29
Sponsored by September 24 – 26, 2015 | JW Marriott Miami | Miami, Florida #CHAIR2015
Sponsored by
September 24 – 26, 2015 | JW Marriott Miami | Miami, Florida
#CHAIR2015
W. Vaughn McCall, MD, MS Medical College of Georgia Augusta, GA
Catatonia

W. Vaughn McCall, MD, MS
● Research/Grants: Janssen Pharmaceuticals; Merck Pharmaceuticals; National Institute of Mental Health (NIMH)
● Speakers Bureau: None ● Consultant: Luitpold ● Stockholder: None ● Other Financial Interest: None ● Advisory Board: None ● Editorial Board: Elsevier Publishing (Guest Editor,
Psychiatric Clinics of North America); Wolters Kewer Publishing (Editor, J ECT)
Disclosures
Describe the common signs of catatonia
Learning Objective 1
Describe the diagnostic approach to the patient with catatonia
Learning Objective 2
Describe the management and treatment of the patient with catatonia
Learning Objective 3
Catatonia
● “The patient remains entirely motionless, without speaking, and with a rigid, masklike facies, the eyes focused at a distance; he seems devoid of any will to move or react to any stimuli; there may be fully developed ‘waxen’ flexibility, as in cataleptic states. The general impression conveyed by such patients is one of profound mental anguish.”
Kahlbaum K. Die Katatonie oder das Spannungs-Irresein, 1874.
.

Catatonia
● From the Greek: “low tone” ● A motor syndrome in psychiatric patients ● Catatonic syndrome was seen in 9% of
140 consecutive adult psychiatry admissions – Catatonic syndrome diagnosed when at least
4 of the following were present: – Immobility, staring, mutism, rigidity, withdrawal,
posturing/grimacing, negativism, catalepsy, echo-phenomena, stereotypy, verbigeration
Rosebush PI, et al. J Clin Psychiatry. 1990;51(9):357-62. PMID: 2211547.

Types of Catatonia
● Catatonia, a syndrome ● Malignant/Lethal Catatonia ● Excited catatonia ● Delirious mania (manic delirium) ● Benign Stupor ● Neuroleptic malignant syndrome ● Toxic Serotonin Syndrome
Rosebush PI, et al. J Clin Psychiatry. 1990;51(9):357-62. PMID: 2211547.

Catatonia: History of the Nomenclature -1
● 1874: Kahlbaum defines catatonia ● 1919: Kraepelin includes
catatonia in dementia praecox ● 1921: August Hoch describes
Benign Stupors ● 1952: DSM-II: Schizophrenic
reaction, catatonic type (22.2)
Fink M. Acta Psychiatr Scand. Suppl. 2013;(441):1-4. PMID: 23215963. 17

Catatonia: Nomenclature-1
● 1980: DSM-III : Schizophrenia, catatonic type (295.20) ● 1994: DSM-IV – 295.20 Schizophrenia, catatonic type – 293.89 Catatonic disorder due to [general
medical condition] – Modifier in affective disorders
1. American Psychiatric Association. (1980). Diagnostic and statistical manual of mental
disorders. (3rd ed., text rev.). Washington, DC. 2. American Psychiatric Association. (2000). Diagnostic and statistical manual of mental
disorders (4th ed., text rev.). Washington, DC.
Catatonia Nomenclature DSM-V ● Associated with Another Mental Disorder; Due to Another
Medical Condition ● “The clinical picture is dominated by > 3 of the following
symptoms” – Stupor (no psychomotor activity, not actively relating to
environment – Catalepsy (passive induction of a posture held against gravity – Waxy Flexibility (slight, even resistance to the examiner – Mutism – Negativism (opposition… to instructions) – Posturing (spontaneous maintenance of posture against gravity)
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders. (5th ed., text rev.). Washington, DC.

Catatonia Nomenclature DSM-V
● Associated with Another Mental Disorder; Due to Another Medical Condition
● “The clinical picture is dominated by > 3 of the following symptoms” – Mannerism (odd…caricature of normal actions) – Stereotypy (repetitive…frequent, non-goal-directed
movements) – Agitation – Grimacing – Echolalia (mimicking another’s speech) – Echopraxia (mimicking another’s movements)
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders. (5th ed., text rev.). Washington, DC.

