43
CHILEAN MINE WORKER HEALTH Workplace Health Promotion HOLLY FLETCHER University of Wollongong School of Health and Society May 2020

CHILEAN MINE WORKER HEALTH
Workplace Health Promotion
HOLLY FLETCHER
University of Wollongong
School of Health and Society
May 2020

2
Acknowledgements:
The researchers wish to acknowledge Codelco Andina and Clinica Rio Blanco who graciously offered the
resources and provided the access required to facilitate the collection of data.
Furthermore, the researchers wish to show special gratitude to Margarita Zambra Acevedo in facilitating the
standardised translation and testing of the research instruments and Maria Victoria Cox in supporting the
transcription and translation of the research data, results and final report and ensuring the integrity of such. We
are very grateful to both of you for your persistence and dedication.
Most significantly, the researchers wish to acknowledge all the research participants who volunteered their time
and effort to participate in this research. We are extremely grateful, as without your contribution this research and
associated body of knowledge would not have been possible.
Finally, but not least, the research team are forever grateful to Dr. José Ignacio Méndez Campos. Your incredible
commitment to this research and continual efforts to ensure resources were allocated and standardised data
collection systems were established meant this whole project was achievable. The words “thank you” are not
enough to express our gratitude.

3
SUMMARY
In Chile, the average body mass index (BMI) in adults increased from 27.2 kg/m2 in 2010 to 28 kg/m2 in 2016 and
when compared to other countries, is rapidly becoming one of the most obese populations globally (WHO, 2016a).
Overweight and obesity are major risk factors of chronic diseases including cardiovascular disease, type 2
diabetes, hypertension and musculoskeletal dysfunction, and in the context of occupational environments is a
likely contributing factor to occupational injuries and illness (Anandacoomarasamy, et al., 2008), among other
adverse outcomes such as healthcare costs, reduced productivity and business performance (Batt, 2009).
Chilean organisation, the Mutual de Seguridad (The Mutual) operates to provide technical services for risk
prevention programs in workplaces, including occupational medical surveillance and the trending of such
population data. Analysis of data has subsequently identified those persons servicing the Chilean mining industry,
generally experience poor health outcomes, including overweight and obesity and musculoskeletal injuries. To
that effect, The Mutual partnered with the University of Wollongong’s (UOW) School of Health and Society to
research workplace interventions that could improve nutrition and physical activity-related behaviours, wellbeing
and decrease musculoskeletal injuries in Chilean mine workers.
The reasearch comprised of two main components. Firstly, a review of the current body of knowledge on the
effectiveness of workplace health promotion interventions. Secondly, population data was collected and analysed
from a representative Chilean mine operation.
This report communicates the results and conclusions of those research activities.
4
Table of Contents
Summary .................................................................................................................................................................3
1 Introduction and Background .......................................................................................................................7
1.1 The “Obesogenic” Environment ................................................................................................................7
1.1.1 Risk of Non-Communicable Disease ................................................................................................7
1.2 Chilean Population Health ........................................................................................................................7
1.2.1 Obesity and the Chilean Adult Population ........................................................................................8
1.2.2 Physical Activity and the Chilean Adult Population ..........................................................................9
1.2.3 Chilean Adult Working Population ....................................................................................................9
2 Problem Definition and Relevance ...............................................................................................................9
2.1 Health Promotion Interventions ............................................................................................................. 13
2.1.1 Approaches to Health Prevention .................................................................................................. 13
2.1.2 Health Promotion in the Occupational Environment ...................................................................... 15
3 Literature Review ......................................................................................................................................... 15
3.1 Method ................................................................................................................................................... 15
3.2 Results ................................................................................................................................................... 16
3.2.1 Demographic Characteristics ......................................................................................................... 17
3.2.2 Health Promotion in the Occupational Environment ...................................................................... 18
3.3 Discussion.............................................................................................................................................. 19
3.3.1 Theoretical Framework for Health Promotion Interventions .......................................................... 19
4 Methodology................................................................................................................................................. 21
4.1 Participant Recruitment ......................................................................................................................... 21
4.2 Data Collection ...................................................................................................................................... 21
4.2.1 Questionnaire................................................................................................................................. 21
4.2.2 Interviews ....................................................................................................................................... 22
4.2.3 Group Medical Surveillance Data .................................................................................................. 22
5 Results .......................................................................................................................................................... 22
5.1 Study Population .................................................................................................................................... 23
5.2 Research Population Health Status ....................................................................................................... 24
5.3 Perceived Health ................................................................................................................................... 27
5.4 Value Placed on Good Health ............................................................................................................... 28
5.5 Desire for Change .................................................................................................................................. 30
5
5.6 Organisational Support .......................................................................................................................... 33
6 Conclusions ................................................................................................................................................. 34
6.1 Literature ................................................................................................................................................ 34
6.2 Research Population ............................................................................................................................. 35
6.2.1 Health Beliefs and Attitudes ........................................................................................................... 36
6.3 Organisation Health Promotion.............................................................................................................. 37
6.4 Recommendations ................................................................................................................................. 38
6.5 Limitations .............................................................................................................................................. 39
7 References.................................................................................................................................................... 40
Tables
Table 1 – Prevalence of Chronic Disease and Risk Behaviours: Chilean Adult Population - 2010 .........................8
Table 2 – Andina Mine Operation Pre-Occupational Medical Examination Data (2015 – 2016) .......................... 10
Table 3 – Specific Conditions Precluding Employment (Employment applications in 2016) ................................ 10
Table 4 – Andina Mine Occupational Medical Examination Data (2015 – 2016) .................................................. 11
Table 5 – Specific Conditions Precluding Continued Employment (2016) ............................................................ 11
Table 6 – Specific Conditions Temporarily Restricting Employment (2016) ......................................................... 12
Table 7 – Comparison of Quantities in Literature Search Results ........................................................................ 17
Table 8 – Characteristics Associated with Identified Reference ........................................................................... 17
Table 9 – Conclusion: Literature Regarding the Effectiveness of Health Promotion Interventions ....................... 35
Table 10 – Conclusion: Health Status of the Research Population ...................................................................... 36
Table 11 – Conclusion: Health Beliefs and Attitudes ............................................................................................ 37
Table 12 – Conclusion: Organisational Health Promotion ..................................................................................... 38
6
Figures
Figure 1 – Mean BMI of Chilean Adults Compared to Other Global Populations ....................................................9
Figure 2 – Method for Selecting and Including Literature for Review ................................................................... 16
Figure 3 – Conceptual model for integrating health promotion into existing systems ........................................... 20
Figure 4 – Participant Age ..................................................................................................................................... 23
Figure 5 – Duration of Employment with Codelco Andina ..................................................................................... 24
Figure 6 – Level of Supervisor Responsibility ....................................................................................................... 24
Figure 7 – Prevalence of Overweight and Obesity ................................................................................................ 25
Figure 8 – Prevalence of Raised Blood Pressure ................................................................................................. 26
Figure 9 – Elevated Fasting Blood Glucose .......................................................................................................... 26
Figure 10 – Prevalence of Elevated Cholesterol ................................................................................................... 26
Figure 11 – Mean Systolic Blood Pressure ........................................................................................................... 26
Figure 12 – Self-Reported Health Status ............................................................................................................... 27
Figure 13 – Prevenance of Chronic Disease ......................................................................................................... 28
Figure 14 – Difficulty Accomplishing Work Tasks Due to Health .......................................................................... 29
Figure 15 – Psychosocial Work Environment Demands, Support, Security and Use of Skills ............................. 30
Figure 16 – Daily Commute Duration .................................................................................................................... 30
Figure 17 – Job Satisfaction and Intention to Leave ............................................................................................. 31
Figure 18 – Justice and Civil Norms ...................................................................................................................... 32
Figure 19 – Motivation to Adopt Healthier Lifestyles ............................................................................................. 32
Figure 20 – Health Opportunities at Work ............................................................................................................. 33

7
1 INTRODUCTION AND BACKGROUND
The Mutual de Seguridad (The Mutual) in Chile and the University of Wollongong (UOW) partnered to undertake
research to identify health interventions that could improve the health of Chilean mine workers. The outcomes of
the research is described within this report.
1.1 The “Obesogenic” Environment
Economic growth and development have profoundly influenced the “globalisation” of economies, people and
resources, affording once marginalised populations with now attractive benefits including employment, education
and access to health care and other services. Health benefits associated with globalisation have been evidenced
by substantial life expectancy increases across all developing countries, a trend expected to continue in the 21st
century (Baum 2008). However, while global populations have achieved high levels of health and well-being, such
health benefits have been opposed by significant and ever-increasing health inequalities including unhealthy diets,
physical inactivity, tobacco smoking, alcohol consumption and climate change stressors (WHO 2016a).
