37
1 Chapter 5 Chapter 5 Drugs for Diabetes Drugs for Diabetes Mellitus Mellitus
| Date post: | 31-Dec-2015 |
| Category: |
Documents |
| Upload: | kaseem-dalton |
| View: | 45 times |
| Download: | 0 times |

11
Chapter 5Chapter 5Drugs for Diabetes Drugs for Diabetes
MellitusMellitus
22
Diabetes MellitusDiabetes Mellitus
Diabetes mellitus is a condition in which Diabetes mellitus is a condition in which the body cannot effectively regulate the body cannot effectively regulate blood glucose or “blood sugar.” blood glucose or “blood sugar.” Hyperglycemia – high blood glucoseHyperglycemia – high blood glucose Hypoglycemia – low blood glucoseHypoglycemia – low blood glucose

33
Glucose MetabolismGlucose Metabolism
As we consume food, the digestive As we consume food, the digestive system predominately converts those system predominately converts those foods into glucose.foods into glucose. Energy Energy
44
Glucose Metabolism Glucose Metabolism ((cont.cont.))
If glucose is not utilized for energy If glucose is not utilized for energy purposes at the time of digestion, it is purposes at the time of digestion, it is stored. stored. Glycogen in the liver and muscles Glycogen in the liver and muscles Adipose Adipose

55
Glucose Utilization in the Glucose Utilization in the BodyBody
Requires Insulin Requires Insulin PancreasPancreas
Insulin binds with specific receptors on Insulin binds with specific receptors on the cell membrane. the cell membrane.
Once bound, the receptors signal protein Once bound, the receptors signal protein messengers within the cell.messengers within the cell.

66
Glucose Utilization in the Glucose Utilization in the Body (Body (cont.cont.))
Proteins migrate to the cytoplasm of the Proteins migrate to the cytoplasm of the cell membrane, bind with glucose, and cell membrane, bind with glucose, and allow passage into the cell by passive allow passage into the cell by passive transport.transport.
77
Glucose Utilization in the Glucose Utilization in the Body (Body (cont.cont.))
Without insulin in the bodyWithout insulin in the body Excess glucose accumulates in the blood, Excess glucose accumulates in the blood,
which goes unusedwhich goes unused Excreted in the urineExcreted in the urine

88
ExceptionsExceptions
The brain requires a constant supply of The brain requires a constant supply of glucose. glucose. The brain is freely permeable to glucose at The brain is freely permeable to glucose at
all times. all times.
During exercise, skeletal muscles can During exercise, skeletal muscles can readily uptake glucose into the cells readily uptake glucose into the cells without the presence of insulin. without the presence of insulin.

