133
Healthy Kansans living in safe and sustainable environments.

Healthy Kansans living in safe and sustainable environments.

Bureau of Epidemiology and Public Health Informatics
Changes to the KDHE Infectious or Contagious Diseases and Conditions Regulations
Sheri TubachChelsea Raybern
Infectious Disease Epidemiology and Response
Agenda
❖ Training Session 1➢ Mandated Reporting and Specimen Submission
Requirements
❖ Training Session 2➢ Isolation and Quarantine Requirements
➢ Rabies Control Requirements
Objectives
▪ Know what infectious diseases are reportable.
▪ Know the timeframe and method of reporting.
▪ Understand the changes to the isolation and
quarantine regulation.
▪ Understand the changes to the rabies control
regulation.

AgendaRegulations Topic Time
KAR 28-1-2 Public Health in Kansas
Mandating Reporting
15 minutes
Changes to the reporting
timeframe and reportable
disease list
45 minutes
KAR 28-1-4 Hospital Reporting
Requirements
15 minutes
KAR 28-1-18 Laboratory reporting and
specimen submission
guidelines
15 minutes
Q & A 15 minutes
Three Levels of Public Health
▪ Local: Local Health Departments
▪ State: State Health Departments
▪ National: CDC
▪ Not a hierarchy
Local Health Departments
▪ Counties or cities
▪ First level of contact with public
▪ Broad power for control measures in Kansas
▪ Outbreak investigations:▪ foodborne, others
▪ Surveillance:▪ reportable diseases
▪ Special projects:▪ usually upon involvement from state/national level
State Health Department
▪ Broad statutory and regulatory power
▪ Outbreak investigations:
▪ assists local health departments
▪ interstate outbreaks
▪ Surveillance:
▪ list of reportable diseases
▪ transmit reports to CDC
▪ prepare state reports
▪ other data sets: cancer registry, hospital discharge
▪ KS health information system
▪ Analytic projects
National Level – CDC
▪ Outbreak investigations:▪ EPI-Aid
▪ Surveillance:▪ MMWR
▪ National surveys
▪ Other special surveillance projects
▪ Analytic projects:▪ Often with local/states
Different Purposes and Methods
▪ State/local level:
▪ Purpose: Link to immediate control efforts/program
evaluation.
▪ Methods: Real-time data on all cases.
▪ Federal level:
▪ Purpose: Monitor national trends, detect emerging
problems, demonstrate need for resources.
▪ Methods: aggregate local data, national sample
surveys.
Surveillance at the State/Local Level is Linked to Control Activities
▪ Case level: Assure appropriate treatment▪ Example: Botulism
▪ Contact level: Assure contacts are treated▪ Example: Pertussis in high risk contacts
▪ Community level: Remove source of outbreaks▪ Example: Listeria in ice cream
▪ Program level: Monitor effectiveness in real time▪ Example: Vaccination
Methods of Surveillance – How Do We Capture the Information?
▪ Passive surveillance: no regular active contact to reporters
▪ Disease reporting from MDs, facilities, labs▪ communicable disease and condition reporting
Surveillance / Case Reporting
▪ Determined by states
▪ Some standardization desirable
▪ Nationally notifiable conditions
▪ Case definitions
▪ Council of State and Territorial Epidemiologists
▪ Since 1951
▪ Collaborative process
The National Notifiable Disease Surveillance System (NNDSS)
▪ Recommended list of conditions under surveillance (CDC and CSTE).
▪ States implement national list according to local considerations through statute/regulatory process.
▪ States collect standard data elements and apply standard case definitions (CDC/CSTE).
▪ States forward individual case-level data to CDC without identifiers on a voluntary basis.
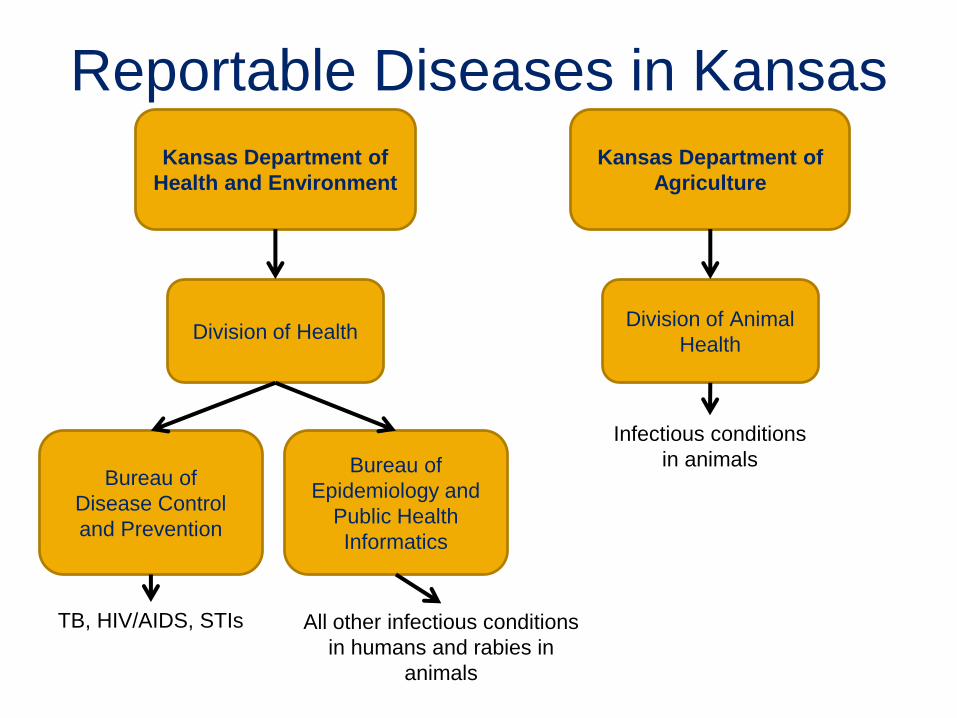
Kansas Department of
Health and Environment
Division of Health
Bureau of
Disease Control
and Prevention
Bureau of
Epidemiology and
Public Health
Informatics
Kansas Department of
Agriculture
Division of Animal
Health
TB, HIV/AIDS, STIs All other infectious conditions
in humans and rabies in
animals
Infectious conditions
in animals
Reportable Diseases in Kansas
Why do we investigate?
16
Why Investigate?
▪ To prevent the spread of illness!
▪ Trace disease source and spread
▪ Identify outbreaks
▪ Implement control and prevention measures
▪ Gain information for policy, education
▪ Used by state, CDC
▪ Design disease control activities
▪ Evaluate programs and vaccine efficacy

Mandated Reporting

Who Reports? KSA 65-118
Immunity for reporting
Confidential
Physicians and
Physician’s Assistants
Dentists
Nurses
Administrator – Hospitals
or LTCF
Social Worker
Teacher or School
Administrator
19
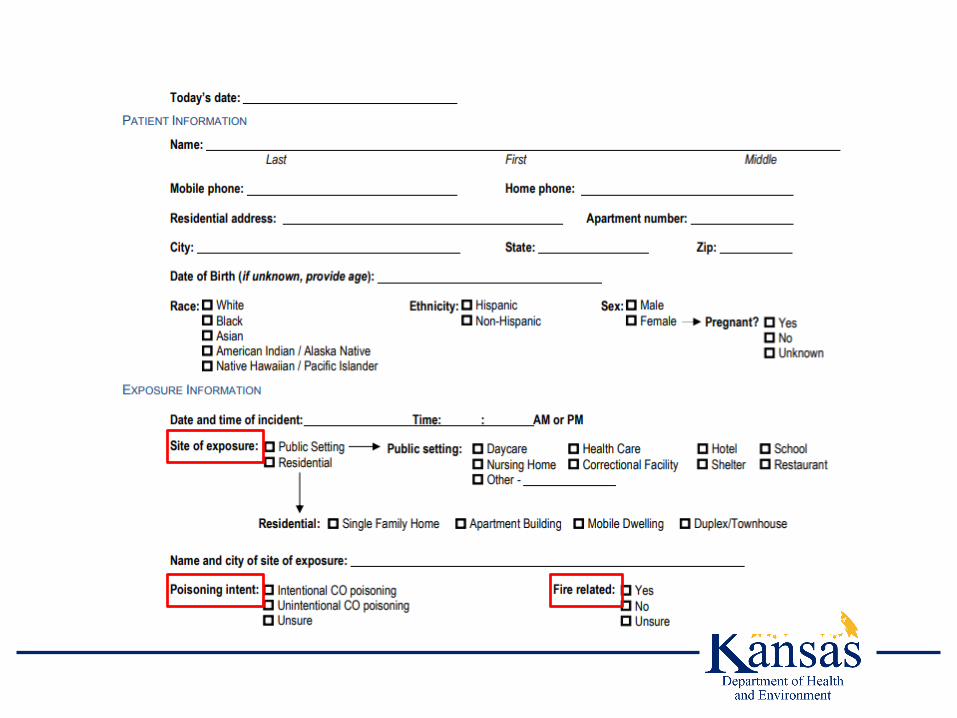
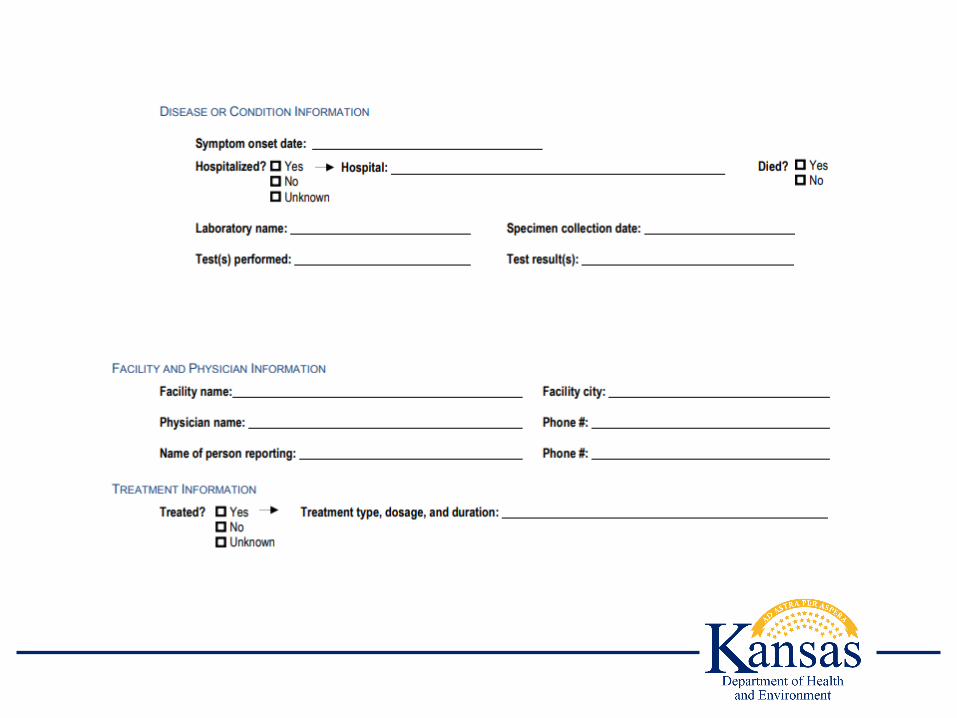
What to report?
▪ First and last name
▪ Address
▪ Telephone number
▪ Date of birth
▪ Sex
▪ Race
▪ Ethnicity
▪ Pregnancy status
▪ Date of symptom onset
▪ Diagnosis
▪ Diagnostic tests
▪ Type and site of specimen
▪ Date of specimen collection
▪ Results
▪ Treatment
▪ Name, address, and telephone
of attending physician
20
How to Report KSA 65-118
KAR 28-1-2
4-Hour Reportable Diseases
Kansas Department of Health
and Environment
All Other Reportable Diseases
Local Health Department
21

Laboratory Reporting KSA 65-118
KAR 28-1-18
4-Hour Reportable Diseases
Kansas Department of Health
and Environment
All Other Reportable Diseases
22

