24
1 Chemotherapy with Renal and Hepatic Insufficiency Mason Assaf ,Pharm.D,RPh Clinical pharmacist King Faisal Specialist Hospital & Research Centre

1
Chemotherapy with Renal and Hepatic Insufficiency
Mason Assaf ,Pharm.D,RPh
Clinical pharmacist King Faisal Specialist Hospital & Research Centre

2
Chemotherapy and Renal Insufficiency Introduction: many chemotherapy agents are nephrotoxic, either acute or chronic renal impairment (e.g., cisplatin) or specific renal lesions (e.g., ifosfamide). Some chemotherapy agents are not usually nephrotoxic but may become so under certain circumstances (e.g. methotrexate). In the presence of renal insufficiency other drugs or their metabolites excreted by the kidney may accumulate and exert more significant systemic toxicities than usual (e.g. cytarabine). Finally, any chemotherapy agent may induce renal failure, acid-base disorders or electrolytes abnormalities as a result of a dramatic response to therapy, as characterized by rapid tumor lysis syndrome or it is called acute uric acid nephropathy. Clinical Presentation (1)
A. Acute renal failure is defined as a sudden decrease in GFR leading to an acute rise in blood urea (BUN) and serum creatinine (SCr) levels.
1- Renal impairment in patients with malignant diseases is the major source of morbidity and mortality, particularly in the elderly patients. Patients may be under or over-dosed
B. Types of acute renal dysfunction (Please see the table below) (2) 1- Pre-renal sec to hypo perfusion, hypovolemia, increased Scr, BUN, and
decreased Na excretion 2- Intrinsic renal dysfunction, wasting electrolytes, renal tubules acidosis,
decrease in the rate of GFR, increasing excretion of uric acid (UA), amino aciduria, glucosuria, small amount of protein and loss ability of concentrating urine.
3- Fanconi syndrome differs from intrinsic renal dysfunction, it is common with ifosfamide, and it is proximal tubular dysfunction, increase excretion of amino acids (AA), bicarbonate, glucose, phosphates, K, Na, and UA.
4- Post-renal-mechanical obstruction of urine outflow (e.g. MTX) 5- Chronic RF, caused by chemotherapy such as nitrosoureas, patients may
present with slowly progressive elevation of SCr with or with out renal tubular dysfunction syndrome.
A c u t e Renal Failure Others Drugs Pre-renal ATN TTP-
HUS Obstructive Renal
tubule dysfunction
Chronic RF
Aminoglycosides √ √ Amphotericin-B √ √ √ CDDP √ Cyclosporine √ √ Cyclophosphamide √ Foscarnet √ √ √ Ifosfamide √ √ Mannitol √

3
Mitomycin C √ Methotrexate √ FK-506 √
TTP-HUS =Thrombotic Thrombocytopenic Purpura-Hemolytic Uremic syndrome
C. Risk factors developing renal impairment in Cancer patients. (3) 1- Tumor types such as multiple myeloma (MM)-(pre-renal), prostate (post-
renal), high grade lymphoma, AML, ALL, and Wilms’ tumor are all have the potential causing renal impairment.
2- Hypovolemia-poor intake, hypovolemia, N/V sec to chemotherapy 3- Age – elderly and children with age 3-5 years of age high risk for renal
impairment. (Please see the tables 1 and 2 listed below). Older patients with cancer are particularly at risk for adverse drug events because in addition to chemotherapy, the patients may be taking supportive-care medications ( anticholinergic, dexamethasone)
4- Febrile neutropenia with bactermia 5- Contrast agents used in cancer staging 6- Transplant patients increased risk for acute renal impairment.
Table-1: Physiologic changes and consequences of chemotherapy associated with aging in Elderly patients with cancer (4)
Physiologic change Consequence of chemotherapy
Slower repair of DNA damage Prolonged toxicities (BM) Reduced stem cell mass & hematopoiesis Slow recovery of blood and mucosal Reduced functional reserve of organs systems
Risk for organ failure
Reduced GI absorptive surfaces, gastric motility, and gastric secretion
Reduced chemotherapy absorption
Reduced fat-free mass Altered drug distribution Greater anemia Increased levels of circulating drugs Decreased liver mass Reduced drug metabolism Decreased nephron mass (25-30%), ↓ GFR by 0.75-1 ml/min per year after age of 40, Cr stabilized due to loss of muscle mass
Reduced drug excretion

