Charlene M. Dewey, M.D., M.Ed., FACP Co-Director, Vanderbilt Center for Professional Health William H. Swiggart, M.S., L.P.C./MHSP Co-Director, Vanderbilt Center for Professional Health Martha E. Brown, M.D. Assistant Medical Director, PRN UF Associate Professor of Psychiatry Proper Prescribing and Substance Abuse Identification: A CME Intervention
Transcript
Charlene M. Dewey, M.D., M.Ed., FACPCo-Director, Vanderbilt Center for Professional Health
William H. Swiggart, M.S., L.P.C./MHSPCo-Director, Vanderbilt Center for Professional Health
Martha E. Brown, M.D.Assistant Medical Director, PRN
UF Associate Professor of Psychiatry
Proper Prescribing and Substance Abuse Identification: A CME Intervention
All speakers acknowledge that they developed, teach, and operate CME courses (fee) for physicians and other health care providers on proper prescribing of CPDs.
COI
1: Discuss current information regarding controlled prescription drug abuse in the U.S., including how physicians continue to overprescribe to their patients
2: Become familiar with the components of screening, brief intervention and referral to treatment, (SBIRT)
3: Identify specific strategies to avoid risky prescribing to help physicians avoid trouble with their Boards or the DEA (including the use of the state prescription drug monitoring program and CME education)
Learning Objectives
Introduction Proper prescribing Continuing Medical Education interventions SBIRT Small group activity
Agenda
“To write a prescription is easy, but to come to an understanding with people is hard.”
~Franz Kafka A Country Doctor,1919
Introduction
“It is not what you prescribe, but rather how well you manage the patient's care, and document that care in legible form, that is important.”
~Released by the Minnesota MBE 1990, adapted by both the North Carolina and TN Boards of Medical Examiners
Introduction
The problem:Substance abuse, including controlled prescription
medication, is the nation's number one health problem affecting millions of individuals.4
Rate of controlled prescription drug (CPD) abuse has almost doubled from 7.8 million to 15.1 million in the past decade (1992 to 2003)2
New drug users of pain relievers-2.4 million. [marijuana (2.1 million) or cocaine (1.0 million)]
Up to 43% of physicians DO NOT ask about controlled prescription drug abuse when taking a patient's health history
Only 19% received any medical school training in identifying prescription drug diversion
Only 40% received training on identifying prescription drug abuse and addiction5
many are not trained to effectively handle drug-seeking patients
due to “confrontational phobia”- a term used to describe physicians’ reluctance to say “no” to a patient, thus making physicians an “easy target for manipulation.”5
Controlled Prescription Drug Abuse
Bollinger et al, 2005
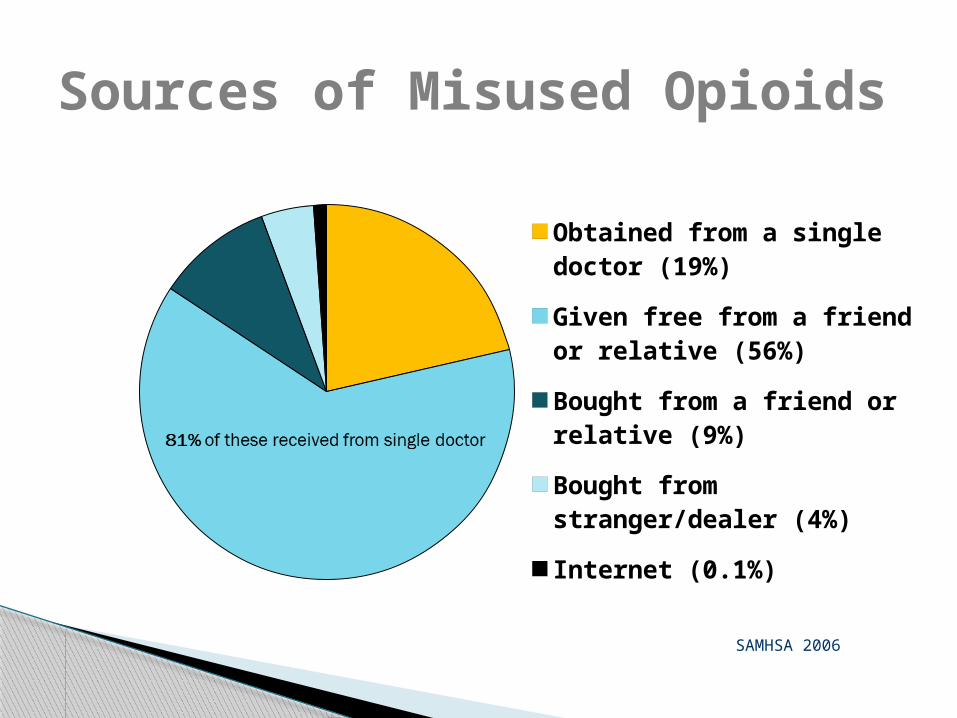
Obtained from a single doctor (19%)
Given free from a friend or rela-tive (56%)
Bought from a friend or relative (9%)
Bought from stranger/dealer (4%)
Internet (0.1%)
Sources of Misused Opioids
SAMHSA 2006
Definition: Prescribing scheduled drugs in quantities and frequency inappropriate for the patient’s complaint or illness.
