47
Chagas Disease: Clues to the Magnitude of the Problem in Texas “EJ” Hanford, ABD Dr. F. Ben Zhan Dr. Yongmei Lu Dr. Alberto Giordano
| Date post: | 25-Dec-2015 |
| Category: |
Documents |
| Upload: | erika-hunter |
| View: | 214 times |
| Download: | 0 times |

Chagas Disease:Clues to the Magnitude of
the Problem in Texas
“EJ” Hanford, ABD
Dr. F. Ben Zhan
Dr. Yongmei Lu
Dr. Alberto Giordano

Research Support & Funding
Texas State UniversityCenter for Geographic Information Science
Border Health Initiative Project
Effort sponsored in part by the
311th Human Systems Wing
PIA FA8909-04-3-5000
Brooks City-Base Foundation, Inc.

New World Disease Dr. Joseph Reinhardt Cooper
• 1850s – Brazil "mal de engasgo"
• Clinical presentation, natural history & epidemiology first written
record
Historical Timeline
1909 Dr. Carlos Chagas
1936 Southern Mexico – first recognized
case
1955 First indigenous cases in U.S. = 2 in Texas
1970s Central Mexico
2006 1st FDA approved blood-screening test
Dr. Carlos Chagas

Protozoan Agent
Trypanosoma cruzi
Life Cycle
Diagnostic Techniques
• Clinical Evaluations & …
• Demonstration of Parasite– Direct microscopic examination– Xenodiagnosis– Lab animal inoculation– Hemoculture (less sensitive)– PCR
• Serologic Testing– CF, IH, DA, IIF– ELISA (Cross reactions can occur to Leishmaniasis,
Blastomycosis, and Toxoplasmosis)
• Fecal contamination • enters Triatomid bite • through mucosal tissue (eye)• through open wound• within consumed food or water
• Blood transfusion from infected person• Organ donation from infected person• Vertical transmission (Congenital multigen.) • Laboratory-acquired• (?) Oral transmission• Other ?
Transmission to Humans
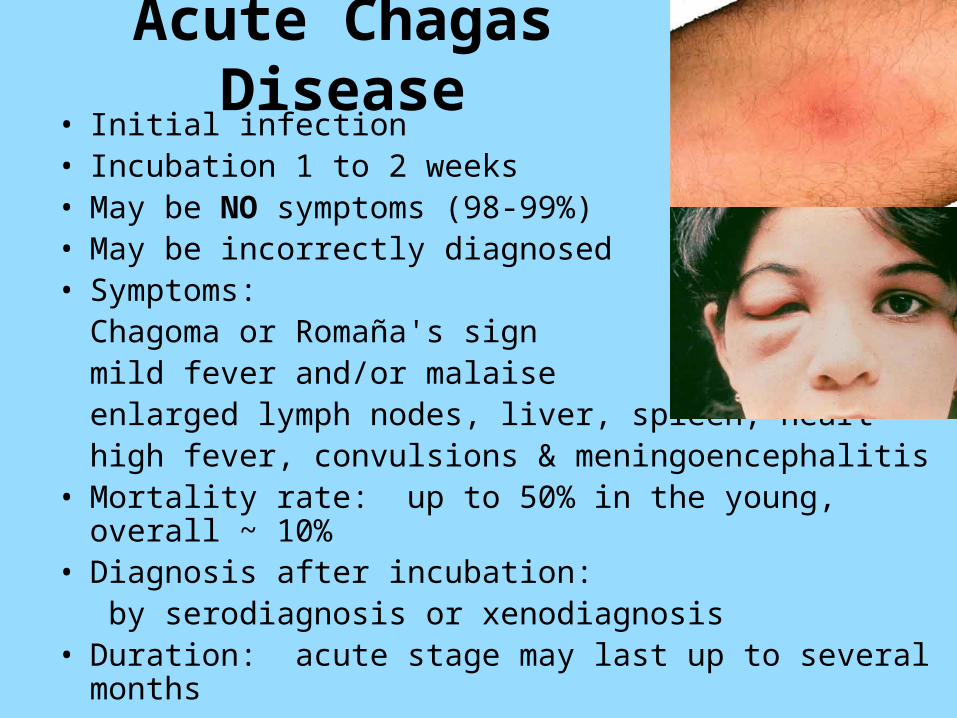
Acute Chagas Disease• Initial infection • Incubation 1 to 2 weeks• May be NO symptoms (98-99%)• May be incorrectly diagnosed• Symptoms:
Chagoma or Romaña's signmild fever and/or malaiseenlarged lymph nodes, liver, spleen, hearthigh fever, convulsions & meningoencephalitis
• Mortality rate: up to 50% in the young, overall ~ 10%• Diagnosis after incubation:
by serodiagnosis or xenodiagnosis• Duration: acute stage may last up to several months