4
Table 2: Relationship of age and the pharmacokinetics of common chemotherapy drugs Study No. of
Patients Age Drug Dose/schedule results
Lichtman et al (5)
122 Range 46-86
Paclitaxel 175mg/m2 over 3h q 3 wk
↑AUC with↑ in age, ↓ clearance
Smorenburg et al. (6)
23 Med 77 Paclitaxel 80mg/m2 iv over 1 hour wkly for 3 wks
↑ with age ↓ clearance of unbound and total paclitaxel
Bruno et al 640 Not specific Docetaxel Not specific Small↓ clearance Ten Tije et al (7)
40 Range 65-80
Docetaxel 75mg/m2 iv over 1 hour q3ks
No associations of age with AUC or clearance
Sorio et al (8)
10 Median 70, range 66-81
Vinorelbine 30mg/m2 day1 and 8 q 3wks
No age difference in PK, no correlation between age and drug-toxicity
Milano et al (9)
380 Med-62, range 25-91
5-FU 1Gm/m2 CIV infusion day 1-5+ CDDP 100 mg/m2 (1 mg/min)
No association of age with 5-FU clearance, female lower clearance of 5-FU
Bressolle et al (10)
62 Cohort 1 38, range 65-83, cohort 2 range 21-45
MTX 7.5-15 mg IM wkly
Age inversely proportional to the clearance of free and total MTX
Toffoli et al (11)
50 Range 50-83
VP-16 100mg PO for 14 days q 3wks
No age related difference in pharmacokinetics when CrCl was accounted for
Li et al (12) 56 Med 50, range 12-74
Doxorubicin Med 50mg/m2, range 30-75mg/m2
Older age associated with lower early clearance due to decreased distribution clearance and lower total body clearance of doxorubicin, patients older than 65 yrs experience greater risk incidence of CHF.
Jen et al (13)
445 Mean 50 range 19-82
Temozolomide Oral
Phase-II 150mg-200mg/m2 for 5 days q28 days
No association between age and PK neutropenia & thrombocytopenia associated with age and gender
5
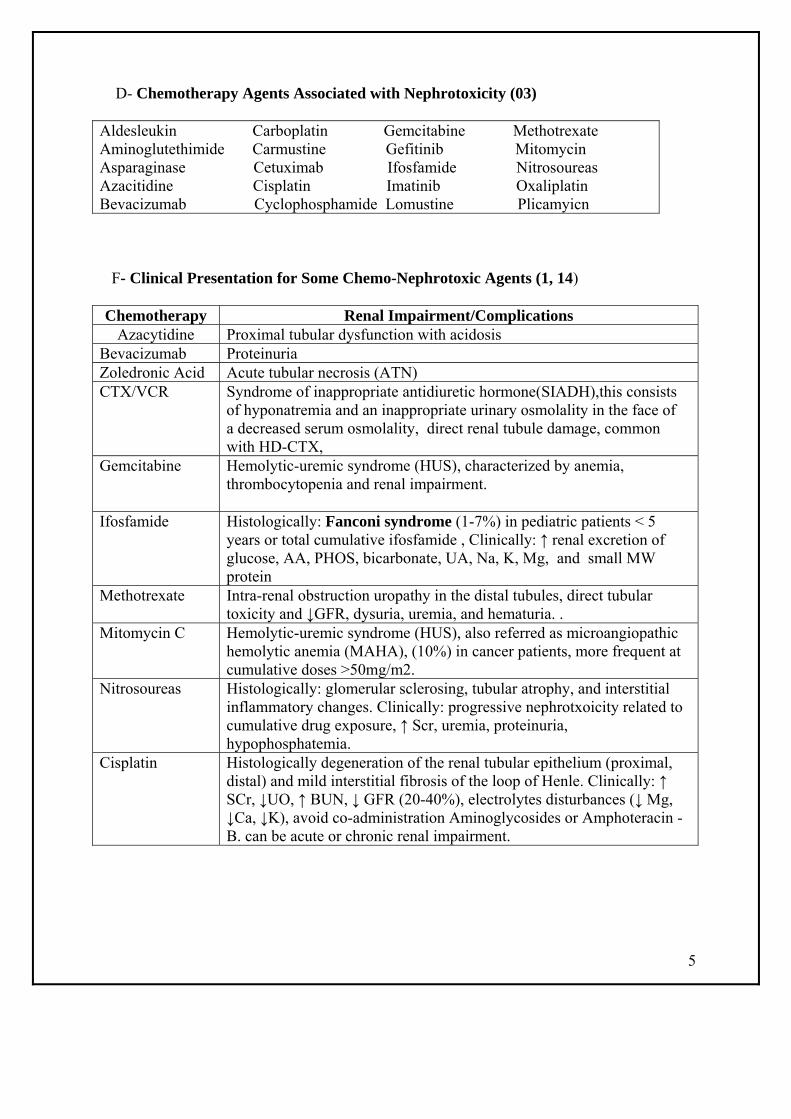
D- Chemotherapy Agents Associated with Nephrotoxicity (03) Aldesleukin Carboplatin Gemcitabine Methotrexate Aminoglutethimide Carmustine Gefitinib Mitomycin Asparaginase Cetuximab Ifosfamide Nitrosoureas Azacitidine Cisplatin Imatinib Oxaliplatin Bevacizumab Cyclophosphamide Lomustine Plicamyicn
F- Clinical Presentation for Some Chemo-Nephrotoxic Agents (1, 14) Chemotherapy Renal Impairment/Complications
Azacytidine Proximal tubular dysfunction with acidosis Bevacizumab Proteinuria Zoledronic Acid Acute tubular necrosis (ATN) CTX/VCR Syndrome of inappropriate antidiuretic hormone(SIADH),this consists
of hyponatremia and an inappropriate urinary osmolality in the face of a decreased serum osmolality, direct renal tubule damage, common with HD-CTX,
Gemcitabine
Hemolytic-uremic syndrome (HUS), characterized by anemia, thrombocytopenia and renal impairment.
Ifosfamide Histologically: Fanconi syndrome (1-7%) in pediatric patients < 5 years or total cumulative ifosfamide , Clinically: ↑ renal excretion of glucose, AA, PHOS, bicarbonate, UA, Na, K, Mg, and small MW protein
Methotrexate Intra-renal obstruction uropathy in the distal tubules, direct tubular toxicity and ↓GFR, dysuria, uremia, and hematuria. .
Mitomycin C Hemolytic-uremic syndrome (HUS), also referred as microangiopathic hemolytic anemia (MAHA), (10%) in cancer patients, more frequent at cumulative doses >50mg/m2.
Nitrosoureas Histologically: glomerular sclerosing, tubular atrophy, and interstitial inflammatory changes. Clinically: progressive nephrotxoicity related to cumulative drug exposure, ↑ Scr, uremia, proteinuria, hypophosphatemia.
Cisplatin Histologically degeneration of the renal tubular epithelium (proximal, distal) and mild interstitial fibrosis of the loop of Henle. Clinically: ↑ SCr, ↓UO, ↑ BUN, ↓ GFR (20-40%), electrolytes disturbances (↓ Mg, ↓Ca, ↓K), avoid co-administration Aminoglycosides or Amphoteracin -B. can be acute or chronic renal impairment.

