CHEST MEASURMENTS a. Carina at T4-5; normal carina angle 60-100deg b. Interlobar artery <16mm c. MPA <3cm d. Left hila 1-2cm higher than highest point of right hila e. R paratracheal stripe ≤5mm f. Vascular pedicle= 38-58mm (should be <7cm otherwise widened mediastinum) on PA view (measure near level azygous vein; from where SVC meets RMSB and to where a perpendicular line is drawn from left subclavian exiting Ao arch) g. Azygous trans dia <1cm upright and <1.5cm supine h. Kids humeral head ossific center at >37wks (term); femoral head ossific center at 4mos i. Kids normal 6ribs ant and 8ribs post (hypeinflation 8ribs ant/10ribs post; hypoinflation 4ribs post) j. Normal thymus (homogenous, bilobed/triangular with concave lateral margins on CT; size increases from birth to age 8yo then decreases; 18mm thickness <20yo and 13mm in older pts; rebound thymic hyperplasia if volume increases by 50%)—sail sign (right) or wave sign (smooth indentations) k. Thoracic aorta (ectasia 3.7-4.0cm, mild enlargement 4.0-4.5cm, ≥4.5cm aneurysm, ≥6cm surgery) i. LVOT ii. Aortic annulus (at valve) iii. Aortic root (SOV) 1. “Cusp to cusp” measurement (cardiologists) upto 4cm 2. Mean “cusp to commisure” (preferred) iv. Sinotubular jct (STJ) v. Asc aorta (@MPA) upto 3.7cm vi. Aortic arch vii. Aortic isthmus (btwn take off of left subclavian artery and ductus arteriosus) viii. Prox desc aorta (@MPA) ix. Distal desc aorta (@dia hiatus) upto 2.8cm l. Normal pericardial thickness=2mm (>4mm is concerning for pericarditis) m. Pericardial fluid: normal 15cc (post CPA blunting with >75cc, lat CPA blunting with >250cc, complete opacification atleast 500cc); >1cm decub free-flowing eff can be tapped without imaging guidance n. Left Atrium AP <4cm o. Left Ventricle chamber transverse in ED <5cm p. LV wall thickness <12mm q. Haller index of pectus excavatum (transverse dia divided by AP diameter) normal ≤2.5 (>3.2 is one criteria for surgical correction) r. PTX >25% requires chest tube evacuation (calculator= ww.chestx-ray.com/calculator) s. Normal dia excursion of 1-2ribs on fluoro sniff test (unless there is mod to large effusion) LINES/ TUBES “correlate for preferred/desired location/placement” t. ETT= 2-6cm above carina and atleast 3cm below vocal cords (carina is usually at about T6; vocal cords at C6)—should be below inf aspects of clavicles (thoracic inlet); cuff <3cm in dia (without bowing of tracheal walls); tube dia should be 2/3 of tracheal dia u. Trach tube= should be halfway btwn neck entrance site and carina v. SGC (for pulm capillary WP)=tip should be distal to pulmonic valve; on the right, measure from where catheter crosses itself and should be within 2cm (should next extend beyond proximal interlobar pulm artery); on the left, measure from most sup turn of catheter at hila and should be within 2cm w. Pacer/AICD (all are pacers; AICD has sensing and shocking electrodes for cardioversion/defibrillation)
Transcript
CHEST MEASURMENTS
a. Carina at T4-5; normal carina angle 60-100deg b. Interlobar artery <16mm c. MPA <3cm d. Left hila 1-2cm higher than highest point of right hila e. R paratracheal stripe ≤5mm f. Vascular pedicle= 38-58mm (should be <7cm otherwise widened mediastinum) on PA view (measure
near level azygous vein; from where SVC meets RMSB and to where a perpendicular line is drawn from left subclavian exiting Ao arch)
g. Azygous trans dia <1cm upright and <1.5cm supine h. Kids humeral head ossific center at >37wks (term); femoral head ossific center at 4mos i. Kids normal 6ribs ant and 8ribs post (hypeinflation 8ribs ant/10ribs post; hypoinflation 4ribs post) j. Normal thymus (homogenous, bilobed/triangular with concave lateral margins on CT; size increases
from birth to age 8yo then decreases; 18mm thickness <20yo and 13mm in older pts; rebound thymic hyperplasia if volume increases by 50%)—sail sign (right) or wave sign (smooth indentations)
k. Thoracic aorta (ectasia 3.7-4.0cm, mild enlargement 4.0-4.5cm, ≥4.5cm aneurysm, ≥6cm surgery) i. LVOT
ii. Aortic annulus (at valve) iii. Aortic root (SOV)
1. “Cusp to cusp” measurement (cardiologists) upto 4cm 2. Mean “cusp to commisure” (preferred)
iv. Sinotubular jct (STJ) v. Asc aorta (@MPA) upto 3.7cm
vi. Aortic arch vii. Aortic isthmus (btwn take off of left subclavian artery and ductus arteriosus)
viii. Prox desc aorta (@MPA) ix. Distal desc aorta (@dia hiatus) upto 2.8cm
l. Normal pericardial thickness=2mm (>4mm is concerning for pericarditis) m. Pericardial fluid: normal 15cc (post CPA blunting with >75cc, lat CPA blunting with >250cc, complete
opacification atleast 500cc); >1cm decub free-flowing eff can be tapped without imaging guidance n. Left Atrium AP <4cm o. Left Ventricle chamber transverse in ED <5cm p. LV wall thickness <12mm q. Haller index of pectus excavatum (transverse dia divided by AP diameter) normal ≤2.5 (>3.2 is one
criteria for surgical correction) r. PTX >25% requires chest tube evacuation (calculator= ww.chestx-ray.com/calculator) s. Normal dia excursion of 1-2ribs on fluoro sniff test (unless there is mod to large effusion)
LINES/ TUBES “correlate for preferred/desired location/placement”
t. ETT= 2-6cm above carina and atleast 3cm below vocal cords (carina is usually at about T6; vocal cords at C6)—should be below inf aspects of clavicles (thoracic inlet); cuff <3cm in dia (without bowing of tracheal walls); tube dia should be 2/3 of tracheal dia