Laboratory Reporting KSA 65-118
KAR 28-1-18
23

Questions
Update to KAR 28-1-2Reporting Requirements of
Infectious or Contagious Diseases and Conditions
Rationale for Revisions▪ Last revised in 2006
▪ Harmonization with Nationally Notifiable Conditions list
desirable
▪ Changes in terminology
▪ K.A.R. 28-1-2 limited to infectious diseases, so
conditions required to be reported in several
places
▪ Inadequate information reported
▪ Need for more rapid reporting and updated
methods (ELR)
Time Frames to Report
▪ Previous Requirements
▪ 4 hours by telephone for urgent conditions
▪ 7 days for others
▪ Current Requirements
▪ 4 hours by telephone for urgent conditions
(no change)
▪ 24 hours for all others
▪ Grace period for weekends and holidays
New 4-hour Reportable Diseases
▪ Changed reporting from 7 days to 4 hours
▪ Diphtheria
▪ Tetanus
▪ New 4-hour reportable diseases
▪ Novel influenza A virus
▪ Vaccinia, post-vaccination or secondary transmission
▪ Viral hemorrhagic fevers
▪ Unexplained death suspected to be due to an
unidentified infectious agent
Novel Influenza A
▪ Human infections with novel influenza A viruses
may signal the beginning of an influenza
pandemic
▪ Rapid detection and reporting of human infections
with novel influenza A viruses
▪ Prompt detection and characterization of the virus
▪ Determine the potential for a pandemic
▪ Accelerate the implementation of effective public health
responses

Novel Influenza A
▪ Different from currently circulating human
influenza H1 and H3 viruses
▪ H2, H5, H7, and H9 subtypes
▪ Influenza H1 and H3 subtypes
▪ from a non-human species
▪ genetic reassortment between animal and human
viruses
▪ Novel subtypes are detected by State Public
Health Laboratory and confirmed at CDC
Vaccinia▪ Purpose of reporting and surveillance
▪ To identify vaccinia disease developing in a person or
close contact following a smallpox vaccination
▪ To ensure prompt evaluation and treatment as
appropriate, and prevent secondary transmission
▪ To ensure reporting of such events to the Vaccine
Adverse Events Reporting Systems (VAERS) to track
the frequency and epidemiology of such events
▪ Primary and secondary cases are reportable
▪ Vaccinia immune globulin (VIG) is available
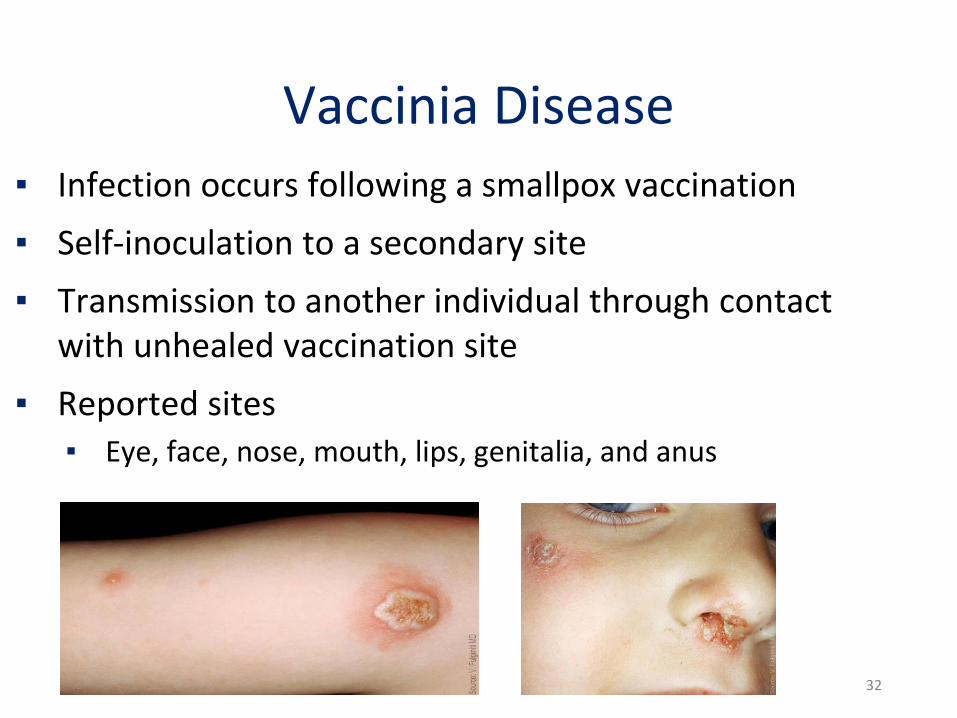
Vaccinia Disease▪ Infection occurs following a smallpox vaccination
▪ Self-inoculation to a secondary site
▪ Transmission to another individual through contact with unhealed vaccination site
▪ Reported sites▪ Eye, face, nose, mouth, lips, genitalia, and anus
32
Viral Hemorrhagic Fever
▪ Includes Crimean-Congo hemorrhagic fever virus,
Ebola virus, Lassa virus, Lujo virus, Marburg virus
and the New World arenaviruses (Guanarito virus,
Junin virus, Machupo virus, and Sabia virus
▪ Used to be reportable when identified in the
course of a possible bioterrorism act
▪ Potential for natural introduction

Unexplained Deaths
▪ Purpose of reporting and surveillance
▪ To identify emerging pathogens in Kansas
▪ To raise the index of suspicion of a possible
bioterrorism event
▪ To recognize infectious diseases with potential
public health impact
Unexplained Deaths – When to Report▪ Clinically consistent with hallmarks of an
infectious process
▪ Fever
▪ Leukocytosis
▪ Histopathologic evidence of an acute infectious
process
▪ Physician-diagnosed syndrome
▪ Preliminary testing has not revealed a cause
▪ Absence of a chronic or immunocompromising
condition, no trauma, no toxic exposure, no
preceding nosocomial infection
Diseases Removed from the 4-hour Reportable List
▪ Not reportable
▪ Bacterial Meningitis
▪ Unless meningitis is thought to be caused by a
reportable disease
▪ Now reportable within 24 hours
▪ Pertussis
▪ Rabies, animals
Still Reportable – 4-Hours
▪ Clusters, outbreaks, and epidemics
▪ Terrorist acts
▪ Biological
▪ Chemical
▪ Radiological
▪ Unusual disease or manifestation of illness
Diseases Added to the 24-hour Reportable List
▪ Acute flaccid myelitis
▪ Anaplasmosis
▪ Babesiosis
▪ Blood lead levels (any
results)
▪ Candida auris
▪ Carbapenem-resistant
bacterial infections or
colonization
▪ Carbon monoxide
poisoning
▪ Coccidioidomycosis
▪ Hepatitis B in children < 5
years – All lab results
▪ Histoplasmosis
▪ Leptospirosis
▪ Vancomycin-intermediate
S. aureus
▪ Vancomycin-resistant S.
aureus
▪ Vibriosis (non-cholera
Vibrio spp.)
Harmonization with Nationally Notifiable Conditions list
▪ Babesiosis
▪ Coccidioidomycosis
▪ Hepatitis A
▪ Histoplasmosis
▪ Leptospirosis
▪ Vancomycin-intermediate S. aureus (VISA)
▪ Vancomycin-resistant S. aureus (VRSA)
▪ Vibriosis (non-cholera Vibrio spp.)
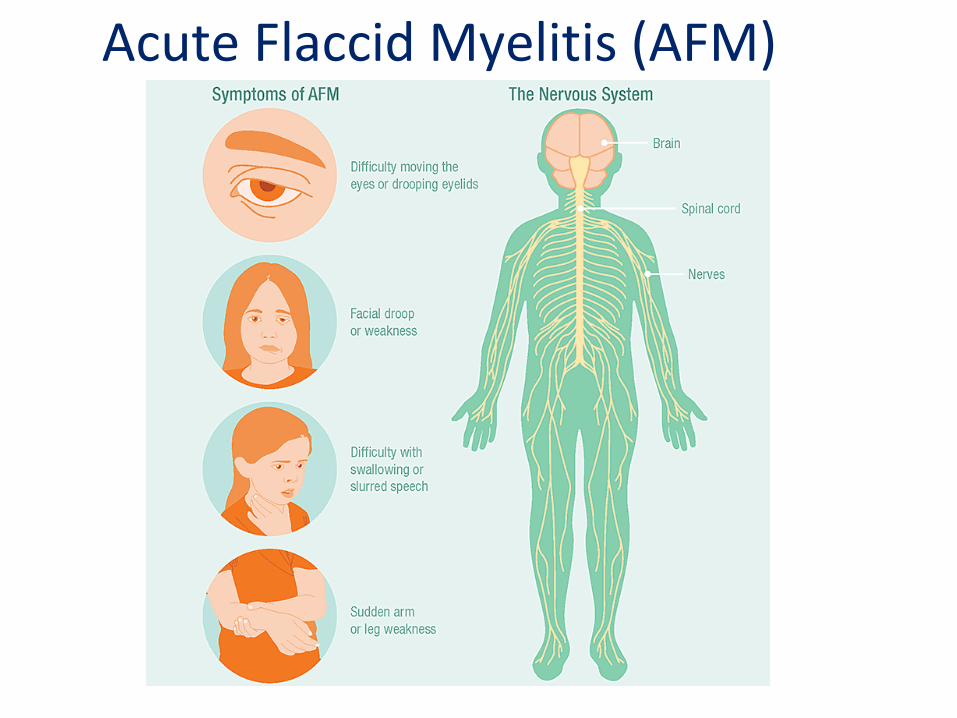
Acute Flaccid Myelitis (AFM)
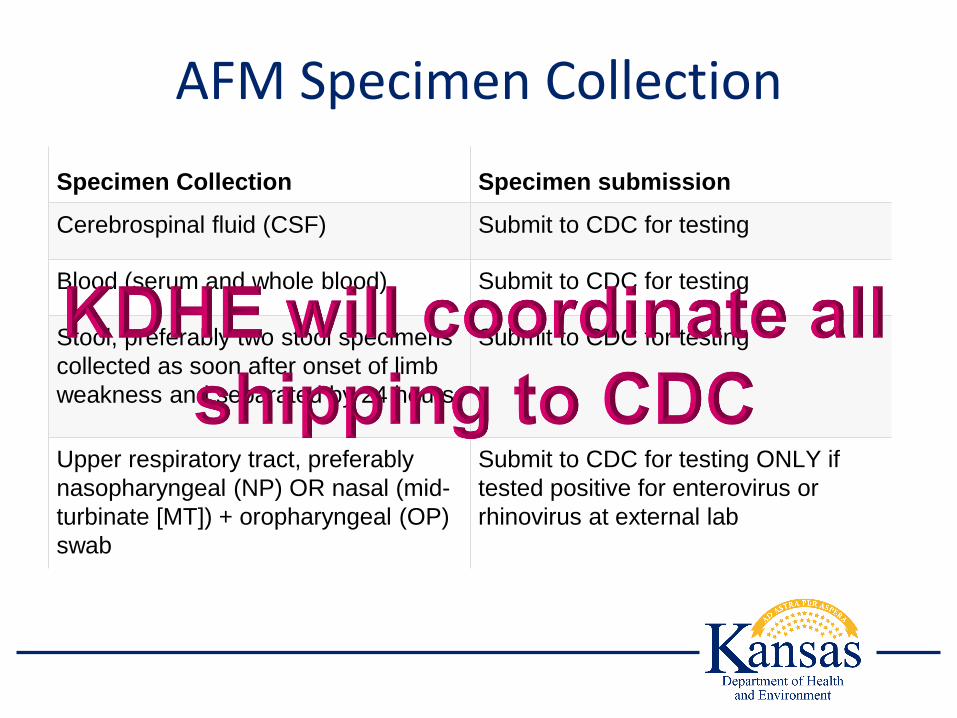
AFM Specimen Collection
Specimen Collection Specimen submission
Cerebrospinal fluid (CSF) Submit to CDC for testing
Blood (serum and whole blood) Submit to CDC for testing
Stool, preferably two stool specimens
collected as soon after onset of limb
weakness and separated by 24 hours
Submit to CDC for testing
Upper respiratory tract, preferably
nasopharyngeal (NP) OR nasal (mid-
turbinate [MT]) + oropharyngeal (OP)
swab
Submit to CDC for testing ONLY if
tested positive for enterovirus or
rhinovirus at external lab