6
G- Chemotherapy Agents excreted by the kidney, in renal insufficiency may accumulate to cause enhanced toxicity. (03)
Bleomycin Dacarbazine Melphalan Carboplatin Etoposide Methotrexate (High-Dose) Cisplatin Hydroxyurea Nitrosoureas Cytarabine (High-Dose) Ifosfamide Pentostatin Topotecan
H- Chemotherapies agents may cause renal failure, acid/base disturbances or electrolytes abnormalities as a result of dramatic response to therapy (tumor lysis syndrome). This topic will be covered by other Clinical Pharmacists under the oncologic-emergencies sections.
I- Prevention of Nephrotoxicity (3,15) 1- Cisplatin
Eliminated primarily (>90%) in the urine and it self highly nephrotoxic. It is mandatory to evaluate renal function either calculated Cr or urine collection to calculate CrCl. Hydration with NS, hypertonic saline infusion and mannitol to keep UO 125ml/hr. There are various hydration regimens but no evidence to recommend one over others. Vigorous hydration reduces but does not eliminate the risk of renal damage caused by cisplatin. The risk factors for cisplatin toxicity are hyperuricemia, Hypoalbuminemia, and inadequate pre-hydration. Patients with older than 70 years of age with out significant co-morbidity and a good performance status should able to tolerate approximately 60mg/m2 of cisplatin without significant toxicity. Amifostine may provide some protection against cisplatin-induced nephrotoxicity, neurotoxicity, and Ototoxicity, which may improve the therapeutic index in the elderly patients.
2- Ifosfamide The toxicity seen more in children may be due to chloroacetaldehyde, a metabolite of ifosfamide. The risk factor include high doses > 60mg/m2, the recommended cumulative dose 80mg/m2, the young age < 5 years, previous or concurrent Carboplatin or cisplatin, previous renal irradiation, single kidney, and history of surgical nephrectomy.
3- Methotrexate The ant metabolite methotrexate is not normally toxic to the kidney, although 90% of the drug is excreted unchanged in the urine. Nephrotoxicity observed high dose of methotrexate can delay methotrexate clearance and markedly intensify the drug‘s other toxic effects. The renal damage related may be related to precipitation of methotrexate or 7-hydroxy-methotrexate in acidic urine or to direct effects on the renal tubules. Drug precipitation can be prevented by vigorous IV hydration and alkalinization of the urine. The risk factors include inadequate pre and post hydration, urine pH< 7. Impaired renal function will predispose patients to renal

