42
Child Health Eight week check Elaine Burfitt July 2010
| Date post: | 02-Jan-2016 |
| Category: |
Documents |
| Upload: | barnaby-hubbard |
| View: | 215 times |
| Download: | 2 times |
Child Health
Eight week check
Elaine Burfitt
July 2010
Child Health
Eight week check
Check list
Referral information
DVD
Pitfalls
Schedule
Screen Newborn - SHO or midwife 6-8 weeks - GP or HV
Non screen status 2 year check - nursery nurse

Eight week check
Newborn & Infant Physical Examination Standards and Competencies March 2008 UK National Screening committee
Local referral information
Awaiting Public Health oversight
Eight week checklist
Examine in appropriate surroundings, preferably with calm, fed baby
Take opportunities to discuss health promotion messages along the way e.g. smoking, back to sleep, careful handling, etc.
Brief review of birth history, general health and feeding.
Review red book information to
date including hearing screening data
Ask carer if they think baby can
see and hear
Ask carer if any concerns about baby
Sets context of examination and growth assessment. May have missed hearing screen or not had a clear response.
Eight week checklist
Head to toe examination All areas of skin must be seen at some point during the examination. May carry out some parts of examination when babe is dressed or partially dressed in order not to disturb ie when auscultating the heart but still need to carry out examination appropriately.
Including general handling, demeanour, skin, head shape and size, fontanelles, dysmorphism, eyes including red reflex and visual fixation and behaviour, palate, neck, heart, abdomen, genitalia, spine, anus, hips, limbs including hands and feet.

Eight week check

Eight week check

Eight week checklist
Plot and assess growth
Complete red book Discuss outcomes with
parent/carer
Send in return slip Make any referrals needed
Immunisation as appropriate With appropriate consent

Eight week check

Eight week check

Eight week check
Sacral dimple is simple if:
< 5mm diameter Lying in midline <25 mm from anus

Heart defects Screen all by 72 hours
Refer all screen positive within 24 hours of examination for pulse oximetry and expert consultation
Review by 10 days if considered at risk of clinical deterioration
1st appointment within 4 weeks if no significant clinical risk
Heart defects
6-8 week check
Refer by phone if symptomatic at that time
No other timescales recommended at present
Hearing
Universal neonatal screening Oto acoustic emissions
Normal Abnormal - further diagnostics Normal but in high risk group – 8 month FU Incomplete test or not done

Hearing
Check parental concerns Check neonatal screening page
Encourage attendance at further screen or diagnostic appointments
If unclear ring neonatal screeners for information on child on pathway
Fill in slip appropriately

Hearing
Several missed in recent years
Presented May 2008 by Hilary Smith
Jan 2008 – Dec 2009
78 babies recorded on 8 week slip as normal hearing when had NCR in one or both ears on neonatal screen

Hearing
Pre screening average age of aiding 22 months
i.e. huge loss of developmental window for learning language
Recent good examples of successes

Vision
Neonatal check no concerns
8 weeks parental concerned about visual behaviour
Reported to HV/ GP at time of 8 w check

Vision
Referred to paediatrician by letter
Seen by paediatrician at 12 weeks
Concern regarding red reflex

Congenital cataract
Tel ref to ophthalmologist
Operation at 13 weeks (despite anaesthetic risk re URTI at the time)
17 m no detectable VI problem over and above lens limitation