Anaplasmosis
▪ Anaplasmosis is a disease caused by the
bacterium Anaplasma phagocytophilum
▪ This organism was previously known by
▪ Ehrlichia equi
▪ Ehrlichia phagocytophilum,
▪ Disease was previously known as human
granulocytic ehrlichiosis (HGE)
▪ Change in 2001 identified that this organism
belonged to the genus Anaplasma

Babesiosis
▪ Became nationally notifiable in 2011
▪ Parasitic tick-borne infection
▪ Blacklegged tick (Ixodes scapularis)
▪ Babesia spp. can also be transmitted via blood
products
▪ There is no licensed screening test available
for detecting Babesia spp. in blood donors
Coccidioidomycosis (Valley Fever)
▪ Coccidioidomycosis is an infection of the lungs
caused by the fungal species Coccidioides
▪ Coccidioides grow in soil, particularly in arid areas
▪ Infection occurs by inhaling contaminated dust
with fungal spores
▪ Purpose of Reporting and Surveillance
▪ To track the emergence of Coccidioides in Kansas
▪ To monitor trends in the disease due to Coccidioides
▪ Nationally notifiable since 1995

Histoplasmosis
▪ Histoplasmosis is one of the most common
endemic fungal infections in the United States
▪ Inhalation of spores found in soil contaminated
with bird or bat droppings
▪ Not nationally notifiable
▪ True number of cases is unknown and is difficult to
ascertain
▪ Ten states track cases
▪ Most in the central states
Leptospirosis▪ Re-emerging bacterial disease affecting both humans
and animals
▪ Incidence is increasing and exposure shifting from occupational to recreational (Climate Change?)
▪ 100-200 human cases of leptospirosis reported annually through 1994
▪ 1995- ceased to be a nationally notifiable condition
▪ Remained reportable disease in 36 states and territories
▪ In 2013 became nationally notifiable again

Hepatitis A
▪ Previously all positive Hepatitis A were reportable
▪ Total antibody positive – most likely immunity not
disease
▪ Only IgM + results are reportable

Hepatitis B in children < 5 years – All lab results
▪ Perinatal Hepatitis B Prevention Program
▪ Ensures prevention of transmission of hepatitis B from
mother to infant during birth
▪ Metrics of the Program
▪ HBIG and hepatitis B birth dose given within 12 hours
▪ Completion of the 3-dose series
▪ Post vaccination serological testing (PVST)
PVST
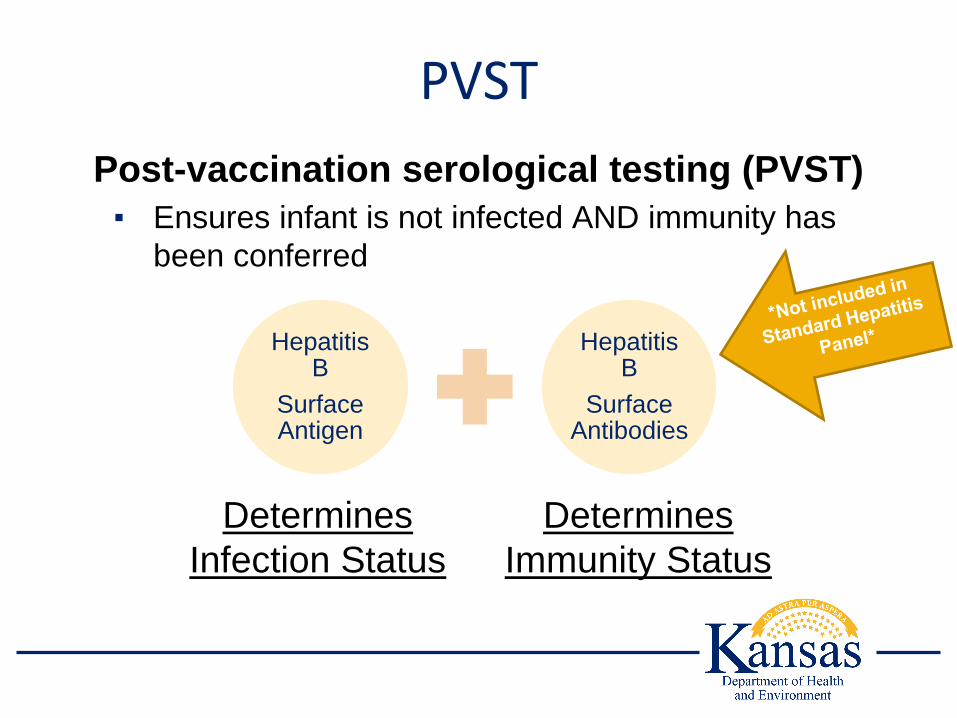
Post-vaccination serological testing (PVST)
▪ Ensures infant is not infected AND immunity has
been conferred
Hepatitis B
Surface Antigen
Hepatitis B
Surface Antibodies
Determines
Infection Status
Determines
Immunity Status
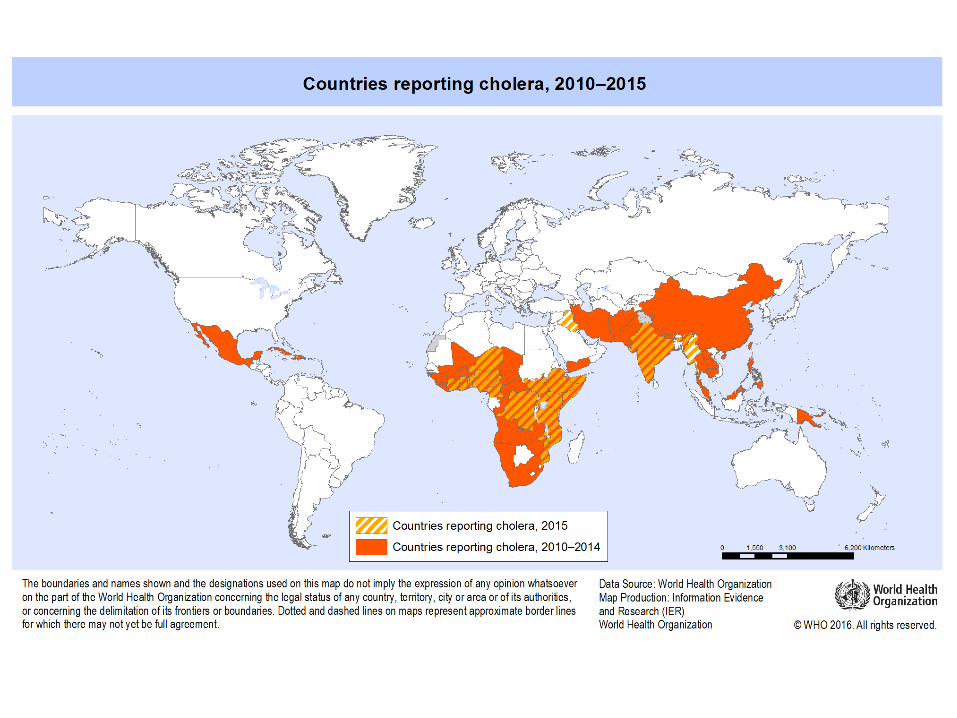
Cholera
▪ Profuse watery diarrhea, vomiting,
and leg cramps
▪ Toxigenic Vibrio cholerae (serogroup O1 or O139)
▪ 12 hours to 5 days for symptoms to appear
▪ Inadequate water treatment, poor sanitation, and
inadequate hygiene
▪ Rare in the US (0-5 cases annually)
▪ Last case in Kansas was in 1988

GI Panel
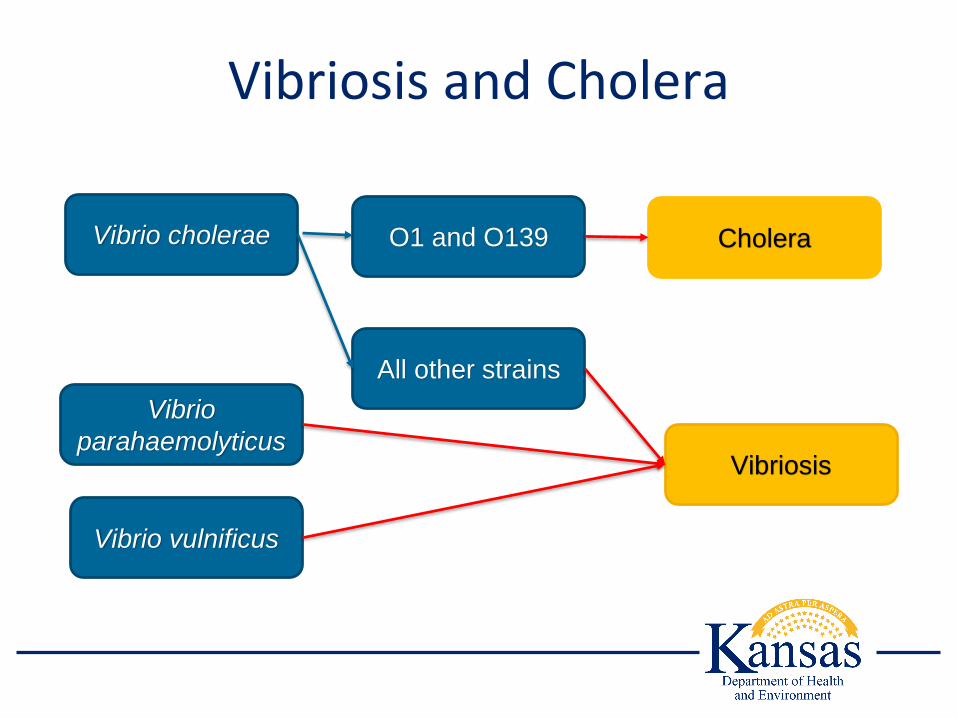
Vibriosis and Cholera
Vibrio vulnificus
O1 and O139 Cholera
All other strains
Vibriosis
Vibrio
parahaemolyticus
Vibrio cholerae
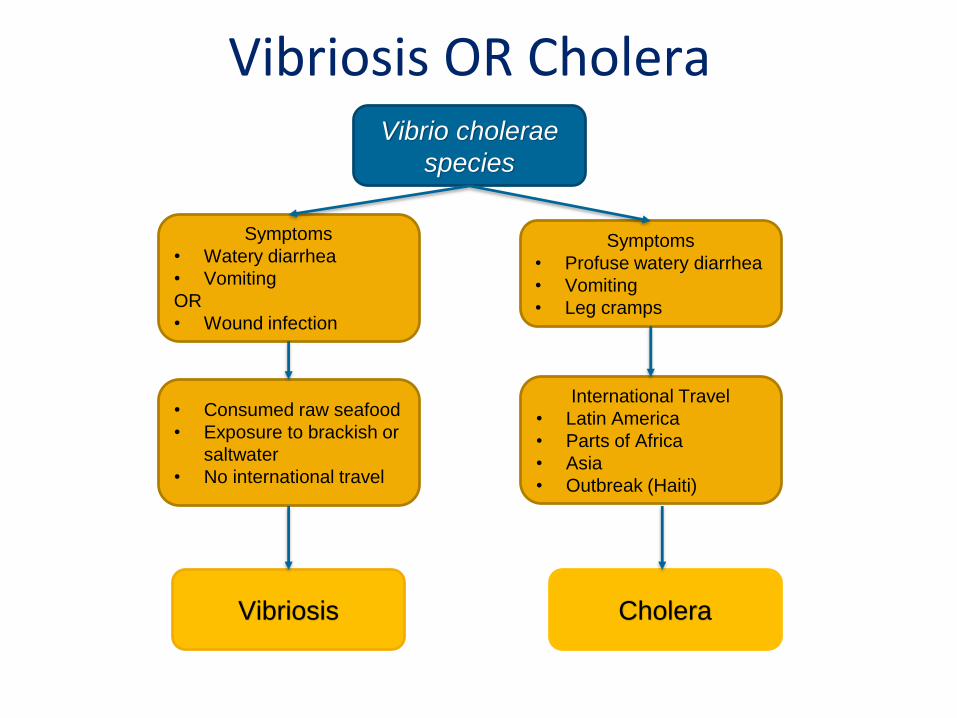
Vibriosis OR Cholera
CholeraVibriosis
Vibrio cholerae
species
International Travel
• Latin America
• Parts of Africa
• Asia
• Outbreak (Haiti)
Symptoms
• Profuse watery diarrhea
• Vomiting
• Leg cramps
• Consumed raw seafood
• Exposure to brackish or
saltwater
• No international travel
Symptoms
• Watery diarrhea
• Vomiting
OR
• Wound infection

