Challenges in Establishing a Neonatal AKI Definition & Long Term Outcomes Cherry Mammen MD, FRCPC, MHSc Pediatric Nephrologist, BC Children’s Hospital Clinical Assistant Professor University of British Columbia Vancouver, BC, Canada Neonatal AKI Symposium Cleveland, Ohio October 7 th , 2017
Transcript
Challenges in Establishing a Neonatal AKI Definition &
Long Term OutcomesCherry Mammen MD, FRCPC, MHSc
Pediatric Nephrologist, BC Children’s HospitalClinical Assistant Professor
University of British ColumbiaVancouver, BC, Canada
Neonatal AKI SymposiumCleveland, Ohio
October 7th, 2017
No Disclosures or Conflicts of Interest
Objectives
• To describe a recently proposed standardized & staged neonatal AKI definition (modified KDIGO definition)
• To review challenges in defining neonatal acute kidney injury (AKI)
• Serum creatinine• Urine output (oliguria)• Other AKI biomarkers
• To discuss the risk of chronic kidney disease (CKD) in survivors of neonatal AKI
AKI Definition Evolution
• >35 definitions of “acute renal failure” before 2000• Kellum JA. Curr Opin Crit Care 2000
• 2004: RIFLE criteria created • Bellomo R et al. Crit Care 2004
• 2007: Acute Kidney Injury Network (AKIN) criteria• Mehta RL et al. Crit Care 2007
• 2007: Pediatric (pRIFLE) criteria• Akcan-Arikan A et al. Kidney Int 2007
• 2012: KDIGO classification• Kidney Int Supplements 2012
• 2013: Neonatal modified KDIGO definition • Jetton J et al. The Lancet (Child/Adolescent)
2017
Neonatal AKI Definition (modified KDIGO criteria)
KDIGO definition independently associated with poor outcomes
Jetton J et al. The Lancet (Child-Adolescent) 2017 (in-press)
Challenges with serum creatinine
• Marker of function (not injury)• Rises once 25-50% of renal function is lost
• Rises late (24-48 hrs after initial injury)• Does not differentiate the nature of injury• Affected by fluid status (dilution from fluid overload)
• AKI incidence/staging changes when corrected for fluid overload
• Type of measurement (Enzymatic vs Jaffe)• Jaffe method
• Interference with albumin & bilirubin• May overestimate Cr (0.2 mg/dL in ELBW infants)
Basu RK et al. Pediatr Crit Care Med 2013Allegaert K et al. J of Maternal-Fetal & Neonatal Med 2012
Issues with creatinine (NICU)
• Interference with maternal creatinine• Highly dynamic GFR in 1st few weeks of life • Low muscle mass population• Frequency of Cr monitoring varies from NICU to
NICU• What threshold of Cr rise should we use?
• Historically, absolute SCr >1.5-2 mg/dL has been used • Are these thresholds too strict?
• Should we be using lower %∆SCr thresholds (pRIFLE, AKIN, KDIGO)?
Neonatal serum creatinine trends
Is this AKI?
Creatinine trends (premature infants)
Divided by levels by gestational age
Gallini F Pediatr Nephrol 2000Guignard JP Pediatrics 1999
Is this AKI?
?Tubular reabsorption of SCr
100 umol/L= 1.1 mg/dL120 umol/L = 1.35 mg/dL
Failure to drop?
Gupta C et al. Pediatr Nephrol 2016
Failure to drop?
Proposes cutoffs and rates of decline as diagnostic of AKI
Gupta C et al. Pediatr Nephrol 2016
Cystatin C vs Serum Creatinine
• Advantages of Cystatin C• Independent of age, sex, weight, height• Minimal amounts cross placenta• Filtered by glomerulus, completely reabsorbed, & not
secreted• Superior to serum Cr in estimating GFR in neonates• However, 5x the cost of SCr ($3-5/assay)
Abitbol CL et al. J Peds 2014
Urine output issues
• What is the definition of “oliguria” in a neonate?• Minimum urine output 1 cc/kg/hr to remain in solute balance• Most standardized definitions define “oliguria” <0.5 cc/kg/hr
• How do we measure U/O accurately?• Many NICU patients do not have Foley catheters• How do we deal with the “poop situation” & “combos” on
flow sheets?
• When do we start the urine output clock in NICU pts?• Many infants do not urinate right away
• Does adding U/O criteria change AKI incidence/staging?
24 hours good time to start the clock?
