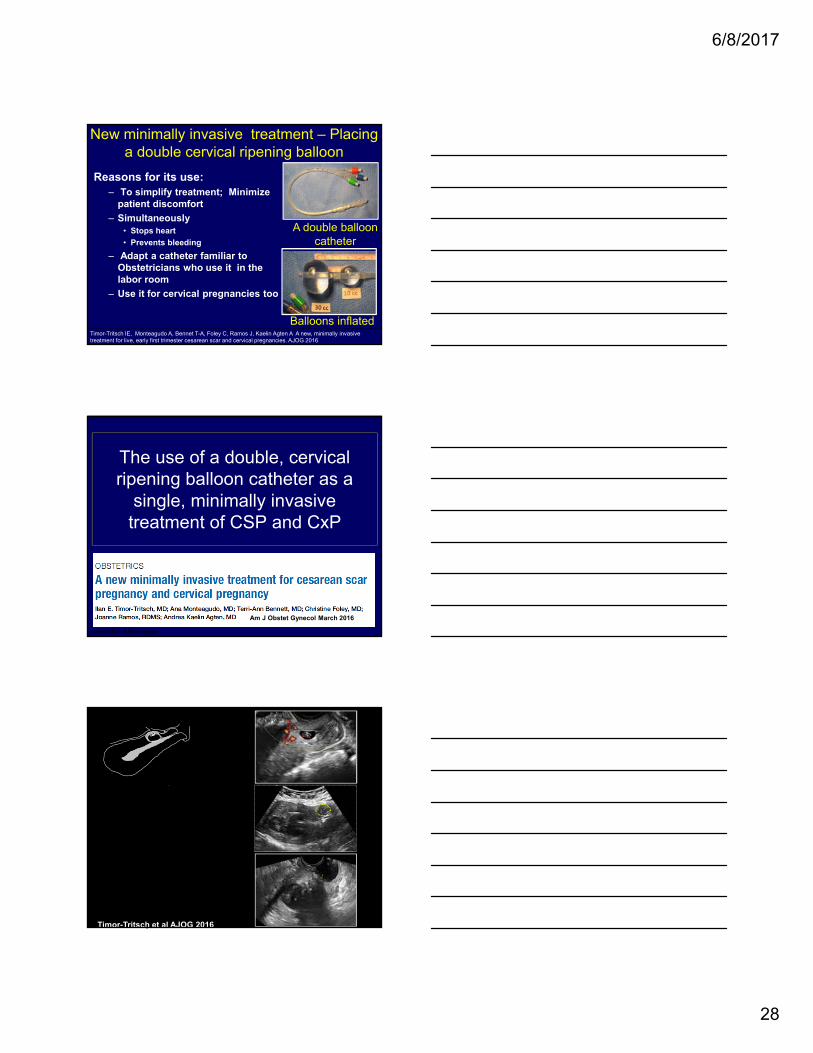
Reasons for its use:– To simplify treatment; Minimize
patient discomfort
– Simultaneously• Stops heart
• Prevents bleeding
– Adapt a catheter familiar to Obstetricians who use it in the labor room
– Use it for cervical pregnancies too
A double balloon catheter
Balloons inflated
New minimally invasive treatment – Placing a double cervical ripening balloon
Timor-Tritsch IE, Monteagudo A, Bennet T-A, Foley C, Ramos J, Kaelin Agten A A new, minimally invasive treatment for live, early first trimester cesarean scar and cervical pregnancies. AJOG 2016
The use of a double, cervical ripening balloon catheter as a
single, minimally invasive treatment of CSP and CxP
Timor-Tritsch & Monteagudo
Am J Obstet Gynecol March 2016
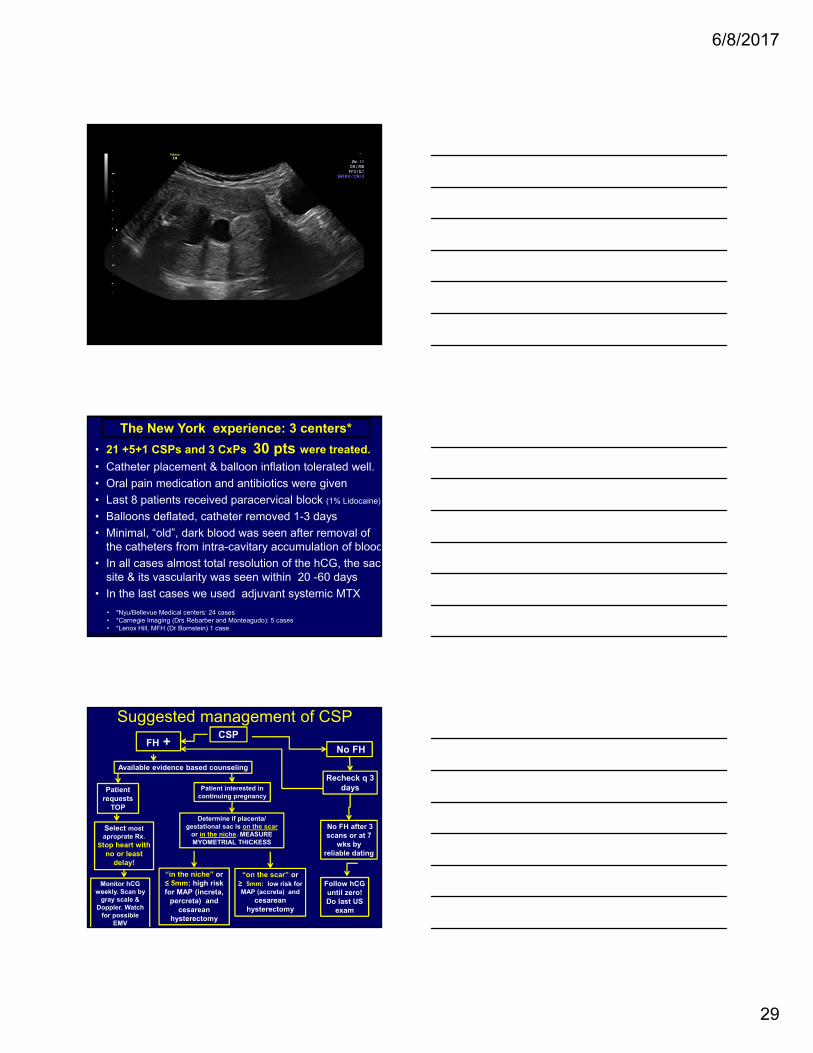