7
toxicity. The dose of methotrexate should be adjusted based on patient's renal function. Patients with pleural effusions or ascites are at risk for prolonged drug elimination and toxicity
4- Nitrosoureas (Carmustine, Lomustine, sesmustine, streptozocin) The cumulative doses of nitrosoureas more than 1500mg/m2 associated with progressive renal atrophy, this complication in children has been seen with sesmustine (methyl-CCNU). The renal tubule disease frequently occurs after the completion of chemotherapy and can be unfortunately irreversible toxicities.
5- Carboplatin The nephrotoxic potential of Carboplatin appear to be less than that of Cisplatin, hyponatremia secondary to increased urinary loss can occur but it is reported rarely. Renal tubules damage has occurred followed treatment with Carboplatin. The Carboplatin dosage should be routinely calculated according the Calvert formula in adult cancer patients. The dose of Carboplatin should always be always based on GFR rather than BSA. Vigorous hydration (3L/m2) should be used with high dose regimens.
6- Cyclophosphamide and Vincristine The incidence of SIADH may be decreased with careful monitoring of serum Na, weight, and urine output with rapid diuresis if necessary.
7- Cytarabine (Ara-C) Reduction in the dose of high-dose Ara-C is highly recommended in patients with renal impairment will decrease the incidence of Neurotoxicity, the alteration in renal function in elderly patients contribute to the increased toxicity of HD-Ara-C and its metabolites Ara-U.
Summary Specific Measures to Prevent Renal Toxicities from Potential Nephrotoxic Agents Listed above. (16)
1- Hydration status should be optimized and renal function evaluated to establish possible need for dose adjustment, serum Cr is not sufficient in assessing renal function.
2- Cockcroft-Gault and Jelliffe equations are available to calculate CrCl in younger patients with normal renal function. However, in older patients, these equations are not accurate.
3- Within each group class, preference may be given to agents that are less likely to be influenced by renal clearance.
4- Or, within each drug class, preference may be given to agents that are less toxic to the kidneys or for which there are ways to prevent renal toxicity.
5- Co administration of known nephrotoxic drugs, such as NSAIDS, Cox-2 inhibitors, or penicillin antibiotics Bactrim or Septra with HD-MTX should be avoided, high risk for delay excretion of MTX, leads to developing mucositis.

8
K- Chemotherapeutics Drugs do not require Dose Modifications in Renal Failure Patients (03) Actinomycin D Gemcitabine Paclitaxel Amsacrine Idarubicin Procarbazine Busulfan Melphalan PO Teniposide Docetaxel 6-MP (???) 6-TG 5-FU Mitoxantrone Vinblastine/ VCR/Vinorelbine L- Chemotherapy Agents Requiring Dose Modifications in Renal Failure (03, 17)
Drug >60ml/min 30-60ml/min 10-30ml/min <10ml/min Bleomycin NC 50% Omit Omit Carboplatin Use Calvert Formula to Calculate the Dose Cisplatin NC 50 Omit Omit CTX NC NC NC 50 Ara-C NC 50 Omit Omit DTIC NC 75 50 Omit VP-16 NC NC NC 50 Fludarabine NC 75 50 Omit Hydroxyurea NC 75 75 50 Ifosfamide NC 75 50 Omit Melphalan (IV) NC 75 75 50 MTX NC 50 Omit Omit Mithramycin NC 75 50 Omit Mitomycin C NC 75 50 Omit Nitrosoureas NC Omit Omit Omit Pentostatin NC 50 Omit Omit Topotecan NC 75 50 Omit The chemotherapy agents requiring dose modifications in renal impairment patients according to the British Royal College of Radiologist. Please see the table on below; they are slightly different from above table. (18)

9
M- Measurement of Renal Function It is typically has been on the basis of SCr levels, Cr endogenous compound produced mainly from muscle catabolism and released into blood, the amount is relatively stable in a given person. The rate of SCr production is affected by body mass muscle, muscle mass, diet, drugs, age, and fluid status of patients. SCr should be interpreted with caution in clinical practice. It should not be used as a "standalone" marker of renal function but should be only be used in conjunction with other parameters. Degree of GFR Rate Decrease (16) Stage Description GFR(ml/min/1.73m2) 1 Kidney damage with normal or increased GFR >90 2 Mild decrease in GFR >60-89 3 Moderate decrease in GFR 30-59 4 Severe decrease in GFR 15-29 5 Kidney failure <15 or dialysis Cr Clearance (16)
1- Estimating of CrCl by measurement of Urine Cr over-24h period. It is lengthy and most of time inaccurate and overestimate of GFR because Cr is secreted as well as filtered.

10
2- Formula to estimate CrCl
A- Cockcroft-Gault (C-G Formula) method was derived from a dataset of 249 non-cancer men, all of whom were inpatients in a veteran's hospital. From 19 up to 92 (mean 57). The C-G formula was not derived in an elderly cancer-specific population, significant underestimation of GFR for decreasing renal function. The formula is not considered to be reliable for obese or edematous patients. The C-G formula approximation underestimates GFR for normal and moderately reduced levels of renal function. For patients with significantly impaired renal function, the C-G overestimates renal function. In the elderly, the C-G formula was shown to produce a consistently low estimate of GFR.
B- The Jelliffe Formula The Jelliffe formula was derived in a group of male and female patients without cancer who had undergone renal transplantation and assumes a 10% reduction in CrCl for female patients. The inaccuracy of the Jelliffe formula is similar to the C-G formula.
C- The Wright formula and Martin formula. The population pharmacokinetics approach was used in the development of Wright or Martin formula; the data were derived from patients with cancer A retrospective analysis of a larger cohort of elderly cancer patients demonstrated the Wright formula to be the most precise and least biased formula over a range of GFR levels
3- Calculations CrCl in Pediatric Patients
A-Swartz Creatinine Clearance Equation
CLCR = (k x Ht) / SCr . . . where Ht is height (length) in cm . . . SCr is the most recent serum Cr . . . k = 0.45 if age < 1 year . . . k = 0.55 if age 1-12 years . . . BSA is body surface area
B-Traub's equation:
CrCl=0.48 x Ht x BSA/ Scr X (0.0113) X 1.73 CrCl = creatinine clearance in ml/min/1.73 m2 Ht = height in cm SCr = serum creatinine in mg/dl This equation can be used for children ages 1 - 18 years. It is less accurate with heights < 107 cm. An equal number of CrCl are over and under estimated with this equation. Traub et al. Amer J Hosp Pharm 1983; 40:107-10