u. Trach tube= should be halfway btwn neck entrance site and carina v. SGC (for pulm capillary WP)=tip should be distal to pulmonic valve; on the right, measure from where
catheter crosses itself and should be within 2cm (should next extend beyond proximal interlobar pulm artery); on the left, measure from most sup turn of catheter at hila and should be within 2cm
w. Pacer/AICD (all are pacers; AICD has sensing and shocking electrodes for cardioversion/defibrillation)
i. Single lead= RV; Dual lead= RA and RV; Triple lead (biventricular for CRT)=RA, RV, and coronary sinus
ii. Battery can with lead pins; leads iii. Look for broken lead (lead damage); dislodged lead tip (pulled back); Twiddler’s syndrome
x. IABP (intra-aortic counterpulsion balloon pump for cardiogenic shock)=inflates during diastole; radiopaque tip 1cm distal to left subclavian; projecting 1-2cm below top of arch
y. Chest tube (pleural drain, thoracostomy tube, pigtail cath)=tip and side ports within thoracic cavity; anterosuperior placement for PTX; posteroinferior placement for effusion; exclude tube within fissure or intra-pulmonary placement
z. NGT/OGT (enteric tube)=tip within stomach, distal to GEJ (side port is located 6cm from the tip); note if coiled or post-pyloric
aa. DHT (feeding tube)=weighted tip should be within 2nd or 3rd portion of duo (prefer near distal 4th portion of duo neat LOT)
bb. CVC (tunneled dialysis cath, PICC, port-a-cath (chest ort) with Huber needle access)=IJ/subclavian/femoral; tip near superior cavo-atrial junction or caudal aspect of SVC; should be medial to 1st rib on frontal and caudal and posterior to clavicle (otherwise suspect intra-arterial)
cc. UVC= umbilicusUVleft PVductus venosusIVC; tip at or slightly above dia at inf cavo-atrial jct; curves medially (convex laterally) thru liver on frontal; on lateral view, directed ant-sup then horiz-post and then heads sup towards heart
dd. UAC= umbilicusUAinternal iliaccommon iliacaorta (ascends parallel to spine); normal high=T6-T9 (above dia); normal low=below L2 (more complications if at L1-2 level of renal arteries); dips inferiorly then ascends superiorly parallel to spine
i. VV (veno-venous) vs VA (veno-arterial) ii. VV=Draining large venous cannula via RIJ (make sure tip and side port within RA); smaller
returning venous catheter via femoral vein (tip within IVC at or above inferior cavo-atrial jct) iii. VA=also has an arterial returning cannula usually within R CCA (tip projects over arch at origin
of innominate artery) iv. Normal to have diffusely opacified lungs
ii. VAD (ventricular assist device)—bridge to cardiac transplant i. Percutaneous vs surgically implanted
ii. LVAD, RVAD, BIVAD iii. Conduits (inflow vs outflow), pump, driveline iv. Look for kinking of cannula/conduit v. Percutaneous VAD (Impella): tip within LV; outflow portion within LVOT
SOLID NODULES
a. Size: 1-3mm=miliary; 3-5mm=micronodule; >5mm=macronodule; >3cm=mass b. B9 calc= central, diffuse, laminated (concentric), popcorn c. Malig calc= eccentric, stippled, amorphous d. Margins= smooth, lobulated (bad), spiculated (bad) e. Attenuation= fat (<-40HU) suggests hamartoma f. Location= subpleural, juxtapleural, perifissural, pleural-based, along mediastinal pleural surface,
peribronchovascular, endobronchial g. Others=satellite nodule suggest infx; pleural tag (bad); central lucency (aka ABG) ddx is BAC,
lymphoma, OP h. Enhancement <15HU is likely benign (>20-25HU is probably malignant ~98% sensitive for CA) i. Volume Doubling Time= increase in dia by 25% correlates with doubling of volume (malig VDT usually
btwn 30-500d or 1.5yrs with median of 100d or 3mos)see calculator on chestxary.com
j. DDX solid non-calcified nodule=non-calcified granuloma, intrapulm LN, CA k. DDX airspace/macrondules nodules= acute varicella (classic), mets, fungal, aspergillosis, kaposi l. DDX calcified micronodules= fungal (histo)/TB, alveolar microlithiasis, malig calcifications, healed
varicella, silicosis, mets m. DDX cavitating mets= primary SCC, secondary SCC (H&N males and cervical females), sarcoma n. DDX calcifying mets= osteo/chondrosarcoma, mucinous colon, leimyosarcoma o. DDX cannon-ball mets (>3cm)= MCSaR melanoma, colon, sarcoma, RCC p. DDX nodules with GG halo (hemorrhagic)= hemorrhagic mets (chorioCA), invasive aspergillosis,
neuroblastoma r. DDX nodules in HIV= TB/fungal, CMV (GG), Kaposi (flame-shaped), aspergillosis (GG halo), PCP (cystic
UL), lymphoma s. PET/CT: size ≥8mm; low (<5%) to mod (5-60%) prob or CA; not for very low prob or high prob;
discordance btwn pretest prob and imaging test; for staging t. PET/CT sensitivity for BAC is 10-30% and false neg rate for carcinoid is 25% u. PET/CT overall sens 97% and spec 80% for characterizing SPN >1cm in dia v. NLST NEJM 2011 LDCT for lung CA screening “reduced lung CA mortality by 20% with LDCT vs CXR
screening w. High risk pts per Fleischner society=smoker, 1st deg relative with lung CA, exposure to
asbestos/radon/uranium x. Fleischner society criteria does not apply to: age<35yo, known/suspected extra-thoracic CA, infectious
symptoms (unexplained fever), non-solid nodules y. Screening chest CT criteria (ACR): 55-80yo with 30pack-yr smoking hx who is current smoker or quit
15yr ago
NON-SOLID NODULES
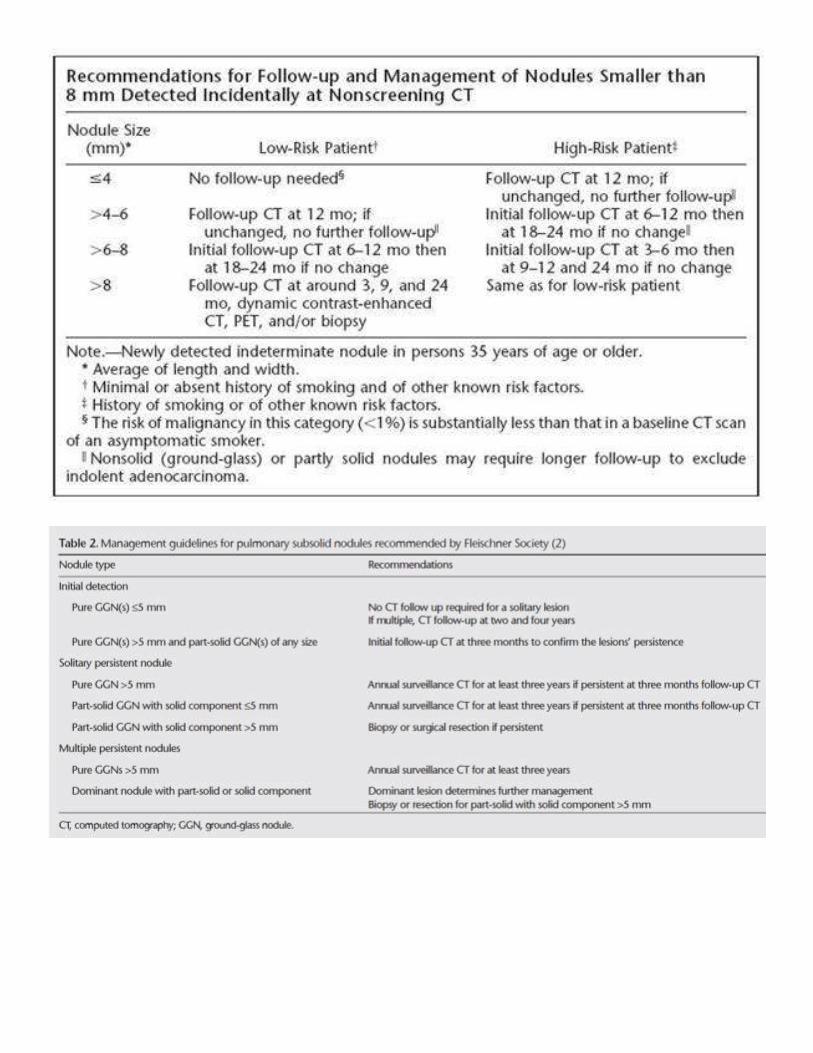