Timor-Tritsch & MonteagudoTimor-Tritsch et al AJOG 2016
• Last 8 patients received paracervical block (1% Lidocaine)
• Balloons deflated, catheter removed 1-3 days
• Minimal, “old”, dark blood was seen after removal of the catheters from intra-cavitary accumulation of blood
• In all cases almost total resolution of the hCG, the sac site & its vascularity was seen within 20 -60 days
• In the last cases we used adjuvant systemic MTX
The New York experience: 3 centers*
Timor-Tritsch & Monteagudo
• *Nyu/Bellevue Medical centers: 24 cases• *Carnegie Imaging (Drs Rebarber and Monteagudo): 5 cases• *Lenox Hill, MFH (Dr Bornstein) 1 case
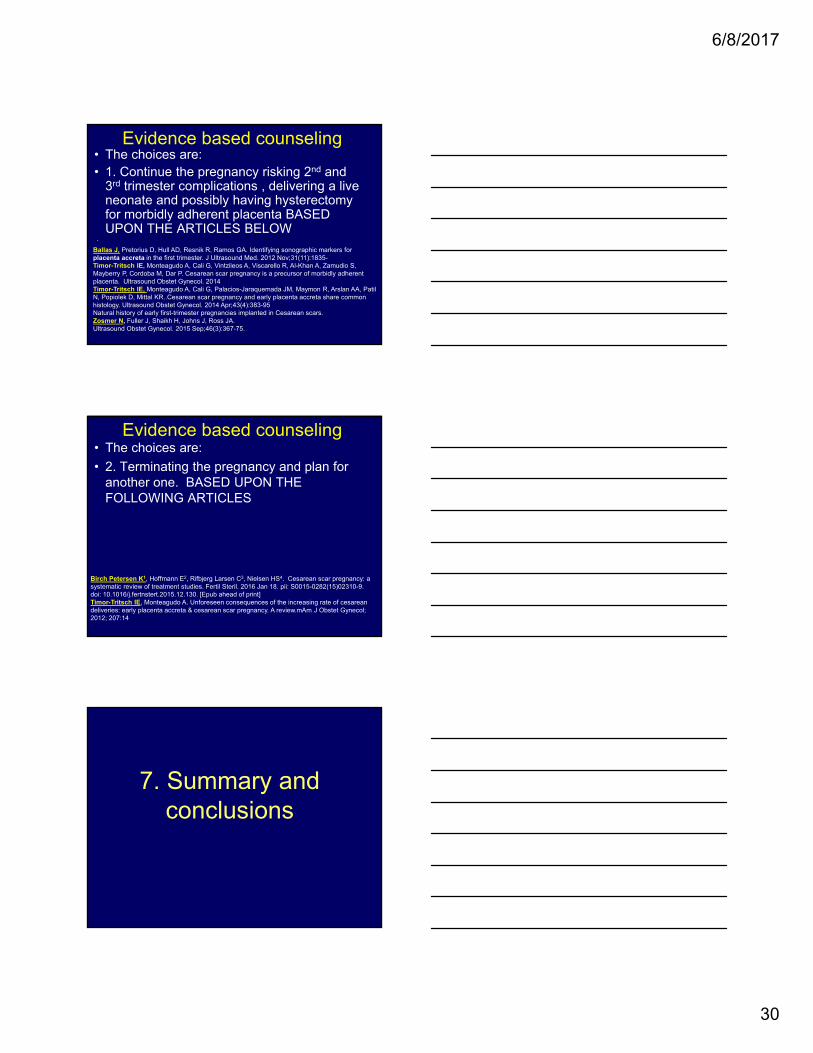
Suggested management of CSPCSP
No FHFH +
Recheck q 3 days
No FH after 3 scans or at 7
wks by reliable dating
Follow hCGuntil zero! Do last US
exam
Select most aproprate Rx.
