LievreLievre------------------------------------------------------------------------------------------------------------------------------------------------epidural with corticosteroidepidural with corticosteroid
..The mechanism that allows local The mechanism that allows local anesthetics to provide anesthetics to provide pain reliefpain relief is is the reversible neural blockadethe reversible neural blockade……
Corticosteroids have been utilized for treatment of Corticosteroids have been utilized for treatment of
musculoskeletal painmusculoskeletal pain because of their because of their antiinflammatory antiinflammatory properties……………………………………………….properties……………………………………………….
They have also been reported to have a direct They have also been reported to have a direct membrane-stabilizing effect, which leads to membrane-stabilizing effect, which leads to decreased afferent ectopic discharges at the neural decreased afferent ectopic discharges at the neural membrane…………..membrane…………..
There is a reversible inhibition of There is a reversible inhibition of nociceptive nociceptive CC-fiber transmission with local -fiber transmission with local application of corticosteroids.there has application of corticosteroids.there has been no demonstration of been no demonstration of AAororBB fiber fiber transmission interruption………………..transmission interruption………………..
Corticosteroids have a modulation effect Corticosteroids have a modulation effect on spinal cord……………………….on spinal cord……………………….
Skin hypopigmentationSkin hypopigmentation,,subcutaneous fat subcutaneous fat atrophyatrophy,,tendon rupturetendon rupture,,fluid retentionfluid retention, , flushingflushing,,hyperglycemiahyperglycemia,,change in tastechange in taste,, insomniainsomnia,,malaise and malaise and dyspepsiadyspepsia………………………………………… …………………………………………
Systemic suppression of the adrenal glands Systemic suppression of the adrenal glands can happen after a local injection of can happen after a local injection of corticosteroids into any structurecorticosteroids into any structure………………
Repeated injections of corticosteroids can lead to Repeated injections of corticosteroids can lead to a cushingoid appearancea cushingoid appearance…………….…………….
Non-ionic contrast agents include Non-ionic contrast agents include metrizamidemetrizamide ((AmnipaqueAmnipaque), ), iopamidoliopamidol ((IsovueIsovue), and), and iohexoliohexol ((OmnipaqueOmnipaque))……………. …………….
These are used in conjunction with These are used in conjunction with fluoroscopyfluoroscopy for needle for needle tip localization in performing spinal injection procedures tip localization in performing spinal injection procedures and some peripheral joint injections………………..and some peripheral joint injections………………..
The use of contrast significantly reduces the risk The use of contrast significantly reduces the risk of an unintended injection into a vascular areaof an unintended injection into a vascular area, , blood vessel blood vessel oror subarachnoid space……………… subarachnoid space………………
The The adverse effectsadverse effects that can result from the use of contrast that can result from the use of contrast agents are due to agents are due to local tissue toxicitylocal tissue toxicity and to and to anaphylaxisanaphylaxis……………………………………………………..……………………………………………………..
Greater than 90% of adverse reactions occur within the first Greater than 90% of adverse reactions occur within the first 15 15 min…………………………………………………….min…………………………………………………….
other side effects :other side effects :nauseanausea,, headache headache, and , and emesisemesis…..….. Pretreatment is recommended with steroids and Pretreatment is recommended with steroids and
antihistaminesantihistamines 12 h, 12 h, and again atand again at 2 h, 2 h, prior to the prior to the procedure in patients with an allergic reaction procedure in patients with an allergic reaction history……………….history……………….
GadoliniumGadolinium is a viable alternative for is a viable alternative for patients with contrast material allergies, patients with contrast material allergies, and provides adequate visualization for and provides adequate visualization for spinal injection spinal injection procedures………………………procedures………………………
GENERAL CONSIDERATIONSGENERAL CONSIDERATIONS Answer all questions. provide the patient with a Answer all questions. provide the patient with a
clear explanation of the risks and clear explanation of the risks and benefits……………………………………………… benefits………………………………………………
Caution should always be used to avoid the risk Caution should always be used to avoid the risk of bleeding. Patients using of bleeding. Patients using aspirinaspirin should should discontinue it for at least discontinue it for at least 7 7 days. If patients days. If patients cannot tolerate being off aspirin, a cannot tolerate being off aspirin, a non-selective non-selective NSAIDNSAID can be substituted for at least the can be substituted for at least the 3 3 days days prior to any injection… prior to any injection…
Women who are pregnant or suspected to be Women who are pregnant or suspected to be pregnant should avoid radiation exposure from pregnant should avoid radiation exposure from fluoroscopyfluoroscopy………………….………………….
The patient is properly positioned on the The patient is properly positioned on the procedure table before beginning the procedure table before beginning the injection………………………………………………… injection…………………………………………………
Prepare and drape the injection site in a sterile Prepare and drape the injection site in a sterile manner with manner with povidone-iodine povidone-iodine ((BetadineBetadine),), chlorhexidine gluconatechlorhexidine gluconate ( (HibiclensHibiclens), and/or ), and/or isopropyl alcoholisopropyl alcohol…………. ………….
Sterile glovesSterile gloves are worn during the injection are worn during the injection procedure………………………………….procedure………………………………….
GownGown, , capcap, and , and maskmask are used when performing are used when performing myelographymyelography and and diskographydiskography…. ….
IntravenousIntravenous or or oral antibioticsoral antibiotics are used are used when performing injection procedures in when performing injection procedures in patients with patients with implanted prosthetic devicesimplanted prosthetic devices or with a history of or with a history of mitral valve mitral valve prolapse…….prolapse…….
The injection site can be anesthetized for The injection site can be anesthetized for patient comfort with a patient comfort with a vapocoolant sprayvapocoolant spray OR OR anesthetic creamanesthetic cream prior to prior to injection…………………. injection………………….
The needle is always The needle is always aspirated aspirated via the syringe via the syringe before the injection to avoid an intravascular or, before the injection to avoid an intravascular or, in the case of some spinal procedures, an in the case of some spinal procedures, an intrathecal injection…………intrathecal injection…………
Avoid injecting into a ligament, a tendon, Avoid injecting into a ligament, a tendon, or the periosteumor the periosteum.. This means repositioning This means repositioning the needle if there is significant the needle if there is significant resistance………………………………resistance………………………………
Avoid needle contact with articular Avoid needle contact with articular cartilage surfaces during joint cartilage surfaces during joint injectionsinjections…………………………………………..…………………………………………..
The injection is given The injection is given slowlyslowly, with , with steady steady pressurepressure…………..…………..
A A dressingdressing is applied to the injection site after is applied to the injection site after the injection is completed……….the injection is completed……….
The patient is encouraged to rest the area The patient is encouraged to rest the area after the injection for several days, after the injection for several days, especially if it is a major weight-bearing especially if it is a major weight-bearing joint……………joint……………
All patients should be driven home and should All patients should be driven home and should not drive for the nextnot drive for the next……………………
Chronic infection distant from the injectionChronic infection distant from the injection****
Allergy to the injection solution Allergy to the injection solution ****
Latex allergy Latex allergy ****
Diabetes mellitus Diabetes mellitus ****
Allergy to contrast agents for fluoroscopically Allergy to contrast agents for fluoroscopically ****
Altered anatomy( surgery or congenital ) Altered anatomy( surgery or congenital ) ****
TendonsTendons and and ligamentsligaments can be can be ruptured if corticosteroids are ruptured if corticosteroids are injected directly into them injected directly into them ((this is this is estimated to occur in less thanestimated to occur in less than 1%1% of such of such casescases))…………………………..…………………………..