z. GGN (pure GG nodule) i. Ddx= atypical adenomatous hyperplasia (precursor to adenoCA) vs AdenoCA (BAC) vs
infx/inflammatory vs focal fibrosis ii. <5mm don’t need f/u esp if enrolled in lung nodule program; but if multiple (then do FU in
1yr) iii. ≥5mm FU in 3-6 mos if stable FU for total of 3-5yr vs if enlarge or develop solid component
recc resection aa. PSN (part-solid nodule)
i. FU in 3-6mos if persist consider PET/CT (some say resect) vs if enlarge recc resection
SCREENING CHEST CT
bb. NLST (national lung screening trial) cc. Published 2011 in NEJM (“Reduced lung cancer mortality with low-dose CT screening”) dd. Pts who received low dose CT had 20% lower risk of dying from lung CA than those who received CXR ee. Screening chest CT criteria (ACR): 55-80yo with 30pack-yr smoking hx who is current smoker or quit
15yr ago ff. What is considered low dose CT
i. Prefer ≥16 detector CT with gantry rotation time ≤0.5s ii. Slice thickness ≤2.5mm (with recon interval ≤ slice thickness) and use ≤1mm for MPRs
iii. End-inspiration iv. Non-contrast v. CTDI vol ≤3mGy for “standard” size pt (DLP ≤75mGy-cm or Est dose ≤1mSv)
gg. Reporting i. Use Lung-RADs version1
ii. Size (measure on lung windows; give avg dia & round it to nearest whole number) iii. Location (lobe/seg)—give image# iv. Attenuation (soft tissue, calcified, mixed) v. Opacity (solid, part-solid, GG)
vi. Margin (smooth, lobulated, spiculated) vii. Comparison (compare to oldest scan)—increase in size by >1.5mm is significant
AIRWAYS (see HRCT for small airways dz and bronchiolitis)
1. Airways thickening on CXR (cheerios and dirty lung): non-specific findings seen with reactive-airways disease (asthma) vs sequel of smoking vs bronchitis(clinical diagnosis)
2. Airways lesions a. B9 solitary=mucus plug, FB, papilloma (multiple in kids; malig transformation to SCC in 10% of adults) b. Multiple airways lesions=papillomatosis, mets, TBO/RP/amyloidosis, TB c. Malignant Trachea=”SAM” SCC, adenoid cystic, mets (breast, melanoma) d. Malignant Bronchus=”BCMM” bronchogenic tumor (SCC, small cell), carcinoid (enhances,
1/3calcified, tip-of-iceberg), mucoepidermoid, mets (breast, melanoma) 3. Unilateral collapsed lung= central obstructive lesion (bronchogenic CA, endobronchial tumor, FB),
scarring, endobronchial TB (multiple stenosis), amyloidosis (does not spare post membr), wegner’s, CA 5. Finger-in-glove=CF, ABPA (asthma), bronchial atresia, central malignancy with distal plugging 6. Unilateral hyperlucent lung
a. Don’t miss: PTX, PE (ologemia), FB (RLL>LLL) b. CLE (LUL>RML>RUL), bronchial atresia c. Bronchiolitis Obilierans (Swyer james in kids <8yo) d. Poland’s, unilat mastectomy, large bulla (emphysema)
MEDIASTINAL LESION
a. Ant med mass i. Thymus
1. Thymic hyperplasia (rebound s/p chemo/xrt >50% increase in vol above baseline; Myasthenia gravis=85% hyperplasia and 15% thymoma)
2. Thymic cyst (unilocular/multilocular; may have peripheral calc) 3. Thymolipoma (b9, soft tumor that drapes down and may change shape w/ decub) 4. Thymoma (middle age pts; b9=encapsulating with homogenous enhancing capsule,
may have lobulated contours and can be cystic VS invasive=malignant with irreg margins, invasion/encasement of mediastinal fat and may have drop mets into pleura or pericardial involvement; assoc with MG=40% w/ thymoma have MG and 10-15% with MG have thymoma; can be cystic w/ mural nodule; 5% may have calcs)
5. Thymic CA (no capsule; can be metastatic--assoc w/ mediastinal lymphadenopathy which is uncommon with thymoma; poor prognosis)
ii. Teratoma and other germ cell tumors (<20yo; mature/immature/malig) iii. Terrible lymphoma (homogenous mass which encases vessels; HD vs NHL) iv. Thyroid substernal goiter v. Mets (neuroblastoma)
vi. Fibrosing mediastinitis (TB, histo) vii. Mediastinal lipomatosis (steroids, obese, cushing’s=endogenous steroids)
b. Cystic med mass i. Duplication (enteric/neuroenteric) vs bronchogenic cyst (subcarinal)
ii. Pericardial cyst (R>L)
iii. Thymic cyst (unilocular/multilocular; may have peripheral calc) iv. Cystic thymoma (can have mural nodule) v. Teratoma (<20yo; look for fat, fat-fluid level, calcification)
c. Fatty med mass i. Epicardial fat pad
ii. Mediastinal lipomatosis iii. Thymolipoma iv. Teratoma v. Hernia (morgagni usually on the right; omental fat)
d. Calcified med mass i. Fibrosing mediastinitis (TB, histo; SVC syndrome, pulm HTN)
ii. Treated lymphoma iii. Teratoma (<20yo; contains fat) iv. Thyroid substernal goiter v. Calcified nodes= TB , sarcoid/silicosis (egg-shell calcs)
e. Cardiophrenic angle mass i. Epicardial fat pad
ii. Pericardial cyst iii. Duplication cyst iv. Thymolipoma v. Epiphrenic LN
vi. Hernia f. Paraspinal mass
i. Neuroenteric cyst (w/ vertebral anomaly) ii. Neurogenic tumor (schwannoma, NF, paraganglioma, neuroblastoma)
iii. Extramedullary hematopoiesis iv. Duplication or bronchogenic cyst v. Descending aortic aneurysm
VASCULAR ANOMALIES
g. Bovine arch (common origin of innominate and left CC arteries) h. Double arch (vascular sling; R arch is larger/higher/posterior than L with midline trachea and
descending left aorta; right dominant 75%, left dominant 20% and co-dominant 5%; encircles trachea and eso in a tight complete ring; reverse S indentation on esophagram)
i. Right arch i. Kommerell diverticulum (at origin of L subclavian) and Dysphagia Lusoria
