Archives of Cardiovascular Disease (2019) xxx, xxx—xxx
Available online at
ScienceDirectwww.sciencedirect.com
CLINICAL RESEARCH
Characteristics and prognosis of patientswith significant tricuspid regurgitationCaractéristiques et pronostic des patients présentant une insuffisancetricuspide significative
Yohann Bohbota,b, Gagandeep Chadhaa,Justine Delabrea, Thomas Landemainea,Christophe Beylsa, Christophe Tribouilloya,b,∗
a Department of Cardiology, Amiens University Hospital, avenue René-Laënnec, 80054,Amiens cedex 1, Franceb EA 7517, MP3CV, Jules Verne University of Picardie, chemin du Thil, 80054, Amiens cedex,France
SummaryBackground. — Severe tricuspid regurgitation (TR) usually remains asymptomatic for a longperiod, and the diagnosis is often delayed until an advanced stage of right heart failure (RHF).Only a minority of patients are referred for surgery.Aim. — To describe the characteristics and prognosis of patients with significant TR, accordingto aetiology.Method. — Two-hundred and eight consecutive patients with moderate-to-severe (grade III) orsevere (grade IV) TR were included from echocardiography reports between 2013 and 2017.Median follow-up was 18 (6—38) months.Results. — Patients (mean age 75 years; 46.6% men) were divided into four groups according to
Please cite this article in press as: Bohbot Y, et al. Characteristics and prognosis of patients with significant tricuspidregurgitation. Arch Cardiovasc Dis (2019), https://doi.org/10.1016/j.acvd.2019.06.011
TR aetiology: group 1, primary TR (14.9%); group 2, TR secondary to left heart disease with ahistory of left heart valve surgery (24.5%); group 3, TR secondary to left heart or pulmonarydisease with no history of left valvular surgery (26.5%); and group 4, idiopathic TR (34.1%). Dur-ing follow-up, 61 patients (29.3%) experienced at least one episode of RHF decompensationrequiring hospitalization. Only 11 patients (5.3%) underwent tricuspid valve surgery during
Abbreviations: CI, confidence interval; HR, hazard ratio; ITVS, isolated tricuspid valve surgery; LV, left ventricular; LVEF, left ventricularejection fraction; NYHA, New York Heart Association; RHF, right heart failure; RV, right ventricular; S’, peak systolic velocity of the tricuspidannulus; TAPSE, tricuspid annular plane systolic excursion; TR, tricuspid regurgitation.
∗ Corresponding author at: Department of Cardiology, Amiens University Hospital, avenue René-Laënnec, Amiens cedex 1, 80054, France.E-mail address: [email protected] (C. Tribouilloy).
r Masson SAS.All rights reserved. - Document downloaded on 26/09/2019 by RODRIGUES SEBASTIEN (948138). It is forbidden and illegal to distribute this document.
he tricuspid valve is often called the ‘‘forgotten valve’’ecause its echocardiographical assessment is relatively dif-cult and the management of patients with tricuspid valveiseases remains poorly defined [1—4]. Significant (at leastoderate) tricuspid regurgitation (TR) is common, affecting
bout 0.5% of the general population [5], and its prevalencencreases markedly after the age of 75 years, especiallyn women and in the presence of atrial fibrillation [6].
hereas trivial TR is extremely frequent and benign, sig-ificant TR is associated with a poor prognosis [7,8]. Theechanisms of TR are mainly secondary [9,10], while pri-ary TR is less common. Idiopathic (or isolated secondary)R, defined by structurally normal tricuspid valves, no overtrganic TR cause, no left-sided valvular heart disease and
Please cite this article in press as: Bohbot Y, et al. Characterregurgitation. Arch Cardiovasc Dis (2019), https://doi.org/10.1
reserved left ventricular ejection fraction (LVEF), is notare [9,10], especially in older patients. TR usually remainssymptomatic for a long time and is often diagnosed only
•
asson SAS.All rights reserved. - Document downloaded on 26/09/2019 by RODRIGUES SEBAST
t an advanced stage of right heart failure (RHF). A minor-ty of patients (< 1%) are referred for surgery because theperative mortality risk is often considered unacceptable inlder patients, especially in the presence of right ventric-lar (RV) dysfunction [11,12]. Guidelines from Europe [1]nd the USA [13] concerning isolated tricuspid valve surgeryi.e. without left-sided valve surgery) remain vague in viewf the small number of prognostic studies and their contra-ictory findings [14,15], which are often influenced by theatients’ major comorbidities [14]. The dynamic nature ofR also highlights the difficulty in identifying patients whore likely to benefit from a surgical procedure. It is there-ore crucial to acquire more data to understand more clearlyhe natural history and prognosis of TR, and to try to definehe optimal timing of surgery.
The aims of this study were to:
istics and prognosis of patients with significant tricuspid016/j.acvd.2019.06.011
describe the clinical and echocardiographic characteris-tics of patients with significant TR who were followed inour heart valve centre;
IEN (948138). It is forbidden and illegal to distribute this document.
• assess the long-term survival of these patients relative tothat of the general population;
• evaluate the frequency of ‘‘idiopathic’’ TR amongmoderate-to-severe and severe TR;
• evaluate the long-term prognosis of ‘‘idiopathic TR’’ com-pared with other causes of TR.
Methods
Inclusion criteria
Between January 2013 and December 2017, 208 consecutivepatients aged ≥ 18 years, with a diagnosis of moderate-to-severe or severe TR on echocardiography, were identifiedprospectively and included in an electronic database.Patients were divided into four groups according to TR aeti-ology: group 1, primary TR (including drug-induced valvediseases, rheumatic valvular disease, myxomatous disease,infective endocarditis, carcinoid syndrome, congenital heartdisease, traumatic and postiatrogenic); group 2, TR sec-ondary to left heart disease with previous left heart valvesurgery; group 3, TR secondary to left heart or pulmonarydisease without previous cardiac surgery; and group 4, idio-pathic TR. Idiopathic TR was defined by structurally normaltricuspid valves with no overt organic TR cause, no left-sided valvular heart disease, preserved LVEF and no previouscardiac surgery [6,10].