Patients requiring anticoagulation medication Patients requiring anticoagulation medication or with a known bleeding diathesis should be or with a known bleeding diathesis should be approached with a great deal of approached with a great deal of caution…………………………..caution…………………………..
Coagulation parameters should be evaluated Coagulation parameters should be evaluated in these cases, including : in these cases, including : prothrombin prothrombin timetime,,,,,,,,activated partial activated partial thromboplastin timethromboplastin time,,,, ,,,, international international normalized ratio normalized ratio ((INRINR) and) and platelet platelet level countlevel count…… ……
Injections should be avoided with Injections should be avoided with prolonged bleeding timesprolonged bleeding times, an , an INRINR greater than greater than 1.21.2 and a platelet and a platelet count of less than count of less than 100 000100 000 per per ml…….ml…….
EFFICACYEFFICACY
Improvement in rheumatoid synovitis Improvement in rheumatoid synovitis has been seen to last for as long as has been seen to last for as long as 33 months after injecting months after injecting glucocorticoids, with improvement in glucocorticoids, with improvement in painpain and in and in knee extensor knee extensor strength……………………………………. strength…………………………………….
intraarticular injections of intraarticular injections of hyaluronanhyaluronan ((hyaluronic acid,,,,,, hyaluronic acid,,,,,, hyaluronatehyaluronate)) were more effective were more effective than placebo in reducing than placebo in reducing painpain and and improving improving joint functionjoint function from from osteoarthritis of the knee……………osteoarthritis of the knee……………
A small randomized controlled trial A small randomized controlled trial found no significant difference found no significant difference between intraarticular injections of between intraarticular injections of methylprednisolone plus lidocaine methylprednisolone plus lidocaine ((lignocainelignocaine)) versus versus lidocaine alonelidocaine alone for the treatment of shoulder pain, for the treatment of shoulder pain, although there was a although there was a small small improvement in pain and range of improvement in pain and range of motion in both groups at 24 motion in both groups at 24 weeks………………………………. weeks……………………………….
Acromioclavicular jointAcromioclavicular joint
The injection is performed with the The injection is performed with the patient in the seated position with patient in the seated position with the upper limb resting the upper limb resting comfortably……………………………….comfortably……………………………….
The acromioclavicular joint is located The acromioclavicular joint is located at a depressed and soft region distal at a depressed and soft region distal to the end of the to the end of the clavicle……………………………………..clavicle……………………………………..
The injection site is The injection site is anterior anterior and and superiorsuperior to acromioclavicular joint to acromioclavicular joint ………………………………………………………………………………
The needle is then advanced The needle is then advanced inferiorly into the joint……………..inferiorly into the joint……………..
Glenohumeral jointGlenohumeral joint
The glenohumeral joint is typically The glenohumeral joint is typically injected from either an anterior or a injected from either an anterior or a posterior approach……………………… posterior approach………………………
In the In the anterior approachanterior approach, a needle is , a needle is inserted lateral to the coracoid process inserted lateral to the coracoid process while avoiding the thoracoacromial while avoiding the thoracoacromial artery .The needle is then directed artery .The needle is then directed dorsally and medially into the joint dorsally and medially into the joint space………… space…………
The posterior approachThe posterior approach is set up by is set up by placing the patient's hand across the placing the patient's hand across the chest on the opposite shoulder. The chest on the opposite shoulder. The needle is inserted needle is inserted 2-32-3 cm below the cm below the posterolateral aspect of the acromion. posterolateral aspect of the acromion. The needle is then advanced toward The needle is then advanced toward the coracoid process in an anterior the coracoid process in an anterior and medial direction into the joint.and medial direction into the joint.
Subacromial bursaSubacromial bursa
The subacromial bursa lies above the The subacromial bursa lies above the supraspinatus tendon and under the supraspinatus tendon and under the acromion……………………………………………..acromion……………………………………………..
A A posterolateral approachposterolateral approach is used to place is used to place the needle into the subacromial space.The the needle into the subacromial space.The needle is inserted underneath the palpable needle is inserted underneath the palpable posterolateral cornerof the acromion and posterolateral cornerof the acromion and advanced toward the coracoid process,which advanced toward the coracoid process,which places the needle tip under the places the needle tip under the acromion………………………….acromion………………………….
Ulnohumeral(elbow)jointUlnohumeral(elbow)joint
The elbow joint consists of three articulations The elbow joint consists of three articulations between the between the humerushumerus, , ulnaulna and and radiusradius, with , with the true elbow joint formed by the humerus the true elbow joint formed by the humerus and ulna………….and ulna………….
Injection of the ulnohumeral joint is Injection of the ulnohumeral joint is
accomplished from a accomplished from a posterolateralposterolateral or or
posteriorposterior approach with the elbow flexed approach with the elbow flexed between 50 and 90°………………….. between 50 and 90°…………………..
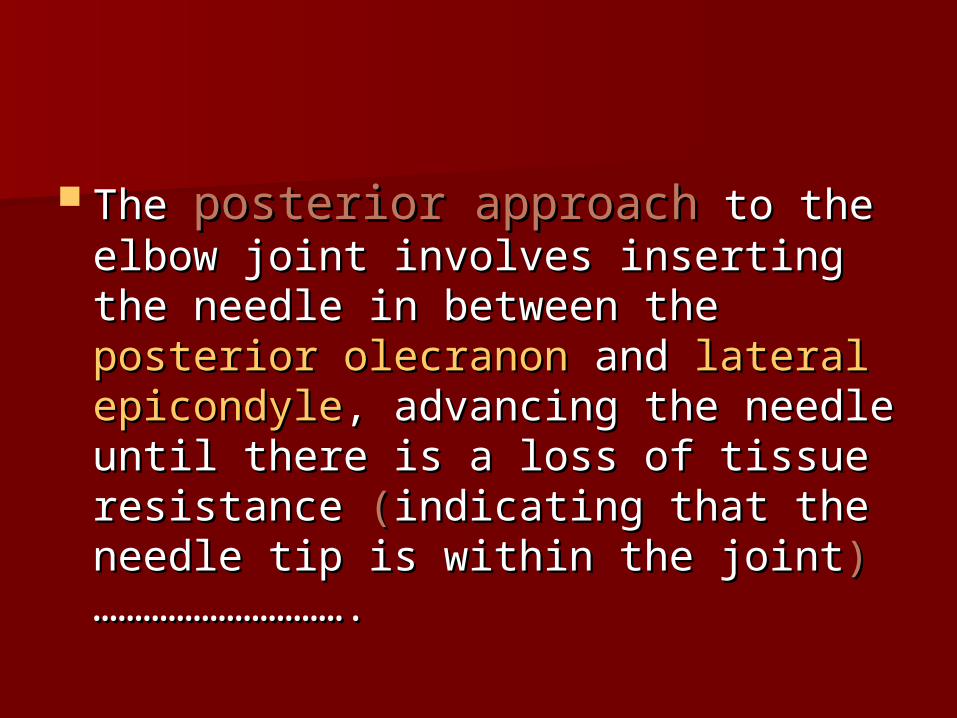
In In posterolateral approachposterolateral approach, the needle is , the needle is inserted in the posterolateral triangle formed inserted in the posterolateral triangle formed by the palpable by the palpable olecranonolecranon, , lateral epicondylelateral epicondyle and and radial headradial head ……………………………………………………………………………………………………
The needle is directed medially away from The needle is directed medially away from the ulnar nerve and proximally toward the the ulnar nerve and proximally toward the head of the radius. A lack of resistance head of the radius. A lack of resistance indicates entry of the needle tip into the indicates entry of the needle tip into the joint…………………………………. joint………………………………….