Clark DA. Pediatrics 1977
• Retrospective NICU study (312 infants)• 48% pre-term, 24% 5-min APGAR <7• Overall mortality 12.8%
• U/O measured by weighing diapers q3hours• AKI defined by pRIFLE (eGFR & U/O criteria)• Patients divided into U/O thresholds (excluding 1st
24 hrs of life)• Group 1: >1.5 cc/kg/hr x 24 hrs • Group 2: 1-1.5 cc/kg/hr x 24 hrs• Group 3: 0.7-1 cc/kg/hr x 24 hrs• Group 4: <0.7 cc/kg/hr x 24 hrs
Bezerra CTM et al. Nephrol Dial Transplant 2013
pRIFLE criteria: AUC for mortality 0.689, addition of proposed U/O criteria 0.885Bezerra CTM et al. Nephrol Dial Transplant 2013
Adding U/O Criteria Changes IncidenceAWAKEN Study
Jetton J et al. The Lancet (Child-Adolescent) 2017 (in-press)
Incidence with creatinine criteria: 380/2022 (19%)Incidence with Cr or U/O criteria: 605/2022 (30%)
Neonatal AKI Biomarkers
Published norms for premature infants without AKI
Saeidi B et al. Pediatr Nephrol 2015
AKI biomarkers in premature infants during first week of life
Askenazi D et al. CJASN 2016
Table 5. Performance for biomarker value to acute kidney injury (maximum biomarker level for all, except those shown with ** which areminimum values)
* log transformed before analysis to normalize the distribution.
Take Home Points• Complex neonatal physiology makes creatinine a
flawed clinical biomarker of AKI• Oliguria is important to document with mortality
association• Ideal threshold (<1 vs 1.5 cc/kg/hr) not yet answered
• Modified KDIGO classification (both SCr & U/O) should be used consistently until improved definitions come out
• Urine AKI biomarkers in neonates are promising, but further work is needed
Long Term Neonatal Renal Outcomes
AKI CKD
What is Chronic Kidney Disease?
Kidney International 2013
eGFR = 0.413 x (height/Scr) if height is expressed in centimeters (Schwartz)
How Bad Is to Have Chronic Kidney Disease?
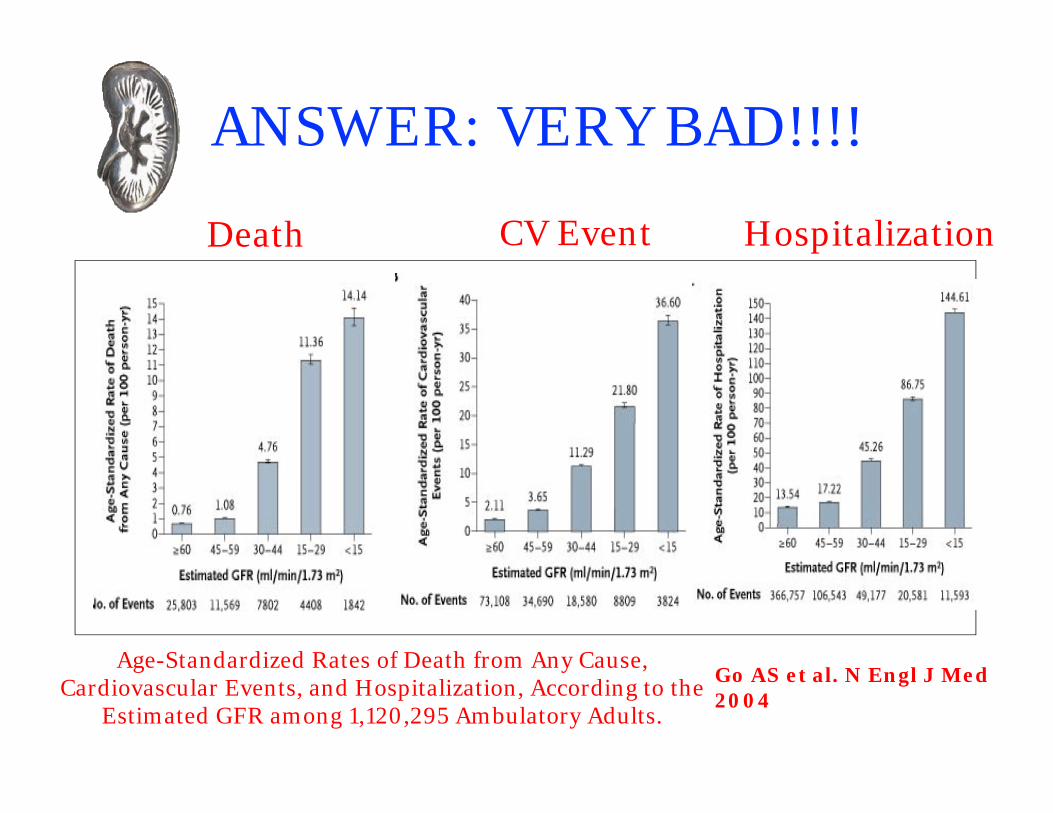
ANSWER: VERY BAD!!!!