Latent Stage Chagas Disease• Outwardly asymptomatic
• May have subtle changes in – sympathetic & parasympathetic nervous system – internal organs
• Duration: decades till death from other cause or
till evolution to chronic stage
• Diagnosis by serological testing(15% prevalence DNA in sero-neg endemic pop.)

Chronic Chagas Disease• Evolves in 20 to 40 % of infected persons
– Repeated re-infections– Genetic polymorphism of T. cruzi– Variation in host susceptibility– Immuno-compromised by disease / drugs
• Cardiomyopathy or Congestive Heart Failure– typically involves right bundle branch block– arrhythmias
• Enlarged colon or esophagus • Ischemic stroke• Diagnosis by serological testing & clinical evaluation
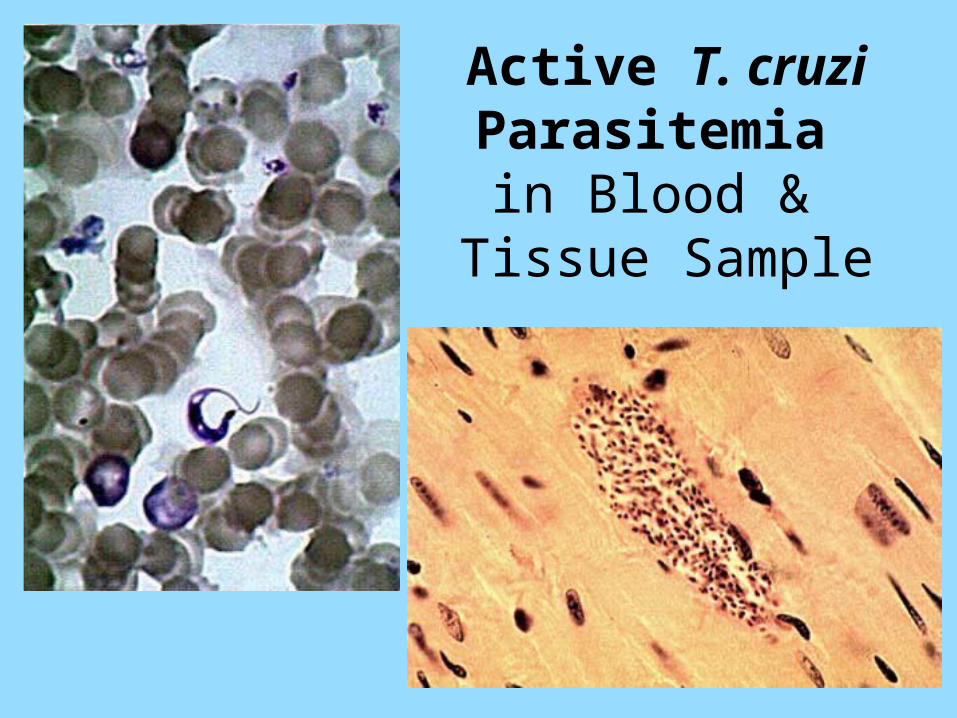
Active T. cruzi Parasitemia in Blood &
Tissue Sample
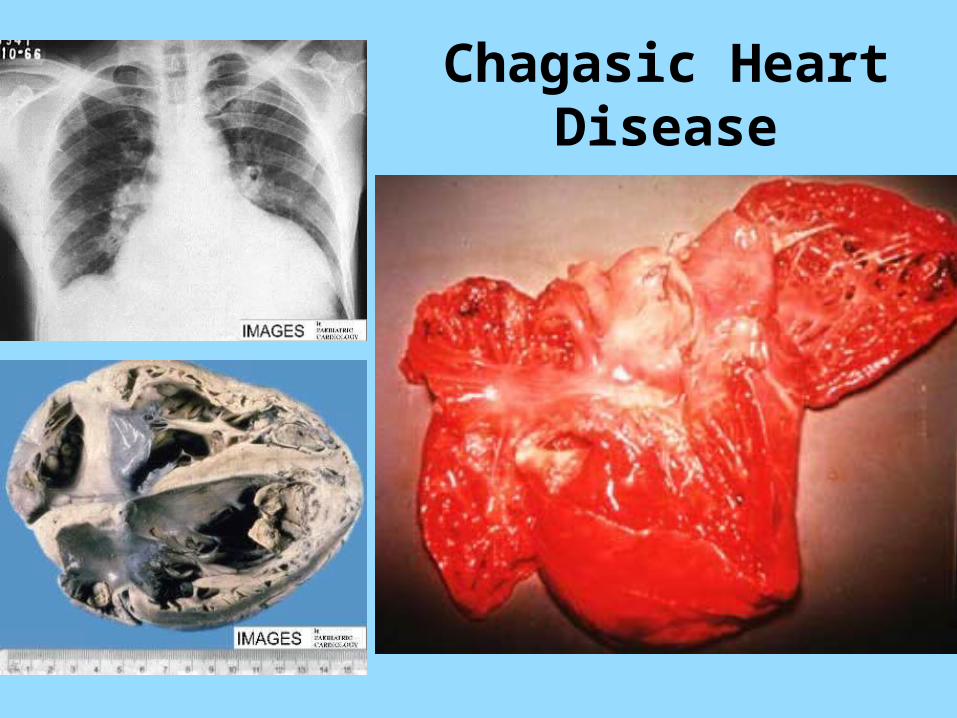
Chagasic Heart Disease