The Grey Zone Between Severe Mood Disorder and Catatonia ● Catatonic stupor – When does psychomotor retardation become
‘stupor’? – When does ‘speech latency’ become ‘mutism’?
● Catatonic excitement – When does psychomotor acceleration become
‘catatonic excitement’? – When does pressured speech with flight of
ideas become ‘verbigeration’?
Catatonia-Manifestation of Mood Disorders
● Catatonia known to more often be a manifestation of mood disorders (48%), rather than schizophrenia (12%) ● 10% of cases are ‘organic’
Rosebush PI, et al. J Clin Psychiatry. 1990;51(9):357-62 .PMID: 2211547.
Catatonia Due to Organic Medical Condition
● Systemic diseases ● Toxic syndromes – Serotonin syndrome – Neuroleptic malignant syndrome
● Neurologic disorders – Intracranial mass – CNS lupus – Non-convulsive status epilepticus – John Cunningham (JC) Disease – Viral Encephalitis
Brasic R. Catatonia. Medscape Website. http://emedicine.medscape.com/article/115485overview#a5. Updated July 9, 2015. Accessed September 15, 2015
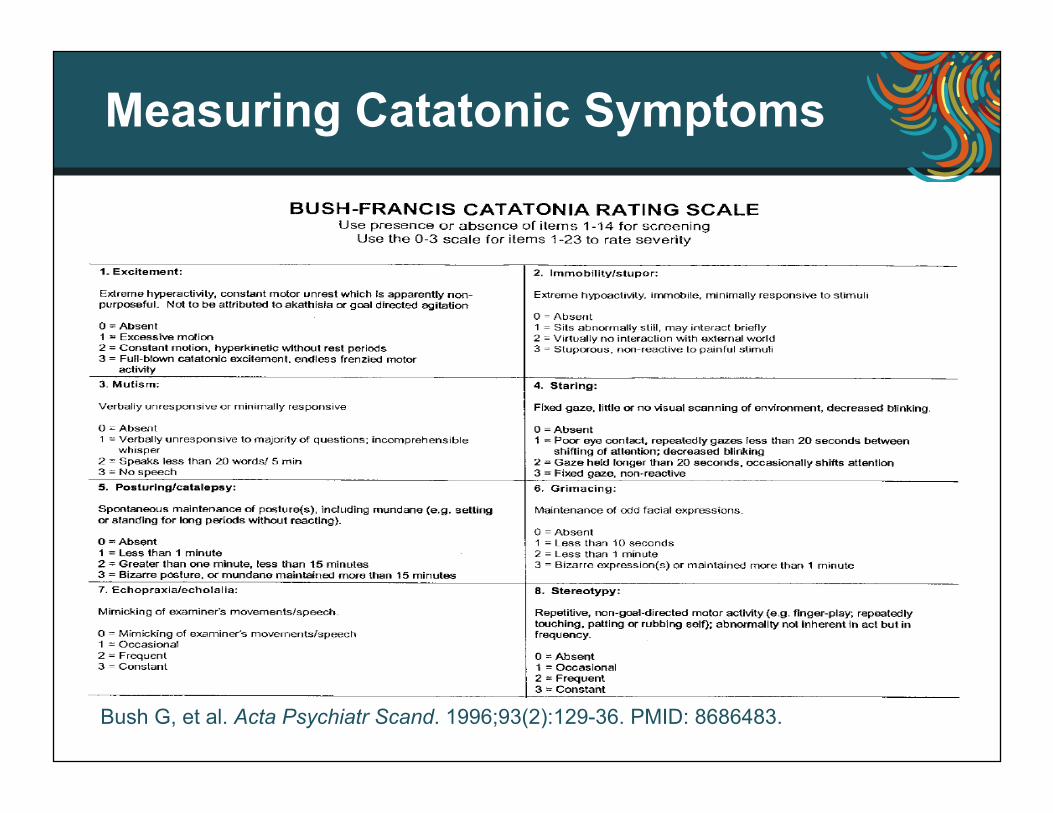
Measuring Catatonic Symptoms
Bush G, et al. Acta Psychiatr Scand. 1996;93(2):129-36. PMID: 8686483.

Catatonia: Primary Signs
● Mutism (85%)
● Immobility / Stupor (100%)
● Staring (92%)
● Posturing/Grimacing (73%)
● Withdrawal/Refusing to eat (78%)
● Rigidity (66%)
Percentage of Patients with Sign
.