Data on baseline clinical and demographic characteris-tics, including age, sex, body mass index and cardiovascularrisk factors, were collected. The Charlson ComorbidityIndex, comprising the sum of individual comorbidities, wascalculated for each patient [16]. Renal failure was defined bya creatinine clearance < 50 mL/min. This study was approvedby an independent ethics committee, and was conductedin accordance with institutional policies, French legislationand the revised Declaration of Helsinki (ID-RCB: 2017-A03233-50).
Echocardiography
All patients underwent a comprehensive Doppler echocar-diographic assessment, using commercially available ultra-sound systems. Three consecutive measurements in patientsin sinus rhythm and five consecutive measurements inpatients in atrial fibrillation were systematically averaged.TR was graded according to an integrative approach [17,18],using semiquantitative (colour flow jet area, vena con-tracta width, proximal isovelocity surface area [PISA] radius,hepatic vein flow and tricuspid inflow) and quantitativevariables (effective regurgitant orifice area, regurgitantvolume) [17—20]. Tricuspid valve morphology was evalu-ated using a multiview approach (parasternal long-axis,parasternal short-axis, apical four-chamber and subcostalviews). Right ventricular (RV) assessment was based onmultiple views. RV function was evaluated using tricuspidannular plane systolic excursion (TAPSE) and peak systolicvelocity of the tricuspid annulus (S’) [21]. RV dilation was
Please cite this article in press as: Bohbot Y, et al. Characterregurgitation. Arch Cardiovasc Dis (2019), https://doi.org/10.1
defined by a basal linear diameter and/or a proximal out-flow diameter > 42 mm, and RV dysfunction was defined byeither TAPSE < 14 mm and/or S’ < 10 cm/s [21]. Left and rightatrial areas were measured in the apical four-chamber
Cwiv
r Masson SAS.All rights reserved. - Document downloaded on 26/09/2019 by RODRIGUES SEBA
PRESS3
iew, and were considered to be enlarged when > 20 cm2
nd > 18 cm2, respectively [21]. Tricuspid annular diameteras considered to be dilated when > 4 cm in the standardpical four-chamber view [21]. Left ventricular (LV) wallhickness and dimensions were assessed from paraster-al long-axis views by two-dimensional guided M-mode,sing the leading-edge methodology at end-diastole andnd-systole. LV dilatation was defined by end-diastolic diam-ter > 60 mm and/or end-systolic diameter > 40 mm. LVEFas calculated using Simpson’s biplane method [21].
ollow-up and endpoints
edian (interquartile range) follow-up was 18 (6—38)onths. Most patients were followed by clinical consul-
ations and echocardiography in the outpatient clinic atmiens Hospital. A few patients were followed in pub-
ic hospitals or private practices by referring cardiologistsorking in collaboration with our centre. All survivingatients (n = 139) were followed until the end of the study,ith an inclusion date corresponding to the date of base-
ine echocardiography. No patients were lost to follow-up.nformation on follow-up was obtained by direct patientnterview and clinical examination and/or repeated follow-p letters, questionnaires and telephone calls to physicians,atients and (if necessary) next of kin. The primary endpointas all-cause mortality. The two secondary endpoints wereospitalization for RHF and the combination of hospitaliza-ion for RHF and cardiovascular mortality. Clinical decisionsegarding medical management or referral for surgery wereade by the Heart Team, with the approval of the patient’s
ardiologist, based on the European Society of Cardiologyuidelines [1].
tatistical analysis
ontinuous variables are expressed as means ± standardeviations or medians (interquartile ranges), and categor-cal variables are expressed as numbers (percentages). Theelationship between baseline continuous variables and thearious groups was explored using 1-way analysis of vari-nce tests. The �2 test was used to compare categoricalariables between groups. The independent-sample t-testr the Mann—Whitney U—test was used to compare contin-ous variables with normal or skewed distribution betweenroups. Event rates ± standard errors were estimated usinghe Kaplan-Meier method, and compared using two-sidedog-rank tests. Survival of patients was compared with thexpected survival of the age- and sex-matched population.ontrol data were obtained from Somme (a French depart-ent with 555,551 inhabitants) life tables, established on
he basis of the 1999 population census carried out by therench Institute of National Statistics (INSEE) [22]. Relativeurvival was computed as the ratio of observed-to-expectedurvival (observed number of deaths in the TR popula-ion/expected number of deaths in the general population).ortality and predictors of hospitalization for RHF analy-
es were performed using Cox proportional hazards models.
istics and prognosis of patients with significant tricuspid016/j.acvd.2019.06.011
ovariates considered to have a potential prognostic impactere tested in a univariate analysis. All significant variables
n univariate analysis with P < 0.1 were included in the multi-ariable Cox analysis. The limit of statistical significance was
STIEN (948138). It is forbidden and illegal to distribute this document.
< 0.05, and all tests were two-tailed. Data were analysedsing SPSS 25.0 (SPSS Inc. Chicago, IL, USA).
esults
aseline demographic and clinicalharacteristics
able 1 summarizes the distribution of TR aetiologies. Of the08 patients included, 119 (57%) had severe TR and 89 (43%)ad moderate-to-severe TR. Secondary TR was the predom-nant aetiology in 177 patients (85.1%), 51 (24.5%) of whomad a history of left heart valve surgery (group 2), 55 (26.5%)ad TR secondary to left heart or pulmonary disease with noistory of left heart valve surgery (group 3) and 71 (34.1%)ad idiopathic TR (group 4), while primary TR was diagnosedn only 31 patients (14.9%) (group 1).