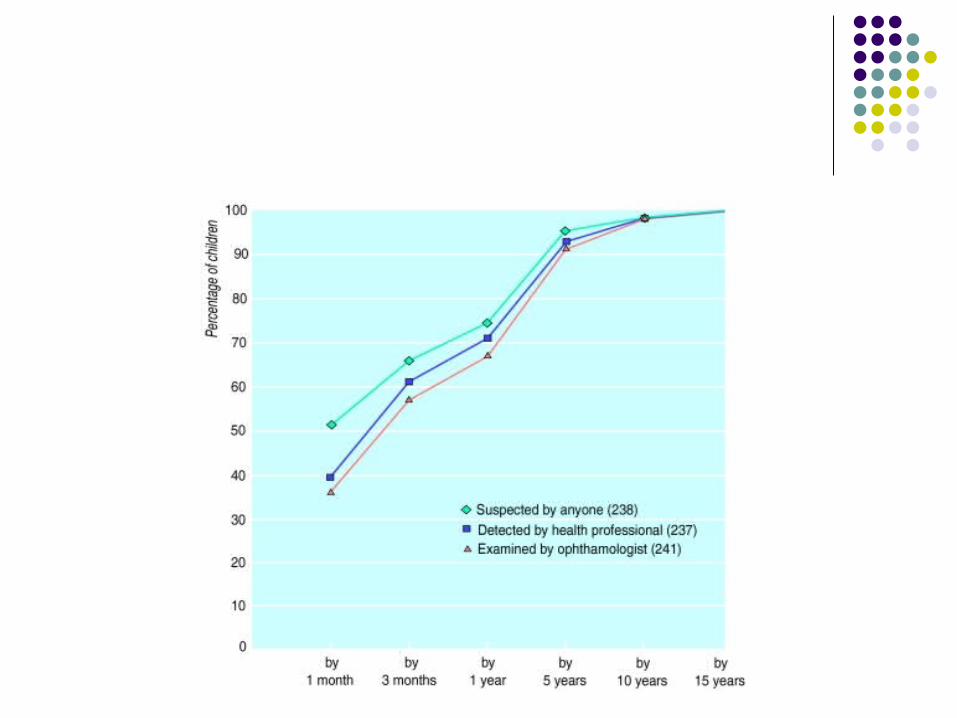
Congenital cataract survey 1995-1996 12 months Data on 235 children
35% detected at newborn 12% detected at 6-8 week check
By 3 months 47% had been detected by screening and 57% of these had seen an ophthalmologist
Vision
Neonatal Inspect external eye structures and red reflex Referral to ophthalmologist see below National recommendation to be seen within 2 weeks of birth Retinopathy of prematurity, < 31 weeks and/ or < 1500g then should be in ophthalmology screening pathway at neonatal unit.



6-8 week check
Establish if any concerns of parents and check relevant family history
Observe visual behaviour Observe visual fixing and following Inspect external eye structures Check red reflexes
Abnormal red reflexes are to be referred urgently to ophthalmology at Manchester Eye Hospital. Urgent means including phone contact ASAP with paediatric ophthalmology, via switch 0161 2761234 Retinoblastoma can be life threatening Congenital cataracts need to be operated upon by 12 weeks of age to prevent loss of vision development.



Other vision concerns include possible severe vision impairment or parental concern of such. Refer to Mr Simon Wallis, Bolton Royal, does weekly Thursday Pendleton Gateway clinic and will see with low threshold urgently. Urgent fax referrals 01204 390051, Confirm by Tel 01204 390390 ext 3935 Squint, family history of squint or any vision concerns/reduced vision will be seen by orthoptists via chose and book and liase with Mr Wallis accordingly

Vision
4-5 years Universal screen by orthoptist. Orthoptists available for discussion of concerns. Work closely with ophthalmology, based in Sandringham 0161 2124128 or [email protected]

8 week vision
Fixing and following

Hips
Neonatal examination
Universal Ortolani and Barlow screen in hospital Dislocated or dislocatable hips for urgent referral to orthopaedics and hip ultrasound Ultrasound arranged for high risk babies, screen positive as above or clinical concern, particularly marked limited abduction.
Referrals are made directly to orthopaedics from neonatology and Dr Jill Carling, paediatric radiologist at SRFT

Hips
8 week check Universal Ortolani and Barlow screen (Not if already seeing orthopaedics for such/ in harness!) Confirm US appointment has been attended if high risk National Screening Committee March 2008 definition of high risk:
Clinical diagnosis of breech presentation at any time, even if cephalic birth
Family history of DDH (Developmental Dysplasia of the Hip)
Locally Talipes or other lower limb abnormality is also considered to indicate a high risk baby Screen positive, clinical concern or high risk baby not already in the system at SRFT or elsewhere then referral for urgent hip ultrasound at SRFT. Urgent fax number at SRFT is 0161 2065494 Note that asymmetrical thigh creases with no other positive findings or history are not an indication for referral.
Hips
Older ages Refer if needed because of clinical concern at any later date direct to Mr Henry orthopaedic surgeon at RMCH Refer via fax to 0161 7015421 Tel confirmation of receipt is requested on 0161 7015352 Referral will be triaged clinically Weekly hips clinic is at RMCH

Hips
Video / DVD

Testes Neonatal check
Bilateral undescended – 100% to see paediatrician within 24 hours
Unilateral – make parent aware and review at 6-8 weeks

Testes 8 weeks
Bilateral undescended
Refer to surgeons
C&B
Appointment by 1 year old Operation by 2 years old

Testes 8 weeks
Unilateral
All reviewed by GP at 22-26 weeks
Child Health computer can notify
Refer to surgeon at review if needed
All seen by 1 year and all operated on by 2 years of age
Eight week check
Be thorough
Check slips and send in returns
Thank you very much
DVD

















