Children’s Mental Health: From One Kid ….. to Ten Kids…… to All Kids Larke Nahme Huang, Ph.D. Office of the Administrator Substance Abuse and Mental Health Services Administration For State Children’s Mental Health Directors December 8 , 2009
Transcript
Children’s Mental Health: From One Kid ….. to Ten Kids……
to All Kids
Larke Nahme Huang, Ph.D.Office of the Administrator
Substance Abuse and Mental Health Services AdministrationFor
State Children’s Mental Health DirectorsDecember 8 , 2009
Connecting with “New Drivers:” new context, new conversations
• The Economic Context and Children• An Unsurmountable Treatment Gap• The Public’s Health
– Surveillance and Data-Smart– Interdisciplinary Prevention– Promoting New Partnerships
• Positioning for Health Care Reform and Administration Policies
• Institute of Medicine Reports
Emerging Trends in 2009 Economic Context
• Economic setbacks for nation’s children: more likely to live in poverty, less likely to have at last one parent employed year round, more living in inadequate housing
• Poverty: 10% of White ; 35% of black and 29% of Hispanic children living in poverty
• Slight declines in preterm birth and low birth weight
• Slight increase in birthrate among adolescent girls; these babies in homes with less emotional support and cognitive stimulation, less likely to earn high school diploma
• Proportion of all births to unmarried women highest ever level recorded
Children Hit Hardest with State Budget Cuts (Urban Institute, 2009)
• Children’s hospital, pediatricians hardest hit by state cuts• One in four children (22M) – health coverage is Medicaid or
Children's Health Insurance Program; turned away at providers, etc.
• Reduced reimbursement rates reduce access• Privately insured affected as hospitals and providers cut staff
due to revenue shortfalls• Medicaid: primary payer for children’s mental health• State furloughs; budget shortfalls impact on children’s
services
Figure 1.1. Causes of Disability*United States, Canada and Western Europe,
2000
Causes of disability for all ages combined. Measures of disability are based on the number of years of "healthy" life lost with less than full health (i.e., YLD: years lost due to disability) for each incidence of disease, illness, or condition.
The Global Burden of Mental and Substance Use Disorders
The Global Burden of Mental and Substance Use Disorders More than 10% of lost years of healthy life Over 30% of all years lived with disability Contributing factors:
Relatively high prevalence Early onset of mental disorders Chronic or recurring nature of these disorders Severity of disability associated with many
mental disorders Low rates of case recognition and lack of
access to effective treatment
World Health Organization, 2006
The Treatment Gap: Importance of partners
In 2006, 23.6 million people aged 12 or older needed treatment for an illicit drug use or alcohol use problem. Of these, only 2.5 million received treatment at a specialty facility.
In 2006, 24.9 million adults (> 18 yrs)reported serious psychological distress, less than half of 10.9 million people (44%) received treatment in the past year.
(NSDUH, 2007)
Had at Least One Major Depressive Episode (MDE) in Past Year and Receipt of Treatment in the Past Year for Depression among Persons Aged 12 to 17 by Race/Ethnicity: Percentages 2005 (NSDUH)
8.8 8.7 9.1
7.6
6.1
0
6
10.59.1
0
2
4
6
8
10
12
14
16
18
20
TOTALNot Hispanic orLatino
White AfricanAmerican
AmericanIndian/Alaska
Native
NativeHawaiian/OtherPacific Islander
Asian Two or MoreRaces
Hispanic orLatino
Race/Ethnicity
Per
cen
t
Past Year MDE
Receipt of Treatment inPast Year among Personswith Past Year MDE
9
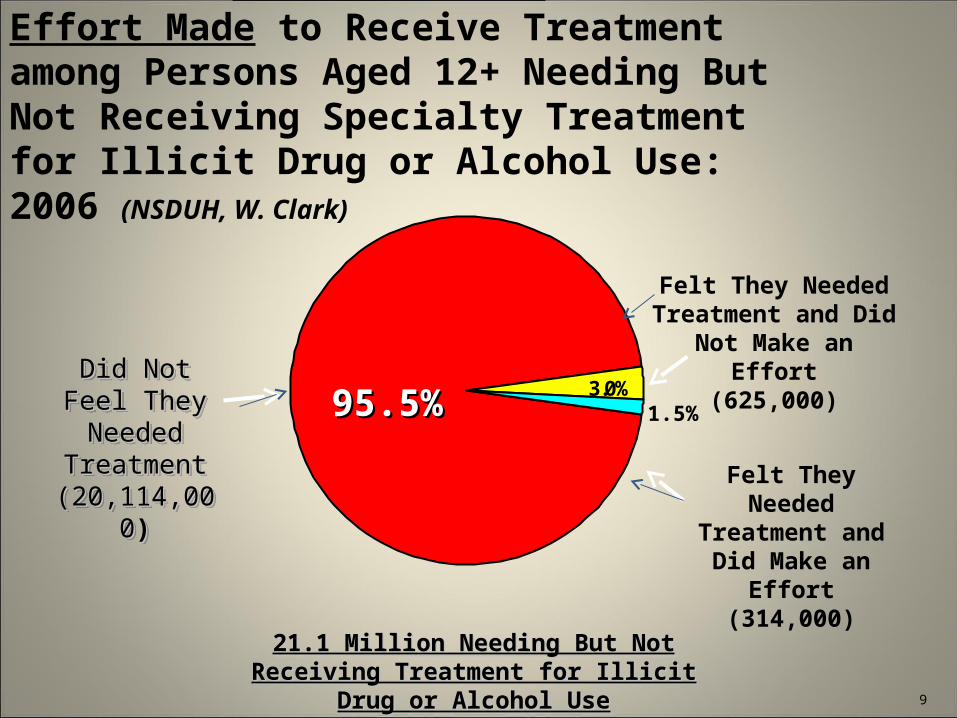
21.1 Million Needing But Not Receiving 21.1 Million Needing But Not Receiving Treatment for Illicit Drug or Alcohol UseTreatment for Illicit Drug or Alcohol Use
3.0%
Felt They Needed Treatment and Did
Make an Effort(314,000)
Did Not Feel Did Not Feel They Needed They Needed
TreatmentTreatment(20,114,000(20,114,000))
Did Not Feel Did Not Feel They Needed They Needed
TreatmentTreatment(20,114,000(20,114,000))
Felt They Needed Treatment and Did Not Make an Effort
