Challenges faced during the Development of new high demand Public Hospitals - with limited Budgets, Land and Time Constraints in the City of Kampala, Uganda by D. Abola, P. Kaliba, R. Sengonzi, S. S. B. Wanda and C.I. Meirovich SAFHE/CEASA 2015 – Johannesburg, South Africa 11-13 th August 2015 1
Transcript
Challenges faced during the Development of new high demand Public Hospitals - with
limited Budgets, Land and Time Constraints in the City of Kampala, Uganda
by
D. Abola, P. Kaliba, R. Sengonzi, S. S. B. Wanda and C.I. Meirovich
SAFHE/CEASA 2015 – Johannesburg, South Africa
11-13th August 2015
1
Presentation Outline
Introduction and Background Project Rationale Health services delivery in Uganda and
Kampala City Project Challenges Project Management Solutions Conclusion and Recommendations
2
Introduction and Background … 1
Uganda: East Africa and bordered by Kenya, Southern Sudan, DRC, Rwanda and
Tanzania. Coverage : 241,038 km2
Population: 34.1 million
Kampala, the Capital City of Uganda
Coverage: 189 km2
Day Population: approx. 4 million Resident Population: approx. 1.79
million
3
Introduction and Background…2
Project Name: Improvement of Health Service Delivery in Mulago Hospital and in the City of Kampala Project (MKCCAP).
Project Funded by: African Development Fund (ADF) and the Nigerian Trust Fund (NTF)
Project coverage: Mulago NRH and Kampala Metropolitan Area
Project Period: July 2012 – 31 December 2016
Project costs : Total Cost: $85 m
Executing Agency: Ministry of Health 4
5
Project Rationale
Improve delivery of quality health services in Mulago Hospital & the City of Kampala
Increase access to quality and affordable healthcare services for the population of Kampala Metropolitan area
Decongest Mulago Hospital by improving services at the Division levels and redirecting high demand for basic health care
Health Service Delivery in Uganda and Kampala City…1
An estimated 24.5% of the population lives below the poverty line: 34.2% from rural areas; and 13.7% from urban areas
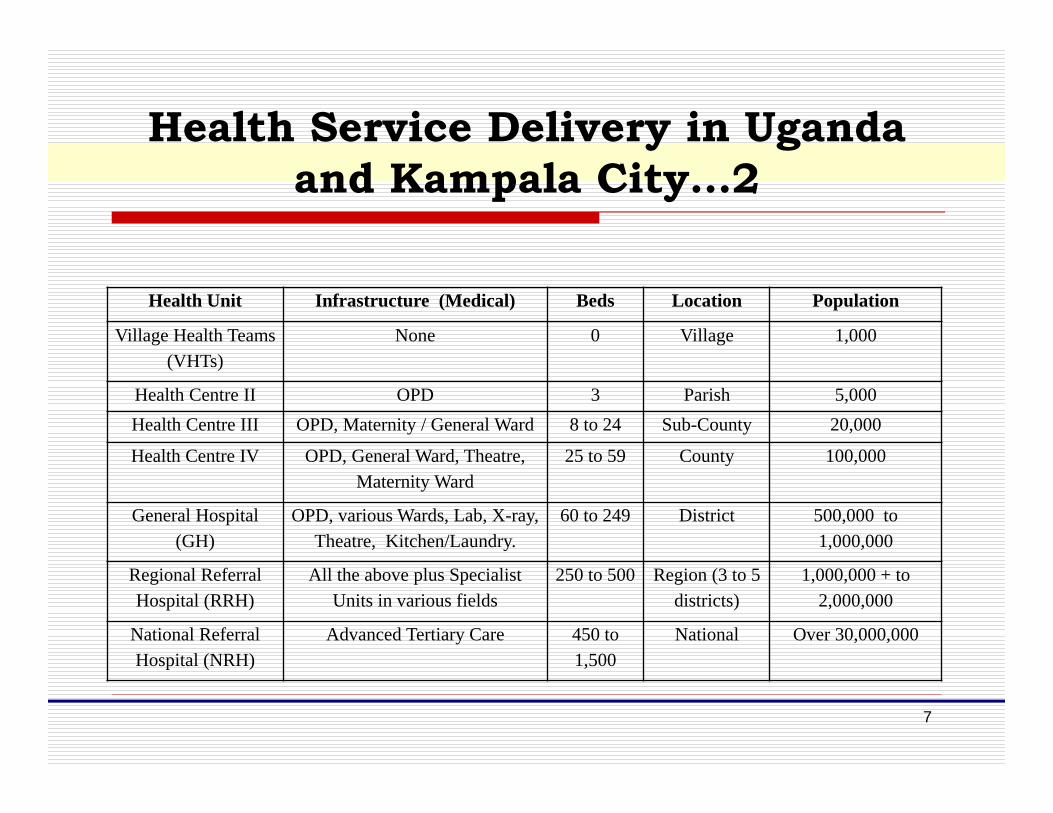
Health service provided through a tiered structure: Village Health Teams (VHTs) at village level to National Referral Hospital Level as per Table overleaf.