Baseline demographic and clinical characteristics of the08 patients (mean age 75 ± 14 years; 46.6% men) andhe results of comparisons between the four groups areisplayed in Table 2. About two-thirds of patients were clas-ified as New York Heart Association (NYHA) stage I or II athe time of baseline echocardiography, and 52.4% of patientsad a history of RHF. Patients with primary TR (group 1) were
Please cite this article in press as: Bohbot Y, et al. Characterregurgitation. Arch Cardiovasc Dis (2019), https://doi.org/10.1
ounger, with a mean age of 65 years (P < 0.001). Group patients had lower rates of atrial fibrillation (P < 0.05),ypertension (P < 0.05), diuretics (P < 0.001) and comorbidi-ies (lower Charlson Comorbidity Index score; P < 0.05) than
v9sa
asson SAS.All rights reserved. - Document downloaded on 26/09/2019 by RODRIGUES SEBAST
PRESSY. Bohbot et al.
he other groups. Patients in the idiopathic TR group (group) (n = 71; mean age 77 years) were mostly women (63.4%).hirty-nine patients (54.9%) from this group had a history ofHF, 88.7% were in atrial fibrillation and 35.2% were NYHAtage III or IV. Fifty-eight patients from group 4 (81.7%) werereated with diuretics, at an average daily dose of 122 mg.
Only 11 patients (5.3%) underwent tricuspid valve surgeryuring follow-up: five tricuspid valve repairs; and six tri-uspid valve replacements (five biological prostheses andne mechanical prosthesis). Tricuspid valve surgery was per-ormed in two patients in group 1 (one valvular prolapse andne drug-induced TR), three patients in group 2 (one withrevious mitral valve replacement and two with previousortic valve replacement), four patients in group 3 (all hadssociated severe mitral regurgitation) and two patients inroup 4.
chocardiographic characteristics
aseline echocardiographic variables are displayed inable 3. Compared to patients with idiopathic TR (group 4),hose with TR secondary to left heart disease (groups 2 and) had a more enlarged left ventricle (all P < 0.001), a lowerVEF (P < 0.001) and poorer RV function, with more impaired’-waves and TAPSE (both P < 0.001). Patients with primaryR (group 1) had a smaller left atrial area (P < 0.05) and a
ower LVEF (P < 0.05) compared with group 4. There were noignificant differences between groups in terms of cardiacutput (P = 0.28), TR severity (P = 0.61), inferior vena cavaize (P = 0.28) and maximum velocity of TR (P = 0.37).
verall mortality
ixty-nine (33.2%) deaths were recorded during follow-up,1 of which were cardiovascular-related deaths (59%). Over-ll survival rates were low: 74 ± 3% at 1 year; 65 ± 3% at 2ears; 61 ± 4% at 3 years; and 56 ± 4% at 4 years (Fig. 1).he 4-year survival of patients with TR was lower than thexpected survival of the general population (56 ± 4% vs 74%).ne-year and 4-year relative survival rates (observed num-er of deaths in the TR population/expected number ofeaths in the general population) were 79.6% and 75.7%,espectively (Fig. 1).
Clinical and laboratory variables associated with mortal-ty in univariate Cox analysis were age, male sex, NYHAtage ≥ III, signs of RHF, Charlson Comorbidity Index, lowaemoglobin, renal failure and a diuretic dose > 125 mg/dayTable 4). In the multivariable Cox analysis, male sex, NYHAtage ≥ III, renal failure and a diuretic dose > 125 mg/dayemained independently associated with mortality (Table 4).
Echocardiographic variables associated with mortality inhe univariate Cox analysis were the presence of significanti.e. at least moderate) left-sided valvular heart diseasend the presence of RV systolic dysfunction (Table 5). Inhe multivariable analysis, only RV systolic dysfunction wasndependently associated with mortality (Table 5).
After pooling clinical, laboratory and echocardiographic
istics and prognosis of patients with significant tricuspid016/j.acvd.2019.06.011
ariables, only male sex (adjusted hazard ratio [HR] 1.93,5% confidence interval [CI] 1.14—3.75; P = 0.014), NYHAtage ≥ III (adjusted HR 1.58, 95% CI 1.01—2.65; P = 0.050)nd a diuretic dose > 125 mg/day (adjusted HR 1.66, 95% CI
IEN (948138). It is forbidden and illegal to distribute this document.
Data are expressed as mean ± standard deviation (continuous variables) or number (%) (categorical variables). ACE-I: angiotensin-converting enzyme inhibitors; ARB: angiotensin receptor blockers; BMI: body mass index; NYHA: New York Heart Association; RHF: rightheart failure; TR: tricuspid regurgitation. Group 1: primary TR; Group 2: TR secondary to left heart disease with previous left heartvalve surgery; Group 3: TR secondary to left heart or pulmonary disease without previous cardiac surgery; and Group 4: idiopathic TR.a P < 0.05 versus group 4.b P < 0.001 versus group 4.
1.03—2.87; P = 0.045) were independently associated withmortality.