Stop heart with no or least
delay!
Monitor hCGweekly. Scan by
gray scale & Doppler. Watch
for possible EMV
Determine if placenta/ gestational sac is on the scar
or in the niche. MEASURE MYOMETRIAL THICKESS
Patientrequests
TOP
Patient interested in continuing pregnancy
Available evidence based counseling
“on the scar” or ≥ 5mm: low risk for MAP (accreta) and
cesarean hysterectomy
“in the niche” or ≤ 5mm: high risk for MAP (increta,
percreta) and cesarean
hysterectomy
6/8/2017
30
Evidence based counseling• The choices are:• 1. Continue the pregnancy risking 2nd and
3rd trimester complications , delivering a live neonate and possibly having hysterectomy for morbidly adherent placenta BASED UPON THE ARTICLES BELOW
Ballas J, Pretorius D, Hull AD, Resnik R, Ramos GA. Identifying sonographic markers for placenta accreta in the first trimester. J Ultrasound Med. 2012 Nov;31(11):1835-Timor-Tritsch IE, Monteagudo A, Cali G, Vintzileos A, Viscarello R, Al-Khan A, Zamudio S, Mayberry P, Cordoba M, Dar P. Cesarean scar pregnancy is a precursor of morbidly adherent placenta. Ultrasound Obstet Gynecol. 2014Timor-Tritsch IE, Monteagudo A, Cali G, Palacios-Jaraquemada JM, Maymon R, Arslan AA, PatilN, Popiolek D, Mittal KR..Cesarean scar pregnancy and early placenta accreta share common histology. Ultrasound Obstet Gynecol. 2014 Apr;43(4):383-95Natural history of early first-trimester pregnancies implanted in Cesarean scars.Zosmer N, Fuller J, Shaikh H, Johns J, Ross JA.Ultrasound Obstet Gynecol. 2015 Sep;46(3):367-75.
.
Evidence based counseling• The choices are:
• 2. Terminating the pregnancy and plan for another one. BASED UPON THE FOLLOWING ARTICLES
Birch Petersen K1, Hoffmann E2, Rifbjerg Larsen C3, Nielsen HS4. Cesarean scar pregnancy: a systematic review of treatment studies. Fertil Steril. 2016 Jan 18. pii: S0015-0282(15)02310-9. doi: 10.1016/j.fertnstert.2015.12.130. [Epub ahead of print]Timor-Tritsch IE, Monteagudo A. Unforeseen consequences of the increasing rate of cesarean deliveries: early placenta accreta & cesarean scar pregnancy. A review.mAm J Obstet Gynecol; 2012; 207:14
7. Summary and conclusions
6/8/2017
31
1. Early Dx of CSP is difficult, but possible.
2. Best diagnostic tool for CSP and for MAP (its
vascularity) is TA & TVUS with color Doppler
3. Implantation site (“on the scar or in the niche”) may be important to select to continue or to terminate the pregnancy
4. CSP is a precursor of MAP
5. CSP can result in a live neonate with a high risk of MAP and of hysterectomy
6. All patients with a previous C/S should have a 5-7 week TVUS scan to rule in or out CSP.
Summary: diagnosis/management of CSP
7. MRI does NOT add to the diagnosis .
8. The earlier the diagnosis is established, and treatment is given the faster the resolution
9. Evidence based counseling crucial
10. Systemic MTX: good adjuvant to treatment
11. Placement of a single Foley balloon catheter is useful after local injection
12. Double cervical ripening balloon treatment is minimally invasive and deserves additional evaluation
Last Suggestion:
Early recognition of CSP starts with patient education.
At the time of discharging women from the hospital after a CD, she should be advised
that in case of a future pregnancy, an early visit (1-2 weeks after a missed
period) at the obstetrician for a TVS is of paramount importance.
6/8/2017
32
Is there a “best treatment”?This is what I do:
• Evidence based counseling!!!
• If no heart beats: just watch (hCG, US)
• Heart beasts: Individualize treatment
• If treat: do it promptly! Stop the heart beats!
• If TV US guided TV local MTX sac injection selected use back-up Foley catheter
• Lately: use Double Cervical Ripening Balloon (up to 8w)
• F/U hCG and US until hCG “0” or sharply declining