The The posterior approachposterior approach to the to the elbow joint involves inserting the elbow joint involves inserting the needle in between the needle in between the posterior posterior olecranonolecranon and and lateral epicondylelateral epicondyle, , advancing the needle until there is a advancing the needle until there is a loss of tissue resistance loss of tissue resistance ((indicating indicating that the needle tip is within the jointthat the needle tip is within the joint))………………………….………………………….
Medial and lateral epicondyleMedial and lateral epicondyle
Medial epicondylitis Medial epicondylitis or or 'golfer's 'golfer's elbowelbow', results from ', results from tendonosistendonosis or or degenerativedegenerative changes at the tendon changes at the tendon attachment of the wrist flexor and pronator attachment of the wrist flexor and pronator muscle groups. The elbow is positioned in muscle groups. The elbow is positioned in abduction,with the forearm in supination.A abduction,with the forearm in supination.A needle is inserted at the site of tenderness needle is inserted at the site of tenderness along the medial epicondyle and advanced along the medial epicondyle and advanced until there is contact with the periosteum.The until there is contact with the periosteum.The needle is slightly withdrawn before the needle is slightly withdrawn before the injection……………injection……………
Lateral epicondylitisLateral epicondylitis or or 'tennis 'tennis elbow',elbow', is a tendonosis from is a tendonosis from repetitive wrist extension and repetitive wrist extension and forearm supination. The elbow is forearm supination. The elbow is flexed to 45° and the forearm is flexed to 45° and the forearm is placed in pronation. A needle is placed in pronation. A needle is inserted at the point of tenderness inserted at the point of tenderness along the lateral epicondyle and along the lateral epicondyle and advanced to the periosteum……….. advanced to the periosteum………..
Olecranon bursaOlecranon bursa
Olecranon bursitis Olecranon bursitis or or 'draftsman's 'draftsman's elbowelbow', occurs in RA, crystal arthropathies, ', occurs in RA, crystal arthropathies, and repetitive trauma. The needle is directed and repetitive trauma. The needle is directed toward the olecranon bursa, which is toward the olecranon bursa, which is superficial to the olecranon and external to superficial to the olecranon and external to the elbow joint ………………….the elbow joint ………………….
Injection of the olecranon bursa should be Injection of the olecranon bursa should be preceded with preceded with aspirationaspiration and and no no corticosteroids should be injected if there is a corticosteroids should be injected if there is a purulent dischargepurulent discharge……………….……………….
Carpal tunnelCarpal tunnel
Injection of the carpal tunnel can be Injection of the carpal tunnel can be approached inapproached in ulnarulnar or or radial radial orientation, orientation, based on positioning relative to the based on positioning relative to the palmaris longus palmaris longus tendon…………………………………………..tendon…………………………………………..
The ulnarThe ulnar approach is preferredapproach is preferred. it is less . it is less likely to injure the median nerve during likely to injure the median nerve during the injection. the injection. The wrist can be flexed to The wrist can be flexed to increase the prominence of the palmaris increase the prominence of the palmaris longus tendon……………. longus tendon…………….
A needle is inserted with the wrist in a A needle is inserted with the wrist in a neutral position at a neutral position at a 30°30° angle ulnar to angle ulnar to the palmaris longus tendon at the distal the palmaris longus tendon at the distal wrist crease .The needle is then advanced wrist crease .The needle is then advanced in a distal and radial direction underneath in a distal and radial direction underneath the transverse carpal ligament. the transverse carpal ligament. The needle The needle is withdrawn if paresthesias are is withdrawn if paresthesias are experienced during the insertion, and experienced during the insertion, and redirected within the tunnel……..redirected within the tunnel……..
Abductor and extensor pollicis Abductor and extensor pollicis tendontendon
De Quervain's tenosynovitisDe Quervain's tenosynovitis is an is an inflammatory disorder of the wrist involving inflammatory disorder of the wrist involving the the abductor pollicis longusabductor pollicis longus and and extensor extensor pollicis brevispollicis brevis tendons. The needle is placed tendons. The needle is placed 1cm1cm proximal to the styloid process at a proximal to the styloid process at a 45°45°angle to the forearm alongside either angle to the forearm alongside either tendon …………tendon …………
The needle is repositioned before the The needle is repositioned before the injection if there are any paresthesias injection if there are any paresthesias encountered from the radial nerve during encountered from the radial nerve during needle insertion………………………needle insertion………………………
Greater trochanter and ischial Greater trochanter and ischial bursaebursae
The patient is placed in the The patient is placed in the lateral lateral decubitusdecubitus position, with the affected position, with the affected hip uprighthip upright and the and the knees flexedknees flexed to to relax the hamstrings…….. relax the hamstrings……..
The lateral hip and inferior buttock The lateral hip and inferior buttock areas are palpated for the point of areas are palpated for the point of greatest tenderness over the greater greatest tenderness over the greater trochanter and the ischial tuberosity, trochanter and the ischial tuberosity, respectively……………… respectively………………
For both injection procedures, the For both injection procedures, the needle is inserted through the skin needle is inserted through the skin and advanced until contact is made and advanced until contact is made with the with the periosteum…………………………….. periosteum……………………………..
The needle is then slightly withdrawn The needle is then slightly withdrawn so that the tip lies within the so that the tip lies within the bursa………………………bursa………………………
Hip jointHip joint
Intraarticular injections of the hip joint require Intraarticular injections of the hip joint require fluoroscopic guidance and contrast fluoroscopic guidance and contrast enhancement, whether using a enhancement, whether using a lateral lateral or an or an anterior anterior approach. approach. Anterior approachAnterior approach, the , the patient is placed in the patient is placed in the supinesupine position with position with the lower limb in the lower limb in external rotationexternal rotation. The . The needle is inserted at a site just inferior to the needle is inserted at a site just inferior to the mid trochanteric mid trochanteric line………………………………… line…………………………………
The needle is inserted at a site just The needle is inserted at a site just inferior to the mid trochanteric line. inferior to the mid trochanteric line. The needle is inserted The needle is inserted 45°45° toward toward the femoral neck, and advanced the femoral neck, and advanced under fluoroscopic guidance through under fluoroscopic guidance through the capsule until contact with the the capsule until contact with the periosteum…………………………………periosteum…………………………………....
Knee jointKnee joint The knee joint is the most common joint site The knee joint is the most common joint site
for both injection and aspiration. There are for both injection and aspiration. There are three possible approaches: three possible approaches: medialmedial, , laterallateral, , and and anterioranterior. The patient is positioned supine . The patient is positioned supine for aspiration, with the knee fully extended or for aspiration, with the knee fully extended or slightly flexed. The superior medial or slightly flexed. The superior medial or superior lateral approaches are generally held superior lateral approaches are generally held to be the best for arthrocentesis…………….. to be the best for arthrocentesis……………..