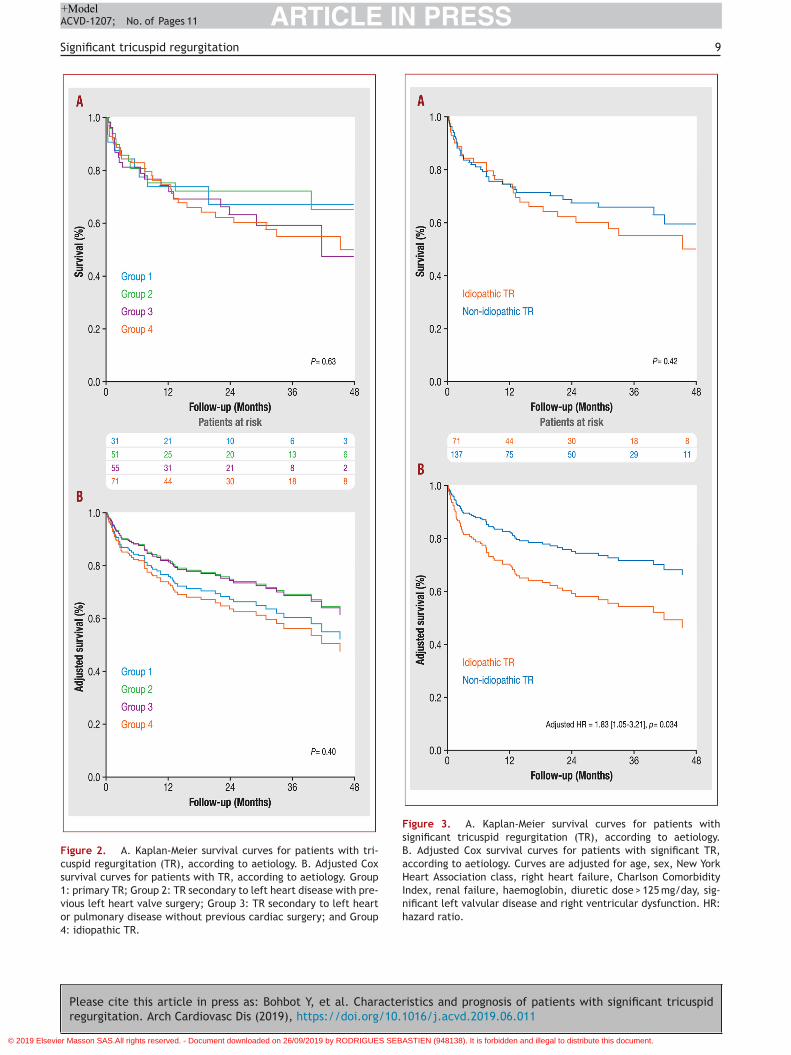
Four-year survival rates were 67 ± 7% for group 1, 65 ± 9%for group 2, 47 ± 11% for group 3 and 50 ± 7% for group 4 (log-rank P = 0.63) (Fig. 2A). In the multivariable Cox analysis,no significant difference in terms of survival was observedbetween the four groups (P = 0.40) (Fig. 2B), with no dif-ference between primary and secondary TR (P = 0.65) orbetween TR secondary to left heart or pulmonary disease(group 2 + group 3) and the other groups (P = 0.68).
In the Kaplan-Meier analysis, there was no significant dif-ference in terms of survival between patients with idiopathicTR and the rest of the population (P = 0.42) (Fig. 3A). How-ever, in the multivariable analysis, idiopathic TR (group 4)was independently associated with significant excess mor-tality compared with the other causes of TR (adjusted HR1.83, 95% CI 1.05—3.21; P = 0.034) (Fig. 3B).
RHF
During follow-up, 61 patients (29.3%) experienced at leastone episode of RHF decompensation requiring hospitaliza-tion: six patients in group 1 (18.8%); 16 patients in group 2(31.4%); 19 patients in group 3 (35.2%); and 20 patients in
Please cite this article in press as: Bohbot Y, et al. Characterregurgitation. Arch Cardiovasc Dis (2019), https://doi.org/10.1
group 4 (28.2%) (P = 0.43).In the univariate Cox analysis, clinical and laboratory
variables associated with RHF decompensation requiringhospitalization were: NYHA stage III or IV (HR 2.53, 95%
at
v
r Masson SAS.All rights reserved. - Document downloaded on 26/09/2019 by RODRIGUES SEBA
I 1.53—4.18; P < 0.001); history of RHF (HR 2.71, 95%I 1.51—4.89; P = 0.001); renal failure (HR 2.30, 95% CI.39—3.80; P = 0.001); and diuretic dose > 125 mg/day (HR.63, 95% CI 1.58—4.38; P < 0.001). In the multivariable Coxnalysis, after inclusion of all of the above variables andirrhosis (P < 0.10 in the univariate analysis), NYHA stage IIIr IV (adjusted HR 2.33, 95% CI 1.40—3.86; P = 0.001), his-ory of RHF (adjusted HR 2.40, 95% CI 1.32—4.34; P = 0.004),enal failure (adjusted HR 2.03, 95% CI 1.21—3.41; P = 0.007)nd diuretic dose > 125 mg/day (adjusted HR 1.90, 95% CI.12—3.21; P = 0.017) were independently associated withHF decompensation requiring hospitalization.
Echocardiographic variables associated with RHF decom-ensation requiring hospitalization in the univariate Coxnalysis were: LV dilatation (HR 1.82, 95% CI 1.08—3.07;
= 0.024); LVEF < 50% (HR 1.93, 95% CI 1.16—3.22; P = 0.011);V dilatation (HR 1.91, 95% CI 1.14—3.21; P = 0.015); righttrial dilatation (HR 2.31, 95% CI 1.19—4.48; P = 0.014); andV dysfunction (HR 1.89, 95% CI 1.14—3.13; P = 0.013). In theultivariable Cox analysis, after inclusion of all of the above
ariables and significant left valvular disease (P < 0.10 in thenivariate analysis), only right atrial dilatation (adjusted HR.09, 95% CI 1.22—4.29; P = 0.024) and LVEF < 50% (adjustedR 1.97, 95% CI 1.02—3.02; P = 0.043) were independently
istics and prognosis of patients with significant tricuspid016/j.acvd.2019.06.011
ssociated with RHF decompensation requiring hospitaliza-ion.
After pooling clinical, laboratory and echocardiographicariables, only NYHA stage III or IV (adjusted HR 2.38, 95%
STIEN (948138). It is forbidden and illegal to distribute this document.