Megacolon

Vinchuca … Kissing bug…Cone-nose….by any other name…
Triatomid species
1 cm
1 inch
Eggs
In-star nymph stages
Adult (winged)
Disease Vectors:
Nymphs & Adults
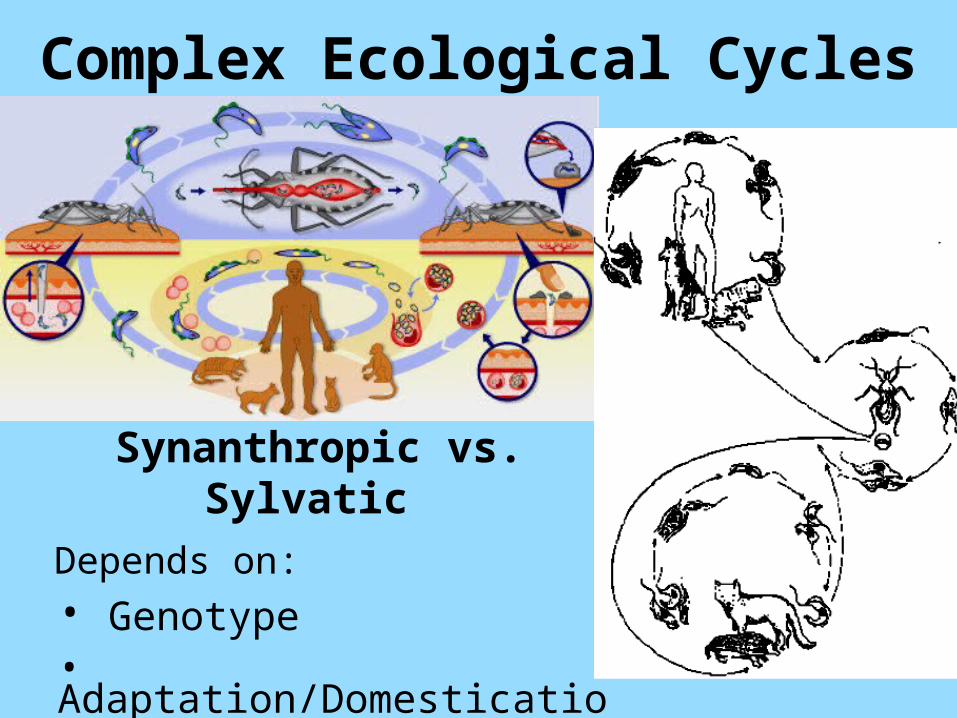
Complex Ecological Cycles
Synanthropic vs. Sylvatic
Depends on:
• Genotype• Adaptation/Domestication• Other factors ?
Chagas Disease in Humans• Become infected for life
• Potentially progresses through 3 stagesAcute Latent/Indeterminate Chronic
• Fatal in acute and/or chronic stages & debilitating
• Higher risk for immuno-compromised persons
• MYTH = a disease only of the rural poor
• NO vaccine
• NO cure
• US FDA approved ELISA blood-screening test