Of all the above-mentioned inequalities, the impact of urban development on physical activity and diet has been
the most profound as residing, working and playing in now globalised “urban environments” significantly demands
lower energy expenditure as energy intense manual labour becomes replaced by sedentary occupational demands
and leisure activities. Modern global commerce, advanced food production, technology and transportation have
promoted low-cost, energy-dense foods on the domestic food market in many developed and developing countries.
Consumption of high energy food combined with reduced energy expenditure has directly contributed to a global
obesity epidemic (Rydin et al. 2012).
The relationship between globalisation and obesity was first observed in developed countries during the 19th and
20th centuries and by the year 2000, for the first time in human evolution, the number of obese adults surpassed
the number of those who were underweight. Obesity is now considered a global health threat and major risk factor
for chronic diseases including cardiovascular disease, type 2 diabetes and hypertension (WHO 2015).
Multiple factors influence obesity in individuals, including genetic predispositions. However, the speed of obesity
prevalence observed in global populations over the past 30 years indicate social and environmental factors play a
significant role in determining obese population outcomes (Rydin et al. 2012).
1.1.1 Risk of Non-Communicable Disease
Overweight and obesity adversely affect blood pressure, cholesterol, triglycerides and insulin resistance. As an
individual’s body mass index (BMI) increases, so too does their risk of mortality and non-communicable diseases
including coronary heart disease, ischemic stroke and type 2 diabetes mellitus, cancer of the breast, endometrium,
colon, prostate, kidney and gall bladder (WHO 2015). For an adult population to achieve optimum health, the
median BMI should be between 21 to 23 kg/m2, while individuals should maintain a BMI between 18.5 to 24.9
kg/m2. Chronic disease risk increases where an individual’s BMI is greater than 25 kg/m2 and becomes significant
where a BMI of > 30 kg/m2 is realised (WHO 2016a).
1.2 Chilean Population Health
Economic growth and development and unhealthy diet and physical inactivity inequalities have been observed in
Chile (Albala et al. 2002), where the Chilean population over the past three decades has experienced rapid
“nutritional transition”, a term used to characterise the predictable changes in the dietary patterns of a population
associated with economic development and increased wealth (Health 2016). Continued economic growth in the
1990’s resulted in income per capita almost doubling from US$2,600 in 1987 to US$5000 in 1997, of which Vio et

8
al. (2008) report a significant proportion “has been spent on processed foods, rich in fat, sugar and salt, television
sets, appliances and cars” and leading to increases in the prevalence of overweight and obesity so significant that
in 1998 the Chilean Ministry of Health (MOH) prioritised a set of goals to reduce the prevalence of overweight and
obesity in the Chilean population between 2000 and 2010 (Albala et al. 2002).
Regardless of intent, the goals established to reverse the prevalence of obesity have proven difficult to convert
into action, primarily because of physical inactivity and consumption of foods high in fat, sugar and salt (Vio et al.
2008). This combined with weak political decision-making contributes to the increased risk of non-communicable
disease (Vio et al. 2008, Celis-Morales et al. 2016) such as those recorded in 2010 by the MOH and displayed in
Table 1.
Table 1 – Prevalence of Chronic Disease and Risk Behaviours: Chilean Adult Population - 2010
DIAGNOSIS/RISK BEHAVIOUR Women % Men % Total %
Obesity 30.7 19.2 25.1
High blood pressure 25.3 28.7 26.9
Hypercholesterolemia 38.1 39.0 38.5
High/moderate cardiovascular risk 37.3 56.4 45.3
Diabetes 10.4 8.4 9.4
Current smoker 37.1 44.2 40.6
Alcohol consumption in last week 24.8 48.0 36.1
(ILO 2012).
1.2.1 Obesity and the Chilean Adult Population
In Chile, 63% of adults aged over 18 years are estimated to be overweight (BMI ≥ 25 kg/m2) and 28% obese (BMI
≥ 30 kg/m2), such rates associated with increased BMI are consistent with those observed in high-income countries
(WHO 2016a).
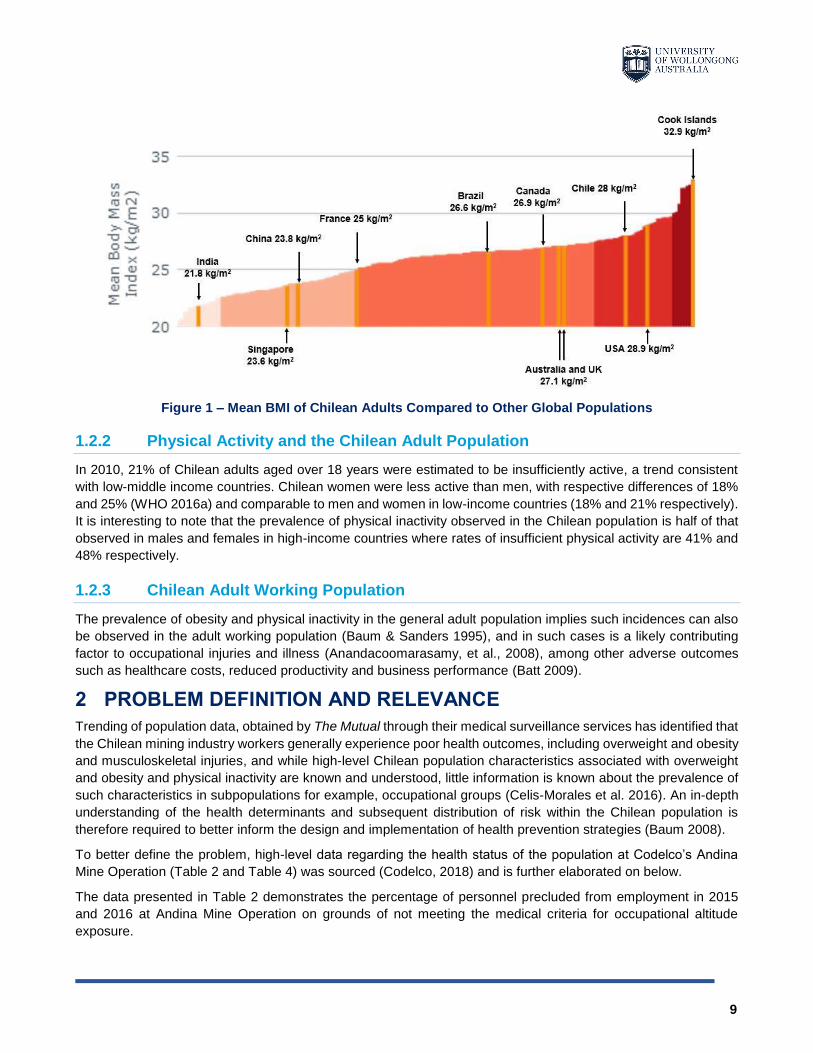
Despite efforts of the Chilean MOH, the mean BMI of the Chilean population increased from in 27.2 kg/m2 in 2010
to 28 kg/m2 in 2016 and when compared to other countries (Figure 1), is rapidly becoming one of the most obese
populations globally (WHO 2016a).
9
Figure 1 – Mean BMI of Chilean Adults Compared to Other Global Populations
1.2.2 Physical Activity and the Chilean Adult Population
In 2010, 21% of Chilean adults aged over 18 years were estimated to be insufficiently active, a trend consistent
with low-middle income countries. Chilean women were less active than men, with respective differences of 18%
and 25% (WHO 2016a) and comparable to men and women in low-income countries (18% and 21% respectively).
It is interesting to note that the prevalence of physical inactivity observed in the Chilean population is half of that
observed in males and females in high-income countries where rates of insufficient physical activity are 41% and
48% respectively.
1.2.3 Chilean Adult Working Population
The prevalence of obesity and physical inactivity in the general adult population implies such incidences can also
be observed in the adult working population (Baum & Sanders 1995), and in such cases is a likely contributing
factor to occupational injuries and illness (Anandacoomarasamy, et al., 2008), among other adverse outcomes
such as healthcare costs, reduced productivity and business performance (Batt 2009).
2 PROBLEM DEFINITION AND RELEVANCE
Trending of population data, obtained by The Mutual through their medical surveillance services has identified that
the Chilean mining industry workers generally experience poor health outcomes, including overweight and obesity
and musculoskeletal injuries, and while high-level Chilean population characteristics associated with overweight
and obesity and physical inactivity are known and understood, little information is known about the prevalence of
such characteristics in subpopulations for example, occupational groups (Celis-Morales et al. 2016). An in-depth
understanding of the health determinants and subsequent distribution of risk within the Chilean population is
therefore required to better inform the design and implementation of health prevention strategies (Baum 2008).