Multi-Drug Resistant Organisms (MDROS)
Carbapenem-Resistant Enterobacteriaceae (CRE)
▪ Enterobacteriaceae are gut bacteria that can
spread to other parts of the body causing infection
▪ These bacteria develop resistance to one or more
carbapenem antibiotics▪ Ertapenem, imipenem, meropenem, and doripenem
▪ Carbapenems are often last resort antibiotic for
difficult to treat infections
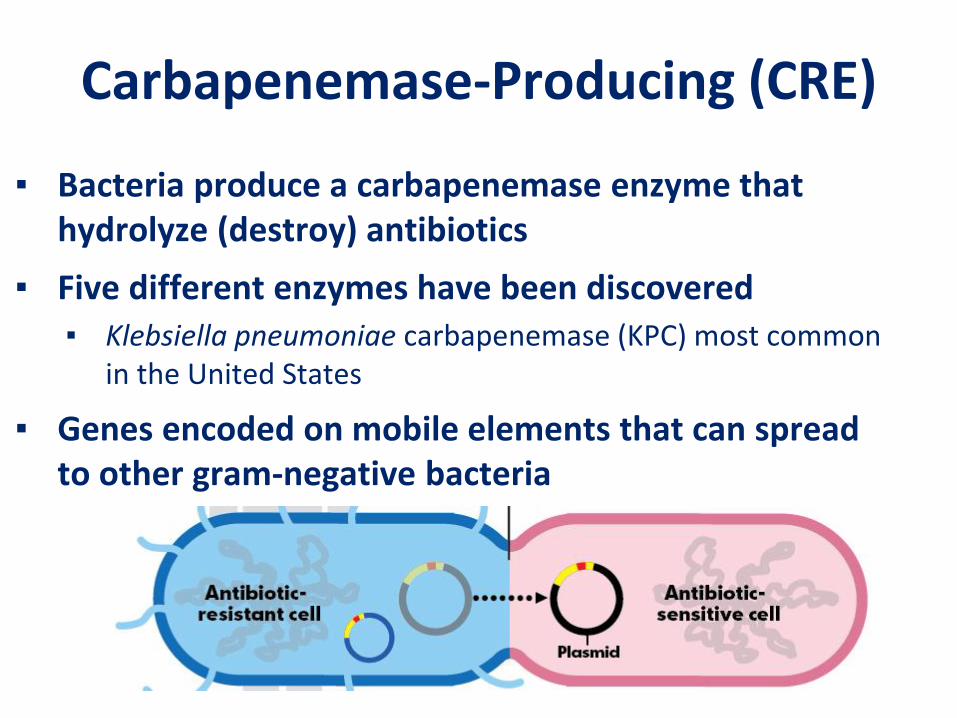
Carbapenemase-Producing (CRE)
▪ Bacteria produce a carbapenemase enzyme that hydrolyze (destroy) antibiotics
▪ Five different enzymes have been discovered▪ Klebsiella pneumoniae carbapenemase (KPC) most common
in the United States
▪ Genes encoded on mobile elements that can spread to other gram-negative bacteria

Carbapenemase-Producing (CRE)
Enterobacteriaceae family (CRE)
Acinetobacter spp. (CRAB)
Pseudomonas aeruginosa (CRPA)
Resistant to any carbapenem: Resistant to any carbapenem: Resistant to any carbapenem:
Ertapenem ≥2 µg/mL or ≤18 mm
Ertapenem N/A (excluded)
Ertapenem N/A (excluded)
Doripenem ≥4 µg/mL or ≤19 mm
Doripenem ≥8 µg/mL or ≤14 mm
Doripenem ≥8 µg/mL or ≤15 mm
Imipenem* ≥4 µg/mL or ≤19 mm
Imipenem ≥8 µg/mL or ≤18 mm
Imipenem ≥8 µg/mL or ≤15 mm
Meropenem ≥4 µg/mL or ≤19 mm
Meropenem ≥8 µg/mL or ≤14 mm
Meropenem ≥8 µg/mL or ≤15 mm
OR Any CRE, CRAB, or CRPA positive for carbapenemase by CIM, mCIM+, CarbaNP, or PCR

Not Your Typical Fungi• Invasive Candida auris mortality 30-60%
(CDC)
• Contaminates patient environment
• Person-person transmission
• Prolonged colonization possible
• Difficult to detect
• Multidrug resistant
Transmission
• Direct contact with infected or
colonized patient
• Direct contact with contaminated
environment and fomites
• CDC study showed persistence >4
weeks on plastic surfaces (in lab)
• Hardy organism
• Standard hospital products inadequate
• Limited treatment options
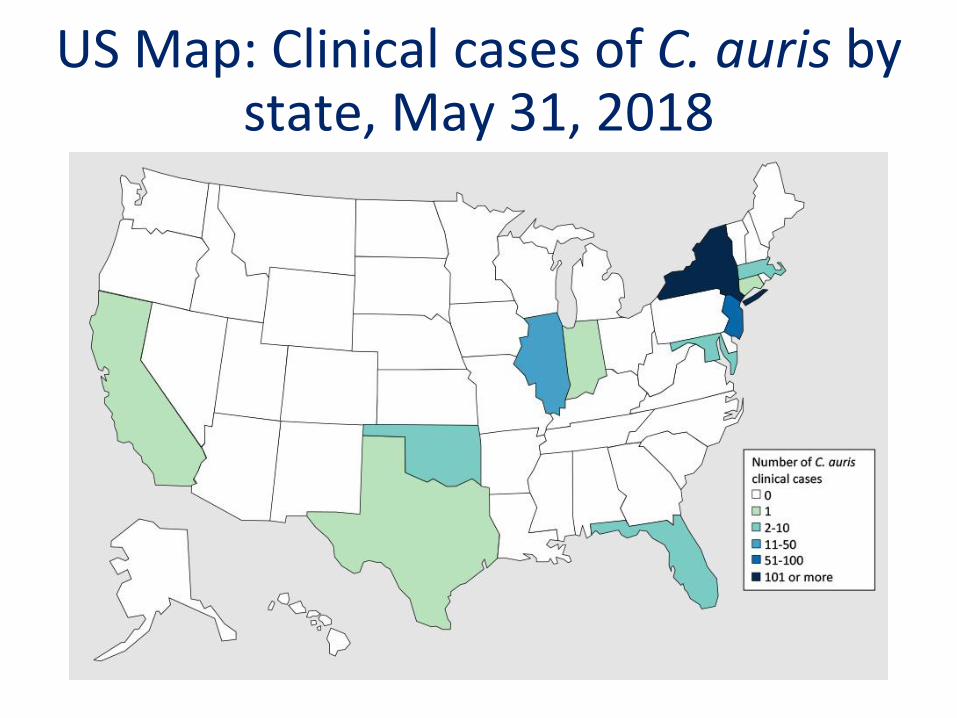
US Map: Clinical cases of C. auris by state, May 31, 2018
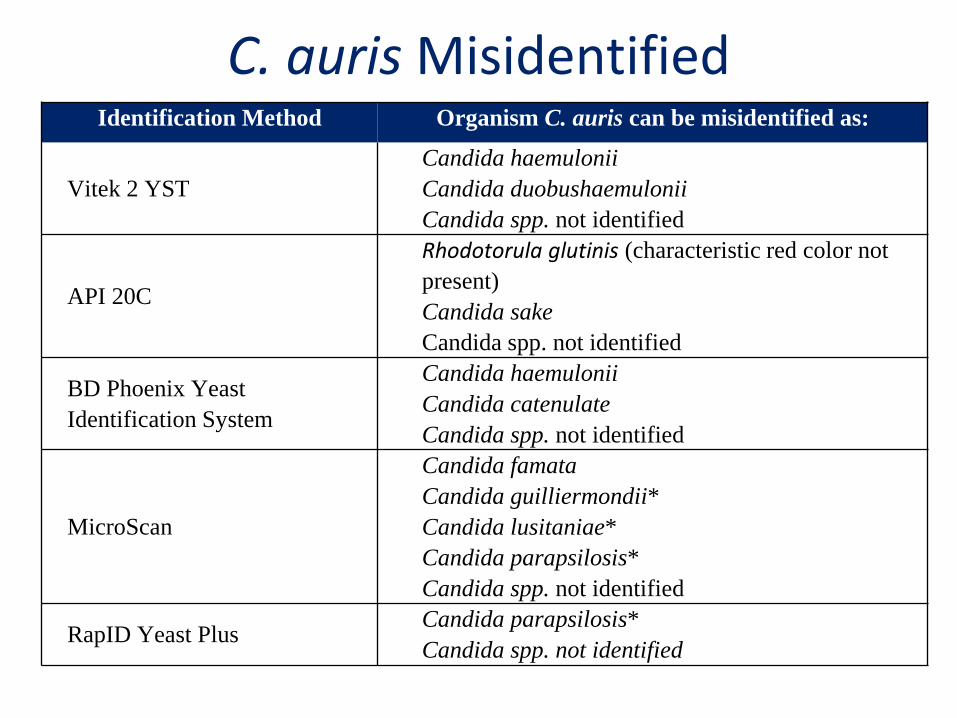
C. auris MisidentifiedIdentification Method Organism C. auris can be misidentified as:
Vitek 2 YST
Candida haemulonii
Candida duobushaemulonii
Candida spp. not identified
API 20C
Rhodotorula glutinis (characteristic red color not
present)
Candida sake
Candida spp. not identified
BD Phoenix Yeast
Identification System
Candida haemulonii
Candida catenulate
Candida spp. not identified
MicroScan
Candida famata
Candida guilliermondii*
Candida lusitaniae*
Candida parapsilosis*
Candida spp. not identified
RapID Yeast PlusCandida parapsilosis*
Candida spp. not identified

VISA and VRSA
▪ Staphylococcus aureus
▪ Intermediate or resistant to vancomycin
▪ Rare
▪ Nationally notifiable in 2004
▪ Monitor for emergence and increasing occurrence
▪ Priority for CDC

Other Reportable Conditions

Blood Lead Poisoning
▪ All blood lead test results are reportable to
KDHE within 24 hours
▪ If blood is being drawn at an external lab, or if
samples are sent to a reference lab for analysis,
a notifiable disease form is not needed
▪ Hospitals/clinics using a point of care machine
should contact Laurie Render
([email protected]) to discuss test result
reporting

Carbon Monoxide Poisoning
▪ All suspect carbon monoxide poisoning cases
(regardless of test results) are reportable to KDHE
within 24 hours
▪ Fax Carbon Monoxide Poisoning Reporting Form
http://www.kdheks.gov/epi/disease_reporting.html
to 877-427-7318
Suspect Cases – 24 Hour Reportable
▪ Need a case report form
▪ Acute Flaccid Myelitis
▪ Carbon monoxide
▪ Chickenpox
▪ Hansen’s disease (Leprosy)
▪ Hantavirus
▪ Hemolytic uremic syndrome
▪ Pediatric influenza deaths
▪ Trichinosis
▪ Whooping cough (Pertussis)