(625,000)
1.5%95.5%95.5%
Past Year Perceived Need for and Effort Made to Receive Treatment among Persons Aged 12+ Needing But Not Receiving Specialty Treatment for Illicit Drug or Alcohol Use: 2006 (NSDUH, W. Clark)
Beyond the “One child at a time” Approach
• Need for a public health approach• Factors contributing to the “public’s health”• Population approach with promotion and prevention
component• Prevention is NOT a single intervention• Interventions must be evidence-based• Integrated prevention is based in both the
community and the health system• Payment reform is critical
Burden of Childhood Mental Emotional Behavioral Disorders
• Most costly and prevalent of all chronic childhood illnesses• Estimates of 20% of children/adol have diagnosable MEB
disorder• Annual financial costs est. $247 billion by National
Research Council, Institute of Medicine, 2009• Non-financial costs: distress and suffering of youth/family,
disruption in families, schooling; burdens on social welfare, education, health care, justice systems
• Cumulative effect over lifetime on productivity, quality of life and physical health
Reform of Health Care Sector, Reform of Health Care Sector, “Necessary but not Sufficient”“Necessary but not Sufficient”
• Access and quality alone will not significantly reduce inequities
• Health care:– is NOT the primary determinant of health– Treats one person at a time– Often comes too late– ~40% health outcomes attributed to
Data Presentation TechnologiesData Presentation Technologies
• Place Matters Place Matters • Geomapping: capacity to map and track dataGeomapping: capacity to map and track data• Compelling Examples:Compelling Examples:
– National Cancer Institute: cancer clustersNational Cancer Institute: cancer clusters– Prevalence of Major Depressive Episodes by Prevalence of Major Depressive Episodes by
Professional Shortage Areas by Census DataProfessional Shortage Areas by Census Data– San Francisco: viral loadings (disease severity) as San Francisco: viral loadings (disease severity) as
determinant of need for AIDs services – beyond determinant of need for AIDs services – beyond just case countsjust case counts
2020
2121
Primary Advantages for Policymakers (J.Holt, CDC 2009)
“Access” to data (tangible and cognitive)Gaining insights into spatial relationships – identifying patterns in the dataInterpretation – how “my” area compares to neighbors and/or other similar areasConveying complex information in an effective way to a variety of audiences
Obesity Trends Among U.S. AdultsBRFSS, 1985BRFSS, 1985
Prevention: Untapped Opportunity to Reduce Burden of Disorders on Children
• Requires paradigm shift to proactively promote health and prevent disorder
• Mental health and physical health inseparable• Successful prevention is inherently interdisciplinary• Coordinated community level systems are needed to
support young people• Developmental perspective is essential• Target risk factors that contribute to wide range of
friend attempting suicide; peer norms• 40% reduction in North Dakota youth suicide
Landmark Studies re Trauma in Childhood and Adult Chronic Diseases
• Emerging evidence of trauma associated with chronic diseases – physical, mental and substance use
• Experiences in childhood have impact throughout life…brain, cognitive and behavioral development early in life are strongly linked to an array of important health outcomes…including cardiovascular disease and stroke, hypertension, diabetes, obesity, smoking, drug use, and depression… (2008 RWJ Report)
• Adverse Childhood Experiences Study: numbers of ACES in childhood directly linked with chronic diseases (Fellitti, et al)• Example: 0-5 year olds more likely to be present when domestic
violence occurs• Greater number of ACES linked with physical, emotional and
substance use disorders in adulthood• 8.3M or 11.9% of children live with a substance dependent or abusing
parent (SAMHSA, NSDUH, 2009)
Optimizing Partnerships
• Child Care/Head Start• Community Health Centers (Primary Care)• After school Programs (USDA/Cooperative Extension)• Public Housing Authorities (HUD)• United We Ride (Transportation)• NGO, Private Entities, Faith-based Orgs.