To better define the problem, high-level data regarding the health status of the population at Codelco’s Andina
Mine Operation (Table 2 and Table 4) was sourced (Codelco, 2018) and is further elaborated on below.
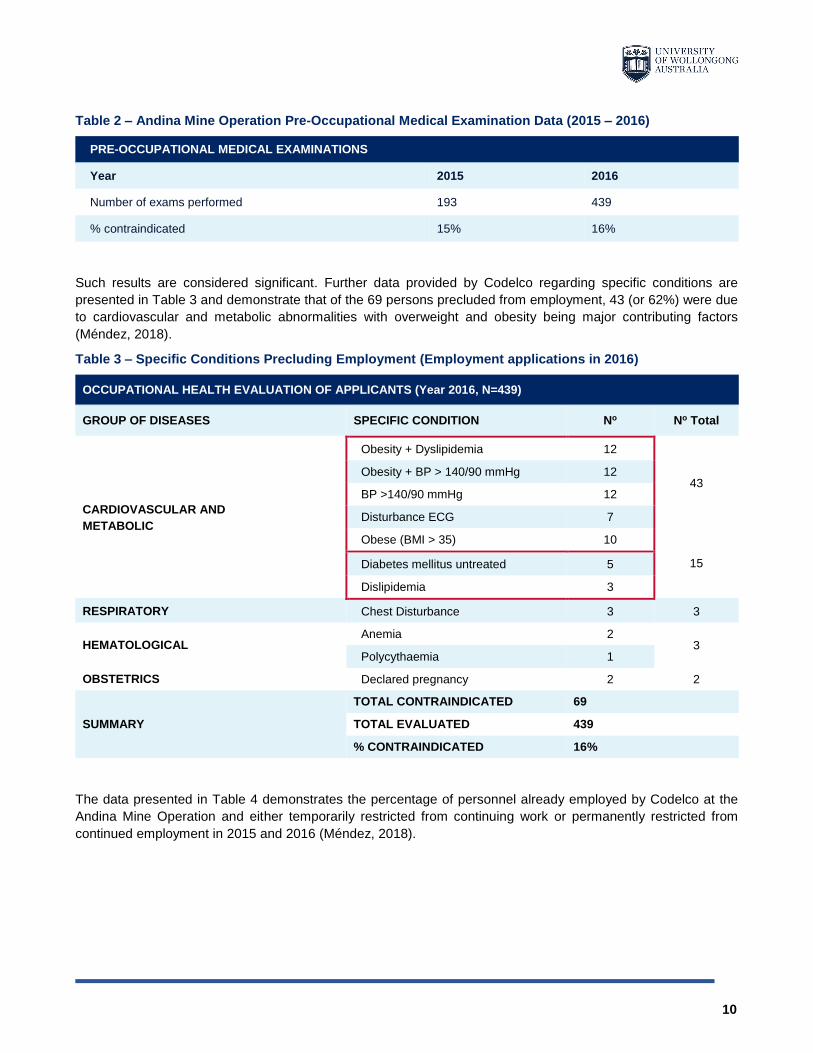
The data presented in Table 2 demonstrates the percentage of personnel precluded from employment in 2015
and 2016 at Andina Mine Operation on grounds of not meeting the medical criteria for occupational altitude
exposure.
10
Table 2 – Andina Mine Operation Pre-Occupational Medical Examination Data (2015 – 2016)
PRE-OCCUPATIONAL MEDICAL EXAMINATIONS
Year 2015 2016
Number of exams performed 193 439
% contraindicated 15% 16%
Such results are considered significant. Further data provided by Codelco regarding specific conditions are
presented in Table 3 and demonstrate that of the 69 persons precluded from employment, 43 (or 62%) were due
to cardiovascular and metabolic abnormalities with overweight and obesity being major contributing factors
(Méndez, 2018).
Table 3 – Specific Conditions Precluding Employment (Employment applications in 2016)
OCCUPATIONAL HEALTH EVALUATION OF APPLICANTS (Year 2016, N=439)
GROUP OF DISEASES SPECIFIC CONDITION No No Total
CARDIOVASCULAR AND
METABOLIC
Obesity + Dyslipidemia 12
43 Obesity + BP > 140/90 mmHg 12
BP >140/90 mmHg 12
Disturbance ECG 7
Obese (BMI > 35) 10
15 Diabetes mellitus untreated 5
Dislipidemia 3
RESPIRATORY Chest Disturbance 3 3
HEMATOLOGICAL Anemia 2
3 Polycythaemia 1
OBSTETRICS Declared pregnancy 2 2
SUMMARY
TOTAL CONTRAINDICATED 69
TOTAL EVALUATED 439
% CONTRAINDICATED 16%
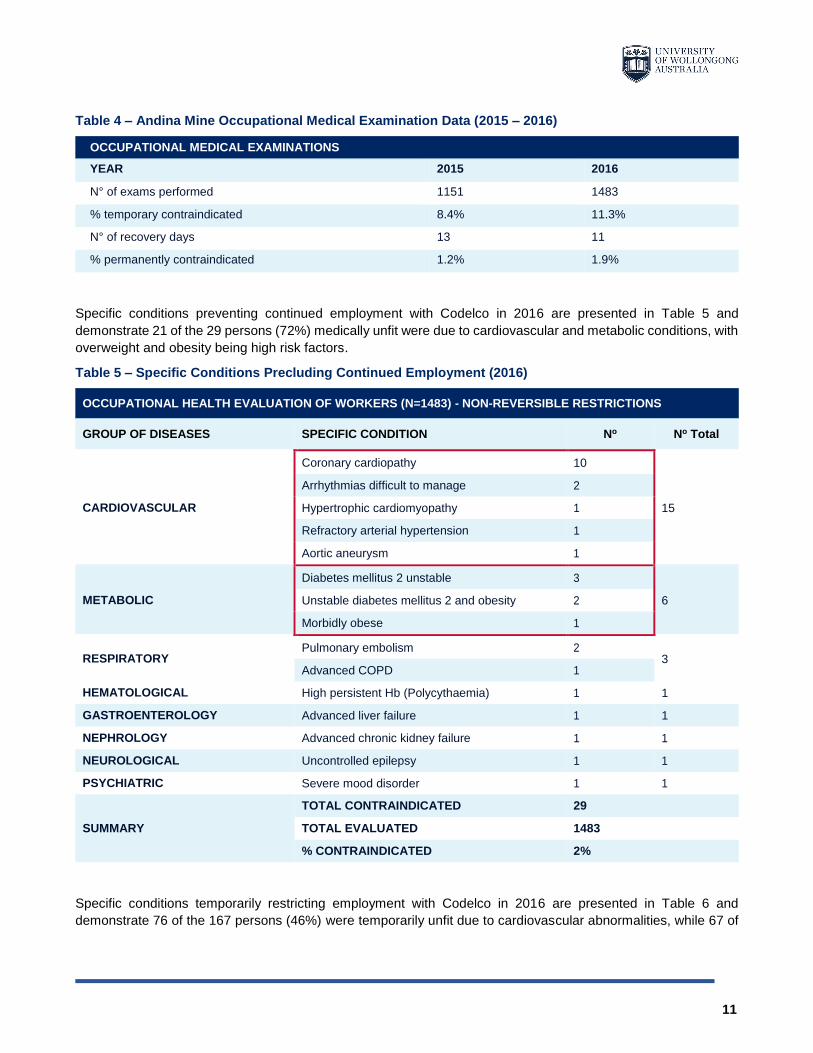
The data presented in Table 4 demonstrates the percentage of personnel already employed by Codelco at the
Andina Mine Operation and either temporarily restricted from continuing work or permanently restricted from
continued employment in 2015 and 2016 (Méndez, 2018).
11
Table 4 – Andina Mine Occupational Medical Examination Data (2015 – 2016)
OCCUPATIONAL MEDICAL EXAMINATIONS
YEAR 2015 2016
N° of exams performed 1151 1483
% temporary contraindicated 8.4% 11.3%
N° of recovery days 13 11
% permanently contraindicated 1.2% 1.9%
Specific conditions preventing continued employment with Codelco in 2016 are presented in Table 5 and
demonstrate 21 of the 29 persons (72%) medically unfit were due to cardiovascular and metabolic conditions, with
overweight and obesity being high risk factors.