Known alcoholic or drug addict Large quantities/frequent intervals Family members For trivial complaints
Misprescribing
Why Physicians Misprescribe Controlled Substances
Family of origin Core personality Patient types Pharmacological knowledge Professional practice system
Theories
DATED - fails to keep current
DISABLED - failed judgment due to impairment
DUPED - fails to detect deception
DISHONEST - personal or financial gain
DISMAYED - Rx as quick fix due to time constraints
DYSFUNCTIONAL - finds it hard to say NO
Categories of Misprescribing Physicians
ADDICTION TREATMENT WORKS
Addiction vs. Substance AbuseRelapse Rates vs. Other Chronic Diseases
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
DrugDependence
Type I Diabetes Hypertension Asthma
40%
to
60
%
30%
to
50
%
50%
to
70%
50%
to
70%
% o
f P
ati
en
ts w
ho
Re
lap
se
Average Age = 51
Male = 88%
Female = 11%
N = 715
Demographics
1940's 1950's 1960's 1970's 1980's 1990's 2000's
635
74
189
227
151
16
Medical School Graduation
January 1996 – March 2010
1%
5%
10%
27%
32%
21%
2%
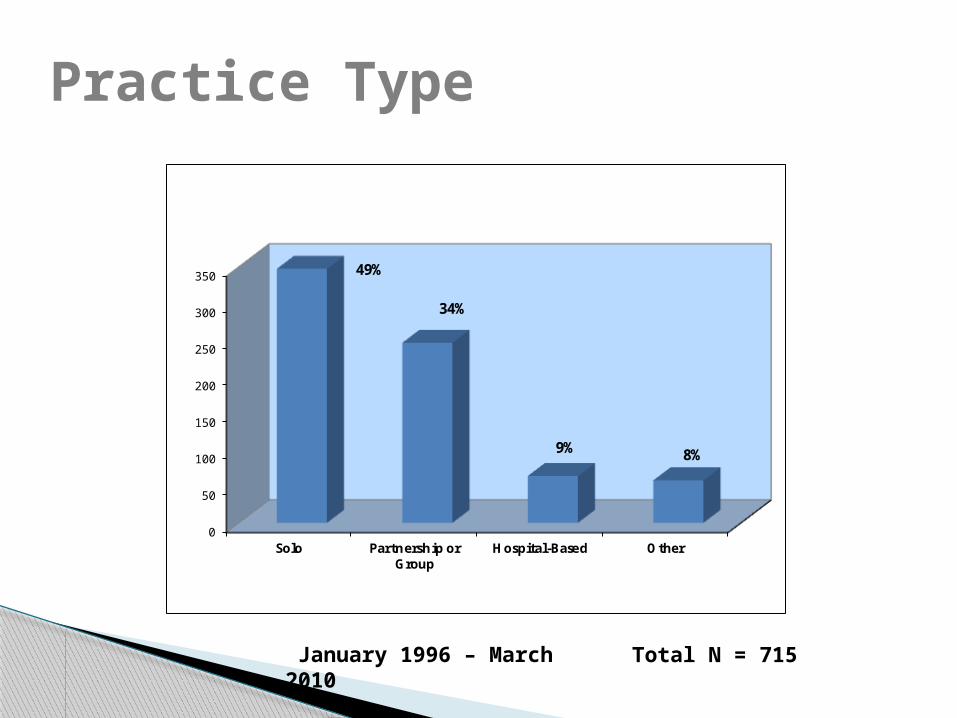
Practice Type
January 1996 – March 2010
Total N = 715
0
50
100
150
200
250
300
350
Solo Partnership orGroup
Hospital-Based Other
49%
34%
9% 8%
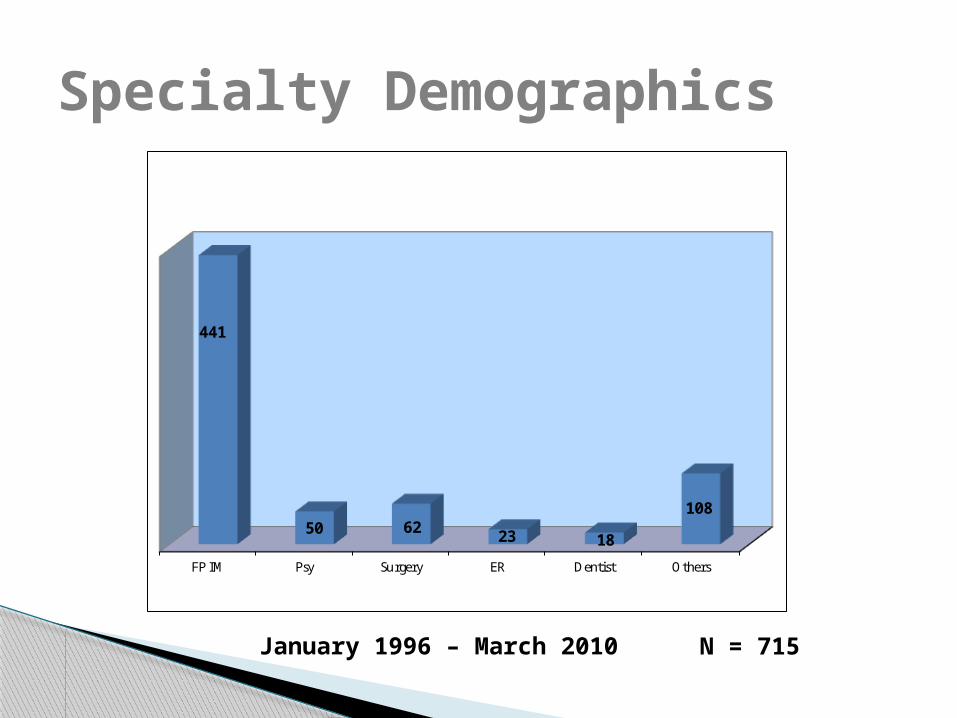
Specialty Demographics
January 1996 – March 2010
62%
7%
N = 715
FP IM Psy Surgery ER Dentist Others
441
50 6223 18
108
62%
7%9%
3% 3%
15%
Misprescribing can happen easily Many physicians are not trained to identify
substance abuse, diversion, or correct protocols for pain management
Medical Boards are becoming more punitive with physicians who misprescribe
DEA is scrutinizing prescribing practices and the flow of controlled substances
Education can be helpful and is imperative!
Challenges with Proper Prescribing
Provide fact-based education Treat pain effectively and safely Reduce contribution to diversion/misuse Use SBIRT to increase referrals and
interventions/treatments Recognize warning signs of abuse or misuse Avoid future misprescribing Assist with Medical Board requirements Avoid legal or professional sanctions by SMB or DEA
in future
CME Goals