11
Formulas for Calculating CrCl in Adult Patients (16)
Dialysis of Chemotherapy (19)
Agent Hemodialysis Peritoneal dialysis Aminoglutethimide Yes Unknown Bleomycin No Unknown Carboplatin Yes No Carmustine No Unknown Cisplatin Yes Unknown CTX Yes Unknown Cytarabine Unknown No Doxorubicin No No info Etposide No No info 5-FU May be Lomustine No MTX Yes NO Teniposide No No Topotecan Yes Known

12
Patients Cases
Case #1 MC is 1.5 yrs Saudi male diagnosed with testicular germ cell, which Revealed advanced disease. He has received 2 cycles BEP and now due to 3rd cycle he returns to CCC clinic prior admission and is found to have the Following WBC=4, Poly=60%, mono=20%, eosinophils =2%, band=5%, BUN=16.5, SCr=115, Na=136 , K=2.9, Mg=0.65, CL=104, CO2=22 A- proceed with hydration and hold chemo B-proceed with hydration+ Mannitol + and chemo full dose C-proceed with hydration+ Mannitol+ and modified Chemo D-proceed with chemo as written previously during cycle 1 &2
Case #2 NS is 11 yrs Saudi F diagnosed with left tibia OS, she is to begin today Ifosfamide (5 days) + doxorubicin (3 days) , the patient recently completed two weeks of Gentamicin, Vancomycin, and Tazocin to treat polymicrobial bactermia, her chemistry Na= 138, K=3.8, Glucose= 3.6, Scr= 150, ALT=40, Tot Bili=40. A- NS should have her dose of Doxo and Ifos decreased B- NS should have her dose of Ifos decrease only C- NS should receive the recommended dose per chemo protocol D- NS should receive decreased dose of doxorubicin
Case #3 13.5 y/o with RMS who will be receiving IFOS 1.8gm/m2 Daily x 5 days, BSA=1.89m2. What is the correct dose of Mesna to be administered to this patient. A- 680mg IV prior to Ifos followed up by 680mg @ 4 and 8 hrs post Ifos infusion. B- 680mg prior to Ifos followed by CIV of 1360mg for 12-24hrs after completion Ifos Infusion C- 1360mg PO prior to Ifos followed up by 680mgIV @ 2h and 1360mg PO @ 8hrs D-680mg IV prior to Ifos followed by 680mg po at 4 and 8hrs

13
Case #4 TT 40 y/o F AML admitted to receive cycle #1 (day 0) of chemotherapy Consolidation high dose Ara-C 3gm/m2 q12h x 4 doses, patient's renal profile and hepatic enzymes function as follow: Na= 138, K=3.8, Cl =102, Scr= 75µM/L, ALT= 45, Tot bilirubin= 22, ALP= 160, another patient SS 55 y/o M diagnosed with AML was admitted in the next room is scheduled to receive cycle #2 (day 7) high dose Ara-C 3gm/m2 q12h x 4 doses , his labs as follow: Na= 136, K= 3.6, Cl =101, CO2=23, Cr=65 , ALT=85, AlP=150, tot bilirubin = 35. Prior receiving the 4th dose of Ara-C, TT’s repeated labs results as follow: Na=136, K=3.5, Cl =100, Scr =280µM/L 5, ALT= 120, Tot bilirubin=45, ALP=165, for SS’s repeated results labs as follow: Na=135, K=3.4, Cl =99, Scr = 90µM/L, ALT =250, ALP=350. Which patient has the potential to be transferred to ICU and why?
A- TT and SS should be transferred to ICU B- SS should go and TT should stay C- TT should go and SS should stay D- SS and TT should receive the 4th dose Ara-C without Dose modifications.
Hepatic Function and Chemotherapy (22)
The liver has a central role in the metabolism and detoxification of many chemotherapeutics agents and is therefore a target for drug toxicity. It is important to distinguish drug causes from viral hepatitis or tumor-related effects of hepatic abnormality. Further more, agents that depends on the liver for metabolism. Thus, to reduce toxicity it becomes necessary to modify therapy with therapeutic agents with liver dependent metabolism. The chemotherapy-induced liver toxicity is variable. Some agents cause reversible toxicity while others are associated with a progressive course that can lead to chronic liver impairment (e.g. fibrosis or cirrhosis) despite drug discontinuation. There are insufficient data to make rational validated dose modifications for most cytotoxic drugs in patients with liver dysfunction. Clinical trials are needed specifically to address the issue of dose modifications in the presence of hepatic impairment. Risk factors for Hepatotoxicity
1- Altered clearance resulting from decreased hepatocyte uptake or impaired liver blood flow.
2- Altered biliary excretion 3- Altered metabolic capacity 4- Decreased albumin production resulting in increased free drugs.