The The patellapatella is located by palpation and is the is located by palpation and is the main landmark for localizing the entry main landmark for localizing the entry site…………………………………………… site……………………………………………
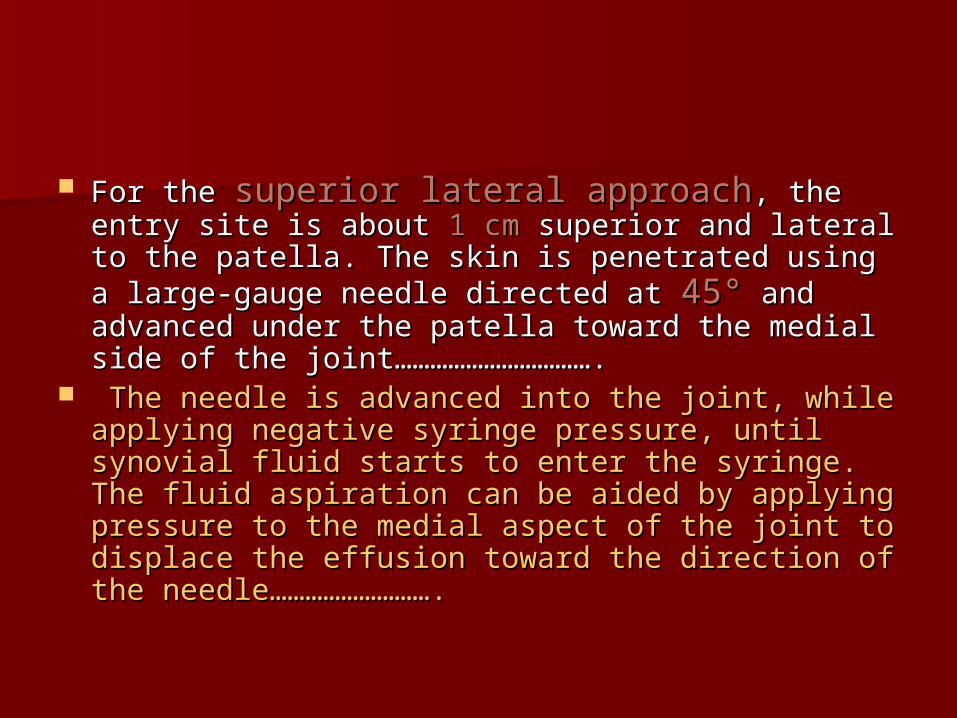
For the For the superior lateral approachsuperior lateral approach, the entry , the entry site is about site is about 1 cm1 cm superior and lateral to the superior and lateral to the patella. The skin is penetrated using a large-patella. The skin is penetrated using a large-gauge needle directed at gauge needle directed at 45°45° and advanced and advanced under the patella toward the medial side of the under the patella toward the medial side of the joint…………………………….joint…………………………….
The needle is advanced into the joint, while The needle is advanced into the joint, while applying negative syringe pressure, until synovial applying negative syringe pressure, until synovial fluid starts to enter the syringe. The fluid fluid starts to enter the syringe. The fluid aspiration can be aided by applying pressure to aspiration can be aided by applying pressure to the medial aspect of the joint to displace the the medial aspect of the joint to displace the effusion toward the direction of the effusion toward the direction of the needle……………………….needle……………………….
For the For the superior medial approachsuperior medial approach, , needle entry is needle entry is 1 cm1 cm superior and superior and medial to the patella………………….. medial to the patella…………………..
The needle is directed under the The needle is directed under the patella and advanced toward the patella and advanced toward the opposite patella midpole, midway opposite patella midpole, midway between the medial border of the between the medial border of the patella and the femur…………………. patella and the femur………………….
The advantage of the The advantage of the anterior anterior approachapproach is greater ease of entry is greater ease of entry into knees with into knees with advanced advanced osteoarthritisosteoarthritis, as well as for patients , as well as for patients who who cannot fully extendcannot fully extend their their knees………………………………… knees…………………………………
The downside to this approach is a The downside to this approach is a greater risk for meniscal and greater risk for meniscal and articular cartilage injury……………..articular cartilage injury……………..
For injections of corticosteroids without For injections of corticosteroids without synovial fluid aspiration, the patient is synovial fluid aspiration, the patient is positioned as described or with positioned as described or with 90°90° of of knee knee flexionflexion………………………………………. ……………………………………….
The entry site for injection with the knee in The entry site for injection with the knee in the flexed position can be on either the the flexed position can be on either the medial or the lateral aspect of the patellar medial or the lateral aspect of the patellar tendon…………………………….. tendon……………………………..
The joint is entered inferior to the patella, The joint is entered inferior to the patella, using a needle directed superiorly toward the using a needle directed superiorly toward the intercondylar intercondylar notch…………………………………………………notch…………………………………………………
The inferior medial approach is The inferior medial approach is technically easier for injection than technically easier for injection than the lateral approach if the patient the lateral approach if the patient can only slightly flex the can only slightly flex the knee………………………………………….knee………………………………………….
pes anserine bursapes anserine bursa
The The pes anserine bursapes anserine bursa is located between is located between the medial collateral ligament and the the medial collateral ligament and the confluence of the confluence of the sartoriussartorius, , gracilisgracilis, and , and semi-tendinosus semi-tendinosus tendon insertion at the tendon insertion at the proximal medial tibia just distal to the joint proximal medial tibia just distal to the joint line………………………………….. line…………………………………..
A needle is inserted at the site of greatest A needle is inserted at the site of greatest palpable tenderness perpendicular to the palpable tenderness perpendicular to the tibia, and advanced until contact is made tibia, and advanced until contact is made with the with the periosteum……………………………… periosteum………………………………
prepatella bursaeprepatella bursae
The prepatellar bursa is located between the The prepatellar bursa is located between the skin and the anterior surface of the patella. skin and the anterior surface of the patella. The needle is inserted at the The needle is inserted at the midportion of midportion of the superior patellar polethe superior patellar pole………………………….………………………….
The bursa can be significant is size from The bursa can be significant is size from inflammation, which often allows for fluid inflammation, which often allows for fluid aspiration that can be aided by direct aspiration that can be aided by direct pressure over the patella before pressure over the patella before injection…………………………………………….injection…………………………………………….
ANKLE JOINTANKLE JOINT
The ankle joint is formed by the The ankle joint is formed by the tibia tibia andand talus talus (tibiotalar mortise), and is not one of the (tibiotalar mortise), and is not one of the more commonly injected more commonly injected joints………………………………………………… joints…………………………………………………
The main indication for injecting the ankle is The main indication for injecting the ankle is for for pain secondary to pain secondary to osteoarthritisosteoarthritis…………………………………..…………………………………..
The two approaches for performing an ankle The two approaches for performing an ankle joint injection are the joint injection are the anterior medialanterior medial and and anterior lateralanterior lateral……………...……………...
The talus is palpated with the foot in The talus is palpated with the foot in the neutral position. A horizontal line the neutral position. A horizontal line can be drawn between the medial can be drawn between the medial and lateral sides of the ankle, just and lateral sides of the ankle, just above the above the malleoli……………………………………malleoli……………………………………
For the For the anterior medial approachanterior medial approach, a soft , a soft spot is identified medial to the anterior tibial spot is identified medial to the anterior tibial tendon and lateral to the medial tendon and lateral to the medial malleolus………………………………..malleolus………………………………..
The needle is inserted perpendicular to the The needle is inserted perpendicular to the tibial joint surface and advanced slightly tibial joint surface and advanced slightly laterally, superiorly, and laterally, superiorly, and posteriorly…………………………………………posteriorly…………………………………………
The injection is then given slowly after there The injection is then given slowly after there is a decrease in tissue resistance indicating is a decrease in tissue resistance indicating that the needle has entered the that the needle has entered the joint…………………………………………….joint…………………………………………….
The The anterior lateral approachanterior lateral approach is done is done with the patient positioned with the foot in with the patient positioned with the foot in plantar flexion…………………….plantar flexion…………………….