– YMCA – 10,000 centers-involved in positive youth development
– Big Brothers/Big Sisters (corporate relationships)– Congregants as “first responders”
Potential Growth Areas: Community Health Centers
• 53% CHC located in rural areas (even split urban/rural)
• Frequently only source of primary and preventive services
• Serve 1 in 7 of all U.S. rural residents• 2/3 rural health center patients are uninsured,
Medicaid• 3/5 are ethnic/racially diverse• 74% of rural CHCs provide MH counseling on site• 60% of rural CHCs provide substance abuse
treatment/counseling
Integration of Behavioral Health and Primary Care
• Funding to build more Community Health Centers and expand services in existing CHCs
• SAMHSA: Screening, Brief Interventions and Referrals to Treatment in CHC
• CDC: Triple P in CHCs; FOA: more behavioral health screening in primary care settings
• Understanding of mental health and substance use disorders as chronic illnesses that start early in youth and need ongoing recovery management
Emerging Technologies• Telecare: extensive telephone follow-up: trained care
managers (nurse or pharmacist) – Demonstrated improvements in depression when
telecare is the primary intervention• Telephone Support: perinatal depression prevention: lower
depressed mood among women• Web-based Interventions: CBT effective when provided
over internet for depression and anxiety: psychoeducation, interaction, and additional telephone or email contact
• Text-messaging – Text4Baby= Health Mothers/Healthy Babies Coalition + Voxiva (provider of mobile health technology) + Johnson & Johnson + Wireless Foundation + federal agencies
Even the Feds are Collaborating: “Early Childhood Systems Federal Partners
Work Group”• Dept Health and Human Services
– ACF: Child Care Bureau, Office of Head Start (Child Abuse Prevention, Home Visiting Child Care Programs, HS/EHS)
– CDC: National Center on Birth Defects/Devel Disability and Human Development (Education/awareness, prevention programs)
– HRSA/MCHB: Early Childhood Comprehensive Systems Grants– SAMHSA: Prevention (Fetal Alcohol Syndrome, Project LAUNCH)
Treatment (Systems of Care, Child Trauma Initiative)
• Dept of Justice: OJJDP (Safe Start/ child Protection Program)• Dept of Education: Office of Special Education Programs (IDEA)• Joint Grantee and EC Summit: Aug 2010, Washington, D.C.
Early Childhood Systems Federal Partners Logic Model
Positioning for Health Reform
• Prevention and Wellness• Comparative Effectiveness Research• Health Information Technology
Important Prevention Components of House Bill
• Invest in prevention research to expand evidence-base
• Expand capacity of 2 independent advisory task forces: U.S. Preventive Services Task Force and Task Force on Community Preventive Services for systematic reviews
• Eliminate cost-sharing on recommended preventive services delivered by Medicaid, Medicare and Health Insurance Exchange
Prevention in House Bill
• Establish Prevention and Wellness Trust funded at $2.4B, FY 2010; $3.5B in 2014
• Fund activities of USPSTF (include expert on behavioral services for primary care)
• $1.1B for community-based prevention and wellness services
• $800M in FY2010 for core public health infrastructure and activities for state and local health departments, rising to $1.3B in FY2014
Important Prevention Components of Senate Bill
• Mandates national public –private partnership for prevention and health promotion outreach and education campaign
• Establish community transformation grants to fund programs that promote individual and community health and prevent chronic diseases, explicitly including mental illness
• Both bills include preventive services in essential benefits package
Other Provisions in the Bills
• Home visitation programs for early childhood • Grant funding for school-based health clinics• SBIRT in primary care settings• Workforce: loan repayment for child and adolescent
behavioral health; educate PCP about mental health• Postpartum depression: research and support
services
2009 Institute of Medicine (IOM) Reports
• Preventing Mental, Emotional, and Behavioral Disorders Among Young People:Progress and Possibilities- February 2009
• Depression in Parents, Parenting, and Children: Opportunities to Improve Identification, Treatment, and Prevention -June 10, 2009
“Preventing Mental, Emotional, and Behavioral Disorders Among Young People”
• Most mental, emotional, and behavioral disorders have their roots in childhood and youth.