6
Health Service Delivery in Uganda and Kampala City…2
Health Unit Infrastructure (Medical) Beds Location Population
Village Health Teams (VHTs)
None 0 Village 1,000
Health Centre II OPD 3 Parish 5,000Health Centre III OPD, Maternity / General Ward 8 to 24 Sub-County 20,000
Health Centre IV OPD, General Ward, Theatre, Maternity Ward
25 to 59 County 100,000
General Hospital (GH)
OPD, various Wards, Lab, X-ray, Theatre, Kitchen/Laundry.
60 to 249 District 500,000 to 1,000,000
Regional Referral Hospital (RRH)
All the above plus Specialist Units in various fields
250 to 500 Region (3 to 5 districts)
1,000,000 + to 2,000,000
National Referral Hospital (NRH)
Advanced Tertiary Care 450 to 1,500
National Over 30,000,000
7
Health Service Delivery in Uganda and Kampala City…3
Government Hospitals in Uganda
8
Category Hospital Name
National Referral and Teaching
Hospitals (4No.)
Mulago (including the Heart and Cancer Institutes), Butabika, Guluand Mbarara
Regional Referral Hospitals (12 No.) Arua, Hoima, Jinja, Kabale, Fort Portal, Masaka, Mbale, Lira, Soroti,Naguru, Mubende and Moroto.
Health Service Delivery in Uganda and Kampala City…4
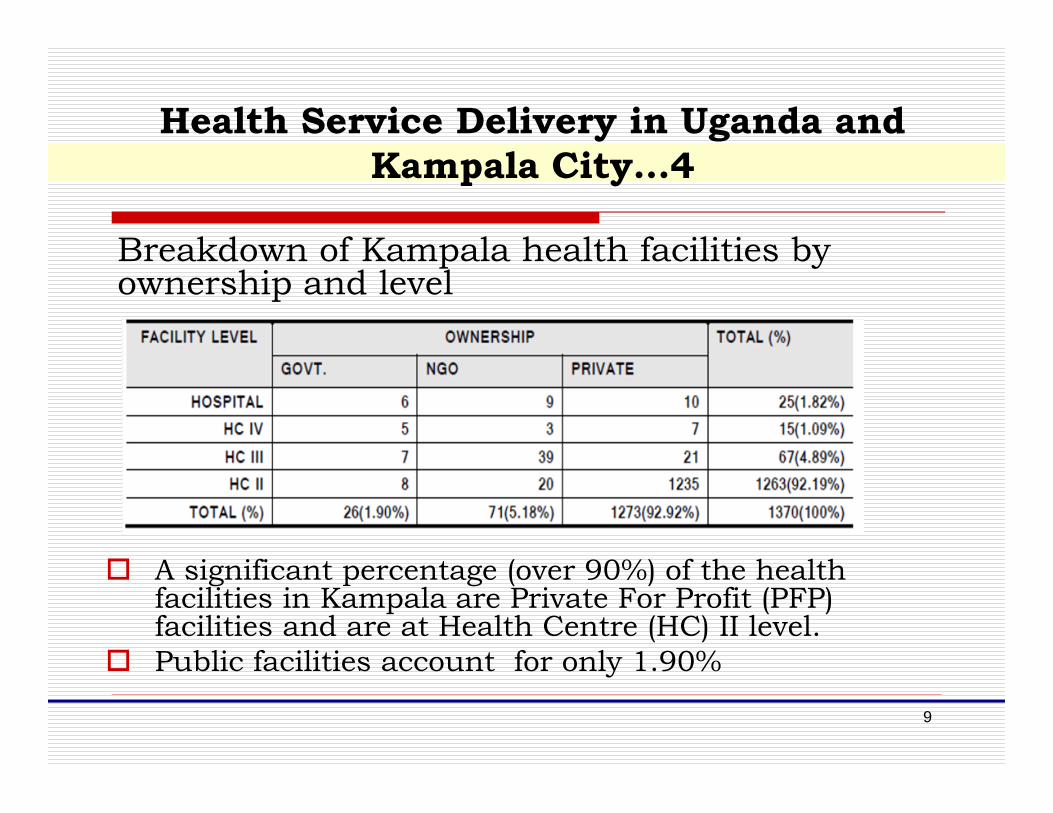
Breakdown of Kampala health facilities by ownership and level
A significant percentage (over 90%) of the health facilities in Kampala are Private For Profit (PFP) facilities and are at Health Centre (HC) II level.
Public facilities account for only 1.90%
9
Project Challenges …1
Competing needs for effective delivery of essential healthcare services Lack of other public providers implies: Mulago Hospital is usually
diverted from its core mandate of providing national referral services to cater for the lower level health service provision.