The needle is inserted from the anterior The needle is inserted from the anterior lateral position and directed posteriorly lateral position and directed posteriorly toward the medial malleolustoward the medial malleolus……………….. ………………..
The needle again is advanced until there is a The needle again is advanced until there is a drop in tissue resistance confirming entry into drop in tissue resistance confirming entry into the joint…………….. the joint……………..
Tarsal tunnelTarsal tunnel
The patient is placed in a The patient is placed in a lateral decubituslateral decubitus position with the symptomatic foot position with the symptomatic foot down…………………….. down……………………..
The posterior tibial nerve is posterior to the The posterior tibial nerve is posterior to the posterior tibialis tendon, which is identified by posterior tibialis tendon, which is identified by resisting foot inversion. The needle is inserted resisting foot inversion. The needle is inserted behind the medial malleolus posterior to the behind the medial malleolus posterior to the tendon,at a tendon,at a 30°30° angle, and advanced a few angle, and advanced a few centimeters before the centimeters before the injection……………………………………………injection……………………………………………
Plantar fasciaPlantar fascia
Plantar fasciitisPlantar fasciitis is the most common problem of is the most common problem of the hind foot, with inflammation that occurs at the hind foot, with inflammation that occurs at its medial attachment to the its medial attachment to the calcaneus…………………calcaneus…………………
The needle is inserted at this location The needle is inserted at this location perpendicular to the calcaneus, and advanced perpendicular to the calcaneus, and advanced until it hits periosteum. The needle is then until it hits periosteum. The needle is then repositioned and advanced distal to the plantar repositioned and advanced distal to the plantar surface of the bone, placing the needle tip surface of the bone, placing the needle tip superior to the plantar superior to the plantar fascia………………………………………. fascia……………………………………….
The injection is then performed in this The injection is then performed in this position, which avoids the superficial fat position, which avoids the superficial fat pad, the subcutaneous tissue, and the pad, the subcutaneous tissue, and the fascia that could otherwise lead to fat fascia that could otherwise lead to fat pad atrophy or tissue necrosis or rupture pad atrophy or tissue necrosis or rupture of the fascia……………………..of the fascia……………………..
The The retrocalcaneal bursaretrocalcaneal bursa is located is located between the calcaneus and the between the calcaneus and the Achilles tendon, whereas the Achilles tendon, whereas the retroAchilles bursaretroAchilles bursa is located is located between the Achilles tendon and the between the Achilles tendon and the skin.Either of these disorders can be skin.Either of these disorders can be mistaken for Achilles tendonitis or mistaken for Achilles tendonitis or occur in combination with Achilles occur in combination with Achilles tendonitis (tendonitis (Haglund syndromeHaglund syndrome)… )…
An injection of the bursa should be considered only in An injection of the bursa should be considered only in severe, disabling cases after failure of conservative severe, disabling cases after failure of conservative treatment……………………………………..treatment……………………………………..
The patient is forewarned about Achilles tendon rupture The patient is forewarned about Achilles tendon rupture as a possible side effect of the corticosteroid as a possible side effect of the corticosteroid injection…………………………………….. injection……………………………………..
To locate the area of To locate the area of maximum tendernessmaximum tenderness, the Achilles , the Achilles tendon insertion site is palpated deep, superficial, and at tendon insertion site is palpated deep, superficial, and at the tendon. The retrocalcaneal bursa is injected deep to the tendon. The retrocalcaneal bursa is injected deep to the tendon, whereas the retroAchilles bursa is injected the tendon, whereas the retroAchilles bursa is injected superficial to the superficial to the tendon………………………………………………………. tendon……………………………………………………….
Morton's neuromaMorton's neuroma
Morton's neuromaMorton's neuroma is actually a is actually a perineural fibrosisperineural fibrosis of the common of the common digital nerve as it passes between digital nerve as it passes between the metatarsal heads…………………. the metatarsal heads………………….
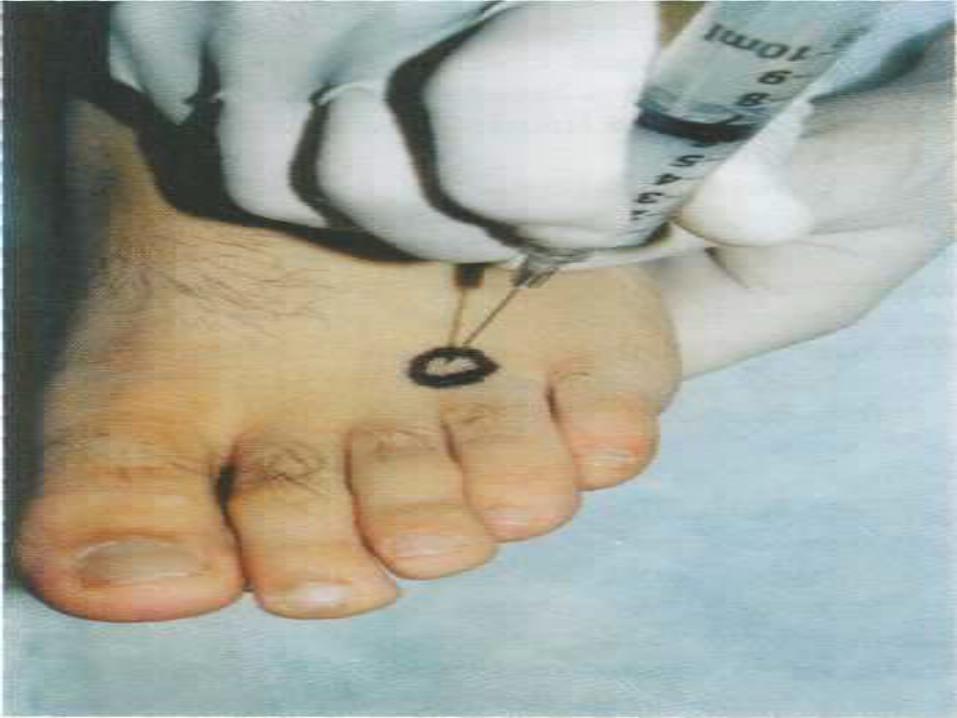
The neuroma most commonly occurs The neuroma most commonly occurs at the distal aspect of the at the distal aspect of the thirdthird metatarsal space……………….. metatarsal space………………..
A needle is passed through the A needle is passed through the dorsal surface of the foot and dorsal surface of the foot and advanced about advanced about 1 cm1 cm proximal to the proximal to the metatarsal web space. The needle is metatarsal web space. The needle is advanced deep enough to place the advanced deep enough to place the tip at the level of the neuroma, while tip at the level of the neuroma, while at the same time avoiding the at the same time avoiding the plantar fat pad…………………plantar fat pad…………………
IndicationsIndications RRadiculopathy******************adiculopathy****************** SI SI joint************************ joint************************ FFacet joint*********************acet joint********************* EEpidurography******************pidurography****************** DDiskography********************iskography******************** MMyelography********************yelography******************** SSympathetic procedures*******ympathetic procedures*******
EPIDUROGRAPHYEPIDUROGRAPHY
Epidurography is utilized during Epidurography is utilized during epidural procedures to determine epidural procedures to determine proper needle placementproper needle placement and to and to avoid intravascular or intrathecal avoid intravascular or intrathecal injections…………………………………..injections…………………………………..