ii. Higher assoc with truncus but TOF overall more common iii. 2 types: mirror image(worse b/c assoc cardiac anomalies like truncus or TOF) vs R arch with
aberrant LS iv. Can be complete ring if intact lig arteriosus or open PDA
j. Aberrant subclavian (travels post to eso) i. L arch with aberrant R subclavian (dysphagia lusoria; diverticulum Kommerell)
ii. R arch with aberrant L subclavian k. Pulmonary sling (LPA arising from RPA; travels btwn trachea and eso; retrotracheal density more
caudal than aberrant subclavian; complete napkin-ring tracheal rings which can lead to tracheobronchial stenosis)
l. Cervical arch m. Anomalous vessel lateral to aortic arch
i. PAPVR ii. Persistent left SVC (left common cardinal vein starts near jct of SC and IJ, descends lateral to
aortic arch and anterior to left hilum, courses post wall of LA, and dumps into coronary sinus) n. Vascular impression on eso and trachea
i. Anterior trachea=innominate artery ii. Posterior impression on eso= L arch with aberrant RS vs R arch with aberrant LS vs Double
arch iii. Btwn trachea and eso=pulmonary sling iv. Encircling trachea and eso=Double arch vs R arch with aberrant LS + open PDA
o. Enlarged azygous vein (note: azygous of rightin SVC; hemiazygous of leftinfo brachiocephalic vein)
i. Azygous continuation of IVC ii. CHF
iii. TR iv. Constrictive pericarditis v. SVC obstruction distal to azygous entry
vi. Portal HTN p. Heterotaxy syndrome
i. Asplenia (right isomerism; worse) 1. M>F 2. Bilat right-sided 3. trilobed lungs 4. eparterial bronchi 5. bilateral right atrial appendage 6. Midline liver and stomach 7. Cardiac apex discordant to abdominal viscera 8. Associated with
a. Severe CHD , GI malformations b. Persistent left SVC c. “piggyback” IVC anterior to aorta (aka ipsilateral aorta and IVC)
ii. Polysplenia (left isomerism) 1. F>M 2. Bilat left-sided 3. bilobed lungs 4. hyparterial bronchi 5. bilateral left atrial appendage 6. Midline liver and stomach 7. Less severe malformations like interrupted IVC w/ azygous continuation and PAPVR
q. Azygous continuation of IVC (Azygous located on the right ends into SVC; Hemiazygous located on the left ends into left brachiocephalic vein; associated with polysplenia)
r. PAPVR i. More common on right (RULPV draining into SVC or azygous; Scimitar vein draining RLL into
IVC or PV or HV with right lung hypoplasia) ii. On left usually draining LUL (LULPV draining into vertical vein which is anterior to aorta and
travels cephalad into L brachiocephalic vein) s. Coronary anomalies
i. High/Low/Commissural takeoff from sinus of Valsalva ii. Multiple ostia (absent LM with separate vs split LAD and LCx origin; conus artery directly off R
sinus) iii. Single coronary artery (associated with CHD) iv. Anomalous origin
1. RCA arising from L anterior sinus with anomalous course (retrocardiac; retro-aortic; btwn aorta and PA; intraseptal; anterior to pulmonary outflow aka precardiac; posteroanterior IV groove)
2. LAD arising from R anterior sinus with anomalous course (btwn aorta and PA aka inter-arterial or malignant course with slit-like narrowing at origin and acute origin
angle; intraseptal; anterior to pulm outflow aka precardiac; posteroanterior IV groove)
3. LCx arising from R anterior sinus with anomalous course (retro-aortic; posterior AV groove)
4. LM arising from R anterior sinus with anomalous course (same as RCA--see above) 5. ALCAPA (anomalous left coronary artery from pulm artery) or Bland-Garland-White
syndrome v. Anomalous course (myocardial bridge or intramyocardial course)
vi. Anomalies of termination (coronary artery fistula most commonly involves RCA or right sided venous structures; most commonly drains in RV>RA>PA)
vii. Others 1. Split LAD (LAD + 1st large septal branch) 2. Double LAD (parallel LADs) 3. Split RCA (proximal + distal PDA both arise from RCA) 4. Ectopic origin of first septal branch (from right sinus; from RCA; from Diagonal; from
Ramus; from LCx) viii. Coronary aneurysm (1.5x normal dia) vs athero with positive remodeling
t. Pulmonary veins i. Three right PV with middle PV drains RML (has strong assoc with AFib)—RML normally drains
into RSPV ii. Single left PV
iii. Absent right PV iv. Common ostia of sup and inf PV trunks v. Separate ostia for apicoposterior vein of LUL
vi. Early branching of pulm vein within 5mm of its ostia u. Pulm vein varix (congenital vs acquired) v. IVC abnormalities
i. Double IVC (left IVC drains into left renal vein)
ii. Double IVC with retro-aortic L or R renal vein and azygous or hemiazygous continuation of IVC
iii. Left IVC (absent normal right IVC)
iv. Azygous continuation of IVC (absent hepatic segment of IVC; IVC interrupted above level of
renal vein and continues as azgous R and hemiazygous L)
v. Absent infrarenal IVC (preservation of supra-renal segment)
vi. Others:
1. Circumcaval ureter
2. Retro-aortic left renal vein
3. Circumaortic left renal vein
AORTA
w. Aneurysm i. Thoracic aorta (ectasia 3.7-4.0cm, mild enlargement 4.0-4.5cm, ≥4.5cm aneurysm, ≥6cm
7. Aortic isthmus (btwn take off of left subclavian artery and ductus arteriosus) 8. Prox desc aorta (@MPA) 9. Distal desc aorta (@dia hiatus) upto 2.8cm
ii. Ectasia vs true aneurysm (fusiform vs saccular)
iii. Sinus of valsalva aneurysm >4cm iv. Annuloaortic ectasia (tulip bulp; Marfans or ED) v. Post-stenotic dilation secondary to aortic stenosis