What is the Physiologic Setting for Primary Catatonic Stupor? ● EEG: Highly variable with patients showing
slowing, or reduced alpha, or bilateral beta, or flat tracings – EEG not helpful unless it shows classic
pathology like epileptiform discharges1
● SPECT: Regional decreases in brain perfusion, improved with ECT
1. Fink M and Taylor MA. Catatonia. Cambridge University Press, Cambridge 2003. 2. Galynker II, et al. J Nucl Med. 1997 ;38(2):251-4. PMID: 9025749. 3. Atre-Vaidya N. Neuropsychol Behav Neurol. 2000 ;13(2):136-9. PMID: 10780632. 4. Northoff G, et al. Psychol Med. 2000;30(3):583-96. PMID: 10883714. 5. Escobar R, et al. J Psychosom Res. 2000;49(6):423-9. PMID: 11182435.

Complications of Catatonic Stupor
● Aspiration pneumonia ● Inanition ● Contractures ● Decubiti ● Deep vein thrombosis ● Pulmonary embolism ● Death McCall WV, et al. J Clin Psychiatry. 1995;56:21-25. PMID: 7836335.
Treatment of Catatonia with Sedatives
● Barbiturates: Amobarbital IV, 500mg/10ml;1 ml/40 seconds to relief or sleep ● Benzodiazepines: Lorazepam – IV, 1mg/2 min to relief or sleep – Oral, 4mg-16 mg/day
● 12 of 15 episodes responded to oral lorazepam
Rosebush PI, et al. J Clin Psychiatry. 1990;51(9):357-62. PMID:2211547.

Treatment of Catatonia with Sedatives
● In a cross-over design, 20 adults with catatonic mutism were assigned 1:1 to first receive i.v. 5% amobarbital (up to 500 mg) versus saline over 10 minutes, then crossed over to the other condition
● 6/10 responded to amobarbital and none to saline (p < 0.005)
● In the cross-over, 4 who had failed saline responded to amobarbital (none who failed amobarbital responded to saline)
● All in all, 10 or 20 responded to amobarbital, and none to saline
McCall WV, et al. Am J Psychiatry 1992;149:202-206. PMID: 1734740.
ECT for Catatonia
● ECT is the definitive treatment, with short-term remission rates of 80%1
● Failure to respond to a sedative does not necessarily mean no response to ECT 2
● Bilateral electrode placement best studied, but case series of RUL in press looks to be effective
● Consider Initial daily treatment x 3 (“en bloc”) ● Sustained by standard ECT regimen ● Catatonia relieved within 2-4 ECT ● May need IM ketamine anesthesia initially if it is
excited catatonia 1. Rey JM, Walter G. Am J Psychiatry. 1997;154(5):595-602. 2. McCall WV. Convulsive Therapy.1992;8(3):174-178.

Catatonia: Treatment Caution
Caution! ● Neuroleptics are risky- may precipitate
neuroleptic malignant syndrome
Van Den Eede F, et al. Eur Psychiatry. 2005;20(5-6):422-9. PMID: 15964746.

Assessment of the Patient with Catatonic Stupor
● Routine psychiatric history and physical ● Catatonic signs checklist or rating scale ● No prior psychiatric history? – Consider anatomic imaging, EEG, LP
● Prior psychiatric history? – Probably can omit neurodiagnostics
● Prior response to ECT? ● Prior history of complications such as DVT? Brasic R. Catatonia. Medscape Website. http://emedicine.medscape.com/article/115485 overview#a5. Updated July 9, 2015. Accessed September 15, 2015.
Management of the Patient with Catatonic Stupor
● Support for intravascular volume and nutrition ● Measure urinary input and output: do not allow
urinary retention ● Assure some mobility or ambulation with nursing
or physical therapy if necessary ● Assess need for compression stockings ● Assess need for subcutaneous heparin ● Consider IV/IM/PO lorazepam – Take care not to cause respiratory suppression
Luchini F, et al. World J Psychiatry. 2015;5(2):182-92. PMID: 26110120.

Management of the Patient with Catatonic Stupor
● Move quickly to make preparations for ECT, whether you think you will need it or not
● How will you get consent? – Advanced directives, next of kin, guardianship, court-
ordered ● If no sustained improvement with (high dose)
lorazepam, or if catatonia has been continuing for more than a few days, then start ECT
● Pick an ECT technique likely to produce quick results: bilateral, high dose, daily sessions
● Cognition is a less important concern Luchini F, et al. World J Psychiatry. 2015;5(2):182-92. PMID: 26110120.

Clinical Connections
● Catatonia is among the most dramatic, the most life-threatening, and most treatment responsive conditions in psychiatry
● Mild forms (‘catatonic features’) are more common than we think
● Understanding of catatonia is hampered by lack of capacity of persons with catatonia
● Is the grimacing, mutism, and stereotypy seen in pervasive developmental delay a form of catatonia? Would it respond to ECT?
Questions & Answers

