MYELOGRAPHYMYELOGRAPHY
Myelography is a diagnostic Myelography is a diagnostic procedure commonly combined with procedure commonly combined with computed tomography (CT) for the computed tomography (CT) for the evaluation of spinal pathology, evaluation of spinal pathology, including:::::::::::::::::::::::including:::::::::::::::::::::::
disk herniationsdisk herniations,, stenosisstenosis, , tumorstumors, , infectioninfection…………………………………… ……………………………………
DISKOGRAPHYDISKOGRAPHY
Diskography is a procedure used to identify Diskography is a procedure used to identify whether or not an intervertebral disk(s) is whether or not an intervertebral disk(s) is generating axial spine pain in the cervical, generating axial spine pain in the cervical, thoracic, or lumbar regions…thoracic, or lumbar regions…
Diskography is recommended after there has Diskography is recommended after there has been no response to conservative treatment been no response to conservative treatment and traditional diagnostic modalities, such as and traditional diagnostic modalities, such as (MRI), CT, myelography and EDX are (MRI), CT, myelography and EDX are unremarkable or not diagnostic…………….. unremarkable or not diagnostic……………..
Diskography is also used for surgical Diskography is also used for surgical planning when considering an intradiskal planning when considering an intradiskal procedure, such asprocedure, such as
intradiskal electrothermal therapyintradiskal electrothermal therapy** fusionfusion********************************************************** artificial disk replacementartificial disk replacement******************
Allergic or anaphylactic reactions can Allergic or anaphylactic reactions can occur from either corticosteroids or occur from either corticosteroids or radio-logic contrast radio-logic contrast material…………………………. material………………………….
Typically, Typically, contrast allergiescontrast allergies occur at the occur at the time of the injections, and can quickly time of the injections, and can quickly progress to an anaphylactic reaction with progress to an anaphylactic reaction with respiratory compromise……………….. respiratory compromise………………..
Corticosteroid allergicCorticosteroid allergic reactions are often reactions are often delayed by up to a week, and present as an delayed by up to a week, and present as an intense hot, erythematous flushing involving intense hot, erythematous flushing involving the neck, face, and occasionally the chest area. the neck, face, and occasionally the chest area.
Corticosteroid anaphylactic reactions often Corticosteroid anaphylactic reactions often occur within occur within 2-62-6 h after the h after the injection………………………………………………injection………………………………………………
While there is concern regarding respiratory While there is concern regarding respiratory compromise, there have been no reported compromise, there have been no reported fatalities…………………………….fatalities…………………………….
VASOVAGAL EPISODESVASOVAGAL EPISODES Vasovagal episodes can occur with any type Vasovagal episodes can occur with any type
of injection procedure, whether it is a joint of injection procedure, whether it is a joint injection or a spinal procedure, due to the injection or a spinal procedure, due to the noxious stimulation effect from the needle. noxious stimulation effect from the needle. Patients typically become Patients typically become diaphoreticdiaphoretic, , hypotensivehypotensive, and , and bradycardicbradycardic……………………………………… ………………………………………
Treatment is primarily supportive, including Treatment is primarily supportive, including fluidsfluids and and oxygenoxygen, but begins with getting rid , but begins with getting rid of the noxious stimulation by remov ing the of the noxious stimulation by remov ing the needle…….needle…….
DURAL PUNCTURESDURAL PUNCTURES Dural punctures have a low reported Dural punctures have a low reported
incidence………………………………………….. incidence………………………………………….. Headaches resulting from dural puncture Headaches resulting from dural puncture
have been reported to range from 7.5% to have been reported to range from 7.5% to 75%..................................... 75%.....................................
The use of The use of smaller gauge needles with conical smaller gauge needles with conical noncutting tipsnoncutting tips has been associated with has been associated with fewer episodes of fewer episodes of headaches…………………………………………headaches…………………………………………
Dural puncture headaches can occur Dural puncture headaches can occur 1-21-2 days days after a translaminar or transforaminal after a translaminar or transforaminal epidural……………………….epidural……………………….
INJECTION INJECTION A subarachnoid or intravascular anesthetic A subarachnoid or intravascular anesthetic
injection can lead to injection can lead to periorbital numbnessperiorbital numbness, , disorientationdisorientation, , light-headednesslight-headedness, , nystagmusnystagmus, , tinnitustinnitus, , complete sensory or motor blockcomplete sensory or motor block, , muscle twitchingmuscle twitching, , respiratory depressionrespiratory depression, and , and seizuresseizures……………………. …………………….
The risk of complications from intrathecal and The risk of complications from intrathecal and intravascular injections of local anesthetic is intravascular injections of local anesthetic is proportional to the proportional to the injected injected volume………………………volume………………………
EPIDURAL ABSCESSEPIDURAL ABSCESS
An epidural abscess is rare from an An epidural abscess is rare from an injection, and is more common with injection, and is more common with the use of an the use of an indwelling indwelling cathetercatheter……………………………………. …………………………………….
Patients with an abscess present with Patients with an abscess present with severe back painsevere back pain, , feverfever, and , and chillschills………………………………………..………………………………………..
EPIDURAL HEMATOMAEPIDURAL HEMATOMA
The risk of epidural hematoma increases with The risk of epidural hematoma increases with anticoagulation but is rare in the presence of anticoagulation but is rare in the presence of normal clotting normal clotting factors………………………………………………factors………………………………………………
A hematoma can potentially lead to caudal A hematoma can potentially lead to caudal equina compression in the lumbar spine, or equina compression in the lumbar spine, or cord compression in the cervical and thoracic cord compression in the cervical and thoracic spine………….. spine…………..
The presence of spinal stenosis increases this The presence of spinal stenosis increases this compression risk…………. compression risk………….
Epidurals should be avoided in Epidurals should be avoided in patients with a platelet count less patients with a platelet count less
thanthan 100 000100 000 per ml and a spinal per ml and a spinal
canal midsagittal diameter less thancanal midsagittal diameter less than 12 12 mm………………………mm………………………
Complications of transforaminal Complications of transforaminal epidural steroid injections (TFESIs)epidural steroid injections (TFESIs)
Injury to the radicular artery, Injury to the radicular artery, particularly the artery of particularly the artery of AdamkiewiczAdamkiewicz (lower thoracic and (lower thoracic and upper lumbar levels), or other upper lumbar levels), or other collateral arteries within the foramen collateral arteries within the foramen is believed to occur as a result of is believed to occur as a result of spasmspasm, , puncturepuncture, , thrombosisthrombosis, or , or embolizationembolization by corticosteroid by corticosteroid particulate matter. particulate matter.
This complication might be reduced This complication might be reduced or eliminated by inserting needles or eliminated by inserting needles into the posterior portion of the into the posterior portion of the foramen, while avoiding injections in foramen, while avoiding injections in the presence of the presence of significant foraminal significant foraminal stenosisstenosis, using , using blunt tip needlesblunt tip needles, and , and injecting with non-particulate injecting with non-particulate corticosteroids................................corticosteroids................................