But NOT in Texas ??
• Lower virulence
• Lower vector density
• Different vector habits – Less frequent domestication– Significantly longer feed-defecation response
• Lack of ‘trypanosomiasis consciousness’– Fail to diagnose nondescript acute infections

Packchanian 1939• Oct ’37 & Sept ’38
• 500 persons bitten
• Found by personal inquiries
Packchanian 1940• 50 infected Triatoma
in TempleLocations:• Austin, Dallas, Galveston, Houston, San Antonio
• Bell, DeWitt, Duval, Live Oak & Jim Wells Co.

Wood 1941 & 1942• Bug ‘epidemic’ in
Quemado Valley• Residents bitten• House infested in
Sanderson (Terrell)“these suckers have sure dealt them misery”
Locations:• Maverick, Terrell & Bandera Co.

Davis & Sullivan 1946• 8-yr old male in Blewett
tested positive
• Compliment Fixation in significant dilution
• T. gerstaeckeri in home
Location:• Uvalde Co.

1st Indigenous CaseWoody & Woody 1955• 10-mo. old white
female born Oct 5, 1954 in Corpus Christi
• Parasites in blood
• Triatomids in home
• Father bitten
Location:• Nueces Co.
Shields & Walsh 1956• 45 persons bitten over
prior 2 years
• Lesions by bite of
T. sanguisuga
• “from all parts of the city, from all types of dwellings, and from all economic levels”Location:
• Fort Worth, Tarrant Co.

2nd Indigenous CaseTDH 1955• 6-mo. old male born
June 16 in Bryan• November: hospitalized
obstructive hydrocephalus
• Hospitalizations for Salmonella enteritis & meningitis
Yaeger 1961• Pediatrician: ? case of
transmission by transfusion
Location:• Brazos Co.

Lathrop & Ominsky ‘65• 63-yr old male
• Compliment Fixation & Hemagglutination
• 48 (of 108) children & adults bitten
• Rural area 20 miles NE of San Antonio: Shertz & Randolph AFB
Location:• Bexar Co.

Woody et al. 1965• 117 bitten in Coastal
Bend & Corpus Christi• 7 weakly positive to
positive titers (ages 5.5 – 72) but no clinical evidence
• 2 infection chagomas (no positive test)
• T. cruzi not isolated• 1st indigenous case still
tested positiveLocation:• Nueces Co.

Faust 1978• 38-yr old male fatality• Oct ’76 vacation in
Caracas, Venezuela & Caribbean
• 2 Amarillo Hospitals:1st Admit = May 11-13, ’77 2nd Admit = May 26-July 1x-ray: cardiomegaly, ECG poor L ventricle function Diagnosis: cardiomyopathy, origin undetermined
• Died at home, July 5• CF & HA tests confirmed
on July 25, 1977
Location:• Potter Co.

Burkholder et al. 1980• 12 of 500 long-term
residents positive titers
• 1 being treated for unexplained myocardial disease & enlarged heart
Locations:• Cameron & Hidalgo Co.

Betz 1984• 7-mo old Hispanic male
fatality July 30, 1983• April 1984 pathology
diagnosis: acute Chagas myocarditis
• Likely infected Mathis (SP) or Alice (JW)
• Family all seronegative in 1984
3rd Indigenous Case
Locations:• San Patricio or Jim Wells Co.
Infection Attributed to Transfusion
Cimo et al. 1993• 59-yr old female fatality
• Acute Chagas
• T. cruzi in peripheral blood & bone marrow
• >500 units transfusion – not identified among 40 Hispanic surnamed donors testedLocation:
• Houston, Harris Co.

Cross-Section Study in HoustonDiPentima et al. 1999• Pregnant women (’93-’96)
ages 13 - 44 • 2107 Hispanic, 1658 non• 22 positive (18 >age 20)
13 (0.6%) Hispanic &
9 (0.5%) White & Black• Risk factors & points of
exposure unknown• Congenital not reported
Location:• Harris Co.