• National priorities should include (1) provision of the best available evidence-based prevention interventions to at-risk individuals and (2) the promotion of positive mental, emotional, and behavioral development for all children and youth .
• Benefits exceed costs for many preventive interventions, with strongest evidence for this potential savings in early childhood.
• A number of specific preventive interventions can modify risk and promote protective factors that are linked to important determinants of mental, emotional, and behavioral health, especially in such areas as family functioning, early childhood experiences, and social skills.
• 148.8 million parents in the U.S.
• 17% parents had major or severe depression in lifetime (Nation Co-morbidity Study-Replication, 2002)
• 7% in past year had depression = 7.5M
• 15.6M children (<18yrs old) living with adult with major depression
• Depression disproportionately affects low income women of color
“Depression in Parents, Parenting and Children”
Impact of Maternal Depression on the Children
Associations: Low birth weight, prematurity, obstetrical complicationsPreschool: internalizing problemsChild’s negative relationship with peersReduced language ability (key to school success)Behavioral and academic problems in early schoolingMore likely to experience depression in adolescentsPeer difficulties
Consistent Exposure to maternal depression linked to disruptive behavior disorders, higher risk for depression, poor emotional/social competence in school and fewer friends (greater than for bipolar or other maternal health conditions).
Two Core Parenting Functions Effected: Fostering Healthy Relationships
Attachment and early brain development, nurturing vs. harsh parenting; balanced relationship and emotional regulation;
Carrying out the Management Functions of ParentingSafety guidelines, consistent routines, discipline, feeding,
facilitate child’s education and obtain “health home” for well-child and acute health care
Maternal history of maltreatment increases women’s risk for depression, substance abuse and domestic violence; puts child at greater risk of maltreatment
Parental Depression: Impact on Parenting
A Two Generation Approach
Barriers Facilities and providers specialize in either adults or
children, not both Rarely asked if adult with disorder has children in the home Child service system not equipped to identify parents with
substance and mental disorders Financing of delivery system – based on adult acute care or
individual well-child or acute care
Treatment for adult may be prevention for the child SAMHSA’s Project LAUNCH SAMHSA’s Pregnant-Postpartum Women in Substance
Abuse Treatment
Impact of Parenting Interventions
Screening in Substance Use Treatment Settings
SAMHSA: 58% of SUD TX Programs screening for mental health disorders
Other Studies: Among mothers: 83-88% screen positive for depressive
symptoms at treatment entry (Connors, et al., 2006; Lincoln et al., 2006)
Among pregnant women with SUD: ~56% have depressive symptoms (Fitzsimons et al., 2007)
48% pregnant drug-dependent women in a comprehensive SUD TX program: have current depressive disorder (Lincoln, et al., 2006)
Brief screeners, assessment and Tx urgently needed in SA treatment and training for frontline staff Mood disorders effect drug treatment success
(Fitzsimons et al., 2007)
Prevention EffortsIndividual Approach• Mothers and Babies Project: 8 week course on strategies to
increase pleasant activities, positive interpersonal relationships, positive thought patterns to control and manage mood; stress reduction through relaxation exercises and regular physical activity (pregnant, low-income women)
• Family Coping Skills Program: 6 group sessions, 2 family session; skills development (low income Latina mothers)
Two Generational Approach:• Family CORE: Communication, Openness, Resilience and
Empowerment; focus is to enhance parent-child communication, knowledge about disorder (single parent families)
Education in Communities re Depression
Early Intervention: Screening for Depression
• American Academy Obstetrics and Gynecology: rec psychosocial screening of pregnant women in 1st trimester– Over the past 2 weeks, have you ever felt down,
depressed, or hopeless?– Over the past 2 weeks, have you felt little interest
or pleasure in doing things?• Edinburgh Postnatal Depression Scale: 10 items,
widely used, multiple languages; CES-D• Screening in WIC Centers. TANF, Community Health