14
Pathophysiology (3)
1- Primary or metastatic tumor ( paraneoplastic associated with cholestasis) involvement of the liver- Please see Table below
2- Hepatotoxic drugs(e.g. cytotoxic, hormones, antiemetics ( phenothiaznes), antibiotics (INH, rifampin)
3- Infections (e.g. hepatic candidiasis, viral hepatitis) 4- Total parenteral nutrition (TPN) 5- Allopurinol
Hepatotoxicity from chemotherapy (23) Drug Agent Dosage Regimens Prevalence Type of toxicity Asparaginase 3 -5 times/week Frequent Hepatocellular liver
steatosis, decreased lipoprotein synthesis
Carmustine Wkly bolus, or daily
Common Hepatocellular
Cytarabine High dose q12h x4 Rare Cholestatic DTIC Daily x 5 Infrequent Hepatocellular VP-16 High dose (BMT) Common Hepatocellular 6-MP DAILY (ALL-
maintenance) Common?? Cholestatic
MTX Daily (PO) Weekly HD-MTX
Common Rare uncommon
Hepatocellular, fibrosis/cirrhosis with chronic oral
Mitomycin C HD Uncommon VOD 6-TG Daily ( ALL) Uncommon VOD Tumors Associated with Paraneoplastic Cholestasis Renal cell carcinoma NHL prostate carcinoma Medullary thyroid cancer HL Schwannoma Wilms' tumor GI carcinoma LCH Cytotoxic where specific dose modifications should be considered (22) Total drug exposure and toxicity are increased in patients with liver dysfunction treated with anthracyclines, vinca alkaloids, taxoids and irinotecan. Dose should be considered. Most studies do not distinguish between liver dysfunction caused by cancer (e.g. breast, germ cell, lymphoma, Langerhan’s Cell Histiocyctosis)

15
Drug Class of
Chemotherapy Dose Modifications (17) Anthracyclines Doxorubicin/Daunorubicin-Greater toxicities (pancytopenia,
painful mucositis) in patients with liver dysfunction (bilirubin >50µM/L). dose modifications recommended in patients with elevated Direct-Bilirubin or AST/ALT >3 x ULN Idarubicin: dose modification in patients with mild-moderate hepatic impairment, the data is insufficient in severe hepatic impairment. Epirubicin: AST is a more sensitive and reliable marker of Epirubicin clearance than bilirubin.
Vinca-alkaloids VCR & Vinblastine metabolized by hepatic microsomes with drugs and metabolites, and then excreted into bile. The biliary system is the main elimination rout. Greater neurotoxicity in patients with liver dysfunction. Dose modifications highly recommended in patients with elevated tot bilirubin.
Epipodophyllotoxins VP-16 partially metabolized into inactive forms in the liver and cleared by both liver and the kidneys. No dose modification needed in patients with mild-to-moderate liver dysfunction (25-80µM/L), severe hepatic impairment can contribute to greater toxicity (myelosuppression, mucositis), patients with low serum albumin more free fraction of VP-16 leads to greater hematological toxicities.
Camptothecins Irinotecan is primarily metabolized into active metabolite SN-38 and eliminated hepatically; the drug and its metabolites are partially excreted renally. Patients with liver dysfunction, high tot bilirubin leads to slower excretion of irinotecan and higher drug exposure, more febrile neutropenia and diarrhea. Dose modifications in elevated tot bilirubin and AST highly recommended. Topotecan, no dose adjustment is recommended in patients with impaired liver function.
Taxanes
Paclitaxel: dose reductions recommended in patients with elevated AST/bilirubin Docetaxel: dose reduction in patients with elevated AST/ALT (>1.5x ULN) /bilirubin (>1x ULN)/ALP (>2.5 x ULN)
Antimetabolites 5-FU primarily metabolized in the liver by the enzyme dihydropyrimidine dehydrogenase (DPD). It is predominately in the liver, patients with DPD deficiency leads to severe toxicities. Patients with mild to moderate renal dysfunction (130-260µM/L), mild to-moderate hepatic dysfunction (tot bilirubin 25-85µM/L), severe hepatic dysfunction (tot bilirubin >85 µM/L) safely treated with weekly CI over 24h without adjustment. Female patients experience more toxicities