Questions

Update to KAR 28-1-4Hospital Reporting Requirements

Hospital Reporting Requirements*
Number of laboratory tests
Number of pharmacy prescriptions
Number of ER visits
* If information can be provided with minimum additional burden
Update to KAR 28-1-18Reporting and Submission
Requirements for Laboratories
Laboratory Reporting
Kansas Department of Health
and Environment
Reportable Diseases
Electronic Laboratory Reporting (ELR)
4-Hour Reportable Diseases
75

Specimens
1. Isolates of positive cultures
2. Original clinical specimen
3. Nucleic acid
4. Other clinical material
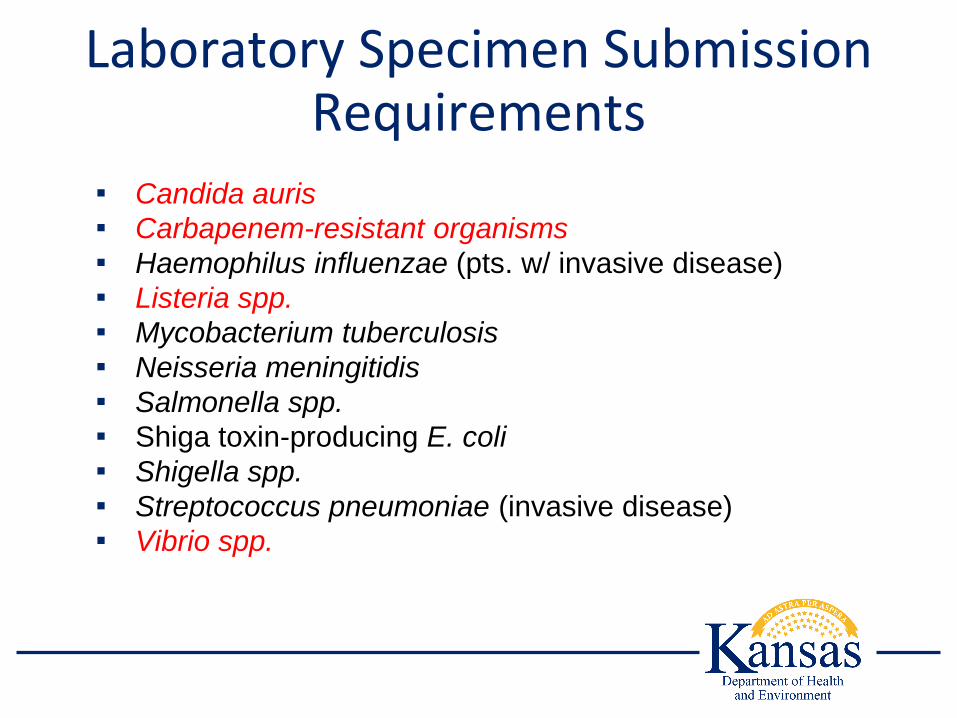
Laboratory Specimen Submission Requirements
▪ Candida auris
▪ Carbapenem-resistant organisms
▪ Haemophilus influenzae (pts. w/ invasive disease)
▪ Listeria spp.
▪ Mycobacterium tuberculosis
▪ Neisseria meningitidis
▪ Salmonella spp.
▪ Shiga toxin-producing E. coli
▪ Shigella spp.
▪ Streptococcus pneumoniae (invasive disease)
▪ Vibrio spp.

Questions

Isolation and QuarantineRabies Control

Agenda
Regulations Topic Time
KAR 28-1-6 Isolation and Quarantine 45 minutes
KAR 28-1-13 Rabies Control 45 minutes
Q & A 15 minutes

KAR 28-1-6Updates to the Isolation and Quarantine of Infectious or
Contagious Diseases

Rationale: Isolation and Quarantine
▪ Last revised: 2007
▪ Need to incorporate current recommendations
▪ Problems with previous regulations
▪ 24-hour vaccination requirement after VPD report to public health
▪ Susceptible health care workers not excluded from work after VPD
exposure
▪ Outdated terminology
▪ Guidance document to be adopted by reference
▪ Requirements for isolation and quarantine for some conditions are
complex
▪ Regulatory format is limiting
http://www.kdheks.gov/epi/download/KDHE_Requirements_for_Isolation_and_Quarantine.pdf

Prevention and Control forSpecific Diseases
▪ a.k.a. “isolation and quarantine”
▪ Scaled measures of prevention and control
▪ Consistent with epidemiology and current
scientific recommendations
▪ Updated terms
▪ Contact, droplet, and airborne precautions
▪ Conditions not subject to isolation or quarantine
are listed
Changes to Format
▪ Guidance document will include specific details
regarding:
▪ Control of Cases
▪ Control of Contacts
▪ Disease are alphabetized
▪ Definitions

Isolation and Quarantine
▪ May be altered by the local health officer or the
secretary of KDHE
▪ Necessary for public health
▪ Based on current medical knowledge
▪ Incubation
▪ Communicable period
▪ Mode of Transmission
▪ Susceptibility
Susceptible Person▪ Person who is
▪ Exposed to a person with an infectious or contagious
disease
▪ Exposed to a contaminated environment
▪ Criteria
▪ Has no history of disease, documented by a physician, that
would confer lifetime immunity; and
▪ No laboratory evidence of immunity; and
▪ No documentation of having been age appropriately
vaccinated according to ACIP; and
▪ No documentation acceptable to the secretary that
demonstrates current immunity

Age Appropriately Vaccinated
▪ Documentation of age-appropriate vaccination
with MMR and Varicella
▪ One dose for preschool-aged children > 12 months
▪ Two doses for children in kindergarten through 12th
grade
▪ Two doses for health-care personnel
CDC. (2013). Prevention of Measles, Rubella, Congenital Rubella
Syndrome, and Mumps. MMWR. 62.
CDC. (2007). Prevention of Varicella. MMWR. 56..
Enteric Diseases
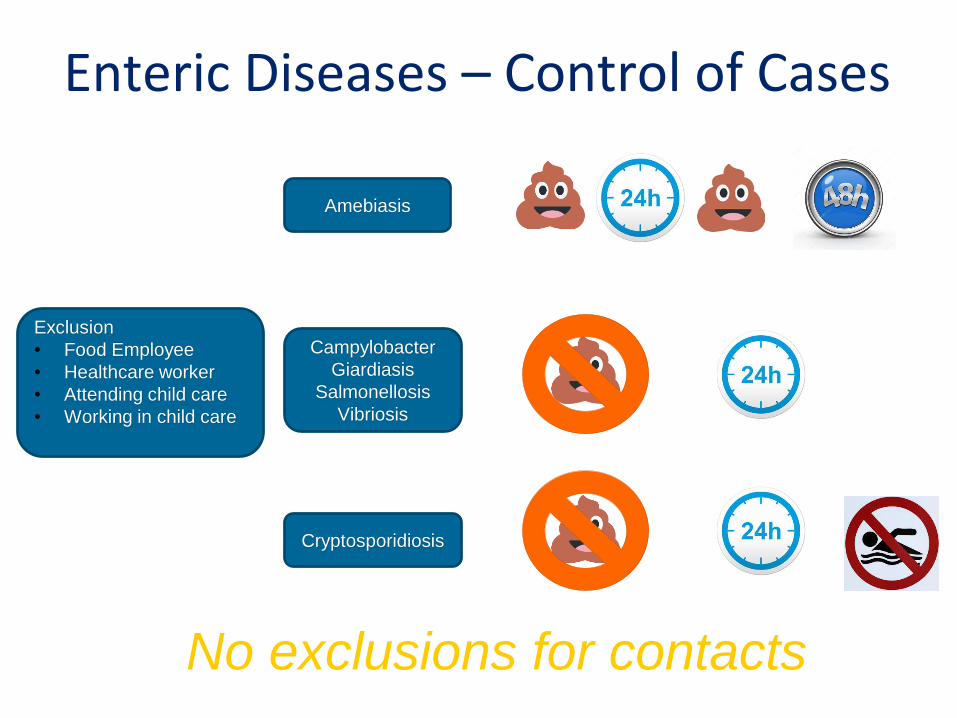
Enteric Diseases – Control of Cases
No exclusions for contacts
Amebiasis
Exclusion
• Food Employee
• Healthcare worker
• Attending child care
• Working in child care
Campylobacter
Giardiasis
Salmonellosis
Vibriosis
Cryptosporidiosis
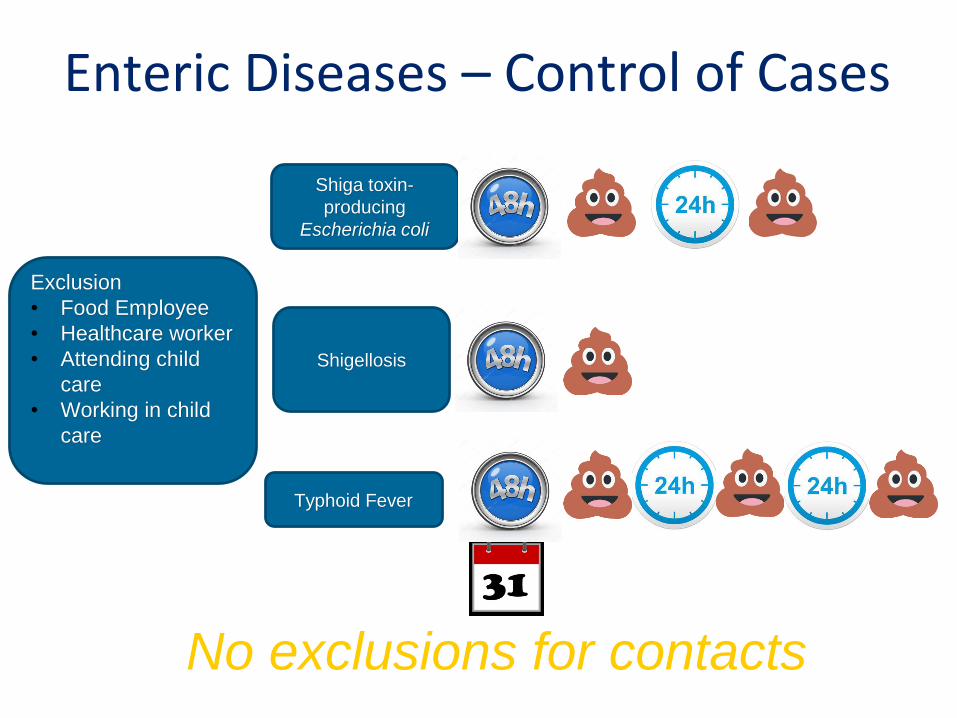
Enteric Diseases – Control of Cases
No exclusions for contacts
Shiga toxin-
producing
Escherichia coli
Exclusion
• Food Employee
• Healthcare worker
• Attending child
care
• Working in child
care
Shigellosis
Typhoid Fever