61 of 69 physicians who completed the Prescribing Controlled Drugs Course at CPH strongly agreed that the course should be taught to all practicing physicians (3/2011-2/2012).
The overall average self score on ability to take a substance abuse history prior to the course on 69 physicians was 2.8 – compared to 4.6 after the course.
CME Course Evaluations
Additional education of physicians after residency is needed
Continuing Medical Education Courses proven helpfulPrescribing Controlled DrugsProgram for Distressed PhysiciansMaintaining Proper Boundaries (Vanderbilt)
Vanderbilt Center for Professional Health and University of Florida CME Initiatives
Small group Identify why/how physicians misprescribe Family Systems Personal reflection Role play of common patient presentations Syllabus of key lectures and readings Discuss practice organization Understand SBIRT and other tools
CME Course Elements
20 hour course to meet Board of Medicine requirements for pain management specialists in Florida scheduled for June 2012 (University of Florida)
Professional Development Series – On-line modules 2012-13 (Vanderbilt University Medical Center)
Future Initiatives
Screening, Brief Intervention and Referral to Treatment (SBIRT)
&Motivational Interviewing (MI)
SBIRTS Screening – Screening patients at risk for substance
abuse; inquiring about family history of addiction; using screening tools such as the NIAA 1-question screening tool for alcohol use, AUDIT, CAGE, CRAFT for adolescents, etc.
BI Brief Intervention - Establish rapport with pt.; ask permission; raise subject; explore pros/cons; explore discrepancies in goals; assess readiness to change; explore options for change; negotiate a plan for change-(motivational interviewing)
RT Referral to Treatment – For patients responding positively to the screening tests, refer to AA, drug addiction clinic, pain clinic, counseling, etc.
Screening, Brief Intervention and Referral to Treatment (SBIRT) is a well-studied screening and intervention procedure to improve patients’ short-term health outcomes and reduce health care costs.
The Joint Commission has proposed SBIRT as a performance measure for accreditation.