Table 5 – Specific Conditions Precluding Continued Employment (2016)
OCCUPATIONAL HEALTH EVALUATION OF WORKERS (N=1483) - NON-REVERSIBLE RESTRICTIONS
GROUP OF DISEASES SPECIFIC CONDITION No No Total
CARDIOVASCULAR
Coronary cardiopathy 10
15
Arrhythmias difficult to manage 2
Hypertrophic cardiomyopathy 1
Refractory arterial hypertension 1
Aortic aneurysm 1
METABOLIC
Diabetes mellitus 2 unstable 3
6 Unstable diabetes mellitus 2 and obesity 2
Morbidly obese 1
RESPIRATORY Pulmonary embolism 2
3 Advanced COPD 1
HEMATOLOGICAL High persistent Hb (Polycythaemia) 1 1
GASTROENTEROLOGY Advanced liver failure 1 1
NEPHROLOGY Advanced chronic kidney failure 1 1
NEUROLOGICAL Uncontrolled epilepsy 1 1
PSYCHIATRIC Severe mood disorder 1 1
SUMMARY
TOTAL CONTRAINDICATED 29
TOTAL EVALUATED 1483
% CONTRAINDICATED 2%
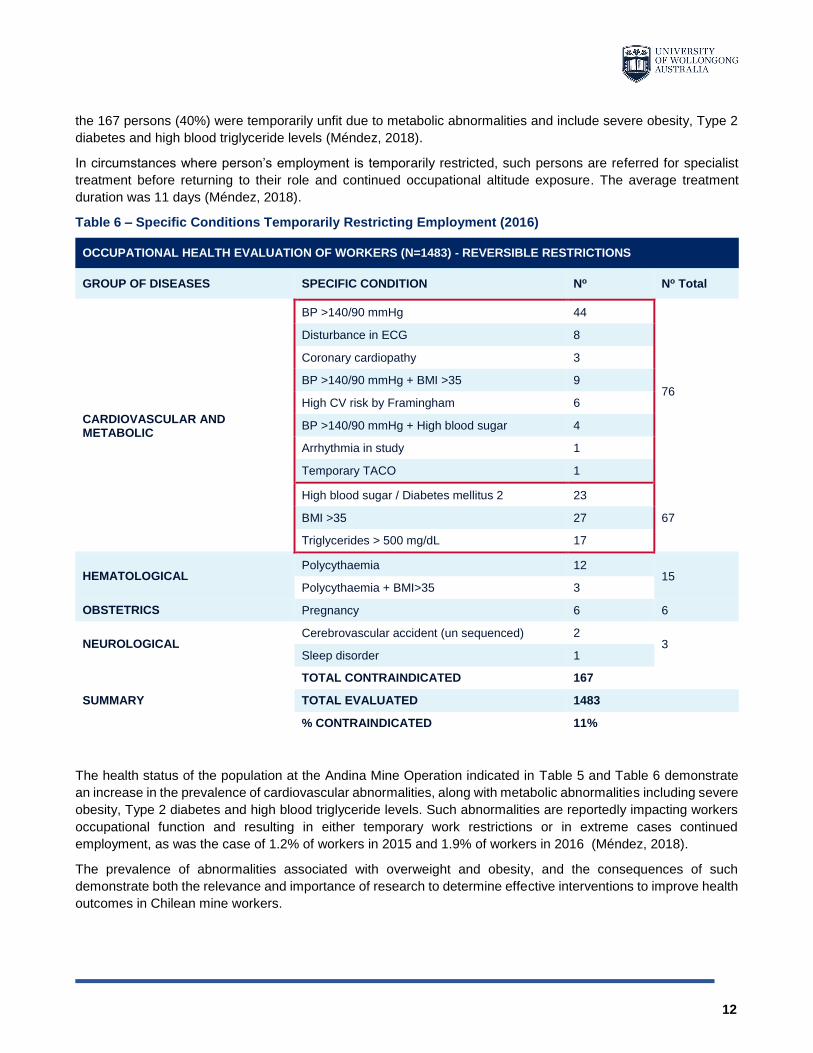
Specific conditions temporarily restricting employment with Codelco in 2016 are presented in Table 6 and
demonstrate 76 of the 167 persons (46%) were temporarily unfit due to cardiovascular abnormalities, while 67 of
12
the 167 persons (40%) were temporarily unfit due to metabolic abnormalities and include severe obesity, Type 2
diabetes and high blood triglyceride levels (Méndez, 2018).
In circumstances where person’s employment is temporarily restricted, such persons are referred for specialist
treatment before returning to their role and continued occupational altitude exposure. The average treatment
duration was 11 days (Méndez, 2018).
Table 6 – Specific Conditions Temporarily Restricting Employment (2016)
OCCUPATIONAL HEALTH EVALUATION OF WORKERS (N=1483) - REVERSIBLE RESTRICTIONS
GROUP OF DISEASES SPECIFIC CONDITION No No Total
CARDIOVASCULAR AND METABOLIC
BP >140/90 mmHg 44
76
Disturbance in ECG 8
Coronary cardiopathy 3
BP >140/90 mmHg + BMI >35 9
High CV risk by Framingham 6
BP >140/90 mmHg + High blood sugar 4
Arrhythmia in study 1
Temporary TACO 1
High blood sugar / Diabetes mellitus 2 23
67 BMI >35 27
Triglycerides > 500 mg/dL 17
HEMATOLOGICAL Polycythaemia 12
15 Polycythaemia + BMI>35 3
OBSTETRICS Pregnancy 6 6
NEUROLOGICAL Cerebrovascular accident (un sequenced) 2
3 Sleep disorder 1
SUMMARY
TOTAL CONTRAINDICATED 167
TOTAL EVALUATED 1483
% CONTRAINDICATED 11%
The health status of the population at the Andina Mine Operation indicated in Table 5 and Table 6 demonstrate
an increase in the prevalence of cardiovascular abnormalities, along with metabolic abnormalities including severe
obesity, Type 2 diabetes and high blood triglyceride levels. Such abnormalities are reportedly impacting workers
occupational function and resulting in either temporary work restrictions or in extreme cases continued
employment, as was the case of 1.2% of workers in 2015 and 1.9% of workers in 2016 (Méndez, 2018).
The prevalence of abnormalities associated with overweight and obesity, and the consequences of such
demonstrate both the relevance and importance of research to determine effective interventions to improve health
outcomes in Chilean mine workers.

13
2.1 Health Promotion Interventions
The Ottawa Charter for Health Promotion and its view on health has been described as the third public health
revolution (Baum 2008, Kickbusch 2007) conceptualising health as a “resource for everyday life, not the object of
living” (WHO 2016b). The Charter, underpinned by a “Health for All” philosophy, facilitated a shift in focus from
factors that cause disease to those that support human health and well-being and subsequently became the driving
force of the “New Public Health” movement. Health Promotion was introduced as a salutogenic approach1 with the
objective of improving the health of populations and involving health sciences, economic, political, cultural and
social sectors of government to guide interventions and reduce systematic, avoidable, and unjust differences in
health between individuals and population sub-groups (Ridde et al. 2007). It proposed a revolutionary shift in
perspective from input to outcomes and governments were to be held accountable for the health of their
populations, not just for the health services they provided (Hancock 2007).
2.1.1 Approaches to Health Prevention
Health systems fundamentally aim to prevent disease and reduce illness such that populations remain as healthy
as possible for as long as possible. Health determinants and subsequent distribution of risk within populations
therefore significantly impact upon the design and implementation of health prevention strategies. Two common
approaches to health prevention have been described and include “Population-Level” strategies, designed to
target and reduce average risk levels in whole populations, regardless of exposure to risk factors or not, and “High-
Risk” strategies, designed to target identified high-risk individuals within a population (Ridde et al. 2007). Both
strategies offer unique advantages and disadvantages and are further discussed below.
2.1.1.1 Population Level Interventions
‘Population level’ strategies are those interventions which specifically target health determinants to improve overall
health by shifting the distribution of risk factors rather than preventing specific diseases. Such interventions
typically take the form of laws and regulations, tax and price interventions, built environment improvements,
awareness campaigns and community-based interventions. At times such interventions may be deployed in
parallel, for example, the implementation of a community-based intervention to improve the built environment and
the corresponding introduction of laws that mandate taxation on health-harming products. While such strategies
intend to reduce exposures and create healthy behaviours into social norms such that the entire population risk is
lowered, they are often difficult to implement as such interventions require collaboration between a number of
societal sectors, each of which often oppose the interests of one another (Ridde et al. 2007).
The advantage of population-level interventions includes addressing the root causes of illnesses to reduce the
incidence and modify the whole population risk profile, including those at low or average risk. Potential gains at a
population level are extensive, however, are often opposed, as preventive measures that afford significant
population change will only appear to offer little benefit to each participating individual, subsequently unfavourably
affecting population motivation at large (Hunt & Emslie 2001). This observable disadvantage was first described
in 1981 as the "prevention paradox" by epidemiologist Geoffrey Rose, characterised as one of the most
fundamental axioms now used in preventive medicine, that is, "a large number of people exposed to a small risk
may generate many more cases than a small number exposed to high risk" (Rose 2001). Rose indicated wherever
this axiom applies, preventive strategies focusing on high-risk individuals will marginally address the issue and
1 Salutogenic Approach – A medical approach to health promotion that focuses on factors that support human health and wellbeing, rather than focusing on factors that cause disease.