Drug Resistant Organisms
Candida auris, Carbapenem-Resistant Bacteria – Control of Cases
▪ Contact precautions for persons
infected or colonized
▪ No other isolation requirements
No exclusions for contacts
Clostridium difficile, VISA, or VRSAInfections
▪ Contact precautions for persons
during acute illness
▪ No other isolation requirements
No exclusions for contacts
Vaccine Preventable Diseases
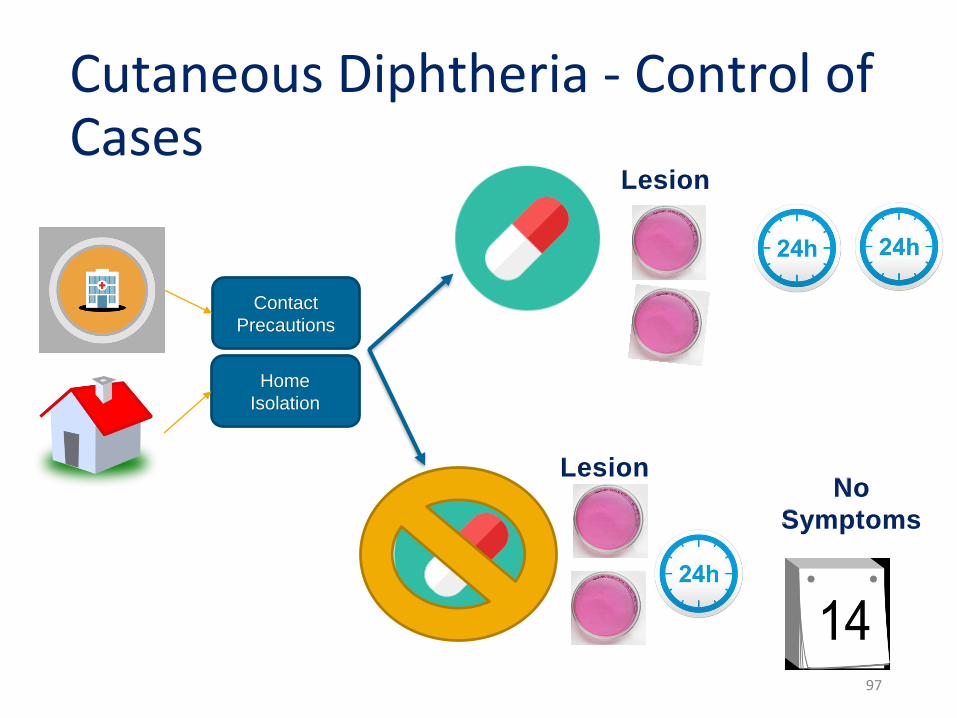
Cutaneous Diphtheria - Control of Cases
97
Contact
Precautions
Home
Isolation
No
Symptoms
Lesion
Lesion
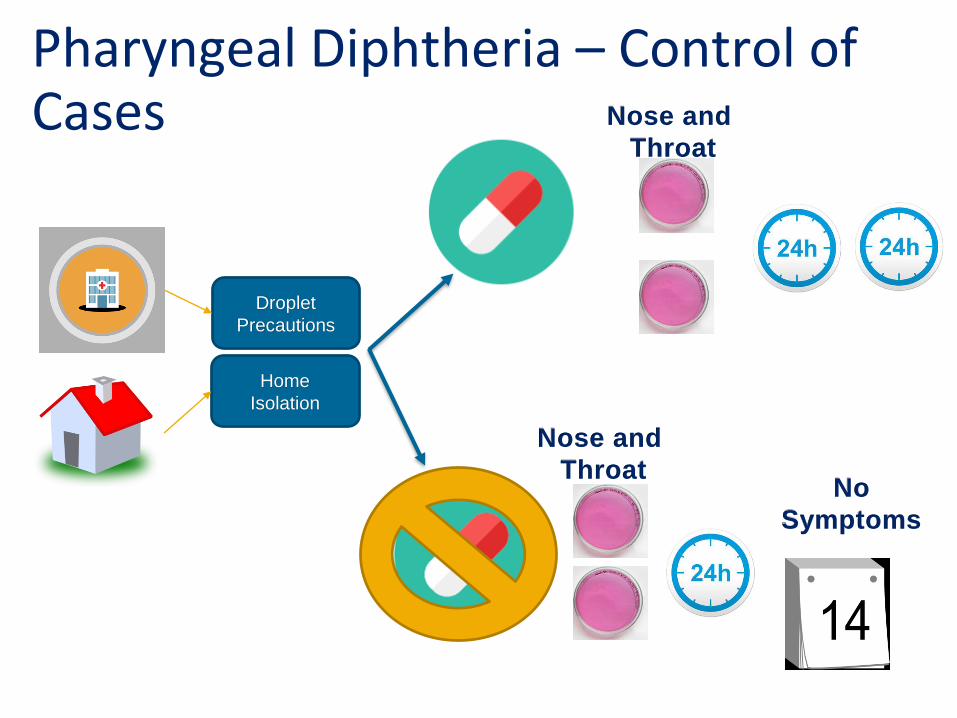
Pharyngeal Diphtheria – Control of Cases
Droplet
Precautions
Home
Isolation
No
Symptoms
Nose and
Throat
Nose and
Throat
Pharyngeal Diphtheria – Control of Contacts
▪ Regardless of immunization status
▪ Monitor for 7 days
▪ Both nose and throat specimens cultured▪ If positive, consider same as case
No exclusion for contacts of
cutaneous diphtheria
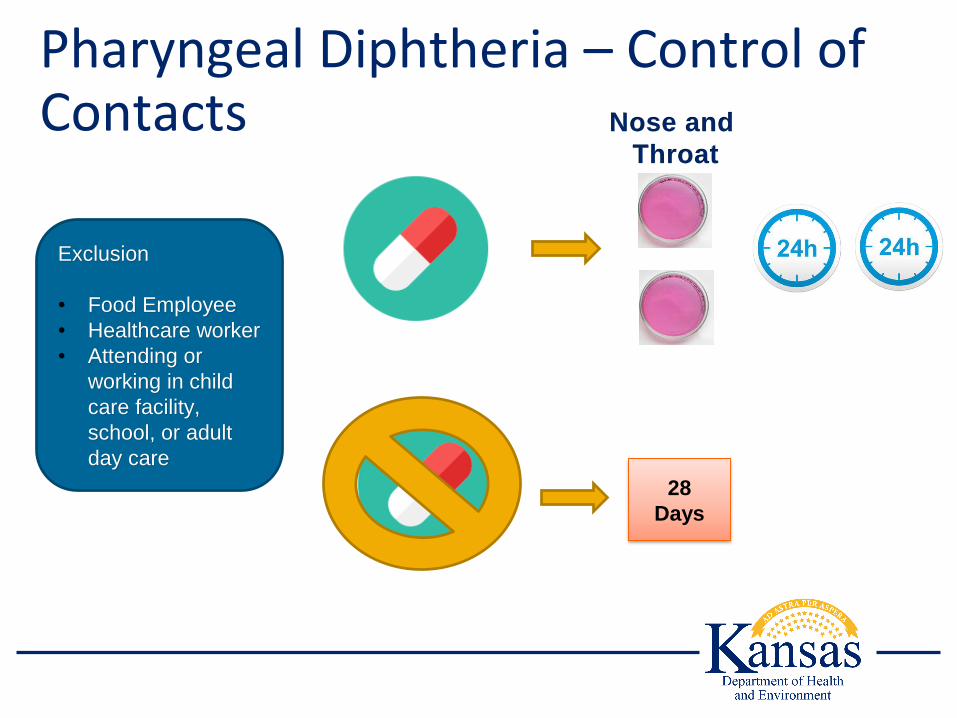
Pharyngeal Diphtheria – Control of Contacts
Exclusion
• Food Employee
• Healthcare worker
• Attending or
working in child
care facility,
school, or adult
day care
Nose and
Throat
28
Days
Haemophilus influenzae, invasive disease – Control of Cases
Droplet precautions for 24 hours after initiation of
antibiotics
No exclusions for contacts
Hepatitis A – Control of Cases
14 Days
from
Onset
7 days
after
jaundice
Exclusion
• Food Employee
• Healthcare worker
• Attending child
care
• Working in child
care

Hepatitis A – Control of Contacts
PEP with
vaccine or IG
within 14 days of
exposure
No Exclusion
No PEP or PEP
after 14 days of
exposure
Excluded for 28
days
Exclusion
• Food Employee
• Healthcare worker
• Attending child
care
• Working in child
care

Herpes Zoster Virus (Shingles) –Control of Cases
Hospitalized and Disseminated
Airborne and contact precautions
until lesions are crusted
Food employees
Health care workers
Attending or working
Child care facility
DisseminatedExclude until lesions are
crusted
Not Disseminated
Cover Lesions
Can’t cover lesions then
exclude104
Influenza – Control of Cases
▪ Droplet precautions for seven days
▪ Immunocompromised for duration of illness
▪ Home isolation for seven days
▪ Immunocompromised for duration of illness
▪ Unless seeking medical care
No regulations for contacts
105
Measles – Control of Cases
Airborne precautions for four days following rash
onset
Home isolation for four days following rash onset
▪ Except when seeking medical care
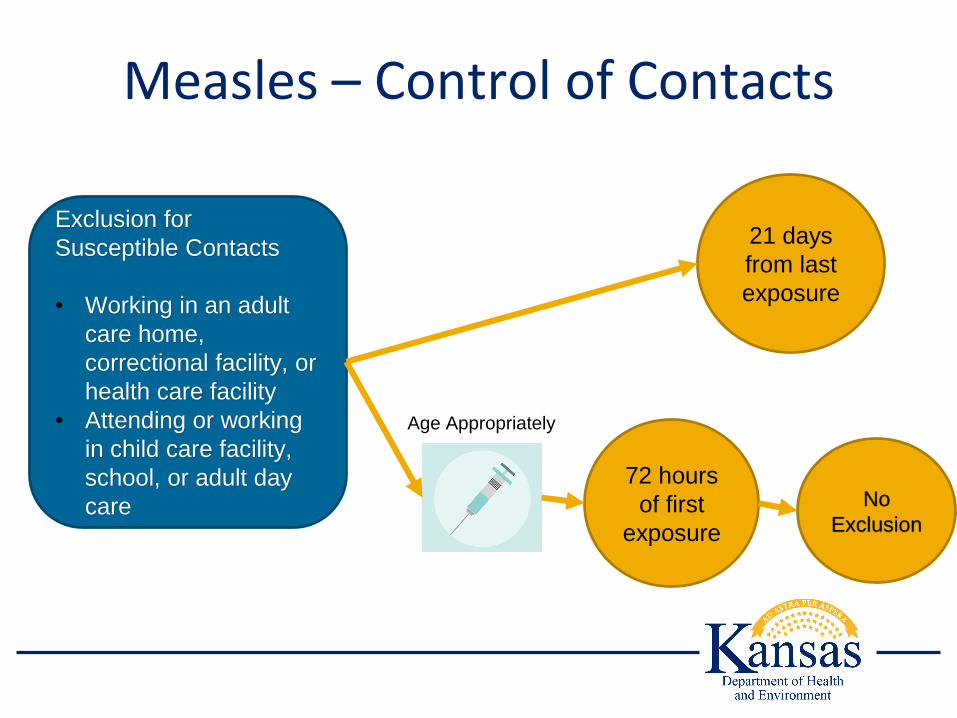
Measles – Control of Contacts
Exclusion for
Susceptible Contacts
• Working in an adult
care home,
correctional facility, or
health care facility
• Attending or working
in child care facility,
school, or adult day
care
21 days
from last
exposure
72 hours
of first
exposure
Age Appropriately
No
Exclusion
Measles - Scenarios

Measles in a Daycare
▪ An infant with suspected measles was reported to
KDHE within 4 hours
▪ There is considerable interaction between all the
children and staff at the daycare