vi. Syphilis aortitis (calcifications) vii. Mycotic aneurysm (saccular with surrounding inflammation)
viii. Ductus bump or diverticula (anteromedial; gentle obtuse bulge as opposed to sharp acute margins of pesudoaneurysm)
ix. Traumatic pseudoaneurysm (acute margins with aorta; saccular without atheroma; at aortic isthmus; s/ trauma)
x. Infundibulum of aortic arch/branch vessels x. Intra-mural hematoma (within aortic wall; hyperdense crescent on non-contrast CT; better prognosis
if <2cm; treat it like focal dissection) y. Mural thrombus (within aneurysm) vs eccentric/ concentric intraluminal thrombus z. Penetrating aortic ulcer (PAU; thru existing atheroma and projecting beyond aortic wall) aa. Ulcerative plaque (does not project beyond aortic wall) bb. Dissection
i. Stanford A=asc aorta (60%); Stanford B=begins beyond brachiocephalic vessels (40%) ii. CXR: widened mediastinum, double or irreg aortic contour, inward displacement of athero
calcs iii. Intimal flap
1. True lumen (smaller b/c compressed by false lumen; surrounded by intimal calcification; brighter lumen)
2. False lumen (larger b/c higher pressure; beak sign=wedges around true lumen; cobweb sign=linear media remnants; lower contrast density if patent due to delayed opacification; may be completely/partially thrombosed or contain thrombus)
iv. Complications 1. Aortic rupture 2. Coronary artery occlusion (acute MI usually involves RCA) 3. Aortic valve incompetence (acute aortic insufficiency) 4. Rupture into pericardial sac with cardiac tamponade 5. Extension into arch/branch vessels with or without occlusion
a. End-organ perfusion compromise b. Ischemic stroke c. Limb ischemia d. Paraplegia (artery of adamkiewicz to anterior spinal artery)
v. Chronic dissection flap (thicker, straighter and may be calcified) vi. Intramural hematoma is a variant
vii. Acute aortic injury 1. CXR: widened mediastinum, indistinct/irreg aortic contour, deviation of trachea to
right, depression of LMSB, left apical pleural cap, thickened paraspinal stripe 2. Location: isthmus (most common; located btwn left subclavian artery and lig
arteriosus)>asc aorta=desc aorta at dia hiatus 3. Findings: irreg aortic contour with mural hematoma; laceration/transection with
active extravasation of contrast; pseudoaneurysm; peri-aortic/mediastinal hematoma (+/- pericardial/pleural hematoma); focal intimal flap/clot; look for concomitant left subclavian artery injury
4. Ddx=ductus bump or diverticula
CARDIAC
viii. LAE= oblique measurement from LA border (double density) to mid point of LMSB >7cm on PA view; slayed carina >90-100deg; walking man sign of posteriorly displaced LMSB on lateral view
ix. LVE=Hoffman rigler sign (LV extends more than 1.8cm beyond posterior border of IVC at 2cm cephalad from intersection of LV and IVC on “true” lateral)
x. RAE=not well discernable on CXR xi. RVE=upper tipped “boot-shaped” apex; filling of retrosternal clear space; enlarged MPA
xii. Acute MR=RUL edema xiii. Sig PS=left PA enlargement xiv. Sig AS=ascending aorta enlargement (look for valvular calcifications) xv. LV aneurysm
1. True=post-MI; wide neck; may contain thrombus; usually inferolateral wall 2. False=post-trauma (aka pseudoaneurysm); narrow neck; may rupture; usually
posterolateral wall; less common xvi. Cardiac mass
1. Thrombus (bland vs tumor) 2. Metastasis (esp ACC, HCC, RCC, Hepatoblastoma and Wilm’s)—10-20x more common
than primary cardiac tumor 3. Primary cardiac tumor
hh. Incidence: AdenoCA>SCC>BAC>Small cell (AFIP) ii. Prognosis: SCC>Large cell>BAC>AdenoCA>Small cell
jj. Small Cell
i. Smokers ii. Unresectable
iii. Paraneoplastic syndromes (hypercalcemia, cushing, SIADH) with oat cell subtypes iv. Centrally located (extensive LAD may result in SVC syndrome)
v. Staging: “limited dz” (confined to tolerable radiation port incld supraclavicular node, regional mediastinal, or effusion) vs “extensive dz”
kk. Non-small cell i. AdenoCA
1. Non-smoker women 2. Peripherally located 3. Subtype=BAC, scar carcinoma
ii. SCC (epidermoid) 1. Smokers 2. Centrally located (around airways but not within it unlike small cell) 3. May cavitate 4. Dysplasiain-situSCC 5. Good prognosis (b/c slow growing) 6. Subtype=pancoast (superios sulcus tumor) w/ SVC syndrome, horner’s, brachial
plexopathy, dysphagia iii. Large cell
1. Rapid growth 2. Peripherally located
ll. Staging
i. Size (2cm, 2.1-3cm, 3.1-5cm, 5.1-7cm) 1. Size>7cm (T3)
ii. Location iii. Multicentric tumor (synchronous) of same histology
1. Satellite nodule in same lobe (T3) 2. Nodule(s) in different ipsilateral lobe (T4) 3. Contralateral lung nodule(s) i.e. intrathoracic met (M1a)
iv. Aggressive features 1. Direct visceral pleural invasion (T2) 2. Direct parietal pleural invasion aka chest wall (including superior sulcus tumors),
recurrent laryngeal nerve (T4) v. Endobronchial lesion
1. Endobronchial lesion not proximal to lobar bronchus (T1) 2. Endobronchial lesion ≥2cm from carina or complete atelectasis/post-obstr
pneumonitis extending to hilum but not involving entire lung (T2) 3. Endobronchial lesion <2cm from carina or partial atelectasis/post-obstr pneumonitis
involving entire lung (T3) 4. Endobronchial lesion with involvement of carina (T4)
vi. Nodal involvement 1. N1=ipsilateral hilar or peribronchial 2. N2=ipsilateral mediastinal and subcarinal 3. N3=contralateral hilar/mediastinal; supraclavicular; scalene