14
subsequently will not impact the large numbers of disease occurring in the moderate risk population (Hunt & Emslie
2001).
Population-level health interventions observed historically in developed countries include well known tobacco
control interventions, now in place for over two decades and include multi-faceted interventions combining tobacco
control laws, regulating businesses to provide smoke-free environments, controlling sales, enforcing restrictions
on advertising including graphic warning labels and sales tax on tobacco products (Wakefield et al. 2014).
Evaluation of interventions on smoking prevalence among adults between 2001 and 2011 demonstrated increased
tobacco taxes, toughened smoke-free laws, increased exposure to tobacco control mass media campaigns and
pharmaceutical company advertising for nicotine replacement therapy contributed to a reduction in smoking
prevalence from 23.6% to 17.3% with stronger smoke-free laws, increased tobacco taxation and greater exposure
to mass media campaigns independently contributing to 76% of the decrease in smoking prevalence (Wakefield
et al. 2014).
Not all population prevention initiatives demonstrate such success, particularly those that rely on mass social
marketing as the only method of intervention (Grunseit et al. 2015; King et al. 2013). Examples of such include the
'Life be in it' and ‘Swap it, don’t drop it’ lifestyle campaigns implemented in Australia in 1977 and 2011 respectively.
Such campaign initiatives, focused on the personal exercise and eating behaviours of individuals, and although
they were inherently plausible at an individual level, such interventions failed to consider the broader social and
environmental contexts in which personal behaviours are embedded (Baum 2011, Christakis & Fowler 2007).
The fact that obesity prevalence is increasing globally, demonstrates interventions that rely on telling people to
change their lifestyles and to be healthier have a limited impact on population health, and if anything act to increase
inequities (Baum 2011, Grunseit et al. 2015, King et al. 2013).
2.1.1.2 High-Risk Interventions
The ‘high-risk’ approach to health prevention inherently relies on the assistance of medical professionals to identify
those persons with risk factors or medical conditions and prescribe interventions that aim to prevent disease
development within the individual.
The advantage of high-risk approaches is interventions are specific to the target individual. Therefore, individuals
are more likely to be motivated and intervention compliant, such advantage is also disadvantageous as treating
individuals results in little impact on the population disease burden as most cases of disease occur in low or
moderate risk people and therefore predicting new cases is difficult (Hunt & Emslie 2001).
High-risk population interventions often promote an over-reliance on the medical health model which consequently
distracts the attention of policy makers away from crucial longer-term adjustments to social and economic policy
(Kickbusch 2015). Baum and Sanders (1995) provide interesting discussion regarding the political advantage of
such, offered historically to those in power, as such circumstances provided maintenance of the status quo. As
previously discussed, chronic disease has replaced infectious disease as the main cause of mortality and
morbidity, this combined with population growth and global population movement mean that the medical health
model, currently relied upon is no longer economically sustainable (Ridde et al. 2007).
Vartiainen et al. (2011) compared the effectiveness of both population and high-risk strategies for cardiovascular
disease (CVD) outcomes in rural Australians between 2004 to 2006, including modelling the effect of changing
risk factors at a population level, among the high-risk individuals, and both to assess the extent of interventions
on CVD prevention.
Results demonstrated the high-risk strategy could reduce cardiovascular events by 12.6% (126 per 1000), the
population strategy by 19.3% (193 per 1000 per 5 years) and when both strategies were combined, a 24.1%
reduction in cardiovascular events (241 per 1000) could be achieved (Vartiainen et al. 2011).
15
The results of the study demonstrate the advantages of treating high-risk individuals to reduce the mean risk-factor
levels in the population, however, also highlight the greater impact overall when high-risk and population strategies
are combined (Vartiainen et al. 2011).
A fundamental aim of any health intervention is to prevent disease and reduce ill health and in practice, as indicated
in the Ottawa Charter, requires preventative health strategies that target different levels, individuals, communities,
and populations simultaneously (WHO 2016b).
2.1.2 Health Promotion in the Occupational Environment
As previously discussed, the Ottawa Charter for Health Promotion is the foundation reference for health promotion
and is considered the strategic framework of the new public health movement to reduce inequalities in health
globally (Labonté 2011). The Charter is founded on the principle that health is created by people within the settings
of their everyday lives, that is, where they live, work and play (WHO 2016b). As such, the workplace has been
recognised by the World Health Organisation (WHO) (2016c) as a setting which significantly “influences the
“physical, mental, economic and social well-being of workers and in turn the health of their families, communities
and society” and therefore has been prioritised as a setting for health promotion.
One such appropriate workplace setting is mining operations, typically established in regional and remote locations
and requiring workers to reside “on-site” for extended periods of time to work and service mining operation
activities. In such environments, food is provided to the workers from an onsite kitchen and such may influence
eating behaviours resulting in over consumption of energy dense nutrient poor food and leading to overweight and
obesity. In Australia, 76% of workers in the mining industry are classified as overweight or obese, the highest
among all national industries (ABS 2008). Such observable patterns may be comparable or even higher in Chile.
However, data to inform such assumptions is currently lacking.
Over the past two decades a framework and associated body of knowledge has emerged that aims to
systematically integrate health promotion in the workplace with traditional occupational health and safety programs
designed to protect workers (NIOSH 2008) and have been founded on the theory that interventions which target
both the workers knowledge and skills, and create a supportive environment for health are more likely to be
successful and sustainable (Seabury et al. 2005). In 2011, the framework and supporting theoretical knowledge
was given the term Total Worker Health® (TWH) by the National Institute of Occupational Safety and Health
(NIOSH) for purposes of expanding dialogue between researchers, practitioners, business leaders and organised
labour representatives such that traditional occupational safety and health programs could be expanded to include
wellness and well-being (Sorensen et al. 2016a). The thoretical framework supporting TWH interventions is futher
discussed and elaborated upon in the literature review Discussion Section.
3 LITERATURE REVIEW
A systematic literature review was conducted with the objective of identifying and evaluating evidence supporting
the effectiveness of interventions conducted in the occupational environment which improves worker’s nutrition
and physical activity-related behaviours and supports the identification of future research on improving wellbeing
and decreasing musculoskeletal injuries in Chilean mine workers.
3.1 Method
A literature seach strategy was applied to identify peer-reviewed literature published between 2000 and 2018 in
multiple databases. Literature was eligible for inclusion if the study pertained to a workplace setting and specifically
measured the effectiveness of interventions implemented for purposes of improving workers diet and physical
activity related outcomes.
16
3.2 Results
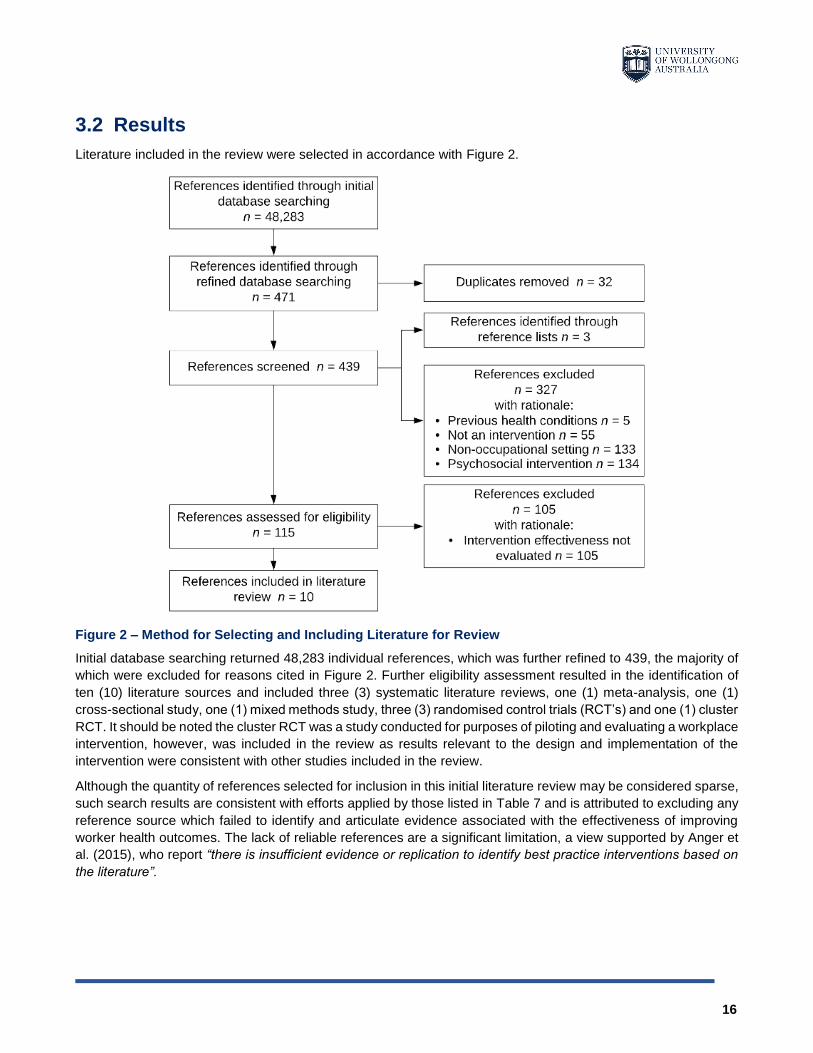
Literature included in the review were selected in accordance with Figure 2.