Age-Standardized Rates of Death from Any Cause, Cardiovascular Events, and Hospitalization, According to the
Estimated GFR among 1,120,295 Ambulatory Adults.
Death CV Event Hospitalization
Go AS et al. N Engl J Med 2004
AKI & CKD Link in Adults is Strong
Greenberg JH et al. BMC Nephrology 2014
Limited neonatal AKI to CKD literature
• Anand SK J Pediatr 1978 • Mocan H Pediatr Nephrol 1991 • Shaw NJ Int J Cardiol 1991• Marks SD J Pediatr 2005• Polito C Clin Pediatr 1998• Abitbol CL Pediatr Nephrol 2003• Zwiers AJM Clin J Am Soc 2014• Bruel A Pediatr Nephrol 2016• Harer MW Pediatr Nephrol 2017 • Maqsood S Pediatr Nephrol 2017• Chaturvedi S Pediatr Nephrol 2017 (Review Article)
• Long term outcome of 20 ELBW infants with AKI • Peak SCr >2mg/dl > 48hrs and/or oliguria (<0.5 ml/kg/hr)
after 3rd DOL
• Mean age at F/U: 7.5 +/- 4.6 yrs (range 3.2-18.5 yrs)• Chronic renal impairment: eGFR <75 ml/min/1.73m2
• Also assessed for proteinuria (Urine PCR >0.2 mg/g), HTN (casual office BP), and renal size (U/S)
• 9/20 (45%) patients identified with low eGFR
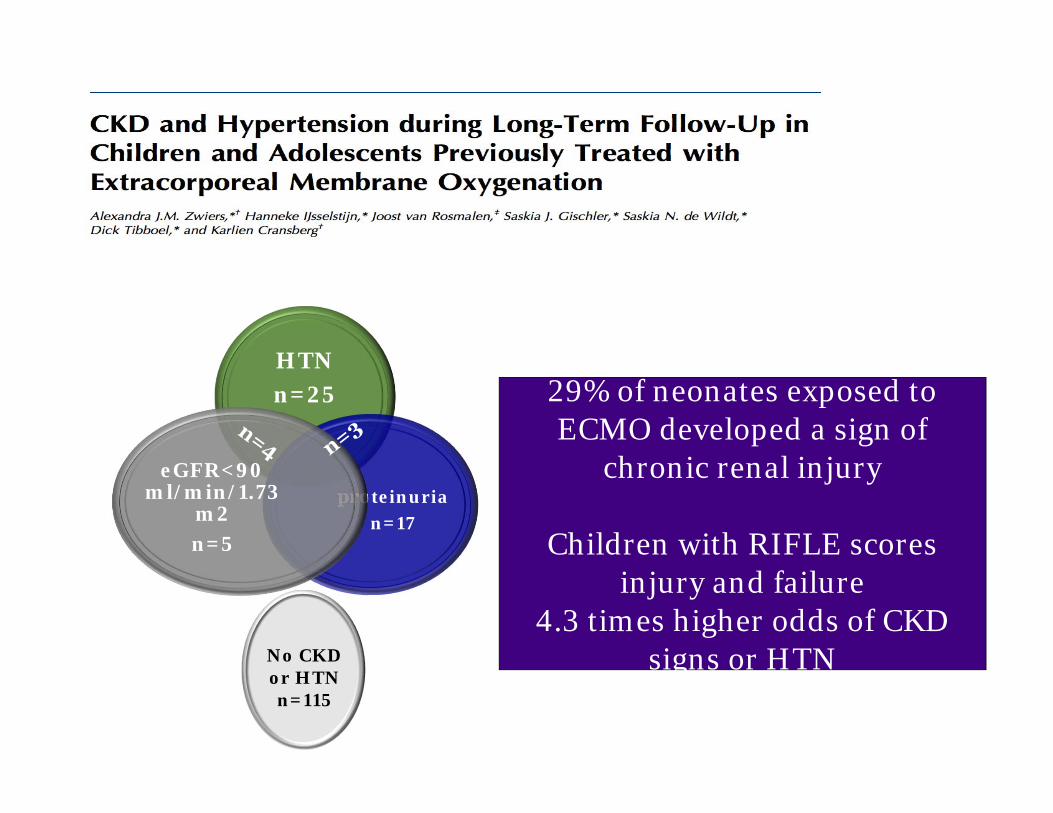
• Rotterdam, Netherlands ECMO program• 423 neonates undergoing ECMO from
1992-2002• 65% Incidence of AKI (pRIFLE)• Median age of follow-up: 8.2 years
Zwiers AJM et al. Clin J Am Soc 2014
HTNn=25
proteinurian=17
eGFR<90 ml/min/1.73
m2n=5
No CKD or HTNn=115
ECMO~620
29% of neonates exposed to ECMO developed a sign of