Data are expressed as mean ± standard deviation. ERO: effective regurgitant orifice; IVC: inferior vena cava; LV: left ventricular; LVEF:left ventricular ejection fraction; TAPSE: tricuspid annular plane systolic excursion; TR: tricuspid regurgitation. Group 1: primary TR;Group 2: TR secondary to left heart disease with previous left heart valve surgery; Group 3: TR secondary to left heart or pulmonarydisease without previous cardiac surgery; and Group 4: idiopathic TR.a P < 0.001 versus group 4.b P < 0.05 versus group 4.
I 1.39—4.08; P = 0.002), history of RHF (adjusted HR 2.62,5% CI 1.43—4.79; P = 0.002), renal failure (adjusted HR.01, 95% CI 1.16—3.47; P = 0.012) and right atrial dilatationadjusted HR 2.11, 95% CI 1.24—4.49; P = 0.030) remainedndependently associated with RHF decompensation requir-ng hospitalization.
ardiovascular mortality and/or RHF
uring follow-up, 79 patients (38%) experienced at leastne episode of RHF decompensation requiring hospitaliza-ion (n = 61) and/or died of a cardiovascular cause (n = 41):0 patients in group 1 (32.2%); 17 patients in group 2 (33.3%);5 patients in group 3 (45.4%); and 27 patients in group
(38%) (P = 0.34). After pooling clinical, laboratory andchocardiographic variables, only baseline NYHA stage III orV (adjusted HR 1.96, 95% CI 1.23—3.14; P = 0.004), historyf RHF (adjusted HR 2.29, 95% CI 1.37—3.80; P = 0.002) andenal failure (adjusted HR 1.98, 95% CI 1.24—3.17; P = 0.004)emained independently associated with RHF decompensa-ion requiring hospitalization and/or cardiovascular death.
iscussion
he results of this study show that the causes of significantR are heterogeneous, but that all causes are associatedith poor outcome, as 69 patients (33.2%) had died at a
Please cite this article in press as: Bohbot Y, et al. Characterregurgitation. Arch Cardiovasc Dis (2019), https://doi.org/10.1
edian follow-up of 18 months, resulting in a much lowerurvival rate than expected (1-year and 4-year observedurvival rates of 74 ± 3% and 56 ± 4% versus expectedurvival rates of 93% and 74%, respectively). Moreover, 61
nspl
asson SAS.All rights reserved. - Document downloaded on 26/09/2019 by RODRIGUES SEBAST
atients (29.3%) experienced at least one episode of RHFequiring hospitalization. In the multivariable analysis,ale sex, NYHA stage ≥ III, renal failure and diureticose > 125 mg/day were associated with increased all-causeortality. After adjustment, idiopathic TR was associatedith a > 80% increase in the risk of all-cause mortality during
ollow-up compared with other causes of TR. Despite theact that TR is associated with a dismal prognosis, it remainsarkedly undertreated compared with left-sided valvular
eart disease, as tricuspid valve surgery was performed innly 5.3% of patients in our study.
etiology of TR
n agreement with previous studies [5,9,10,23], distribu-ion patterns show that TR secondary to left heart disease50.5%) was the leading cause of TR, and that primary TR15.4%) was the rarest cause. Patients with TR secondaryo left heart disease had dilated left ventricles, with moreeverely impaired LV and RV systolic function compared withhe other groups. Valve prolapse was the leading cause ofrimary TR. Messika-Zeitoun et al. [15] showed that TRaused by valve prolapse is most often traumatic and severe,nd can be treated successfully by surgery. Patients with pri-ary TR were younger, with fewer comorbidities and a lowerrevalence of atrial fibrillation, and less frequently requirediuretics compared with the other groups.
In our study, idiopathic TR was defined by structurally
istics and prognosis of patients with significant tricuspid016/j.acvd.2019.06.011
ormal tricuspid valves, no overt organic TR cause, no left-ided valvular or myocardial diseases or pulmonary disease,reserved LVEF and no previous valve surgery (tricuspid oreft-sided valve surgery). This form was frequent (34.1%),
IEN (948138). It is forbidden and illegal to distribute this document.
Please cite this article in press as: Bohbot Y, et al. Characterregurgitation. Arch Cardiovasc Dis (2019), https://doi.org/10.1
ARTICLE IN+ModelACVD-1207; No. of Pages 11
Significant tricuspid regurgitation
Figure 1. Survival of patients with significant tricuspid regurgi-tation compared with that in the age- and sex-matched generalpopulation. Relative survival was computed as the ratio of observed-to-expected survival (observed number of deaths in the studypopulation/expected number of deaths in the general population).