Serologic Tests & Look-back
Leiby et al. 1999• 3 EIA repeatably
reactive and RIPA seropositive – all from Waco
• 1 from Durango MX
• 2 TX natives (17 & 40)
• All 3 families: history of heart ailments & complications (enlarged heart & arrhythmias)
Location:• McClennan Co.

Cardiac Surgery PatientsLeiby et al. 2000• 23 repeatably reactive
6 confirmed at 3 hospitals, including:Methodist Hospital & St. Luke’s Episcopal in Houston
• Original source of infection unknown; all had received blood transfusions
Location:• Harris Co.
ElMunzer et al. 2004
• 70-yr old Hispanic male• Immigrated to TX 20 yrs• Oct 2002 presented to
ER Parkland Memorial• History of acute MI, with
right bundle branch block on ECG, ventricular arrythmia
• Diagnosis confirmed by Complement Fixation
Location:• Dallas Co.

T. Cruzi Reactivation by AIDSRivera et al. 2004• 29-yr old male Honduran
fatality• 5-yr Immigrant was
diagnosed 5-mo. with HIV • Developed acute
congestive heart failure secondary to cardiac Chagas Disease
• Necropsy showed T.cruzi amastigotes in myocardium – no atherosclerosis
Location:• Dallas Co.

Hosts & Reservoirs in TX Woodrats (Neotoma)
Opossums (Didelphis)
Armadillos (Dasypus)
Coyotes (Canis)
Others (+ humans)
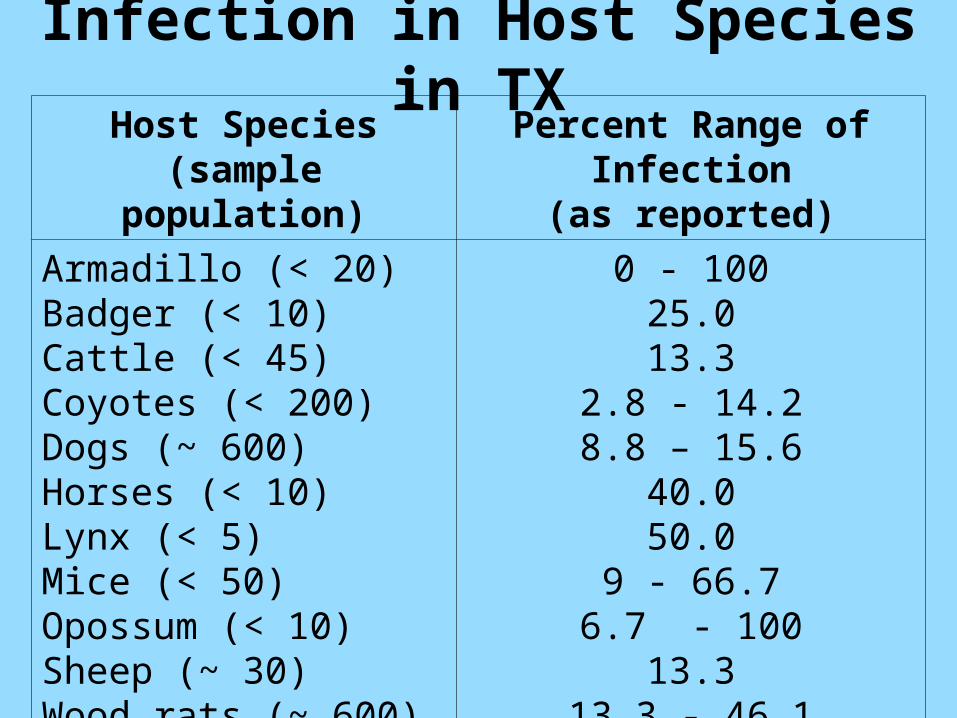
Host Species(sample population)
Percent Range of Infection(as reported)
Armadillo (< 20)Badger (< 10)Cattle (< 45)Coyotes (< 200)Dogs (~ 600)Horses (< 10)Lynx (< 5)Mice (< 50)Opossum (< 10)Sheep (~ 30)Wood rats (~ 600)
0 - 10025.013.3
2.8 - 14.28.8 – 15.6
40.050.0
9 - 66.76.7 - 100
13.313.3 - 46.1
Infection in Host Species in TX