Complications from cervical facet Complications from cervical facet injectioninjection
Vertebral artery punctureVertebral artery puncture****************************************************** Motor and sensory blockMotor and sensory block******************************************************** Phrenic and recurrent laryngeal nerve paralysisPhrenic and recurrent laryngeal nerve paralysis**********Spinal cord traumaSpinal cord trauma******************************************************************** Spinal anesthesiaSpinal anesthesia********************************************************************** Dural punctureDural puncture****************************************************************************Intravascular injectionIntravascular injection************************************************************Chemical meningitisChemical meningitis****************************************************************Hematoma formationHematoma formation**************************************************************PneumothoraxPneumothorax****************************************************************************InfectionInfection**************************************************************************************
complications of SIJ injectioncomplications of SIJ injection
Posterior leakage of contrast into the Posterior leakage of contrast into the dorsal sacral foramina,can affect the dorsal sacral foramina,can affect the nearby neural structures such as nearby neural structures such as L5L5 &&lumbosacral plexus**lumbosacral plexus**
Trauma to the Trauma to the sciaticsciatic nerve nerve************ InfectionInfection************************* ************************* Adverse drug reactionsAdverse drug reactions*********** ***********
complications from stellate ganglion complications from stellate ganglion blocksblocks
PneumothoraxPneumothorax******************** ******************** central nervous system toxicitycentral nervous system toxicity****** low blood pressurelow blood pressure******************************** phrenic nerve blockphrenic nerve block****************************** brachial plexus blockbrachial plexus block************************** blockage of recurrent laryngealblockage of recurrent laryngeal******
This procedure is rarely performed This procedure is rarely performed bilaterally, because of the risk of bilaterally, because of the risk of blocking the blocking the phrenicphrenic and and recurrent recurrent laryngeallaryngeal nerve…………. nerve………….
Complications from lumbar Complications from lumbar sympathetic blockssympathetic blocks
complication from a myelogramcomplication from a myelogram
Postdural puncture headachePostdural puncture headache is the is the most common complication from a most common complication from a myelogram……………………….myelogram……………………….
Epidural hemorrhageEpidural hemorrhage is a reported is a reported complication of myelography……………….complication of myelography……………….
Spinal cord punctureSpinal cord puncture is another potentially is another potentially serious complication when cervical serious complication when cervical myelography is performed with a lateral Cl, myelography is performed with a lateral Cl, C2 approach……………………..C2 approach……………………..
This risk can be eliminated by using a lumbar This risk can be eliminated by using a lumbar puncture to instill contrast for a cervical puncture to instill contrast for a cervical myelography………………………….myelography………………………….
complications from diskographycomplications from diskography
diskitisdiskitis, , nerve root injurynerve root injury, , bleedingbleeding, , allergic reactionallergic reaction, , subarachnoid subarachnoid puncturepuncture, , soft tissue infectionsoft tissue infection and and chemical chemical meningitismeningitis……………………………………… ………………………………………
The incidence of diskitis can be reduced with The incidence of diskitis can be reduced with meticulous meticulous aseptic techniqueaseptic technique, , prophylactic prophylactic antibioticsantibiotics and and two-needle two-needle technique…………………………………………..technique…………………………………………..
EFFICACYEFFICACY
The largest number of epidural The largest number of epidural outcome studies has been reported outcome studies has been reported for for lumbarlumbar epidural steroid injections epidural steroid injections followed by followed by cervicalcervical epidural steroid epidural steroid injections…………………………………..injections…………………………………..
There are no published randomized There are no published randomized studies for thoracic epidural steroid studies for thoracic epidural steroid injections…………..injections…………..
The evidence for The evidence for caudalcaudal epidurals is epidurals is strongstrong for short-term relief and for short-term relief and moderatemoderate for long- for long-term relief……………… term relief………………
The findings for The findings for interlaminar interlaminar epidurals are epidurals are moderatemoderate for short-term relief and for short-term relief and limitedlimited for for long-term relief of symptoms.long-term relief of symptoms.
The results for The results for TFESIsTFESIs are are strongstrong for both for both short- and long-term relief…………..short- and long-term relief…………..
There is a There is a 10-30%10-30% prevalence of sacroiliac prevalence of sacroiliac joint dysfunction as the cause of low back joint dysfunction as the cause of low back pain.There are no definitive historical, pain.There are no definitive historical, physical examination, or diagnostic findings physical examination, or diagnostic findings that are specific for sacroiliac joint that are specific for sacroiliac joint pain……………………………pain……………………………
Only 22% of sacroiliac joint injections are Only 22% of sacroiliac joint injections are successfully performed without fluoroscopic successfully performed without fluoroscopic guidanceguidance ……………………….. ………………………..
Epidurography Epidurography is an integral part of is an integral part of performing interlaminar and performing interlaminar and transforaminal steroid injections. transforaminal steroid injections. Epidurography is used to confirm Epidurography is used to confirm needle placementneedle placement in the epidural in the epidural space prior to instilling therapeutic space prior to instilling therapeutic agents and agents and to avoid intravascular or to avoid intravascular or intrathecal intrathecal injection……………………………………. injection…………………………………….
Epidurography is also used to Epidurography is also used to evaluate the status of the evaluate the status of the epidural epidural spacespace, such as in the postoperative , such as in the postoperative spine patient…………spine patient…………
MyelographyMyelography is a diagnostic is a diagnostic imaging study in which radiopaque imaging study in which radiopaque contrast material is injected into the contrast material is injected into the intrathecal space under direct intrathecal space under direct fluoroscopic observation. Multiple x-fluoroscopic observation. Multiple x-rays are obtained after contrast rays are obtained after contrast injection to evaluate specific areas of injection to evaluate specific areas of the spinal canal…………….. the spinal canal……………..
Myelography is helpful (particularly Myelography is helpful (particularly when combined with CT) in the when combined with CT) in the evaluation of intrathecal pathology, evaluation of intrathecal pathology, such assuch as
Myelography with flexion and Myelography with flexion and extension views allows for a dynamic extension views allows for a dynamic spine evaluation under fluoroscopy spine evaluation under fluoroscopy that is not possible with MRI or that is not possible with MRI or CT……………………………CT……………………………
Myelography is also used when MRI Myelography is also used when MRI or CT are inconclusive………….or CT are inconclusive………….
Diskography Diskography has demonstrated a has demonstrated a 60%60% prevalence of diskogenic neck pain in the prevalence of diskogenic neck pain in the post-traumatic chronic neck painpost-traumatic chronic neck pain population…………………………………..population…………………………………..
Diskography has detected a Diskography has detected a 40%40% prevalence prevalence of diskogenic pain in patients with of diskogenic pain in patients with 6 months 6 months of chronic low back painof chronic low back pain, who have had an , who have had an otherwise unremarkable diagnostic workup otherwise unremarkable diagnostic workup including imaging studies …………………..including imaging studies …………………..
Imaging studies (MRI or CT) of the cervical Imaging studies (MRI or CT) of the cervical and thoracic spine are recommended to and thoracic spine are recommended to evaluate any possible compromise to the evaluate any possible compromise to the epidural space prior to performing an epidural space prior to performing an interlaminar epidural injection at the interlaminar epidural injection at the cervicalcervical, , thoracicthoracic, and , and upper lumbarupper lumbar levels……………………………. levels…………………………….
The same applies toThe same applies to mid mid andand lower lower lumbar lumbar levels in the postoperative levels in the postoperative patient………………………………………………. patient……………………………………………….
The patient is positioned prone on the The patient is positioned prone on the fluoroscopy table ………………………………fluoroscopy table ………………………………
The entry level for the The entry level for the cervicalcervical spine is spine is typically at the typically at the C7-T1C7-T1 level……………….. level………………..
At the site of pathologyAt the site of pathology for the for the thoracic thoracic and and lumbarlumbar spine………………………………. spine……………………………….
Epidural injections are avoided at sites of Epidural injections are avoided at sites of previous posterior spine surgery, due to the previous posterior spine surgery, due to the obliteration of the epidural space and the obliteration of the epidural space and the subsequent increased risk of intrathecal subsequent increased risk of intrathecal penetration……………………..penetration……………………..