Figure 2 – Method for Selecting and Including Literature for Review
Initial database searching returned 48,283 individual references, which was further refined to 439, the majority of
which were excluded for reasons cited in Figure 2. Further eligibility assessment resulted in the identification of
ten (10) literature sources and included three (3) systematic literature reviews, one (1) meta-analysis, one (1)
cross-sectional study, one (1) mixed methods study, three (3) randomised control trials (RCT’s) and one (1) cluster
RCT. It should be noted the cluster RCT was a study conducted for purposes of piloting and evaluating a workplace
intervention, however, was included in the review as results relevant to the design and implementation of the
intervention were consistent with other studies included in the review.
Although the quantity of references selected for inclusion in this initial literature review may be considered sparse,
such search results are consistent with efforts applied by those listed in Table 7 and is attributed to excluding any
reference source which failed to identify and articulate evidence associated with the effectiveness of improving
worker health outcomes. The lack of reliable references are a significant limitation, a view supported by Anger et
al. (2015), who report “there is insufficient evidence or replication to identify best practice interventions based on
the literature”.
17
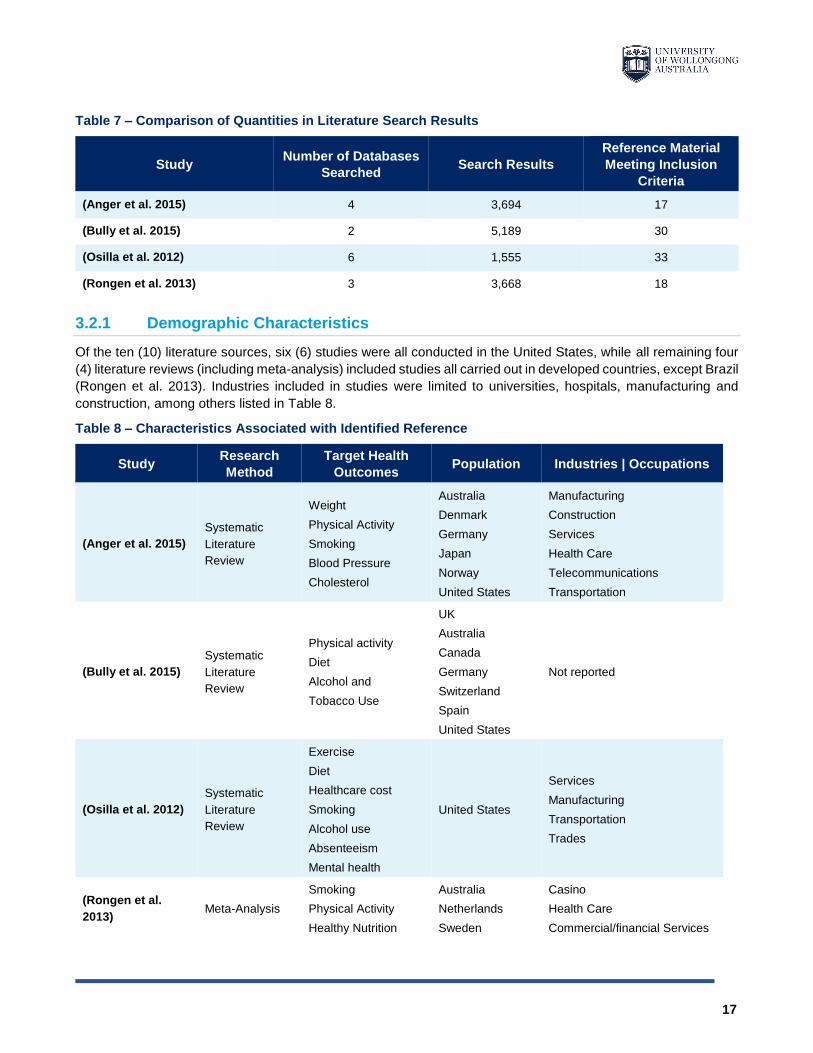
Table 7 – Comparison of Quantities in Literature Search Results
Study Number of Databases
Searched Search Results
Reference Material
Meeting Inclusion
Criteria
(Anger et al. 2015) 4 3,694 17
(Bully et al. 2015) 2 5,189 30
(Osilla et al. 2012) 6 1,555 33
(Rongen et al. 2013) 3 3,668 18
3.2.1 Demographic Characteristics
Of the ten (10) literature sources, six (6) studies were all conducted in the United States, while all remaining four
(4) literature reviews (including meta-analysis) included studies all carried out in developed countries, except Brazil
(Rongen et al. 2013). Industries included in studies were limited to universities, hospitals, manufacturing and
construction, among others listed in Table 8.
Table 8 – Characteristics Associated with Identified Reference
Study Research
Method
Target Health
Outcomes Population Industries | Occupations
(Anger et al. 2015)
Systematic
Literature
Review
Weight
Physical Activity
Smoking
Blood Pressure
Cholesterol
Australia
Denmark
Germany
Japan
Norway
United States
Manufacturing
Construction
Services
Health Care
Telecommunications
Transportation
(Bully et al. 2015)
Systematic
Literature
Review
Physical activity
Diet
Alcohol and
Tobacco Use
UK
Australia
Canada
Germany
Switzerland
Spain
United States
Not reported
(Osilla et al. 2012)
Systematic
Literature
Review
Exercise
Diet
Healthcare cost
Smoking
Alcohol use
Absenteeism
Mental health
United States
Services
Manufacturing
Transportation
Trades
(Rongen et al.
2013) Meta-Analysis
Smoking
Physical Activity
Healthy Nutrition
Australia
Netherlands
Sweden
Casino
Health Care
Commercial/financial Services
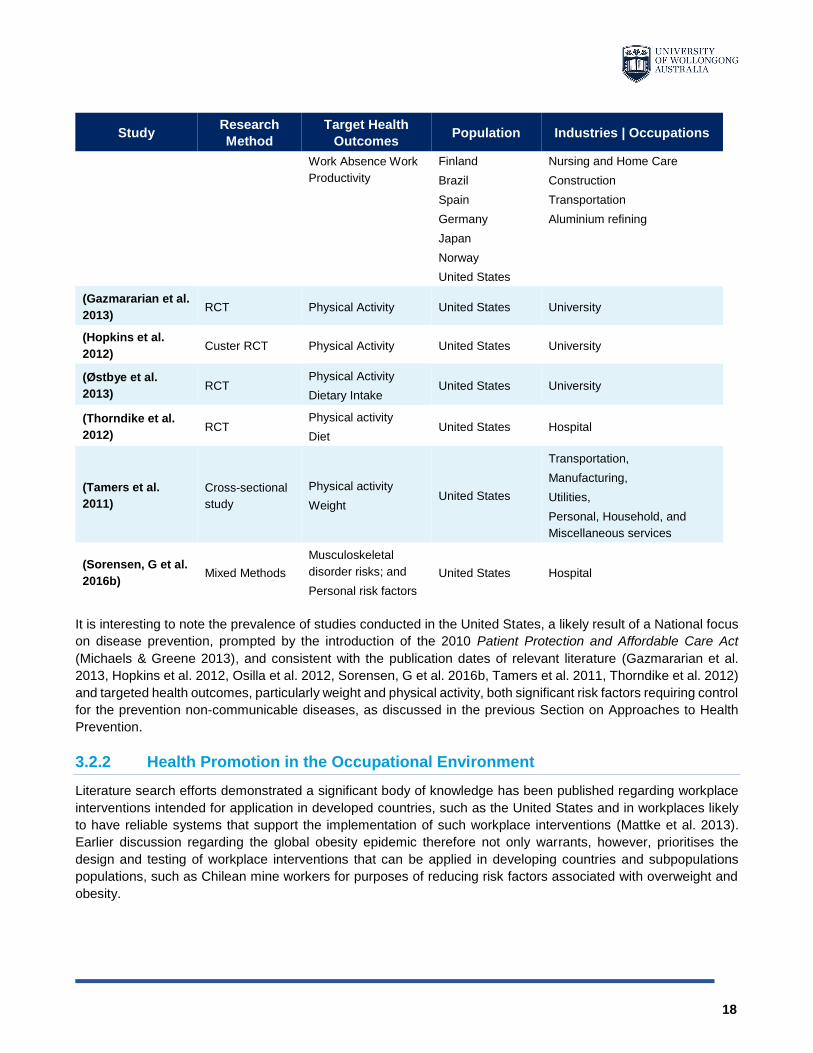
18
Study Research
Method
Target Health
Outcomes Population Industries | Occupations
Work Absence Work
Productivity
Finland
Brazil
Spain
Germany
Japan
Norway
United States
Nursing and Home Care
Construction
Transportation
Aluminium refining
(Gazmararian et al.