16
comparing to male patients. Patients over the age 70 experience more grade3-4 toxicities. Cytarabine (Ara-C): no definite evidence of hepatotoxicity could be found. Leukemia patient were give high-dose of Ara-C given by CI over 72hr developed abnormal liver tests, the effects are reversible. 6-MP used mainly in the maintenance phase therapy of ALL patients. Hepatotoxicity induced by 6-MP may occur with doses exceeds 2mg/kg, may present either Hepatocellular or Cholestatic liver. 6-TG has been implicated in the production of hepatic veno-occlusive disease (HVOD). Methotrexate: is an antifolate and it is used for the maintenance therapy in children with ALL, it led to the development of hepatic cirrhosis and fibrosis. Fatty change, focal hepatitis, or portal fibrosis. The tot MTX clearance for tot and free MTX is inversely proportional to age. Elevations of ALT/LDH are common following high-dose MTX, the abnormalities resolve within 2 weeks. Chronic low dose MTX leads to fibrosis/cirrhosis, while high-dose MTX cause altered liver function tests.
Case # 5 14 years old Saudi male diagnosed stage IV with B syndrome, highly suspicious bone marrow involvement, patient’s lab results prior starting chemotherapy. Renal profile as follow Na= 138, K= 3.8, Cl = 104, SCr= 160 (H), ALT= 185, Tot bilirubin 95 (H), Direct bilirubin 60(H). Patient is due to first cycle ABVD. What recommend to this patient? A) Proceed with ABVD B) Modify ABVD dose C) Hold chemotherapy D) Seek another chemotherapy treatment on this patient

17
Dose Modifications in Hepatic Impairment (17)

18

19

20
Specific Dose Modifications of Chemotherapy Agents with Liver-Dependent Metabolism According to Supportive Care of Children with Cancer, Current Therapy and Guidelines from the Children’s Cancer Group (CCG). (21)
Bilirubin <25 Bilirubin 25-50
Bilirubin >50 Bilirubin >50-85
Bilirubin >85 Drug
ALT<70 ALT 60-180 ALT>180 ALT>85 ALT>180 VCR/VBL 100% 50% HOLD --- ----- VP-16 100% 50% HOLD --- ---- Doxo/Dauno/Ida 100% 50% - 25% HOLD Actinomycin-D 100% 50% - 25% HOLD MTX/CTX 100% 50% - 25% HOLD CCNU/BCNU/5-FU/Ara-C/DTIC Procarbazine
100% 100% 100% 100% HOLD

21
Answers for patients Cases Case #1 B is the answer, the patient is obviously exhibits signs of renal dysfunction secondary to CDDP therapy (BUN= 16.5, Cr= 115). His chemotherapy regimens is a curative regimen for testicular cancer even in advanced stages. Holding the chemotherapy or reducing doses of any drugs would not be an option for this patient. Something should be done to assist the patient with elimination of these chemotherapy agents by giving the patient vigorous hydration with mannitol diuresis is an effective means of doing this. A recent study showed increased toxicity in patients receiving mannitol. Case#2 A is the answer, patient having elevated serum Cr, Ifos should be adjusted accoding to patient’s calculated CrCl, also the patiet having high total bilirubin, should order fractionation of tot bilirubin, if direct bilirubin high then doxorubicin dose be adjusted. Case #3 A is the answer, the recommended dose of mesna 60% of the ifos dose divided into 3 doses at 0 prior Ifos infusion and at 4 and 8 hours post ifos infusion., the CIV of mesna only for patients with persistent +3 RBC and above in the urine. Oral Mesna is twice of the iv mesna, if this patient tolerate oral mesna the correct dose of oral mesna at 4 and 8 hours will be 1360mg. Case #4 C is the answer, Patient TT has the potential to go to ICU because the patient is very high risk developing cerebellar toxicities leads to impaired balance, TT having elevated serum Cr and Ara-C metabolized into Ara-U and eliminated renally. Ara-U accumulates in the CNS of patients with poor renal function resulting in higher CNS levels of the Ara-CTP that is believed to be the neurotoxic agent. (20)

22
Case # 5 D is the correct answer ABVD regimen has the potential to be highly toxic for this patient (17) Chemotherapy Toxicities with hepatic impairment Doxorubicin Giving doxorubcin to patients with elevated tot bili/high direct bili
greater toxicities (pancytopenia, paiful mucositis, possible death) Bleomycin This patients having compromized renal function, dose limiting
toxicities for bleomycin is interstitial pneumonitis with a 1-2% fetal lung damage, this patient will have higher risk for pulmonary toxities, dose modification highly recommended.
Vinblastine Biliary system is the main elimination route for Vinblastine, this patient will have greater toxicities (e.g. pancytopenia and Neurotoxicity)
DTIC No dose modifications in hepatic impairment, dose modification with renal impairmet.
Alternative regimen for this patient will be COPP (CTX, VCR, Procarbazine, and Prednisone) Chemotherapy Toxicities with hepatic impairment CTX No dose adjustment needed, dose adjusted in patient with renal
impairment only with large doses. VCR Biliary system is the main elimination route for VCR, this patient will
have greater toxicities (e.g. SIADH and Neurotoxicity), and Clinical judgment is needed to give minimal dose 25% of the VCR dose.
Procarbazine Dose adjustment needed only in patient with severe renal or hepatic impairment.
Prednisone Would switch to prednisolone if there is a concern for the inadequate conversion of prednisone to prednisolone occurs.
Third alternative will be APPE (Ara-C, Cisplatin, Prednisone, and Etoposide) , this the third line of chemotherapy in patients with Hodgkin’s lymphoma. This combination is very myelosuppressive and it is highly recommended to discharge patient GCSF therapy.