ab[wbcwafiirptsotdraagmarTsl
T
VTry
Table 4 Univariate and multivariable Cox analysis of clinical a
Variables All-cause mor
Univariate ana
HR (95% CI)
Age (per year) 1.02(1.01—1.0Male sex 1.74 (1.10—2.8Body surface area (per 0.1cm2 decrease) 1.39 (0.48—4.0NYHA stage (III—IV vs. I—II) 1.88 (1.16—3.0Hypertension 0.98 (0.57—1.6Coronary artery disease 1.18 (0.66—2.0Diabetes 0.74 (0.44—1.2Atrial fibrillation 1.47 (0.10—5.2Right heart failure 1.68 (1.03—2.7Cirrhosis 1.65 (0.70—3.8Charlson Comorbidity Index 1.10 (1.01—2.1Renal failure 2.57 (1 60—4.1Haemoglobin (per g/dL) 0.88 (0.78—0.9Diuretics dose > 125 mg/day 2.66 (1.65—4.2Tricuspid valve surgery 2.01 (0.72—5.5Previous left heart surgery 1.31 (0.75—2.2
CI: confidence interval; HR: hazard ratio; NYHA: New York Heart Assoc
nd more frequent than in previous reports, such as thosey Topilsky et al. [6], Mutlak et al. [9] and Kasai et al.24], in which idiopathic TR rates of 12%, 9.5% and 21%ere reported, respectively. This higher frequency coulde explained by the selection of only patients with signifi-ant (at least moderate-to-severe) TR. In our study, patientsith idiopathic TR were mostly women (63.4%), had a meange of 77 years, and more frequently had a history of atrialbrillation (88.7%), which is consistent with previous find-
ngs, suggesting a growing burden of idiopathic TR, thereforeequiring better understanding of this entity in order toropose appropriate treatment. Our results showed markedricuspid annular enlargement in the idiopathic TR group,imilar to that observed in the other groups. We includednly patients with moderate-to-severe and severe TR and, athis stage, regurgitation leads to right atrial and ventricularilation, and consequently tricuspid annular enlargement,egardless of the cause. However, we are convinced thatnnular dilation precedes regurgitation in idiopathic TR,s suggested by the prevalence of atrial fibrillation in thisroup, leading to progressive right atrial enlargement thatay contribute to annular dilation [6]. The mechanism of
nnular enlargement could also be linked to ageing, and mayeflect annular degeneration [6,25]. Patients with idiopathicR tended to be more symptomatic at baseline (25% in NYHAtage III—IV, 39% with a history of RHF), which may reflectate diagnosis because of poor knowledge of this entity.
R outcome
istics and prognosis of patients with significant tricuspid016/j.acvd.2019.06.011
arious studies have highlighted the poor outcome of severeR [7,8], with a direct relationship between the grade ofegurgitation and the risk of death [26]. In our study, 4-ear survival was only 56 ± 4%, with an excess mortality of
nd biological variables associated with all-cause mortality.
lmost 20% by the first year compared with the expectedurvival in the age- and sex-matched general population.linical and laboratory variables independently associatedith mortality were male sex, NYHA stage ≥ III, renal failurend diuretic dose > 125 mg/day. The only echocardiographicariable independently associated with mortality was theresence of RV systolic dysfunction, defined in accordanceith current guidelines [21]. Sun et al. [27] studied therognosis of 26 patients who underwent isolated tricuspidalve surgery for severe secondary TR, and reported anxcess mortality in patients with TAPSE < 14 mm. However,APSE and S’ should be interpreted with caution in patientsith previous cardiac surgery, as they can remain alteredven years after surgery without meaning RV dysfunction.umerous studies [6,26—28] have shown that primary andecondary TR are associated with poor prognosis. However,nly limited data are available concerning the prognosis ofdiopathic TR. The results of the present study show thatdiopathic TR is associated with a > 80% increased risk ofll-cause mortality during follow-up compared with otherauses of TR. Patients with severe idiopathic TR oftenresent numerous co-morbidities, as illustrated by the highean Charlson Comorbidity Index score of 3.6 in our study.
t is therefore difficult to know whether TR affects the prog-osis independently or whether mortality is mainly relatedo co-morbidities. However, in our study, although the Charl-on Comorbidity Index score was associated with mortalityn the univariate analysis, it was no longer associated in theultivariable analysis.Severe TR leads to RHF in the absence of surgical mana-
ement [29]. In our study, 61 patients (29.3%) experiencedt least one episode of RHF requiring hospitalization duringollow-up. Only baseline NYHA stage III or IV, history of RHF,
Please cite this article in press as: Bohbot Y, et al. Characterregurgitation. Arch Cardiovasc Dis (2019), https://doi.org/10.1
enal failure and right atrial dilatation were independentlyssociated with RHF decompensation requiring hospitaliza-ion. Worsening of TR leads to dilation of the right atrium andight ventricle, resulting in RV systolic dysfunction. These
Tav
asson SAS.All rights reserved. - Document downloaded on 26/09/2019 by RODRIGUES SEBAST
esults suggest that patients should be referred for surgeryt an earlier stage, before the onset of RV systolic dysfunc-ion and RHF.
ricuspid valve surgery
nly 11 patients in our study (5.3%) underwent tricuspidalve surgery during follow-up. Operative mortality is higheror tricuspid valve surgery than for other valves, proba-ly as a result of RV dysfunction and co-morbidities [30],s an in-hospital mortality rate of 10% has been reportedor isolated tricuspid valve surgery (ITVS) [6,31]. Accord-ng to the study by Dreyfus et al. [32], based on a nationaldministrative database, only 241 patients underwent ITVSn France during a 2-year period (2013—2014). ITVS wasssociated with high mortality (10%) and morbidity, with a5% rate of complications, including a 19% rate of majoromplications [32]. The authors concluded that patients areften referred for surgery too late, and that earlier inter-ention may consequently improve immediate and possiblyedium-term outcomes [32]. According to current European
uidelines [1], ITVS should be performed (class I; level of evi-ence C) in the presence of severe symptomatic TR withoutV dysfunction, and should be considered (class IIa; level ofvidence C) in the presence of asymptomatic TR with pro-ressive enlargement of the right ventricle, before the onsetf systolic dysfunction. Unfortunately, these guidelines arearely applied [12], and patients are operated on too late32], while earlier treatment would probably improve theirurvival [26]. In our study, only 11 patients (5.3%) underwentricuspid valve surgery during follow-up.
tudy limitations
istics and prognosis of patients with significant tricuspid016/j.acvd.2019.06.011
his study has the limitations inherent to retrospectivenalysis of follow-up data. The study sample size was notery large (n = 208), but corresponds to all consecutive
IEN (948138). It is forbidden and illegal to distribute this document.