Line list of Exposed Children and Staff
Child – 4 years
Child – 6
months
Child -
Kindergarten
Child -
Kindergarten
Child - 12
months
Child – 12
months
Child -
Kindergarten
1 MMR
No MMR
No MMR
2 MMR
No MMR
1 MMR
1 MMR
Exclude for 21 days
MMR within 72 hours
or Exclude for 21 days
No Exclusion
Recommend MMR; No
Exclusion
Exclude for 21 days
MMR within 72 hours
or Exclude for 21 days
No Exclusion
Staff – 25
years
2 MMR – Not
DocumentedTiters or Exclusion
Staff – 65
yearsUnknown
No Exclusion; born
before 1957
Measles in a Hospital
▪ An unvaccinated child was admitted to the
hospital with suspected measles
▪ The hospital reported this case to KDHE within 4
hours
▪ Three nurses and a physician were exposed
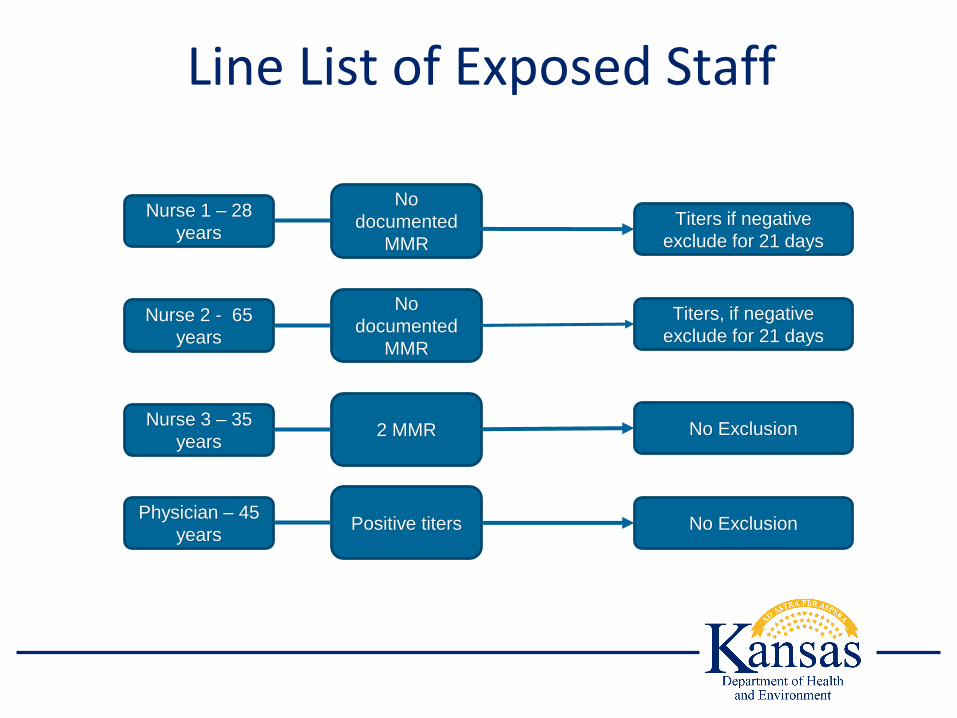
Line List of Exposed Staff
Physician – 45
years
Nurse 1 – 28
years
Nurse 2 - 65
years
Nurse 3 – 35
years
Positive titers
No
documented
MMR
No
documented
MMR
2 MMR
Titers if negative
exclude for 21 days
Titers, if negative
exclude for 21 days
No Exclusion
No Exclusion

Meningococcal Disease
▪ Droplet precautions until 24 hours after initiation of
antibiotic therapy
No regulation for non-hospitalized
persons or contacts

Mumps – Control of Cases
▪ Droplet precautions
▪ Nine days following onset of any symptom
▪ Five days after onset of parotitis
▪ In home isolation
▪ Nine days following onset of any symptom
▪ Five days following the onset of parotitis
▪ Except when seeking medical care
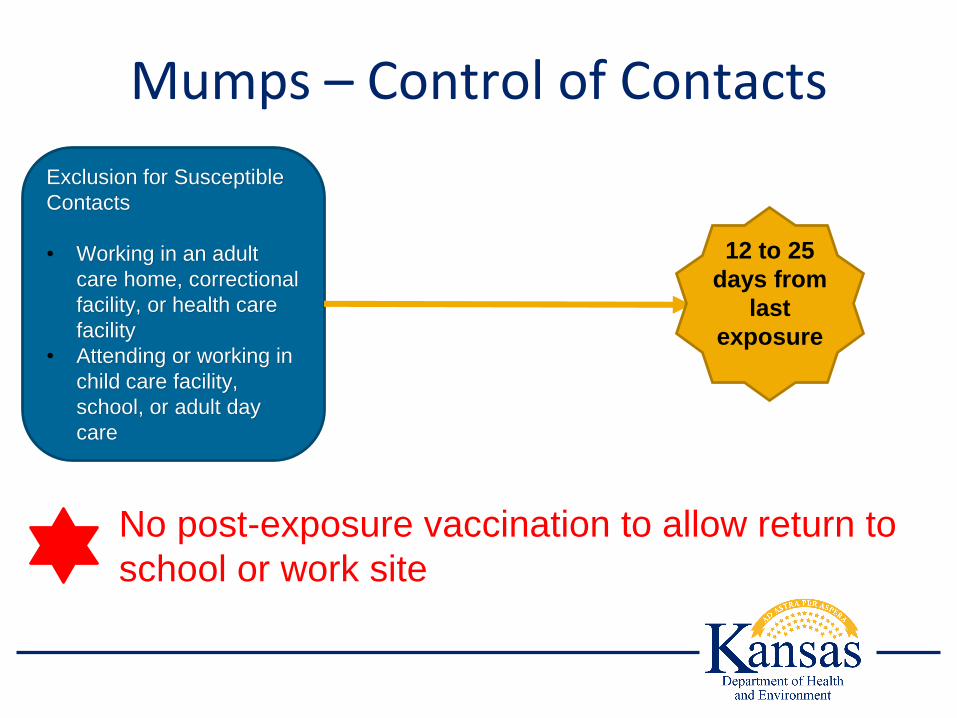
Mumps – Control of Contacts
No post-exposure vaccination to allow return to
school or work site
Exclusion for Susceptible
Contacts
• Working in an adult
care home, correctional
facility, or health care
facility
• Attending or working in
child care facility,
school, or adult day
care
12 to 25
days from
last
exposure

Mumps Scenario
Mumps in a School
▪ A 15 year old child was diagnosed with mumps
and KDHE was notified by telephone with 4 hours
▪ Exposed persons were identified
▪ One household contact that attends daycare
▪ Two student contacts in a classroom
▪ One teacher in a classroom
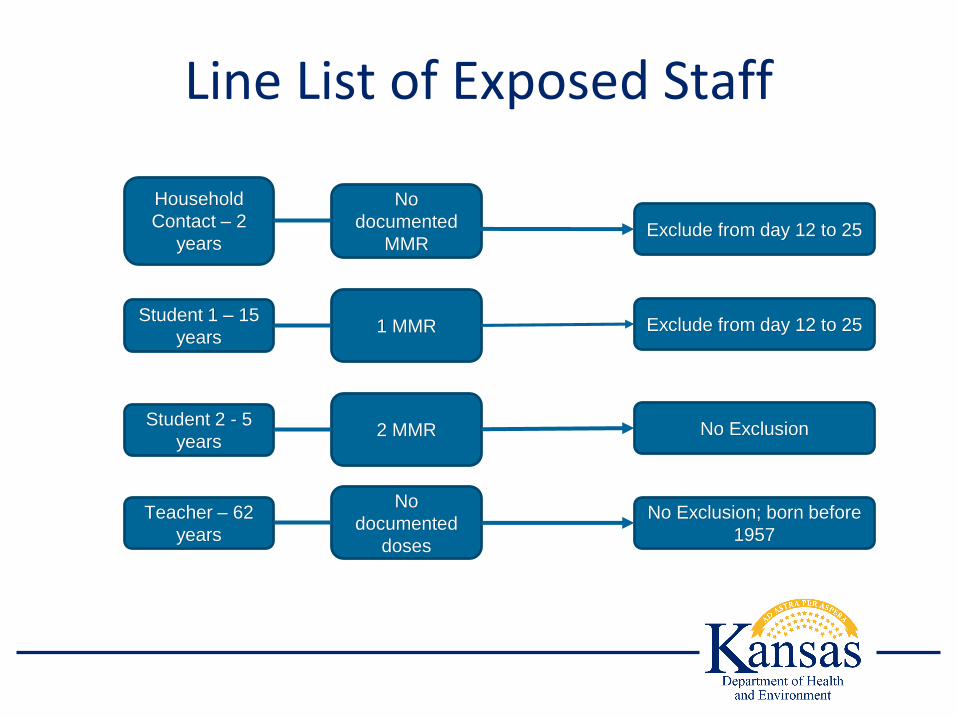
Line List of Exposed Staff
Teacher – 62
years
Household
Contact – 2
years
Student 1 – 15
years
Student 2 - 5
years
No
documented
doses
No
documented
MMR
1 MMR
2 MMR
Exclude from day 12 to 25
Exclude from day 12 to 25
No Exclusion
No Exclusion; born before
1957
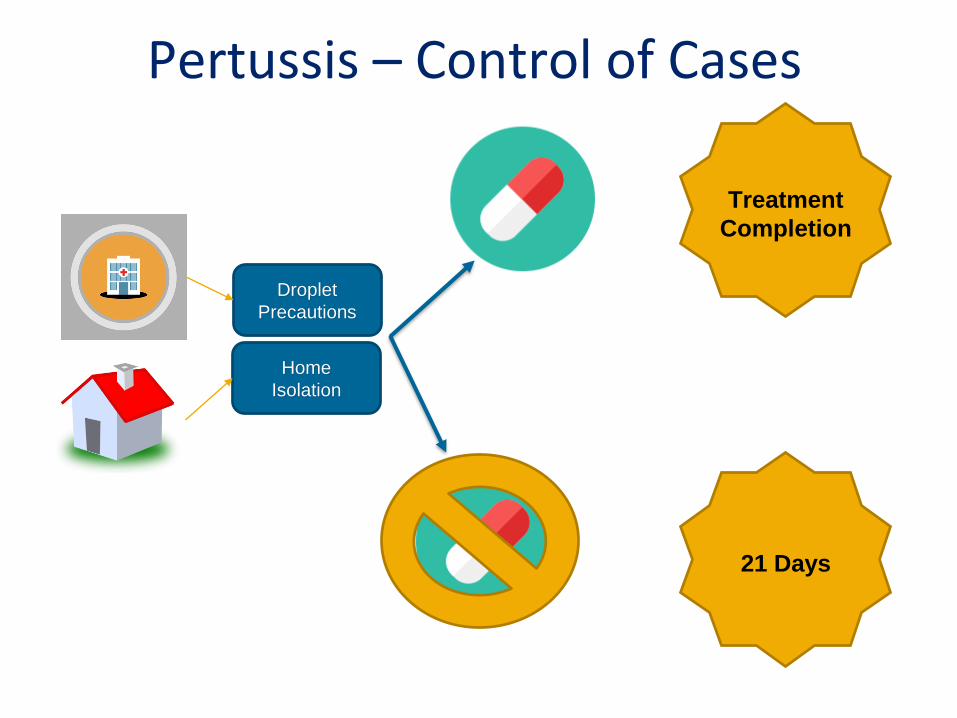
Pertussis – Control of Cases
Droplet
Precautions
Home
Isolation
21 Days
Treatment
Completion
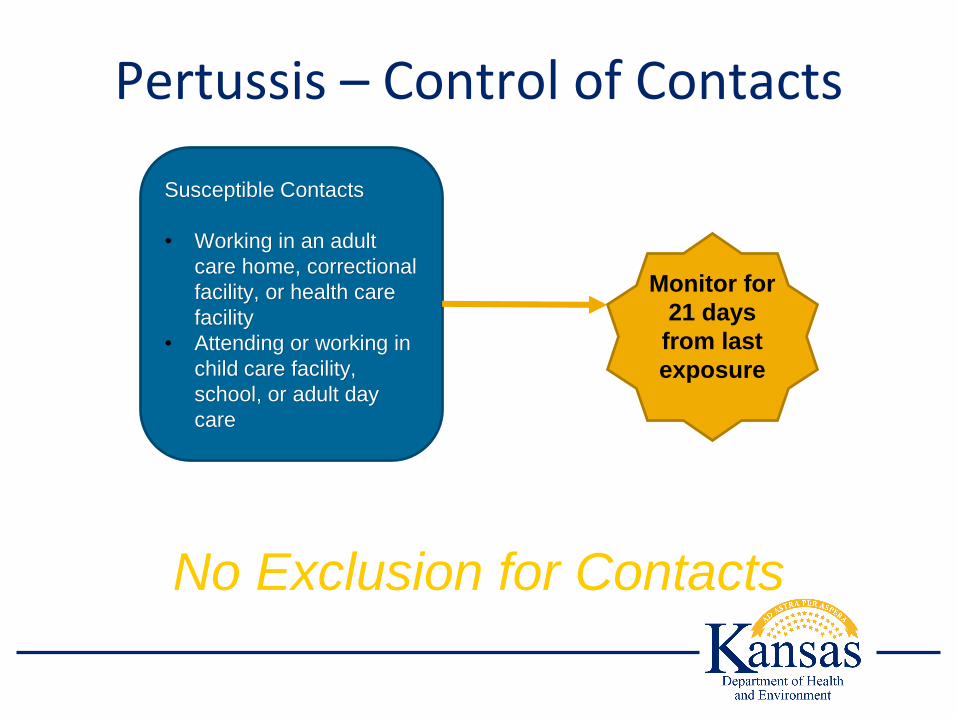
Pertussis – Control of Contacts
Susceptible Contacts
• Working in an adult
care home, correctional
facility, or health care
facility
• Attending or working in
child care facility,
school, or adult day
care
Monitor for
21 days
from last
exposure
No Exclusion for Contacts
Poliomyelitis – Control of Cases
▪ Contact precautions for duration of illness
No regulations for non-hospitalized
cases or contacts