vii. Malignant effusion i.e. pleural dissemination or pleural nodules (not direct pleural invasion) and/or Malignant pericardial effusion (M1a)
viii. Distant (extrathoracic) met (M1b)
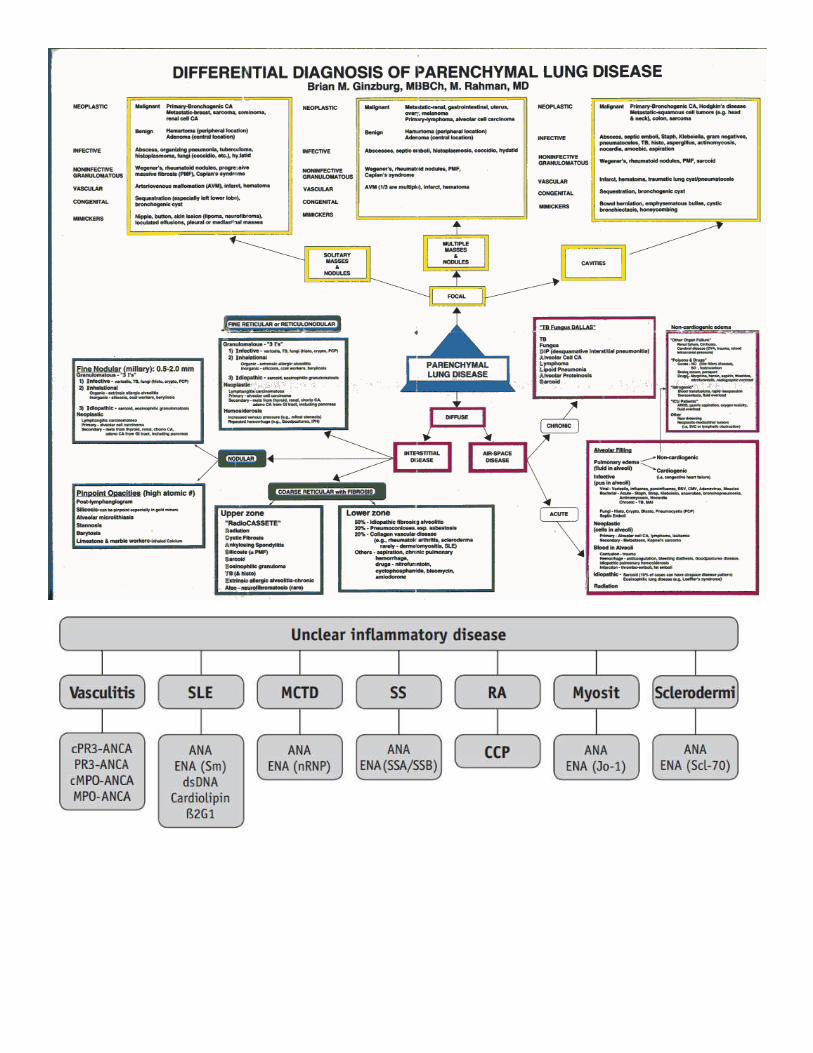
PATTERN BASED EVALUATION OF ILD
a. History and Labs
i. Age (20-40yo=sarcoid, EG, CVD; consider IPF in >50yo) ii. Sex (LAM exclusively in women)
iii. Smoking hx (smokers=EG, RB/RBILD/DIP; non-smokers=HP, sarcoidosis) iv. Time course (acute onset=AIP) v. Family hx (LAM, sarcoidosis)
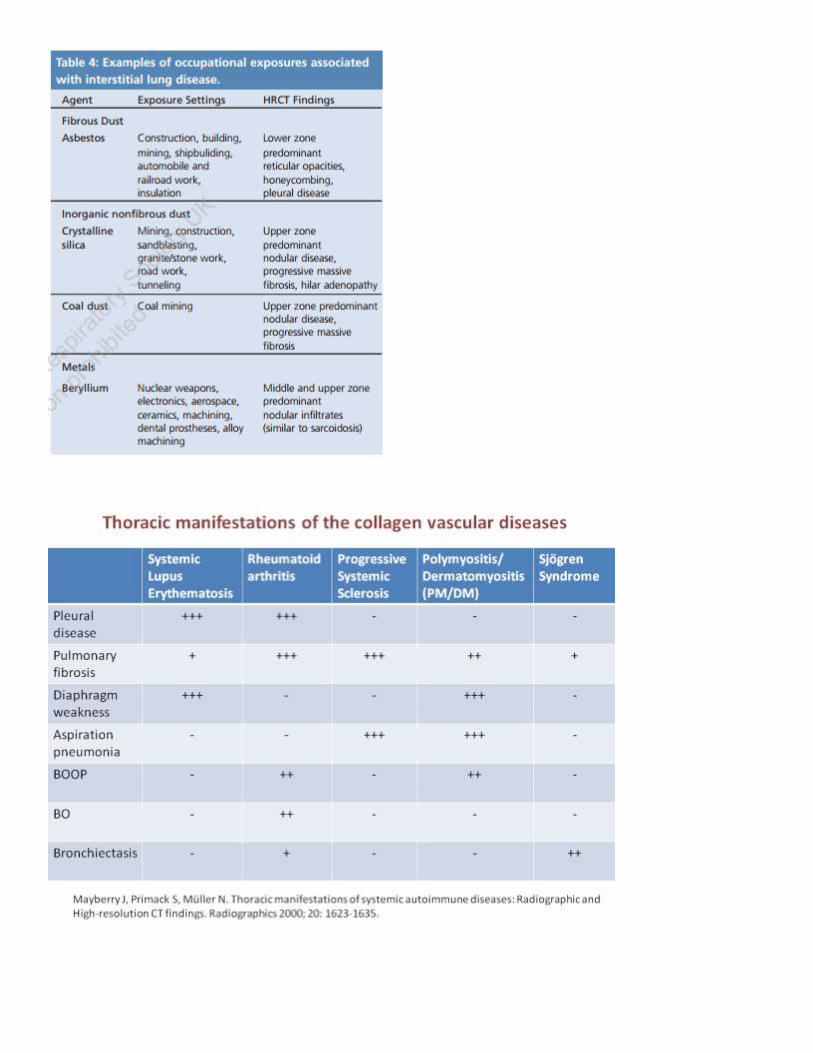
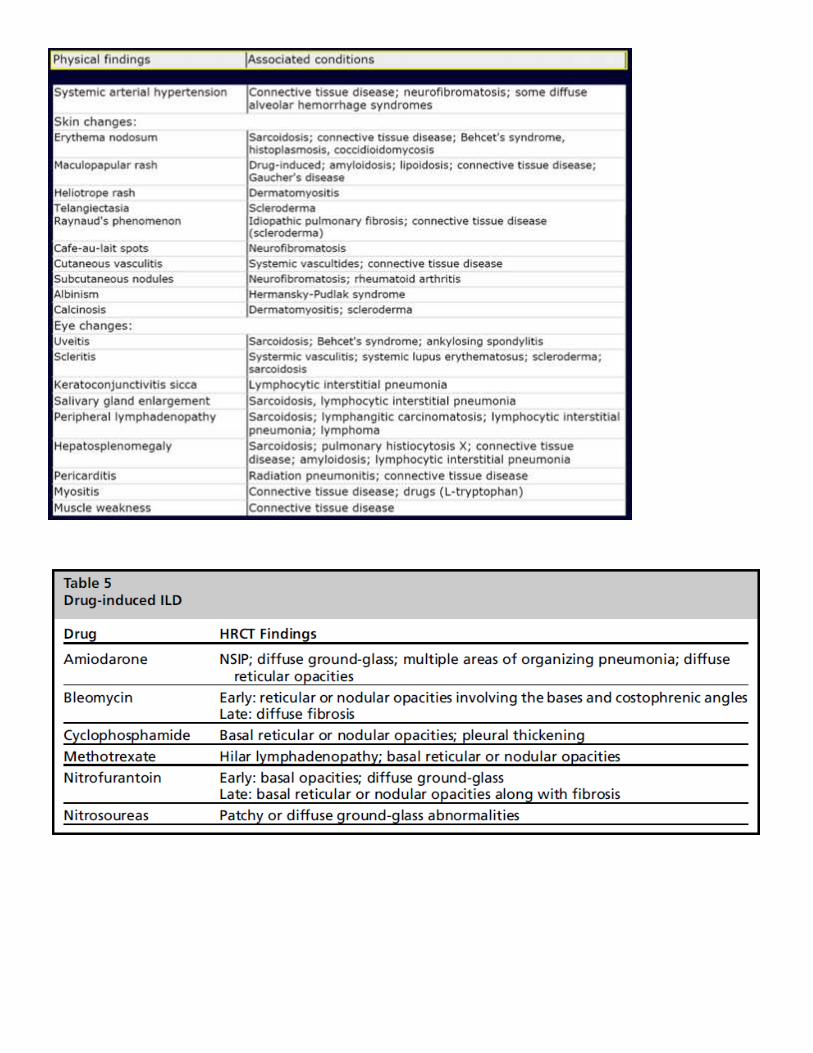
vi. Exposure/toxins (pets/hobbies/occupation/home environment) vii. CVD (RA, scleroderma etc)
viii. Malignancy ix. Symptoms (no extrapulm sxs in IPF; CP pleurisy in CVD) x. Labs (PFTS with DLCO, ANA, RF, ANCA, anti-BM ab, cryoglobulins, hypersensitivity panel)
b. Location/distribution i. Focal vs patchy vs diffuse
ii. Upper, middle, lower lobe pre-dominant (vs panlobar) iii. Peripheral vs central vs peribronchovascular (sarcoid, lymphangitic spread, LIP, lymphoma or
lymphoproliferative d/o, amyloid) iv. Reticular, reticulonodular, micronodular v. What is “fibrosis”? intra-lobular septal thickening (fine reticulation), traction bronchiectasis,
honeycombing all are considered fibrosis
c. Lines i. Peripheral reticular pattern if lower lobe predominant
1. UIP 2. Fibrotic NSIP assoc with chronic CVD (esp scleroderma) and RA (distal clav absorption) 3. Drug toxicity (BAM=bleomycin, amiodarone, methotrexate) 4. Asbestosis (parenchymal bands and curvilinear subpleural lines) 5. Chronic emphysema (smoking-related interstitial dz)
ii. linear pattern (aka lines radiating from hila +/- kerley lines) “LIFE” 1. Lymphagitic spread 2. (Atypical) infection like viral/mycoplasma 3. Fibrosis like IPF 4. Edema
iii. Septal thickening 1. Intra-lobular (fine reticular=fibrosis) 2. Inter-lobular septal thickening (secondary lobules)—if not the predominant finding,
can ignore this!! a. Smooth septal thickening (water=edema, pus=infx, blood=hemorrhage,
protein=PAP) b. Nodular septal thickening (sarcoid, lymphangitic spread, LIP, lymphoma or
lymphoproliferative d/o, amyloid) c. Irregular (any fibrosing lung dz)
iv. Subpleural lines or parenchymal bands (scarring/fibrosis, atelectasis, asbestosis)
d. Nodules i. Micronodules (<3-5mm)
1. Centrilobular (evenly spaced, don’t extend to pleura or fissure) a. GG (ill-defined)
i. HP subacute in non-smoker (classic), hemosiderosis ii. RB or RBILD in smokers (“subtle GG nodules” in smokers)
iii. Associated with NSIP (CVD) and OP/COP b. Solid with TIB (90% infectious bronchiolitis)
i. Think inflammatory /infectious bronchiolitis vs Aspiration
ii. If central mucus plugging (finger-in-glove), consider asthma, CF, ABPA iii. Mimicker=tumor emboli (branching tumor in enlarged vessel in
peribronchovascular distribution) iv. AIDS-related airways disease v. Endobronchial mucinous adenoCA (BAC)
c. Solid without TIB i. Pneumoconiosis/Silicosis (look for PMF etc)
ii. EG (aka pulm LCH)--if nodules are dense; may cavitate 2. Perilymphatic (patchy and abut pleura and fissure)
a. Sarcoid, lymphangitic spread, LIP, lymphoma or lymphoproliferative d/o, amyloid
3. Random (aka miliary; diffuse/uniform unlike perilymphatic) a. METS-B=hematogenous mets (thyroid/renal/melanoma), EG, miliary
TB/fungal/disseminated viral, sarcoid/silicosis, BAC ii. Branching nodules within enlarged vessel in peribronchovascular distribution = consider
tumor emboli
e. GGO (can see vessels thru it) i. Differential similar to consolidation
ii. “ABCDEH”= PAP, BOOP/COP, PCP, DIP, Drugs, Edema, HP, Hemorrhage iii. Acute vs chronic
1. Acute GGO a. Edema (CHF and in ICU pts consider ARDS/DAD/AIP) b. Hemorrhage (hemosiderosis) c. Atypical infx (PCP in AIDS and CMV in post-transplant) d. Subacute HP (“head-cheese”)
2. Chronic GGO a. PAP (“crazy paving”=geographic GG with septal thickening), PCP (UL cysts and
perihilar GG in HIV pt) b. BOOP/COP (peribronchial and subpleural “polygonal” fleeting consolidations,
GGO, and nodules) c. DIP and NSIP d. Drugs (BAM=bleomycin, amiodarone, methotrexate) e. HP (exposure) f. BAC
iv. Crazy paving ddx= PAP, pulm edema, pulm hemorrhage, drug-induced pneumonitis, PNA (bacterial like mycoplasma etc), BAC, COP
v. History helps 1. Hemoptysis=hemorrhage 2. Immunocompromised=infx (PCP) 3. Exposure=HP (non-smoker) 4. CVD or ILD=alveolitis
f. Mosaic attenuation
i. How to tell from GGO=Geographic (sharply demarcation on inspiratory view), differential vessel size (smaller in lucent areas), air-trapping (on expiration dark areas remain dark), stable over time
ii. Note: Mosaic attenuation is an INSPIRATORY HRCT finding while air-trapping is a EXPIRATORY HRCT findings!!
iii. small airways disease vs small vessel disease do expiratory view to distinguish btwn the two
iv. SMALL VESSEL DISEASE (less common) =no air-trapping; larger areas of non-lobular lucencies with normal vessel size; pulm HTN and R heart enlargement
1. Chronic PE (look for associated pulm HTN) 2. Vasculitis (CVD)
v. SMALL AIRWAYS DISEASE =with air-trapping; lobular areas of lucencies with small vessel size; peribronchial thickening
1. PFTs=decreased VC; decreased FEV1; increased RV; normal FEV1/VC ratio; normal TLC 2. Direct signs of small airways dz=bronchial wall thickening, bronchiolectasis,