99
Exceptions (Exceptions (cont.cont.))
The liver is also non-insulin dependent The liver is also non-insulin dependent but insulin will enhance the metabolism but insulin will enhance the metabolism of glucose throughout the body.of glucose throughout the body.
1010
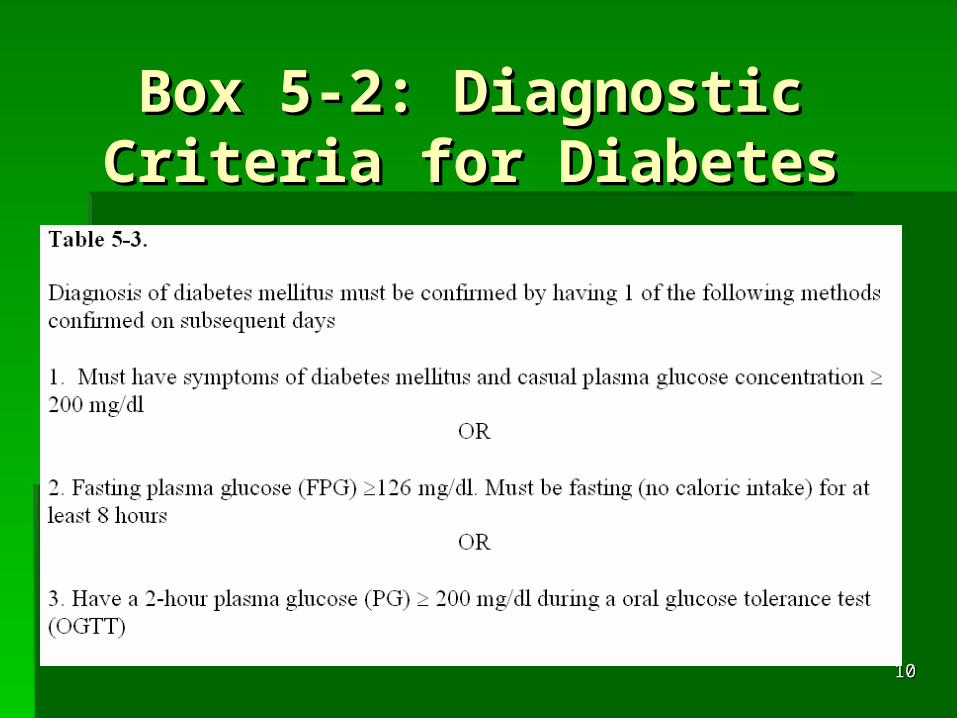
Box 5-2: Diagnostic Box 5-2: Diagnostic Criteria for DiabetesCriteria for Diabetes
1111
Types of DiabetesTypes of Diabetes
Type 1 DiabetesType 1 Diabetes Formally known as “insulin Dependent Formally known as “insulin Dependent
Diabetes Mellitus” (IDDM) or “Juvenile-onset Diabetes Mellitus” (IDDM) or “Juvenile-onset diabetes” diabetes”
Diagnosed in children, teenagers, and young Diagnosed in children, teenagers, and young adults adults
Can result from an autoimmune destruction Can result from an autoimmune destruction of the pancreatic of the pancreatic -cells -cells
Requires exogenous insulin to sustain life Requires exogenous insulin to sustain life

1212
Why Type 1 DiabetesWhy Type 1 Diabetes
Auto-immune destruction of the pancreatic Auto-immune destruction of the pancreatic -cells. -cells.
Some will have rapid destruction and others Some will have rapid destruction and others will have slower rate of destruction. will have slower rate of destruction.
Cell destruction can take place over weeks, Cell destruction can take place over weeks, months, or even years. months, or even years.
Virus, toxin, or some environmental Virus, toxin, or some environmental condition is thought to stimulate the condition is thought to stimulate the destruction of the destruction of the -cells.-cells.
The exact destruction process is unclear.The exact destruction process is unclear.

1313
Type 2 DiabetesType 2 Diabetes
Formally known as “Non-Insulin Dependent Formally known as “Non-Insulin Dependent Diabetes” (NIDDM)Diabetes” (NIDDM)
Previously known as “Adult-onset diabetes” Previously known as “Adult-onset diabetes” Can occur at any age, including Can occur at any age, including
adolescence, but usually affects older adolescence, but usually affects older individualsindividuals
May stem from insulin deficiency or May stem from insulin deficiency or resistanceresistance

1414
Why Type 2 DiabetesWhy Type 2 Diabetes
Age Age Lack of exercise Lack of exercise ObesityObesity Hypertension, Hypertension, Dyslipidemia – abnormal amount of lipids Dyslipidemia – abnormal amount of lipids
in the bloodin the blood

1515
Why Type 2 Diabetes Why Type 2 Diabetes ((cont.cont.))
Certain racial/ethnic groups Certain racial/ethnic groups Women who were diagnosed with Women who were diagnosed with
gestational diabetesgestational diabetes A strong genetic disposition plays a A strong genetic disposition plays a
contributing role in developing type 2 contributing role in developing type 2 diabetes, although the specific genetic diabetes, although the specific genetic link is not clearly knownlink is not clearly known
1616
Management of Diabetes Management of Diabetes
Glucose MonitoringGlucose Monitoring Blood glucose levels are measured using Blood glucose levels are measured using
Self-Monitored Blood Glucose (SMBG) Self-Monitored Blood Glucose (SMBG) equipment equipment
Blood tests 4 to 6 times per dayBlood tests 4 to 6 times per day