Lack of adequate infrastructure and logistics for provision of equitable health services especially for the urban poor About 15% of all pregnancies develop life threatening
complications and require emergency obstetric care (EmOC); and, Only 11.7% of women deliver in fully functional comprehensive
EmOC facilities the slow progress in addressing maternal health problems in
Uganda is partly due to lack of appropriate buildings and equipment (Health Sector Strategic Plan (HSSP III)
10
Project Challenges … 2
Challenge: ensure a network of functional, efficient and sustainable health infrastructure for effective health services delivery closer to the population especially for the urban poor who cannot afford to pay for services in the predominantly for-profit healthcare industry in the City.
Budgetary Constraints: At project appraisal, construction and equipping the three
hospitals was estimated to cost USD 75Million The 2 new hospitals are expected to provide various services at
the Regional Referral Hospital level Challenge: Budgetary constraints arising from having to
establish the 2 new hospitals and fully renovating the national referral hospital, as well as fully equipping all three, within the budgeted 75Million UD Dollars.
11
Project Challenges … 3
Outdated project estimates: Project appraisal carried out in 2009 Actual project implementation did not take place until
October 2012 Challenge: Estimates prepared at inception of the
project rendered outdated because of the long passage of time between project appraisal and project implementation stage
Project implementation team has to constantly keep adjusting the original scope at the same time having to strike a balance with the expected project outcomes
12
Project Challenges … 4
Late recruitment of the Biomedical Engineer: Plan at appraisal stage of this project: few key
technical staff would be initially recruited to supervise day-to-day project activities
long-term technical staff recruited at the time included: the project health architect, the project engineer,
the project quantity surveyor, the procurement officer, the financial specialist and his assistant
The biomedical engineer came on board much later on: hospitals’ designs had already been reviewed and construction of the structural frame and walling in advanced stages
13
Project Challenges … 5
The Biomedical engineer found several design flaws that could affect the optimal functionality of the hospitals and equipment and advised on remedial design changes: which involved demolition of walls and electro-
mechanical works re-alignment These changes further stretched an already
constrained budget and caused delays due to rework
Suggested increasing the equipment budget from under USD 2 m to USD 4 m
14
The Solutions
Same service design, 2 different sites Ten-storey main hospital building on a compact site
15
The Solutions…….2
Compromising with space standards In order to meet the high demand for lower level
services, project to provide various clinical services (i.e. A&E; pathology; OPD with services including dental, Eye/ENT, orthopaedics, antenatal, paediatrics; imaging diagnostics & laboratories; 5 operating theatres and inpatient services) on existing land of less than 2 acres
Each hospital – also designed for 173 beds housed in a ten (10) storey building
Total area for different clinical, clinical support, non-clinical support and administrative services: estimated at 7,800 m2.
16
The Solutions ……3
Compromising with space standards Total space per bed = up to 76 sq m Used to be considered adequate in the 1980s Now considered low for achieving and compliance
with a number of international standards Ratios above 100 would be more appropriate but
would lead to:- a reduction in the number of beds per room/bay and
consequently 150 beds However, due to space constraints, having to deliver
the project objective of decongesting the National Referral Hospital less beds not an option.
17
The Solutions….4
Stakeholder Involvement
At the onset of the project’s implementation, architectural and structural designs had already been prepared
Due to passage of time: key stakeholders had changed; new information available; and, Original budgets no longer sufficient Designs had to be reviewed and modified by
another consultant
18
The Solutions….5
It was deemed critically important to involve key project stakeholders in the design review These stakeholders were be part of the
problem-solving Stakeholder buy-in was considered
critical to the success of the constrained project
19
The Solutions….6
Stakeholders have since been involved in the project’s implementation: at design review stage; at evaluation stage for both supervision
consultants and building contractors; as well as, the construction stage - active role
in decision making and attending the monthly site meeting
20
The Solutions……7
Re-programming project funds In order to overcome budgetary deficits
brought about by: Under funding of medical equipment allocations Price fluctuations arising from passage of time between appraisal
stage and actual implementation (2009 v. 2013), as well as, fluctuating dollar rates
The project has had to re-programme funds that were previously allocated to activities that are no longer considered a priority in order to the complete construction and equipping.
e.g. The two hospitals originally allocated less than USD 2 million for medical equipment and furniture have sourced the shortfall be sought from other planned but non-priority project activities.
21
Conclusions
The construction of the 2 new hospitals is in advanced stages, at about 65% progress and with a scheduled completion date of 31st
December 2015. Equipment tenders advertised and hopefully the hospitals to be occupied by end of January 2016
It is hoped that service delivery will be as planned to achieve project objective
22
Recommendations
Phasing of works in case of inadequate budgets to avoid stretching expectations
Assembling full technical teams early on in the project to avoid project delays and rework arising from late technical advice
Provision of contingency funds as part of the project appraisal – safety net to cover unforeseen eventualities
Early engagement of key stakeholders to enable effective management of expectations and increasing satisfaction with end product.





















![GW 1# ;] - Kampala](https://static.documents.pub/doc/80x56/620e40353090141c8a298df6/gw-1-kampala.jpg)