centrilobular nodules with TIB 3. Indirect signs of small airways disease dz= mosaic attenuation (described in
inspiration), air-trapping (described in expiration; mosaic attenuation persists and contours get even more sharply marginated)
4. Bronchiolitis a. Smokers (RB, RBILD) b. Infectious (viral in kids like RSV/adenovirus/mycoplasma; MAC/TB/fungal in
adults) i. Swyer James (recurrent viral infx in kids <8yo; unilateral hyperlucent
small lung identified on CXR) c. Diffuse panbronchiolitis (exclusively Japanese) d. Follicular bronchiolitis (CVD like sjogrens, RA, HIV)
5. B.O./constrictive bronchiolitis (swyer james in kids <8yo with unilat hyperlucent small lung identified on CXR)
a. Etiology: i. Recurrent viral infx (including mycoplasma)
iii. Bronchiectasis 1. Cylindrical vs varicose (beaded) vs cystic (saccular) 2. Bronchiectasis ddx
a. Recurrent infx/aspiration (like TB, MAI=lady widemere) b. Finger-in-glove=CF/ABPA c. Congenital=immotile cilia (kartageners)/william-campbell (Mounier
Kuhn=tracheobronchomegaly) d. Fibrosis=traction bronchiectasis e. Emphysema
iv. Honeycombing 1. Associated with interface sign=irreg margins of pleural and vessels; associate with
i. Others i. Air-trapping (emphysema, BO/swyer james, LAM, EG, CF)
ii. LN (not uncommon in IPF esp if <15mm and only involves 1-2 nodal stations like paratracheal or subcarinal; usually responds to therapy like steroids)
1. Low density LAD= TB/MAI, wipples/crohns, untreated lymphoma, mets (testicular etc) 2. High density LAD= castlemans, carcinoid, Kaposi, LN mets from RCC (hemorrhage) 3. Calcified LAD= TB, sarcoid/silicosis, treated lymphoma, papillary thyroid CA
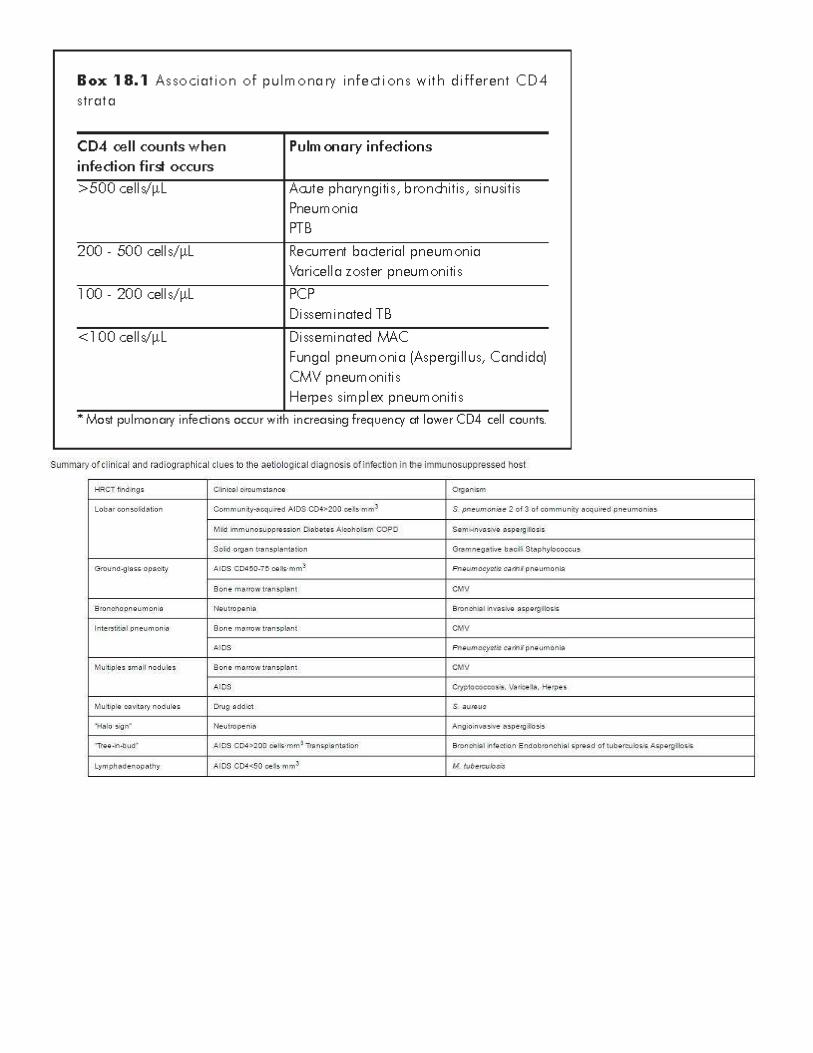
iii. Effusion (pleural/pericardial)—think CVD or RA iv. HIV “please test my CDfour”
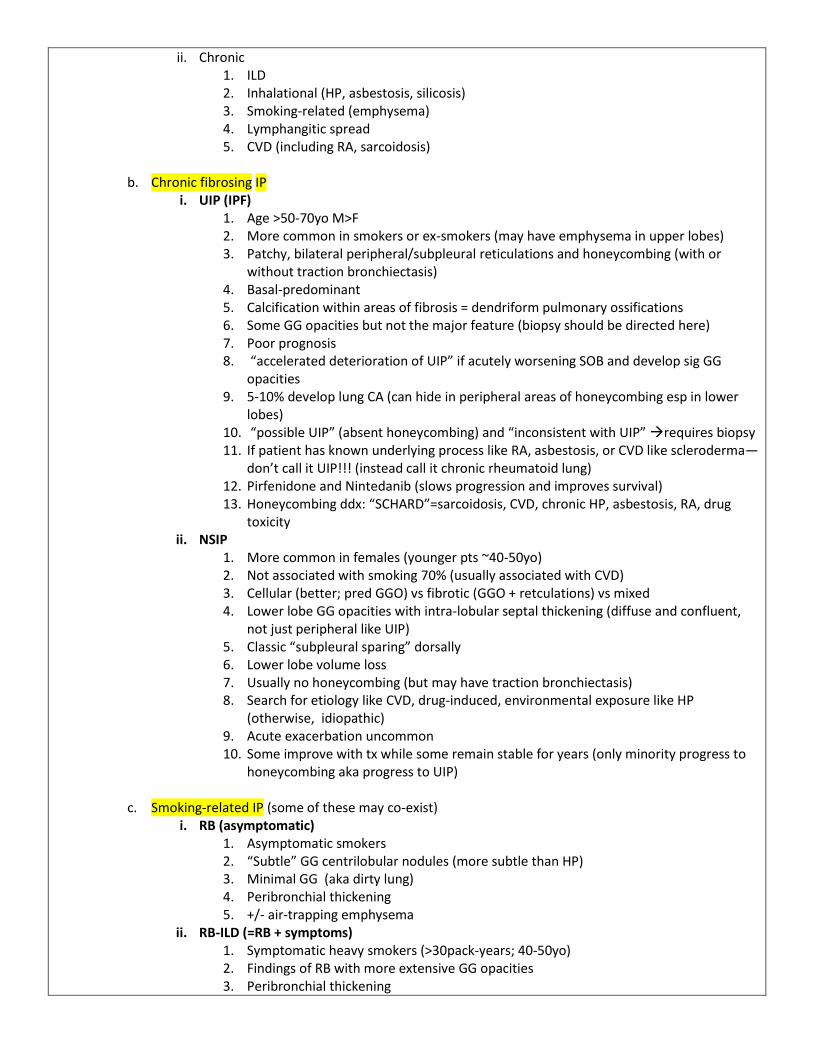
i. UIP (IPF) 1. Age >50-70yo M>F 2. More common in smokers or ex-smokers (may have emphysema in upper lobes) 3. Patchy, bilateral peripheral/subpleural reticulations and honeycombing (with or
without traction bronchiectasis) 4. Basal-predominant 5. Calcification within areas of fibrosis = dendriform pulmonary ossifications 6. Some GG opacities but not the major feature (biopsy should be directed here) 7. Poor prognosis 8. “accelerated deterioration of UIP” if acutely worsening SOB and develop sig GG
opacities 9. 5-10% develop lung CA (can hide in peripheral areas of honeycombing esp in lower
lobes) 10. “possible UIP” (absent honeycombing) and “inconsistent with UIP” requires biopsy 11. If patient has known underlying process like RA, asbestosis, or CVD like scleroderma—
don’t call it UIP!!! (instead call it chronic rheumatoid lung) 12. Pirfenidone and Nintedanib (slows progression and improves survival) 13. Honeycombing ddx: “SCHARD”=sarcoidosis, CVD, chronic HP, asbestosis, RA, drug
toxicity ii. NSIP
1. More common in females (younger pts ~40-50yo) 2. Not associated with smoking 70% (usually associated with CVD) 3. Cellular (better; pred GGO) vs fibrotic (GGO + retculations) vs mixed 4. Lower lobe GG opacities with intra-lobular septal thickening (diffuse and confluent,
not just peripheral like UIP) 5. Classic “subpleural sparing” dorsally 6. Lower lobe volume loss 7. Usually no honeycombing (but may have traction bronchiectasis) 8. Search for etiology like CVD, drug-induced, environmental exposure like HP
(otherwise, idiopathic) 9. Acute exacerbation uncommon 10. Some improve with tx while some remain stable for years (only minority progress to
honeycombing aka progress to UIP)
c. Smoking-related IP (some of these may co-exist) i. RB (asymptomatic)
ii. RB-ILD (=RB + symptoms) 1. Symptomatic heavy smokers (>30pack-years; 40-50yo) 2. Findings of RB with more extensive GG opacities 3. Peribronchial thickening
4. Air-trapping (emphysema) 5. Self-limiting
iii. DIP (not very common; less common than RBILD) 1. M>F smokers (30-40yo) 2. Bibasilar predominance GG with +/-fine reticulations (not much septal thickening) 3. Classic “cystic changes within GG opacities”may represent bleb related to
emphysema 4. No fibrosis 5. Treat with cessation of smoking and steroids
iv. EG (pulmonary LCH) 1. 20-40yo smokers, M+F, whites more common 2. Upper lobe pred nodules thin-walled cyst thick-walled cyst irregular/bizzare-
1. Upper lobe honeycombing, septal thickening, and traction bronchiectasis vi. CPFE (combined pulmonary fibrosis & emphysema)
1. 60-70yo male who are heavy smokers 2. Upper lobe emphysema 3. Lower lobe NSIP fibrosis 4. Lung vol are preserved 5. Decreased DLCO 6. 50% have pulm HTN 7. Worse prognosis than UIP
d. Acute/subacute IP
i. OP/COP 1. More common in non-smokers 2. Assoc with infx, drugs, autoimmune dz (esp myositis syndromes) 3. Acute onset <3mos of flu-like syndrome (SOB/cough/fever/chills/wtloss) 4. Peribronchial and subpleural consolidations (“polygonal shaped” or irregular)—can be
migratory (may have lobar predominance, not diffuse) 5. GGO (crazy paving) 6. Centrilobular nodules 7. Classic “reverse halo” or “atoll” sign (rare but specific) 8. Involve mid to lower lung 9. May have small effusion 10. Can be idiopathic or assoc with CVD, drugs, aspiration, infx 11. Restrictive lung disease like other ILDs 12. Excellent response to steroids (with complete recover in most pts) 13. Main DDx is chronic eos PNA can look very similar (look for peripheral eso)!!