1717
Blood Glucose LevelsBlood Glucose Levels
Normal fasting plasma glucose (FPG) Normal fasting plasma glucose (FPG) levels = 70 – 120 mg/dLlevels = 70 – 120 mg/dL Fasting test is most appropriate to determine Fasting test is most appropriate to determine
blood glucose levels (diabetes)blood glucose levels (diabetes)
Two hours after a meal, glucose levels Two hours after a meal, glucose levels should be <140 mg/dLshould be <140 mg/dL
1818
Managing DiabetesManaging Diabetes
Diet Diet Exercise Exercise Insulin AdministrationInsulin Administration
Injection Injection Oral anti-diabetic agentsOral anti-diabetic agents

1919
DietDiet
Timing of food intakeTiming of food intake Type of foods eaten Type of foods eaten
(carbohydrate, fat, protein)(carbohydrate, fat, protein) Total caloric intakeTotal caloric intake
2020
ExerciseExercise
Recommended forRecommended for:: Type 1Type 1 Type 2Type 2
2121
Insulin AdministrationInsulin Administration
Exogenous insulin is required in:Exogenous insulin is required in: Gestational diabetes Gestational diabetes Type 1Type 1 Sometimes Type 2 Sometimes Type 2
2222
Insulin Injection DevicesInsulin Injection Devices
Syringe/needleSyringe/needle Insulin pump/refillableInsulin pump/refillable Prefilled insulin pens Prefilled insulin pens

2323
Insulin TypesInsulin Types
Rapid-actingRapid-acting HumalogHumalog
Short-actingShort-acting RegularRegular – slightly longer onset of action – slightly longer onset of action
compared to rapid-actingcompared to rapid-acting Intermediate-acting Intermediate-acting
LenteLente Long-actingLong-acting
UltralenteUltralente Combination ProductsCombination Products
2424
Rapid-Acting InsulinRapid-Acting Insulin
Humalog Humalog FDA (1996) – first available rapid-acting FDA (1996) – first available rapid-acting
insulininsulin Injected 15 minutes before mealInjected 15 minutes before meal
Onset = < 30 minOnset = < 30 min Peak = 30 min to 1 hour (longer depending on Peak = 30 min to 1 hour (longer depending on
type)type) Duration = 2 to 4 hours (+/Duration = 2 to 4 hours (+/––))

2525
Short-Acting InsulinShort-Acting Insulin
RegularRegular Longer onset of action compared to rapid-Longer onset of action compared to rapid-
acting acting Onset = ½ Onset = ½ –– 1 hr. 1 hr. Peak = 2 Peak = 2 – – 5 hrs.5 hrs. Duration = 5 Duration = 5 – – 10 hrs. 10 hrs.

2626
Intermediate-Acting Intermediate-Acting InsulinInsulin
Lente Lente Onset = 1 – 3 hrs.Onset = 1 – 3 hrs. Peak = 6 – 14 hrs.Peak = 6 – 14 hrs. Duration = 18 – 24 hrs. (+/Duration = 18 – 24 hrs. (+/––))

2727
Long-Acting InsulinLong-Acting Insulin
UltralenteUltralente Onset = 4 Onset = 4 –– 6 hrs. 6 hrs. Peak = 16 Peak = 16 –– 24 hrs. 24 hrs. Duration = 24 Duration = 24 –– 28 hrs. (+/ 28 hrs. (+/––))

2828
Table 5-4: Insulin Types Table 5-4: Insulin Types and Actions*and Actions*
2929
Injections/DayInjections/Day
Two Two One in the morningOne in the morning One in the late afternoonOne in the late afternoon
Mix of short and intermediateMix of short and intermediate
Three to FourThree to Four Mainly used for more control of the diabetesMainly used for more control of the diabetes

3030
Figure 5-8: Onset and Figure 5-8: Onset and Duration of ActionDuration of Action

3131
Adverse Effects of Adverse Effects of Injections Injections
Insulin shock – HypoglycemiaInsulin shock – Hypoglycemia Excess levels of insulin in the bodyExcess levels of insulin in the body Weak, drowsy, confused, hungry, or dizzy Weak, drowsy, confused, hungry, or dizzy Loss of consciousness and possibly coma Loss of consciousness and possibly coma