chronic renal injury
Children with RIFLE scores injury and failure
4.3 times higher odds of CKD signs or HTN
• 34 VLBW infants followed up at 5 years of age • 20 with neonatal AKI and 14 without Neonatal AKI
• 9/34 (26%) had Cystatin C eGFR<90 mL/min/1.73 m2 (p = 0.25)• 7/20 (35%) with AKI • 2/14 (14%) without AKI
• At least one sign of CKD (p< 0.05)• 13/20 (65%) with AKI• 2/14 (14%) w/o AKI
VLBW neonates with AKI had a
4.5 times greater risk of CKD
Harer MW et al. Pediatr Nephrol 2017
Many other factors associated with CKD in neonates
Chaturvedi S et al. Pediatr Nephrol 2017
Albuminuria:
OR = 1.81 (1.19, 2.77)
ESRD:
OR = 1.58 (1.33, 1.88)
Low eGFR:
OR = 1.79 (1.31, 2.45)
White SL et al. Am J Kidney Dis 2009
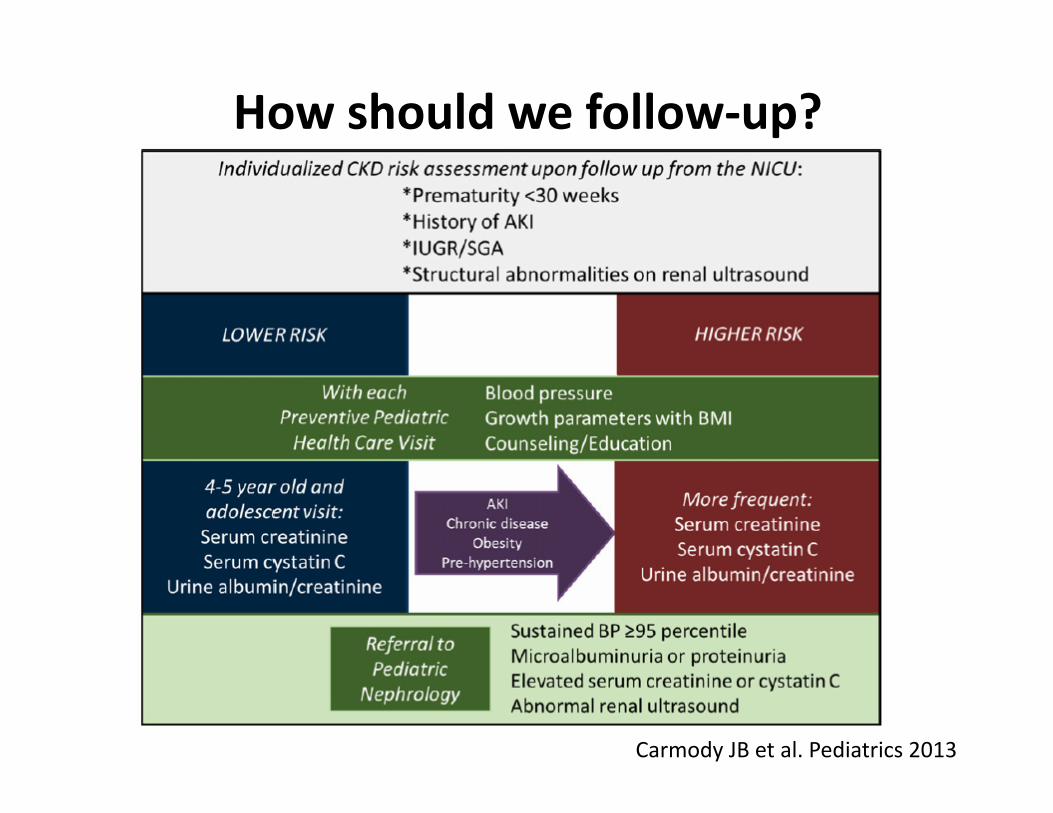
How should we follow-up?
Carmody JB et al. Pediatrics 2013
Take Home Points• Survivors of neonatal AKI may be at high risk of CKD• Even without AKI, babies with LBW/IUGR and/or
prematurity are at risk of CKD• Long-term renal surveillance is needed
• Nephrologists & neonatologists need to work together to make this happen
• What can “we” do for now?• Improve knowledge translation (spread the word)• Better recognition and recording of AKI episodes• Concentrate on AKI awareness & prevention• Design better larger scale prospective studies
Questions/CommentsDr. Cherry Mammen
Clinical Assistant Professor (UBC)Pediatric Nephrologist/Director of Dialysis