2013) RCT Physical Activity United States University
(Hopkins et al.
2012) Custer RCT Physical Activity United States University
(Østbye et al.
2013) RCT
Physical Activity
Dietary Intake United States University
(Thorndike et al.
2012) RCT
Physical activity
Diet United States Hospital
(Tamers et al.
2011)
Cross-sectional
study
Physical activity
Weight United States
Transportation,
Manufacturing,
Utilities,
Personal, Household, and
Miscellaneous services
(Sorensen, G et al.
2016b) Mixed Methods
Musculoskeletal
disorder risks; and
Personal risk factors
United States Hospital
It is interesting to note the prevalence of studies conducted in the United States, a likely result of a National focus
on disease prevention, prompted by the introduction of the 2010 Patient Protection and Affordable Care Act
(Michaels & Greene 2013), and consistent with the publication dates of relevant literature (Gazmararian et al.
2013, Hopkins et al. 2012, Osilla et al. 2012, Sorensen, G et al. 2016b, Tamers et al. 2011, Thorndike et al. 2012)
and targeted health outcomes, particularly weight and physical activity, both significant risk factors requiring control
for the prevention non-communicable diseases, as discussed in the previous Section on Approaches to Health
Prevention.
3.2.2 Health Promotion in the Occupational Environment
Literature search efforts demonstrated a significant body of knowledge has been published regarding workplace
interventions intended for application in developed countries, such as the United States and in workplaces likely
to have reliable systems that support the implementation of such workplace interventions (Mattke et al. 2013).
Earlier discussion regarding the global obesity epidemic therefore not only warrants, however, prioritises the
design and testing of workplace interventions that can be applied in developing countries and subpopulations
populations, such as Chilean mine workers for purposes of reducing risk factors associated with overweight and
obesity.

19
Studies relevant to the effectiveness of health promotion interventions implemented in the mining industry were
not identified in any of the sources, nor were studies relevant to the Chilean working population, therefore
reinforcing the priority for research efforts.
The abundance of reference material has been surmised by Mattke et al. (2012), who reports many employers
provide anecdotal evidence and express support and for workplace wellness programs, particularly with regards
to improvements in worker health and reductions in healthcare costs. Statements which have been further
supported by independent literature review (Mattke et al. 2013) demonstrating evidence of positive effects on diet
and exercise, smoking and alcohol use and health care costs, however, limited evidence of effects on absenteeism
and mental health. It is important to note however, that such findings were not conclusive as positive correlations
associated with intervention intensity are likely to contribute to reported outcomes.
Mattke et al. (2012) conclude that the strength of such evidence is currently insufficient to conclusively assess the
impact of workplace health interventions on worker health outcomes. The abundance of peer-reviewed literature
reports mostly positive outcomes, however, such literature only encompasses a minor proportion of the abundance
of interventions, and therefore prompts questions with regards to the generalisability of reported findings,
particularly in developing countries and in subpopulations.
As such, research is needed to evaluate the impact of workplace health interventions in “real world” settings such
that policymakers are informed when making decisions and improved health outcomes are achieved.
One such research method is supported by a “Total Worker Health” framework, which when applied, establishes
to integrate policies, programs, and practices within the workplace that focus on health and safety activities that
advance the overall well-being of individual workers, their families, communities, employers and the economy as
a whole (Sorensen et al. 2016a).
3.3 Discussion
For people to remain as healthy as possible for as long as possible, health prevention strategies comprising both
“Population-Level” and “High-Risk” strategies, described previously are necessary and are important to ensure
efforts are effective and support sustained positive behaviour change (Hunt & Emslie, 2001). Such approaches
when implemented are complementary, however, require considerable balance. Finding that balance is the
challenge as described by Rose (2001) and requires oversight of disease, its causes and solutions, ultimately
leading to the acknowledgement and development of strategies that address the broader social and environmental
determinants of disease.
Literature review activities identified the Total Worker Health® framework as one specific strategy that can be
applied in the occupational environment to improve worker’s nutrition and physical activity-related behaviours while
supporting improved wellbeing and decreasing musculoskeletal injuries in Chilean mine workers. Such is further
discussed below.
3.3.1 Theoretical Framework for Health Promotion Interventions
In 2011, the Total Worker Health® (TWH) framework was termed by NIOSH to expand the dialogue between
researchers, practitioners, business leaders and organised labour representatives for purposes of expanding the
theoretical knowledge that supports the integration of health promotion interventions into traditional occupational
safety and health programs (Sorensen et al. 2016a).
Sorensen et al. (2016a) most recently published a conceptual model (Figure 3) with the intention of guiding social
epidemiological research on the determinants of worker health and safety for purposes of informing the design,
implementation and evaluation of strategies that promote and protect worker health. The conceptual model

20
embeds multiple theories, enhances NIOSH’s TWH framework and contributes to the growing body of knowledge
and associated evidence demonstrating the benefit of integrated interventions on health behaviours.
The model, represented in Figure 3, was developed by the Centre for Work, Health and Well-being at the Harvard
School of Public Health, and is founded on the premise that policies, programs and practices designed to address
multiple pathways within the work environment in an integrated manner, will result in improved health outcomes
far greater than that what would be expected if each pathway was addressed individually, as such Sorensen et al.
(2016a) report the model is expected to “provide a valuable tool for future research aimed at testing the
effectiveness of integrated approaches to worker health protection and health promotion, as well as a framework
for translating research to practice”.
Figure 3 – Conceptual model for integrating health promotion into existing systems
Figure 3 pictorially demonstrates each model component and the many pathways through which policies,
programs and practices concurrently operate and affect the conditions of work. As such, the physical work
environment and organisation of work, along with mediating effects on health behaviours are central to the model
as determinants of health and safety outcomes. The model demonstrates the relationship of such work conditions,
along with the potential influence of business and workforce characteristics and where policies, programs and
practices may contribute to improvements in business performance such as turnover and workers’ compensation
and health care costs. It is fundamental to recognise however, that such relationships occur within the context of
labour market and economic trends, legal and political forces, and most importantly within the context of social
norms and cultural influences (Sorensen et al. 2016a).
It is important to note that although the model is conceptual, it has been structured by applying multiple theoretical
frameworks including the social-ecological model, social contextual model of health behaviour change, hierarchy
of controls, organisational ergonomics, community-based participatory research framework, job strain and
sociotechnical systems theory. Such diverse theoretical foundations demonstrate the complex interaction of
factors between individual workers and their immediate work environment and the characteristics associated with
the broader context in which both the worker and the worksite are embedded. Understanding and designing health
interventions that take into consideration the broader context in which health behaviours occur are more likely to
be successful and sustainable as such interventions will be implemented to address pathways across multiple
dimensions (Sorensen et al. 2016a).
As such, the model affords both research and practice a systematic approach to identifying the causal pathways
through which work influences health outcomes, and in particular, designing and testing interventions that are
responsive to workplace conditions that are meaningful for workers and employers and are successful in improving
health behaviours (Sorensen et al. 2016a).
21
4 METHODOLOGY
4.1 Participant Recruitment
Participant recruitment and data collection activities took place at Clinica Rio Blanco’s Occupational Health Unit in
Los Andes, Chile. Clinica Rio Blanco are contracted by Codelco Andina to provide occupational health services
including pre-employment evaluations and periodic medical surveillance for those employed by Codelco’s Andina
Division.
All Andina employees attending the clinic to participate in periodic health evaluation activities were invited to
participate in the study, a total of 242 persons were recruited between September 30, 2019 and February 28,
2020.