Please cite this article in press as: Bohbot Y, et al. Characteristics and prognosis of patients with significant tricuspidregurgitation. Arch Cardiovasc Dis (2019), https://doi.org/10.1016/j.acvd.2019.06.011
ARTICLE IN PRESS+ModelACVD-1207; No. of Pages 11
Significant tricuspid regurgitation 9
Figure 2. A. Kaplan-Meier survival curves for patients with tri-cuspid regurgitation (TR), according to aetiology. B. Adjusted Coxsurvival curves for patients with TR, according to aetiology. Group1: primary TR; Group 2: TR secondary to left heart disease with pre-vious left heart valve surgery; Group 3: TR secondary to left heartor pulmonary disease without previous cardiac surgery; and Group4: idiopathic TR.
Figure 3. A. Kaplan-Meier survival curves for patients withsignificant tricuspid regurgitation (TR), according to aetiology.B. Adjusted Cox survival curves for patients with significant TR,according to aetiology. Curves are adjusted for age, sex, New YorkHeart Association class, right heart failure, Charlson ComorbidityIndex, renal failure, haemoglobin, diuretic dose > 125 mg/day, sig-nificant left valvular disease and right ventricular dysfunction. HR:hazard ratio.
atients diagnosed with significant TR in our echocardiogra-hy laboratory between 2013 and 2017. Further prospectiveulticentre studies are needed. Because right atrial vol-
mes were not reported in our database, we defined righttrial dilatation using right atrial area. However, volumesre more robust and accurate than areas for right atrial sizeetermination [21]. We used TAPSE and S’ to define RV dys-unction. However, those variables should be interpretedith caution in patients with previous cardiac surgery, as
hey can remain altered even years after surgery withouteaning RV dysfunction. Given the small number of patientsho underwent tricuspid valve surgery during follow-up, weould not test its impact on survival.
onclusions
he results of this study show that TR has various causes, butll forms of TR are associated with poor outcome. SecondaryR was the most common aetiology, and was mostly idio-athic, while primary TR was the rarest form. Patients withoderate-to-severe or severe TR have a markedly increased
isk of mortality compared with the general population.diopathic TR, a new entity that has not yet been studiedxtensively, has a poorer prognosis than the other aeti-logies. Prospective studies are needed to more reliablydentify patients at risk of developing idiopathic TR, to pre-ent its onset or at least prevent deterioration. Despite theact that TR is associated with a dismal prognosis, it remainsarkedly undertreated compared with left-sided valvular
eart diseases, as only 5.3% of patients underwent tricuspidalve surgery in our study. The development of transcatheterherapies might represent an alternative treatment optiono surgery in this high-risk population of patients with severeymptomatic TR [33].
ources of funding
one.
isclosure of interest
he authors declare that they have no competing interest.
eferences
[1] Baumgartner H, Falk V, Bax JJ, et al. 2017 ESC/EACTS Guide-lines for the management of valvular heart disease. Eur HeartJ 2017;38:2739—91.
[2] Calafiore AM, Bartoloni G, Al Amri H, et al. Functional tri-cuspid regurgitation and the right ventricle: what we do notknow is more than we know. Expert Rev Cardiovasc Ther2012;10:1351—66.
[3] Di Mauro M, Bezante GP, Di Baldassarre A, et al. Functionaltricuspid regurgitation: an underestimated issue. Int J Cardiol2013;168:707—15.
Please cite this article in press as: Bohbot Y, et al. Characterregurgitation. Arch Cardiovasc Dis (2019), https://doi.org/10.1
[4] Irwin RB, Luckie M, Khattar RS. Tricuspid regurgitation:contemporary management of a neglected valvular lesion.Postgrad Med J 2010;86:648—55.
asson SAS.All rights reserved. - Document downloaded on 26/09/2019 by RODRIGUES SEBAST
PRESSY. Bohbot et al.
[5] Topilsky Y, Maltais S, Medina Inojosa J, et al. Burden of tricuspidregurgitation in patients diagnosed in the community setting.JACC Cardiovasc Imaging 2019;12:433—42.
[6] Topilsky Y, Khanna A, Le Tourneau T, et al. Clinical contextand mechanism of functional tricuspid regurgitation in patientswith and without pulmonary hypertension. Circ CardiovascImaging 2012;5:314—23.
[7] Nath J, Foster E, Heidenreich PA. Impact of tricuspid regurgi-tation on long-term survival. J Am Coll Cardiol 2004;43:405—9.
[8] Sadeghpour A, Hassanzadeh M, Kyavar M, et al. Impact ofsevere tricuspid regurgitation on long term survival. Res Car-diovasc Med 2013;2:121—6.
[9] Mutlak D, Lessick J, Reisner SA, Aronson D, Dabbah S, AgmonY. Echocardiography-based spectrum of severe tricuspid regur-gitation: the frequency of apparently idiopathic tricuspidregurgitation. J Am Soc Echocardiogr 2007;20:405—8.
10] Prihadi EA, Delgado V, Leon MB, Enriquez-Sarano M, Topilsky Y,Bax JJ. Morphologic types of tricuspid regurgitation: charac-teristics and prognostic implications. JACC Cardiovasc Imaging2019;12:491—9.
11] Antunes MJ, Rodriguez-Palomares J, Prendergast B, et al. Mana-gement of tricuspid valve regurgitation: position statement ofthe European Society of Cardiology Working Groups of Cardio-vascular Surgery and Valvular Heart Disease. Eur J CardiothoracSurg 2017;52:1022—30.
12] Singh JP, Evans JC, Levy D, et al. Prevalence and clinicaldeterminants of mitral, tricuspid, and aortic regurgitation (theFramingham Heart Study). Am J Cardiol 1999;83:897—902.
13] Nishimura RA, Otto CM, Bonow RO, et al. 2017 AHA/ACCfocused update of the 2014 AHA/ACC guideline for the mana-gement of patients with valvular heart disease: a report of theAmerican College of Cardiology/American Heart AssociationTask Force on Clinical Practice Guidelines. J Am Coll Cardiol2017;70:252—89.