An epidural needle is advanced through the skin using a An epidural needle is advanced through the skin using a paramedian approach under intermittent fluoroscopy paramedian approach under intermittent fluoroscopy until contact is made with the lamina The needle is until contact is made with the lamina The needle is 'walked off' the laminar edge on to the 'walked off' the laminar edge on to the ligamentum ligamentum flavumflavum……………………………………. …………………………………….
A A 2-3cc2-3cc volume of volume of non-ionic contrastnon-ionic contrast is slowly injected is slowly injected under fluoroscopy after negative aspiration to produce under fluoroscopy after negative aspiration to produce an epidurogram to confirm appropriate needle an epidurogram to confirm appropriate needle placement…………………………... placement…………………………...
A A 1-cc 1-cc test dose of test dose of lidocainelidocaine (lignocaine) is injected, after (lignocaine) is injected, after which the anesthetic and corticosteroid solution is slowly which the anesthetic and corticosteroid solution is slowly injected into the epidural injected into the epidural space………………………………………………….space………………………………………………….
Transforaminal approachTransforaminal approach
The patient is positioned in the The patient is positioned in the supinesupine position for a cervical TFESI, position for a cervical TFESI, and the C arm or the patient is and the C arm or the patient is positioned obliquely until there is a positioned obliquely until there is a clear view of the clear view of the foramen………………………………….. foramen…………………………………..
The patient is positioned in the The patient is positioned in the proneprone position for a position for a thoracic thoracic or or lumbarlumbar TFESI, and the C arm or the patient is TFESI, and the C arm or the patient is positioned obliquely until the tip of positioned obliquely until the tip of the ipsilateral subjacent superior the ipsilateral subjacent superior articular process divides the pedicle articular process divides the pedicle in half. in half.
At least 0.5 cc of non-ionic contrast is At least 0.5 cc of non-ionic contrast is injected under injected under fluoroscopy……………………………… fluoroscopy………………………………
Syringes are exchanged for the Syringes are exchanged for the anesthetic and steroid mixture…..anesthetic and steroid mixture…..
The solution is slowly injected after a The solution is slowly injected after a negative 1-cc test dose……negative 1-cc test dose……
Caudal injectionCaudal injection
A spinal needle penetrates the skin A spinal needle penetrates the skin at a at a 45°45° angle between the sacral angle between the sacral cornu, and is advanced until it cornu, and is advanced until it contacts the sacrum. The needle is contacts the sacrum. The needle is slightly withdrawn and advanced at a slightly withdrawn and advanced at a shallow shallow 10°10° angle through the angle through the sacrococcygeal ligament into the sacrococcygeal ligament into the epidural space….epidural space….
After negative aspiration, contrast is After negative aspiration, contrast is injected under fluoroscopy into the injected under fluoroscopy into the epidural space, followed by the epidural space, followed by the injectate solution………………………..injectate solution………………………..
The needle pierces the posterior The needle pierces the posterior sacroiliac ligament and then enters sacroiliac ligament and then enters the joint at the hyperlucent the joint at the hyperlucent area………………………………………….. area…………………………………………..
Contrast is injected after negative Contrast is injected after negative aspiration to produce an arthrogram aspiration to produce an arthrogram to confirm needle tip to confirm needle tip placement…………………………………. placement………………………………….
The patient is placedThe patient is placed prone prone on the on the fluoroscopy table, with the head of the table fluoroscopy table, with the head of the table elevated elevated 5-105-10°…………………………… °……………………………
The skin and subcutaneous tissue are The skin and subcutaneous tissue are anesthetized with anesthetized with 1%1% lidocaine (lignocaine) lidocaine (lignocaine)………………………………………. ……………………………………….
A spinal needle is placed midline at the A spinal needle is placed midline at the L2, L3L2, L3 level to ensure the introduction of contrast level to ensure the introduction of contrast above the L3 vertebral level. above the L3 vertebral level.
The spinal needle is advanced under The spinal needle is advanced under fluoroscopy………………………fluoroscopy………………………
There is resistance as the needle There is resistance as the needle enters the enters the ligamentum flavumligamentum flavum, which , which decreases as it passes through the decreases as it passes through the ligament into the subarachnoid ligament into the subarachnoid space…………………… space……………………
The needle tip bevel is turned cephalad, and The needle tip bevel is turned cephalad, and there is flow of there is flow of CSFCSF after removing the after removing the stylet………………………………………….. stylet…………………………………………..
If there is noIf there is no CSF CSF flow, a lateral radiographic flow, a lateral radiographic view is recommended to check the needle view is recommended to check the needle depth……………………… depth………………………
If the needle depth is correct, the patient is If the needle depth is correct, the patient is asked to perform asked to perform Valsalva's maneuverValsalva's maneuver, which , which inevitably leads to flow of inevitably leads to flow of CSFCSF through the through the needle…………… needle……………
Approximately Approximately 18-2018-20 cc of contrast is cc of contrast is injected to complete the myelogram, injected to complete the myelogram, after which x-rays are obtained, after which x-rays are obtained, including anteroposterior, lateral, including anteroposterior, lateral, oblique, flexion and extension views oblique, flexion and extension views ……….……….
A CT scan is performed afterward to A CT scan is performed afterward to complement the complement the myelogrammyelogram………………………………………………………………
For For cervicalcervical and and thoracicthoracic myelography, the myelography, the contrast is injected in the same manner into the contrast is injected in the same manner into the lumbar subarachnoid space. The patient is then lumbar subarachnoid space. The patient is then placed into placed into Trendelenburg's positionTrendelenburg's position to allow for to allow for flow of contrast into the cervical and thoracic flow of contrast into the cervical and thoracic areas………………………………………………….. areas…………………………………………………..
Care is taken to avoid contrast flow into the Care is taken to avoid contrast flow into the foramen magnum……………………………. foramen magnum…………………………….
CT and regular x-rays are performed after the CT and regular x-rays are performed after the myelogram injection……………………….. myelogram injection………………………..
Routine postmyelography instructions Routine postmyelography instructions include head elevation at include head elevation at 30-45°30-45° above above the horizontal plane for the horizontal plane for 12-24 h12-24 h and oral and oral fluids……………..fluids……………..
Diskography injection Diskography injection
Intravenous antibioticsIntravenous antibiotics and and light light intravenous sedationintravenous sedation are given to the are given to the patient prior to starting the patient prior to starting the procedure………………..procedure………………..
Intradiskal antibiotics can be given Intradiskal antibiotics can be given as an alternative or in addition to the as an alternative or in addition to the intravenous antibiotics for prevention intravenous antibiotics for prevention of disk infection…………………………..of disk infection…………………………..
The patient is positioned in a The patient is positioned in a modified lateral decubitus position modified lateral decubitus position when performing when performing thoracicthoracic and and lumbarlumbar diskography, with the diskography, with the symptomatic side down……………… symptomatic side down………………
The needles are then placed into the The needles are then placed into the disks from the asymptomatic disks from the asymptomatic side…………………side…………………
Although the needle site entry for cervical Although the needle site entry for cervical diskography can be performed with the same diskography can be performed with the same methodology, this is not as critical, because methodology, this is not as critical, because the needles are being placed through the the needles are being placed through the anterior portion of the anterior portion of the neck…………………………….. neck……………………………..
In addition, needle insertion from the left side In addition, needle insertion from the left side carries a greater risk of esophageal carries a greater risk of esophageal puncture………………………puncture………………………