The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, research- related, and evidence-based nursing materials. Take credit for all your work, not just books and journal articles. To learn more, visit www.nursingrepository.org Item type Presentation Format Text-based Document Title Changing Hospital Culture: Collaborative Response to Emergency Cesarean Sections Authors Schuch, Barbara C.; Krempel, Sally M. Downloaded 21-Jun-2018 23:30:58 Link to item http://hdl.handle.net/10755/603000
Transcript
The Henderson Repository is a free resource of the HonorSociety of Nursing, Sigma Theta Tau International. It isdedicated to the dissemination of nursing research, research-related, and evidence-based nursing materials. Take credit for allyour work, not just books and journal articles. To learn more,visit www.nursingrepository.org
Item type Presentation
Format Text-based Document
Title Changing Hospital Culture: Collaborative Response toEmergency Cesarean Sections
• Illinois Dept. of Public Health (IDPH) Visit January 2012
• Decision to Incision time for Emergency Cesarean Sections-“30-Minute Rule”
• American College of Obstetrics & Gynecology (ACOG) Standard of Care
• Data Collection
• Gap Analysis
1. All Birth Center Staff not using Standardized Nomenclature
2. Perceived Lack of Communication & Teamwork
Continuing Education
• Departmental process improvement project
• Planned for interprofessional groups
• The group planned 2.0 CNE through the Ohio
Nurse’s Association (ONA) & 1.0 CME through the
hospital’s CME Coordinator
• 9 classes were held for OB physicians,
anesthesiologists, residents, APNs, Birth Center
nursing staff, OBTs, PCTs, medical and nursing
students were presented
IOM Report
• “At least 44,000 people, and perhaps as many as 98,000 people, die in hospitals each year as a result of medical errors that could have been prevented, according to estimates from two major studies.”
Erockson, L., & Daniels, K., (2012). Simulation-based team training on obstetric emergencies. Contemporaryobgyn.net, 5.
• Bloom, S., Leveno, K., Spong, C., Gilbert, s., Hauth, J., Landon, M., Gabbe, S. (2006). Decision-to-incision times and maternal and infant outcomes. Obstetrics & Gynecology, 108(1), 6-11.
• Daniel, L.T., & Simpson, E.K. (2009). Integrating team training strategies into obstetrical emergency simulation training. Journal for Healthcare Quality, 31 (5), 38-42.
• Elmir, R., Schmied, V., Wilkes, L. & Jackson, D. (2010). Women’s perceptions and experiences of a traumatic birth: A meta-ethnography. Journal of Advanced Nursing, 66(10), 2142-2153. doi:10.1111/j.1365-2648.2010.05391.x
• Gum, l.., Greenhill, J., & Dix, K., (2010). Clinical simulation in maternity (CSiM):Interprofessional learning through simulation team training, Quality and Safety in Health
Care, doi: 10.1136/qshc.2008.030767.
• IOM Report; “To Err is Human: Building a Safer Health System,” November 1999.
References, (cont’d)
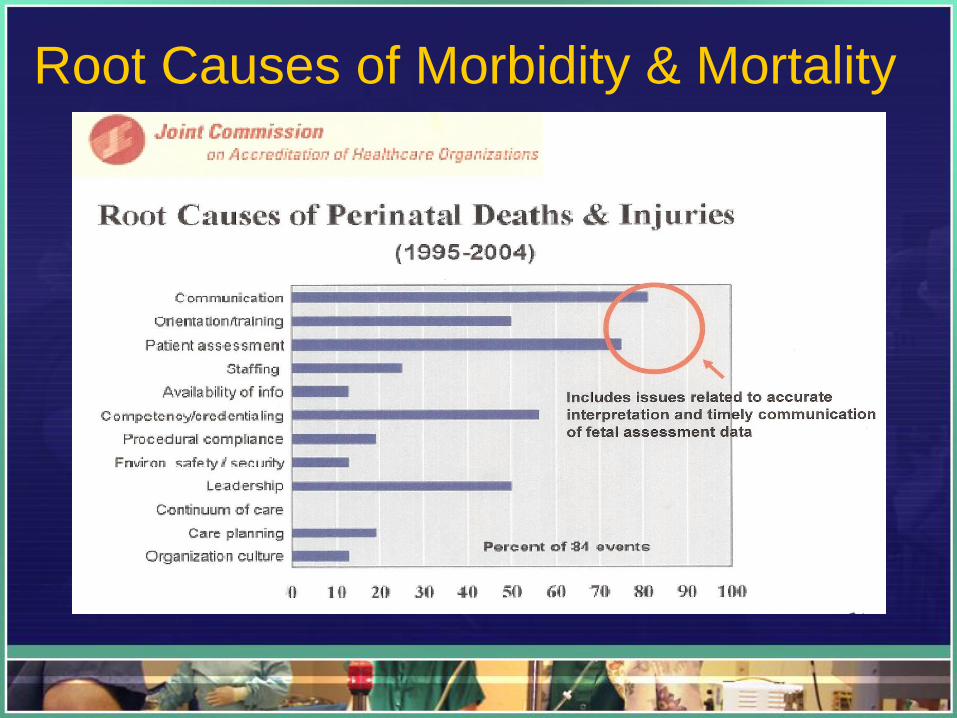
• Joint Commission on Accreditation of Healthcare Organizations Sentinel Event Alert. Oak Brook. Ill (2004). Joint Commission on Accreditation of Healthcare Organizations, Issue No.3
• Martinez-Biarge, M., Madero R., Gonzalez, A., Quero, J., & Garcia-Alix, A. (2012) Perinatal morbidity and risk of hypoxic-ischemic encephalopathy associated with intrapartum sentinel events. American Journal of Obstetrics & Gynecology, 148, e1-7. doi: 10.1016/j.ajog.2011.09.031. Epub 2011 Oct 6.
• Miller, David, A. (2011). A reasoned plan to manage a persistent category-II FHR tracing. OBG
Management, (23)12, 30-35, & 49.
• NCC Monograph, (2010). NICHD definitions and classifications: Application to electronic fetal monitoring interpretation. National Certification Corporation.
• Redshaw, M. & Hockley, C. (2010). Institutional processes and individual responses: Women’s experiences of care in relation to cesarean birth. Birth: Issues in Perinatal Care, 37(2), 150-159. doi:10.1111/j.1523-536X.2010.00395.x
References, (cont’d)
• Rice, K.S., (2004). Standardized language for electronic fetal heart rate