Rubella – Control of Cases
Droplet precautions for seven days after onset of rash
In home isolation for seven days after onset of rash
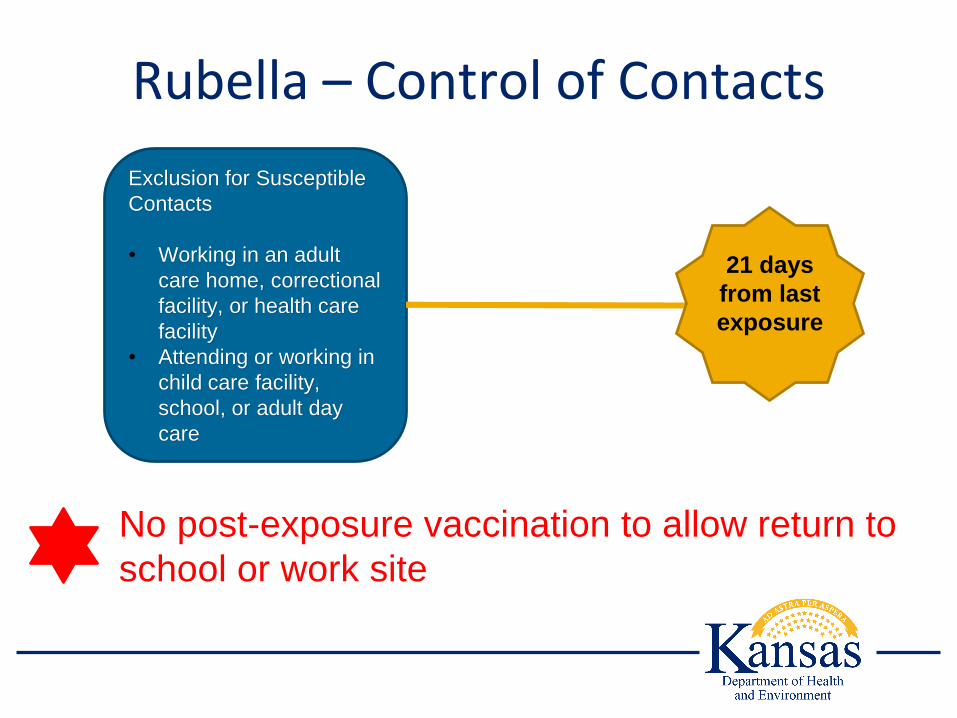
Rubella – Control of Contacts
No post-exposure vaccination to allow return to
school or work site
Exclusion for Susceptible
Contacts
• Working in an adult
care home, correctional
facility, or health care
facility
• Attending or working in
child care facility,
school, or adult day
care
21 days
from last
exposure
Varicella – Control of Cases
▪ Airborne precautions until vesicles are dry and
crusted or for six days following onset of rash
▪ Remain in home isolation until vesicles are dry and
crusted or for six days following onset of rash
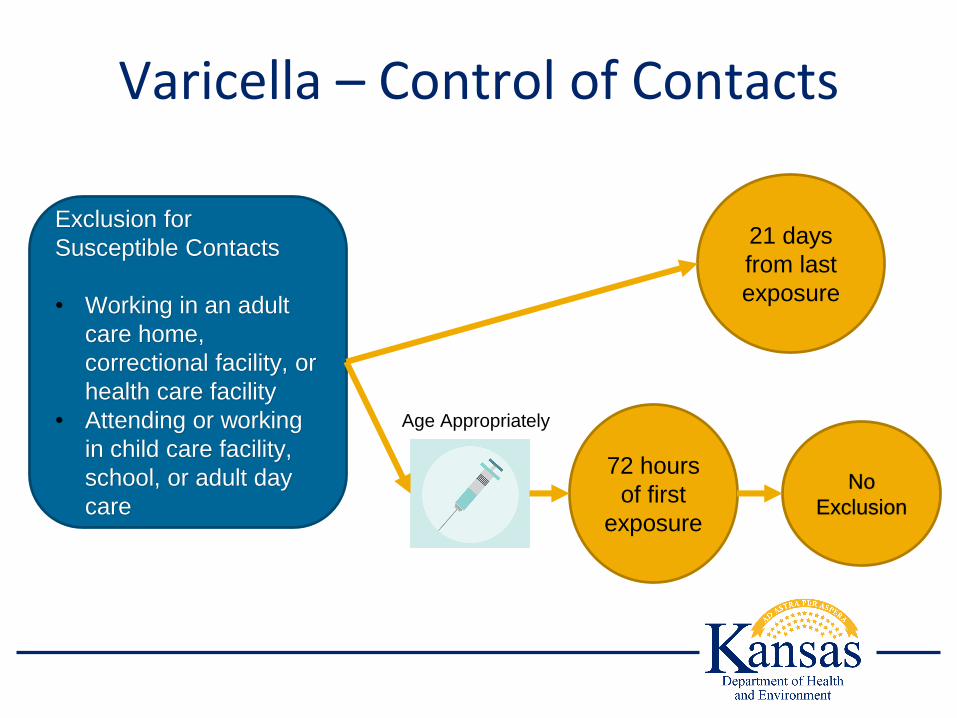
Varicella – Control of Contacts
Exclusion for
Susceptible Contacts
• Working in an adult
care home,
correctional facility, or
health care facility
• Attending or working
in child care facility,
school, or adult day
care
21 days
from last
exposure
72 hours
of first
exposure
Age Appropriately
No
Exclusion

Other Diseases
Pediculosis (head lice)
▪ No regulation
▪ CDC, American Academy of Pediatrics, and
National Association of School Nurses advocate
that children should not be excluded for lice or nits
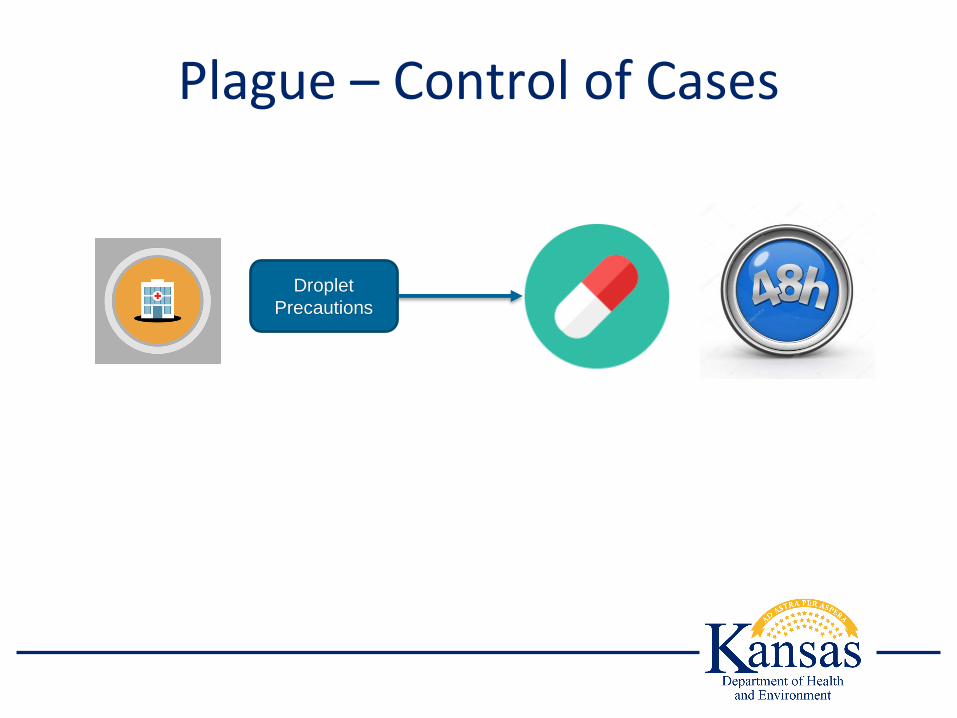
Plague – Control of Cases
Droplet
Precautions

Plague – Control of Cases
7
Days
No
Isolation
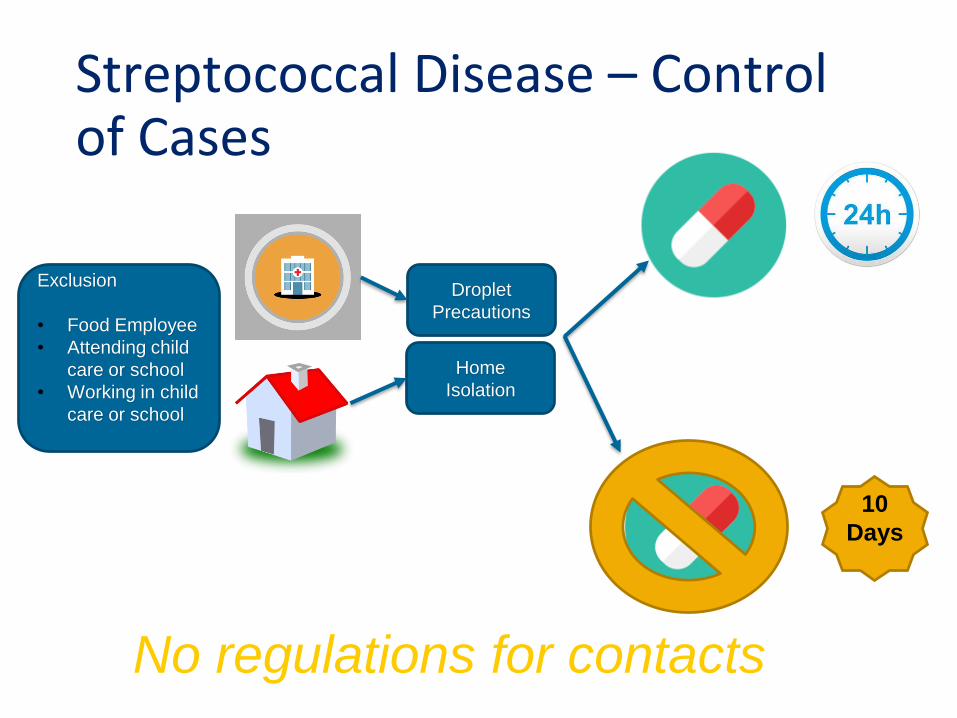
Streptococcal Disease – Control of Cases
Droplet
Precautions
Home
Isolation
Exclusion
• Food Employee
• Attending child
care or school
• Working in child
care or school
10
Days
No regulations for contacts
Vaccinia – Control of Cases
131
Contact precautions duration of acute illness
and lesions are dry and crusted
No regulation for non-hospitalized
persons or contacts

Viral hemorrhagic fevers
▪ Droplet precautions
▪ Airborne precautions if performing aerosol-
generating procedures
No regulation for non-hospitalized
persons or contacts

Discussion / Questions

