SBIRT: Introduction
SBIRT
Proposed Accreditation Standards Could Compel U.S. Hospitals to Screen Patients for Addictions (Bob Curley, 9/11/09)
Individual and family history“Have you ever used or currently use….[fill in the blank]?”
tobacco, ETOH, marijuana, street drugs, prescription drugs or other recreational drugs
Identify & quantify use
Within your family, has anyone ever used or currently use…
Use standard form/tests:5 A’sCAGE, AUDIT, DAST, MAST, CRAFT, ASSIST, etc.Combination: SMaRT
35 year-old female with fibromyalgia and low back pain who is requesting opioids for pain management
Things to watch for: Red flags to indicate aberrancy/addiction Techniques to elicit relevant history in a patient with pain How to deal with an angry, demanding patient Technique for screening, referral, and brief intervention
(SBIRT)
SBIRT Demonstration: DVD
Adopted from: Jackson T, Dewey C, Swiggart W, Baron M and Moore D. Guidelines for Proper Opioid Prescription. Vanderbilt University School of Medicine 2009
SBIRT Demonstration
DVD SBIRT Discussion
Break into small groups Discuss question Prioritize two ideas per group Two minute report out Large group discussion
Small Group Activity
Statements: Legal issues and consequences for misprescribing are becoming more prevalent. The Joint Commission is considering requiring SBIRT as a quality indicator.
Question: How might you involve your state to require physician training in SBIRT, use of the PDMP for all patients, and training proper prescribing practices to avoid misprescribing and consequences of misprescribing?
The Future
More states are passing laws that regulate prescribing:
Regulations for pain clinics Regulations for who can prescribe CME hours required in order to prescribe long-term
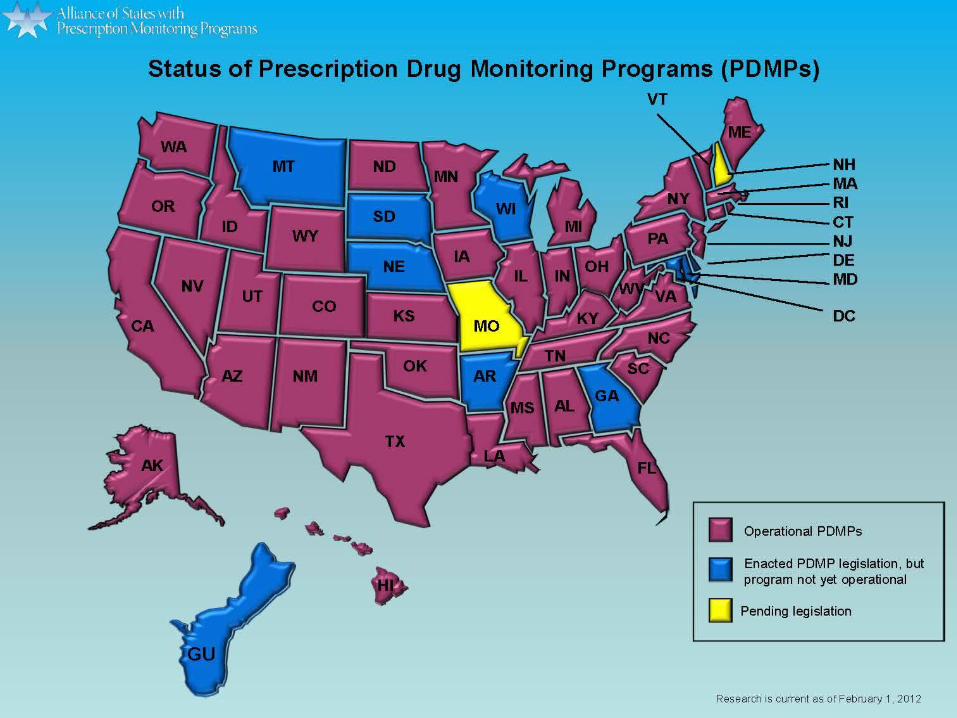
narcotics Laws making diversion for own use a possible felony State Prescription Drug Monitoring Programs
Legal Issues and Consequences
Continue to push for additional education of our medical students and residents
Raise awareness of DEA rules and changes that occur http://www.deadiversion.usdoj.gov
Implement laws on regular use of State Prescription Monitoring Program http://www.pmpalliance.org
Monitor state laws and regulations that may be draconian with education of legislators
Strategies to Help Physicians
Most physicians are not bad physicians but lack: information tools to deal with patients who have substance
abuse or difficult pain issues resources
Small group education can make a difference Prevention is first priority
Lessons Learned
Reviewed guidelines and regulations Described CPD problem Discussed SBIRT Reviewed CME courses and benefits Planned for improvements in each state Reviewed consequences and future directions
Summary
The Center for Professional Health, Vanderbilt University Medical Center, Nashville, TN. www.mc.vanderbilt.edu/cph
Prescribing Controlled Drugs: Critical Issues & Common Pitfalls of Misprescribing, The University of Florida at Gainesville, FL. http://ufcme.info/Misprescribing.html