Human Reservoirs
• Canada (1%) • Berlin, Germany (2%)• Spain, Romania, Japan …

Chagas Disease in the U.S.
• Blood Transfusion
Immuno-compromised individuals
? Immuno-competent
• Organ Transplants
2002 = 3 from 1 donor
2006 = 2 cases, 6 monitor from 2 donors
• 6 Autochthonous cases: TX, CA, TN, LA
• Unrecognized ????
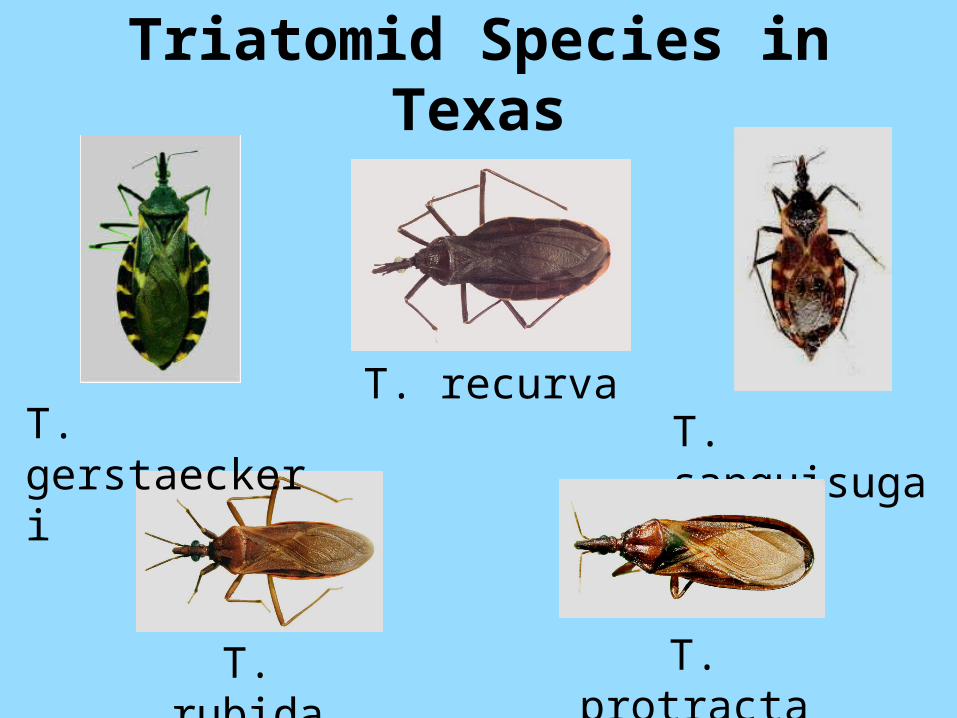
Triatomid Species in Texas
T. gerstaeckeri
T. recurva
T. rubida
T. sanguisuga
T. protracta

Historical Biogeographical
Analysis77 Counties with Triatomids
64 Counties with infected vectors/hosts

Documented Reports in Humans
Bitten: 1200+
Seropositive/ diagnosed cases = 55

Demographics & Estimates
• Latin America: DALY 2.7m ~ U.S.$6.5b
United States:
16 m (incl 6.2 undoc) Latin Am immigrants
~ 7% infection rate
1m + infected
150,000+ chronicTEXAS:
~ 300,000 - 600,000 infected
~ 50,000 - 100,000 chronic
Under-Estimation ??
Actual infection rate
Number of undocumented immigrants
Number of congenital cases
Multi-generational transmission
Infected immuno-competent Sero-negative but still infected More aggressive genotype

Significance = Emerging Disease
More is needed in Texas:
• Education & Prevention
• Research & Development
• Awareness / Recognition
And in other states
• Endemic regions
• Introduced

• Improved understanding of environmental ecology of vectors & hosts (adaptability)
• Field studies to determine infection rates and ranges of endemic vector and host species
• Field studies to monitor introduced/migrating vectors and hosts & interactions with native species
• FDA-approved tests for diagnosis & screening of blood supply & donor organs
• Preventative vaccine• Pharmaceuticals to control disease progression
or to produce a “cure”
Research & Development

Recognition as– endemic zoonotic risk for humans
– introduced disease associated with changing human demographics & genotypes
Education Prevention & Awareness– public health, physicians & cardiologists– veterinary & animal care workers
Recommendations – Inclusion as Communicable / Reportable to TDSHS
– Serologic screening test
What is needed…


