14] Arbulu A, Holmes RJ, Asfaw I. Tricuspid valvulectomy withoutreplacement. Twenty years’ experience. J Thorac CardiovascSurg 1991;102:917—22.
15] Messika-Zeitoun D, Thomson H, Bellamy M, et al. Medicaland surgical outcome of tricuspid regurgitation caused by flailleaflets. J Thorac Cardiovasc Surg 2004;128:296—302.
16] Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new methodof classifying prognostic comorbidity in longitudinal studies:development and validation. J Chronic Dis 1987;40:373—83.
17] Lancellotti P, Tribouilloy C, Hagendorff A, et al. Recommenda-tions for the echocardiographic assessment of native valvularregurgitation: an executive summary from the European Asso-ciation of Cardiovascular Imaging. Eur Heart J CardiovascImaging 2013;14:611—44.
18] Zoghbi WA, Adams D, Bonow RO, et al. Recommendationsfor noninvasive evaluation of native valvular regurgitation: aReport from the American Society of Echocardiography Devel-oped in Collaboration with the Society for CardiovascularMagnetic Resonance. J Am Soc Echocardiogr 2017;30:303—71.
19] Tribouilloy CM, Enriquez-Sarano M, Bailey KR, Tajik AJ, SewardJB. Quantification of tricuspid regurgitation by measuring thewidth of the vena contracta with Doppler color flow imaging:a clinical study. J Am Coll Cardiol 2000;36:472—8.
20] Tribouilloy CM, Enriquez-Sarano M, Capps MA, Bailey KR,Tajik AJ. Contrasting effect of similar effective regurgitantorifice area in mitral and tricuspid regurgitation: a quantita-tive Doppler echocardiographic study. J Am Soc Echocardiogr2002;15:958—65.
21] Lang RM, Badano LP, Mor-Avi V, et al. Recommendations forcardiac chamber quantification by echocardiography in adults:
istics and prognosis of patients with significant tricuspid016/j.acvd.2019.06.011
an update from the American Society of Echocardiography andthe European Association of Cardiovascular Imaging. Eur HeartJ Cardiovasc Imaging 2015;16:233—70.
IEN (948138). It is forbidden and illegal to distribute this document.
[22] Mahjoub H, Rusinaru D, Souliere V, Durier C, Peltier M, Tri-bouilloy C. Long-term survival in patients older than 80 yearshospitalised for heart failure. A 5-year prospective study. EurJ Heart Fail 2008;10:78—84.
[23] Rogers JH, Bolling SF. The tricuspid valve: current perspectiveand evolving management of tricuspid regurgitation. Circula-tion 2009;119:2718—25.
[24] Kasai A, Nishikawa H, Ono N, et al. [Clinical evalua-tion of severe idiopathic tricuspid regurgitation]. J Cardiol1990;20:937—44.
[25] Girard SE, Nishimura RA, Warnes CA, Dearani JA, Puga FJ.Idiopathic annular dilation: a rare cause of isolated severetricuspid regurgitation. J Heart Valve Dis 2000;9:283—7.
[26] Kelly BJ, Ho Luxford JM, Butler CG, et al. Severity of tricuspidregurgitation is associated with long-term mortality. J ThoracCardiovasc Surg 2018;155:1032—8 [e2].
[27] Sun X, Zhang H, Aike B, et al. Tricuspid annular plane systolicexcursion (TAPSE) can predict the outcome of isolated tricus-pid valve surgery in patients with previous cardiac surgery? J
Please cite this article in press as: Bohbot Y, et al. Characterregurgitation. Arch Cardiovasc Dis (2019), https://doi.org/10.1
Thorac Dis 2016;8:369—74.[28] Hung J, Koelling T, Semigran MJ, Dec GW, Levine RA, Di
Salvo TG. Usefulness of echocardiographic determined tricus-pid regurgitation in predicting event-free survival in severe
r Masson SAS.All rights reserved. - Document downloaded on 26/09/2019 by RODRIGUES SEBA
PRESS11
heart failure secondary to idiopathic-dilated cardiomyopathyor to ischemic cardiomyopathy. Am J Cardiol 1998;82:1301—3[A10].
29] Di Mauro M, Petroni R, Clemente D, et al. Clinical profileof patients with heart failure can predict rehospitaliza-tion and quality of life. J Cardiovasc Med (Hagerstown)2018;19:98—104.
30] Vassileva CM, Shabosky J, Boley T, Markwell S, Hazelrigg S.Tricuspid valve surgery: the past 10 years from the Nation-wide Inpatient Sample (NIS) database. J Thorac Cardiovasc Surg2012;143:1043—9.
31] Topilsky Y, Khanna AD, Oh JK, et al. Preoperative factors associ-ated with adverse outcome after tricuspid valve replacement.Circulation 2011;123:1929—39.
32] Dreyfus J, Ghalem N, Garbarz E, et al. Timing of referral ofpatients with severe isolated tricuspid valve regurgitation tosurgeons (from a French Nationwide Database). Am J Cardiol2018;122:323—6.
istics and prognosis of patients with significant tricuspid016/j.acvd.2019.06.011
current transcatheter tricuspid valve intervention: mid-termresults from the international TriValve registry. JACC Cardio-vasc Interv 2019;12:155—65.
STIEN (948138). It is forbidden and illegal to distribute this document.



















![Assessment of pathologic increase in liver stiffness ... · Patients with other diagnosed causes for chronic hepatobiliary diseases were excluded of this study [8]. All patients underwent](https://static.documents.pub/doc/80x56/5ecdba41a342de15e83c4058/assessment-of-pathologic-increase-in-liver-stiffness-patients-with-other-diagnosed.jpg)