23
Reference:
1- Humphreys BD, Soiffer RJ, Magee CC. Renal failure associated with cancer and its treatment: An update. J Am Soc Nephrol 2005;16(1):151-61.
2- Chike Nzerue. How to Prevent, Recognize and Treat Drug-Induced Nephrotoxicity. Cleveland Clinic Journal of Medicine 2002;69(4): 289-312.
3- King PD, Perry MC. Nephrotoxicity of chemotherapeutic agents.In: Perry MC, ed. The Chemotherapy Source Book. 3rd edition. Philadelphia: Lippinocott Williams & Wlkins; 2001:494-504...
4- Repetto Lazzaro. Greater Risks of Chemotherpay Toxicity in Elderly Patients with Cancer. J Support Oncol 2003; 1 (suppl 2):18-24.
5- Lichtman SM, Hollis D, et al. Prospective evaluation of the relationship of patient age and paclitaxel clinuical pharmacology; Cancer and leukemia Group B (CALGB 9762). J Clin Oncol 2006;24:1846-1851.
6- Smorenburg CH, Ten Tije AJ, et al. Altered clearance of unbound paclitaxel in elderly patients with metastatic breast cancer. Euro J Cancer, 2003;39:196-206.
7- Bruno R, Viveir N, et al. Population pharmacokinetics and pharmacikinetics-pharmacodynamics relationships for docetaxel. Invest New Drugs, 2001;19:163-169.
8- Sorio R, Robieux I, et al. Pharmacokineucs and tolerance of vinorelbine in elderly patients with metastatic breast cancer. Eur J Cancer, 1997; 33:301-33.
9- Milano G, Etience MC, et al. Influence of sex and age on fluorouracil clearance. J Clin Oncol, 1992;10:1171-05.
10- Bressolle F, Bolonga C, et al. Effects of moderate renal insuffiency on pharmacokinetics of methotrexate in rheumatoid arthritis patients. Ann Rheum Dis, 1998;57:110-113.
11- Toffoli G, Corona G, et al. Population pharmaokinetics and pharmadynamics of oral etoposide. Br J Clin Pharmacol, 2001; 52:511-519.
12- Li J, Gwitt PR, et al. The effects of age on the early disposition of doxorubicin. Cancer Chemother Pharmacol, 2003;51:395-402.
13- Jen JF, Gutler DL, et al. Population pharmacokinetics of temozolamide in cancer patients. Pharm Res. 2000;17:1284-1289.
14- Lameire NH, Flombaum CD, et al. Acute renal failure in cancer patients. Ann Med 2005;37(1):13-25.
15- Renal function and chemotherapy (section-3). Clinical oncology.2001;13 (suppl211):S222-S225.
16- Launay-Vacher V, Chatelut E, et al. Renal insufficiency in elderly cancer patients: International Society of Geriatric Oncolgy Clinical Practice recommendations. Annals of Oncology. 2007; 18:1314-1321.
17- Superfin D, Iannucci A, et al. Commentary: Oncologic Drugs in Patients with Organ dysfunction:A Summary. The oncoligst 2007;12:1070-1083.
18- Kintzel PE, Dorr RT, et al. Anticancer drug renal toxicities and elemination: dosing guidelines for altered renal function. Cancer Treat Rev 1995;21:33-64.
19- Enerman JD, Philips GK, et al. Cancer management in patients with end stage renal failure disease. Oncology (Huntington) 2005;19(9):1119-212.
20- Smith GA, Damon LE, Rugo HS, et al.high dose cytarabine dose modification reduces the incidence of neurotoxicity in patients wth renal insuffiency. J Clin Oncol 1997;15:834.

24
21- Arthur R Ablin, Supportive Care of Children with Cancer- Current therapy and Guidelines from the Children’s Cancer Group, second edition, the Johns Hopkins University Press, 1997:86-89.
22- King PD, Perry MC. Hepatoxicity of chemotherapeutic agents. In: Perry MC, ed. The Chemotherapy Source Book. 3rd edition. Philadelphia: Lippinocott Williams & Wilkins; 2001:483-493.
23- LLoyod Yee Young, Mary Anne Koda-Kimble, Adverse effects of chemotherapy. In: Applied Therapeutics: The Clinical Use of Drugs, 6th Edition. Applied Therapeutics, Inc. Vancouver, WA, 1995; (91):91-33.

