ii. DAD/AIP (Hamman rich) 1. AIP= idiopathic ARDS (which responds to steroids which are generally avoided in
infectious ARDS)—if have patient with ARDS who is not responding to conventional tx, consider this diagnosis
2. Acute (<1wk) fulminant (ICU patients) 3. Appearance similar to ARDS but higher mortality 4. Diffuse confluent GG sparing CPAproliferative/organizing anterior upper lobe
fibrosis fibrotic with traction bronchiectasis
e. Others entities i. LIP
1. B9 lymphoproliferative disorder with lymphocytic infiltrates 2. Exclusively in Sjogrens or RA (adults) or AIDS (kids<13yo) 3. Retriculonodular pattern, GGO, and cysts
a. Peribronchovascular and centrilobular nodules b. GGO c. Peribronchovascular/subpleural/randomly-distributed cysts
4. Associated with monoclonal or polyclonal gammopathy 5. May progress to lymphoma (5%)
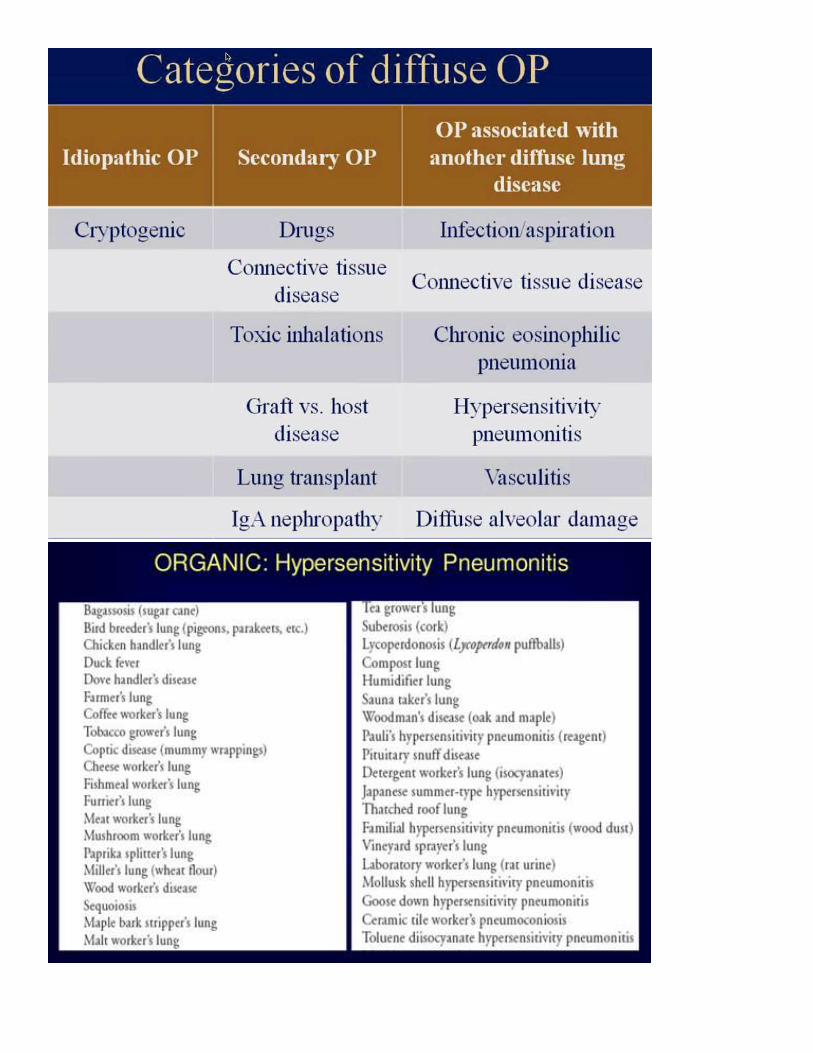
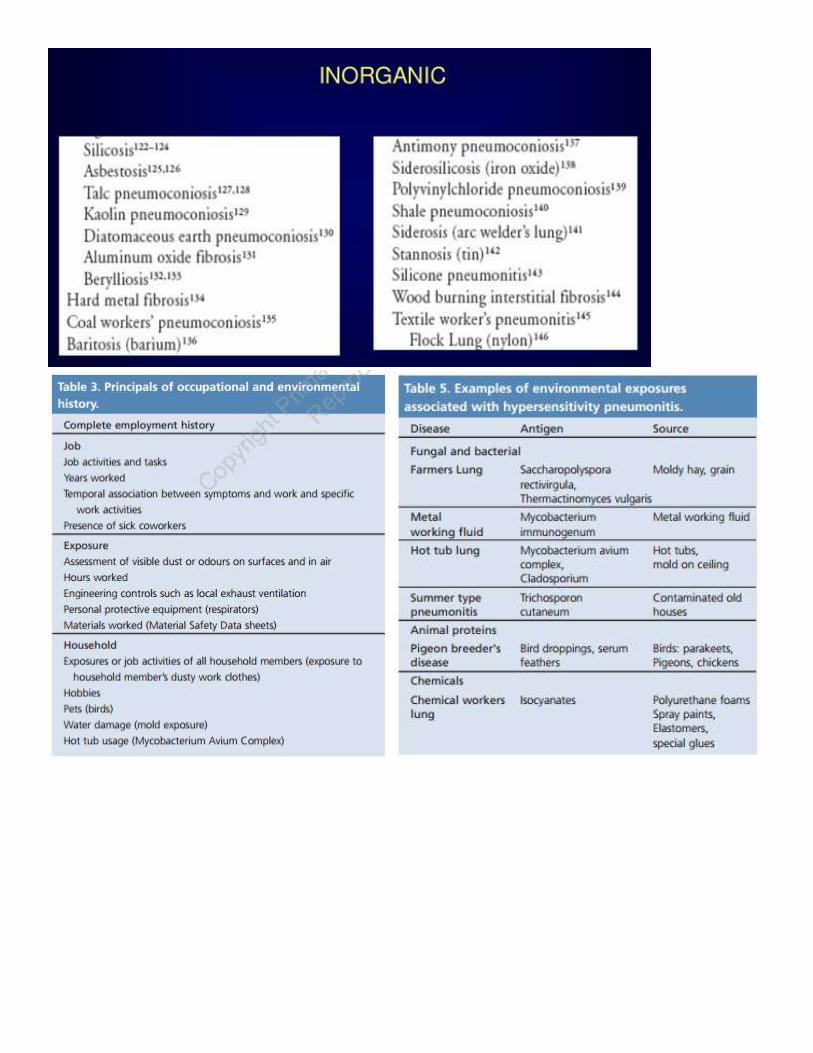
ii. HP (EAA) 1. Organic antigen=EAA (farmer, bird fancier, pigeon breeder etc) 2. Inorganic antigen=pneumoconiosis 3. Acute (lower lobe pred; diffuse airspace dz w/ GGO; mimics edema or
ARDS)=symptoms <1mo 4. Subacute (symptoms wks to 4mos)
a. Upper to mid lung b. GG Centrilobular nodules (classic—ddx is hemosiderosis or RBILD if subtle) c. Head-cheese (mosaic attenuation)
5. Chronic (fibrosis in similar pattern as the head-cheese pattern of subacute dz with mosaic attenuation and air-trapping)=symptoms >4mos to yrs
6. Smoking is protective (tell the pigeon-fancier to start smoking!) iii. PPFE (pleuroparenchymal fibroelastosis)
1. 50-60yo (usually post-lung or BM transplant) 2. Similar to fibrotic TB in upper lung zone 3. Peripheral upper lobe fibrosis, pleural thickening, and upward retraction of hila
f. CVD (usually associated with NSIP)
i. RA 1. Pleural/pericardial effusion 2. Necrobiotic nodules 3. Distal clavicular erosions 4. Constrictive bronchiolitis (B.O.) and BOOP may co-exist
ii. Scleroderma 1. Dilated eso 2. Pulm HTN 3. Calcinosis (calc arounds joints if CREST syndrome)