3232
Diabetic ConcernsDiabetic Concerns
Diabetic ketoacidosis Diabetic ketoacidosis More common in Type 1More common in Type 1 Insulin deficiency results in use of fatty acids Insulin deficiency results in use of fatty acids
for energyfor energy Ketones are released as a by-product of fat Ketones are released as a by-product of fat
metabolism = high blood levels of ketonesmetabolism = high blood levels of ketones Hyperglycemia, thirst, excess urination, Hyperglycemia, thirst, excess urination,
fatigue, blurred vision, fruity breath, nausea, fatigue, blurred vision, fruity breath, nausea, muscular stiffness, and difficulty breathing muscular stiffness, and difficulty breathing
Ketoacidosis can lead to coma and Ketoacidosis can lead to coma and potentially deathpotentially death
3333
Oral Antidiabetic AgentsOral Antidiabetic Agents
Combination of oral antidiabetic Combination of oral antidiabetic medications plus a regimen of diet and medications plus a regimen of diet and exercise allows diabetics to better exercise allows diabetics to better manage hyperglycemia manage hyperglycemia
Variety or oral antidiabetic agentsVariety or oral antidiabetic agents

3434
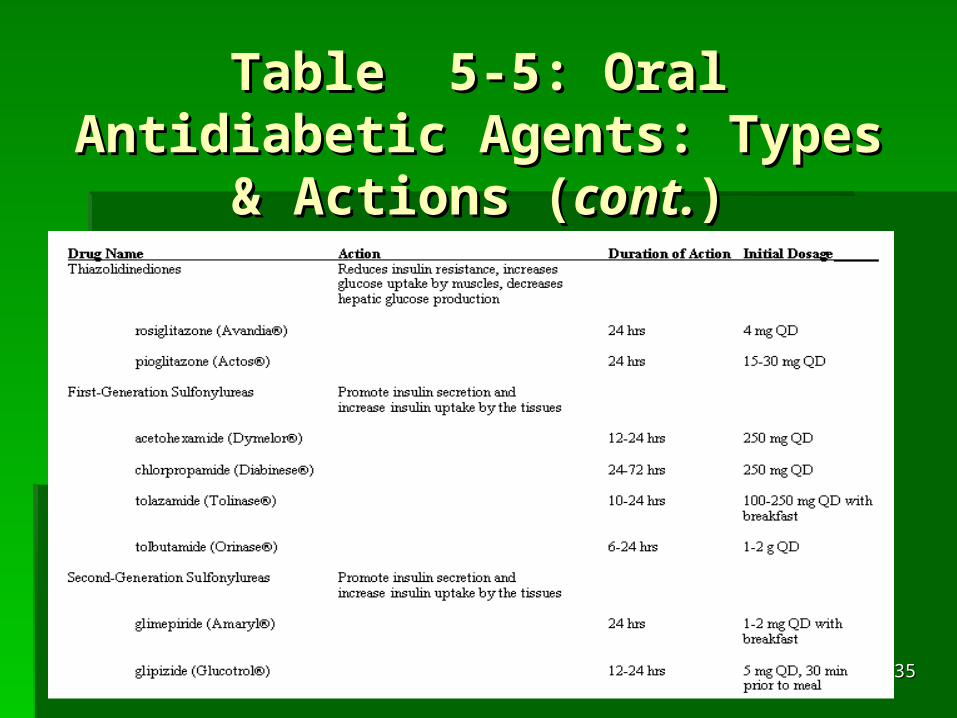
Table 5-5: Oral Antidiabetic Table 5-5: Oral Antidiabetic Agents: Types & ActionsAgents: Types & Actions
3535
Table 5-5: Oral Antidiabetic Table 5-5: Oral Antidiabetic Agents: Types & Actions Agents: Types & Actions
((cont.cont.))

3636
Box 5-1: Complications Box 5-1: Complications of Diabetesof Diabetes

3737
The Athletic Trainer’s The Athletic Trainer’s ResponsibilityResponsibility
Monitor blood glucose levels – before Monitor blood glucose levels – before and after exerciseand after exercise
Record food and insulin intakes for all Record food and insulin intakes for all types of activitytypes of activity
Monitor athlete/person for hypoglycemiaMonitor athlete/person for hypoglycemia Make appropriate decisions regarding Make appropriate decisions regarding
activity and blood glucose levelsactivity and blood glucose levels

