4.2 Data Collection
Data collection activities included the administration and analysis of 242 questionnaires and 40 face-to-face
interviews were performed to gain an understanding of the extent of overweight, obesity and physical activity in
the study population and contextualise the social, environmental and cultural variables that influence such health
outcomes (Ivankova et al. 2006)
In addition to the above, de-identified group medical surveillance data was also examined for purposes of
comparing non-communicable disease risk factors in the study population with the Chilean adult population.
Translation and Adaptation of Research Instruments
The forward-translation and back-translation method (WHO, 2020) was followed to translate and adapt the All
Employee Survey (CPH-NEW 2014) and interview questions such that both instruments were culturally and
conceptually equivalent in Chile, this method included:
1. Forward Translation of the instruments from English into Spanish;
2. Review of the translated instruments, specifically the words, intent of questions and concepts to ensure
inadequate expressions and concepts were identified and resolved;
3. Back Translation of the instruments from Spanish into English, specifically limited to terms and concepts
that were considered fundamental to the instrument and those that were identified as sensitive to cross
cultural translation; and
4. Pre-Testing of the each modified instrument with a sample of the target population.
4.2.1 Questionnaire
Questionnaires were self-administered by all study participants (n = 242) whilst they waited to participate in
scheduled medical evaluations at Clinica Rio Blanco.
The questionnaire was a modified version of the Healthy Workplace All Employee Survey developed by
researchers at the Center for the Promotion of Health in the New England Workplace (CPH-NEW 2014).
The questionnaire was deployed for purposes of assessing worker attitudes in relation to their physical and
psychosocial work environment, including factors that support or reduce a healthy worksite culture, in addition to
capturing the participant’s perceived health and associated health behaviours.
22
4.2.2 Interviews
Semi-structured face-to-face interviews were conducted with 40 participants, already recruited into the study. The
interviews were conducted for exploratory purposes and followed a standardised set of questions designed to
identify themes and trends in participants lived experiences, beliefs and values.
The face-to-face interviews were administered by a Chilean national member of the research team, with audio
recordings of each interview. Each audio recording was transcribed into written text (Spanish). Following
transcription, the participants were provided with the opportunity to review their transcript for accuracy and
completeness through the Chilean research team member. Following revision, each transcript was translated from
Spanish into English by a Chilean professional translator for purposes of analysis and interpretation.
4.2.3 Group Medical Surveillance Data
Chilean legislation introduced in 2012, requires all persons occupationally exposed to high altitude (> 3000 m) to
participate in annual medical surveillance. The altitude of Codelco’s Andina Operation is between 3200 m and
4500 m and therefore medical assessment is performed by Codelco on every person working at the mine annually.
De-identified group data collected during 2018 on approximately 1622 full-time employees was provided by
Codelco to UOW in Microsoft Excel format and included parameters pertaining to the following non-communicable
disease risk factors:
Overweight and obesity;
Blood pressure;
Blood glucose; and
Cholesterol.
For purposes of comparison, Codelco group population data for each of the above parameters was compared to
the corresponding Chilean adult population data, maintained by the World Health Organisation (WHO 2008, WHO
2014, WHO 2015b, WHO 2015c, WHO 2016c).
5 RESULTS
Analysis of 242 questionnaires and 40 face-to-face interviews was performed to gain an understanding of the
extent of overweight, obesity and physical activity in the study population and contextualise the social,
environmental and cultural variables that influence such health outcomes (Ivankova et al. 2006).
De-identified group medical surveillance data was reviewed to compare non-communicable disease risk factors in
the study population with the Chilean adult population (WHO 2016d). The results of such comparison were used
to support identified themes relevant to the research and determine suitable interventions or recommendations to
support improved health outcomes in Chilean mine workers.
This results section has been structured to provide the reader with an understanding of the following key themes
from the analysis:
Research population health status;
Participants perception of own health status;
The value placed on health;
Personal health and impact of family life and employment; and
Workplace health promotion programs.
The terms used in this section of the report are:

23
Research Participant – A person recruited into this study and who participated in the questionnaire (n =
242);
Interview Participant – A person recruited into this study and who participated in a face to face interview
(n = 40); and
Study Population – A person employed by Codelco Andina and participated in an occupational medical
examination in 2018 (n = 1622).
5.1 Study Population
A total of 242 persons were recruited into the study. Participant ages ranged between 24 years and 69 years with
a mean age of 45 years (Figure 4).
Figure 4 – Participant Age
The duration of participant employment with Codelco Andina ranged between 1 year and 49 years with a mean of
16 years (Figure 5).
0%
10%
20%
32%
29%
8%
< 20 >20 <30 >30 <40 >40 <50 >50 <60 > 60
PARTI C I PANT AG E D I STRI BUTION ( YEARS)

24
Figure 5 – Duration of Employment with Codelco Andina
The majority of participants (64%) had no supervisory responsibilities. The remaining 36% were responsible for
the supervision of others at Codelco Andina with the majority being Team Leaders (Figure 6).
Figure 6 – Level of Supervisor Responsibility
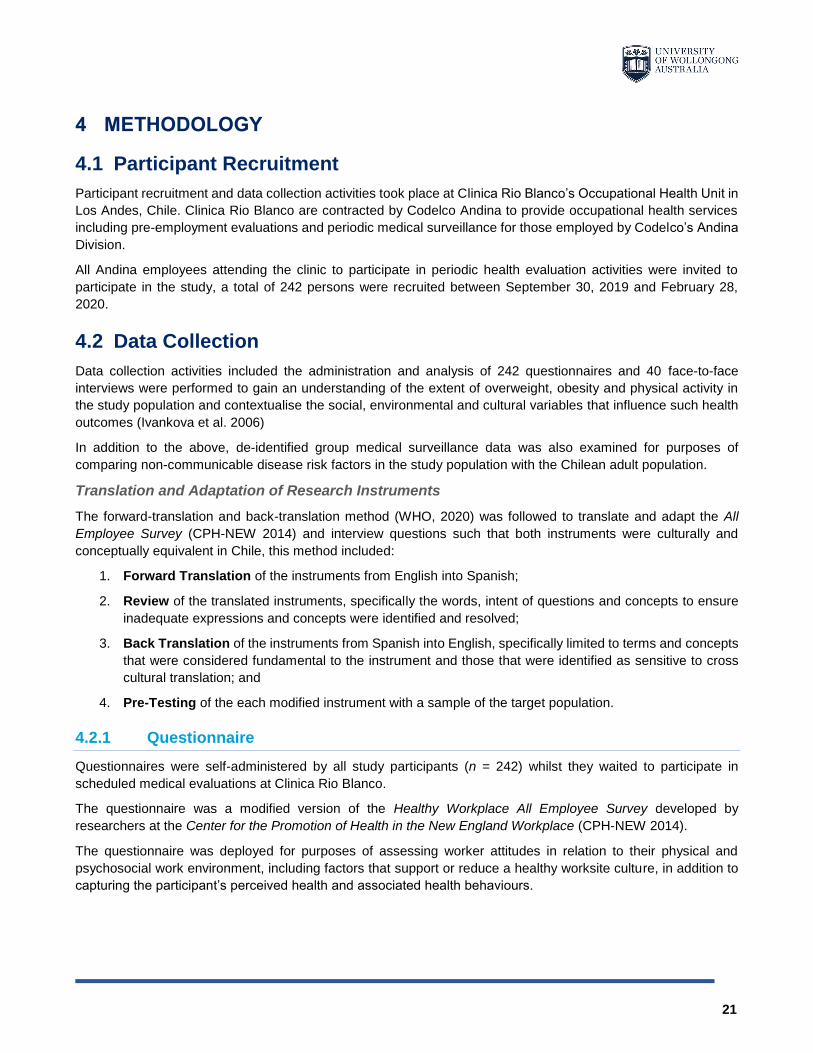
5.2 Research Population Health Status
The mean BMI of Codelco’s Andina population is 27.8 kg/m2 with 80.6% of employees classified as overweight or
obese. Such results are commensurate with the mean BMI (28 kg/m2) of the general Chilean adult population.
Further examination of both Andina and Chilean Adult population data (Figure 7), in particular the percentage
distribution of each population in each BMI category suggests the prevalence of overweight and obesity in
Codelco’s Andina population is less than that observed in the general Chilean adult population, with the exception
of those classified with a "Normal” BMI.
11%
25%
21%
3%
21%
17%
2%
<5 >5 < 10 >10 <15 >15 <20 >20 <30 > 30 > 40
DURATI O N O F EM PLOYMENT ( YEARS)
64%
18%13%
4%0%
No supervisoryresponsibility
Team Leader Supervisor Manager Execuitive
PO SI T ION I N O RG ANI SATI O N
25
Figure 7 – Prevalence of Overweight and Obesity
(WHO 2016a)
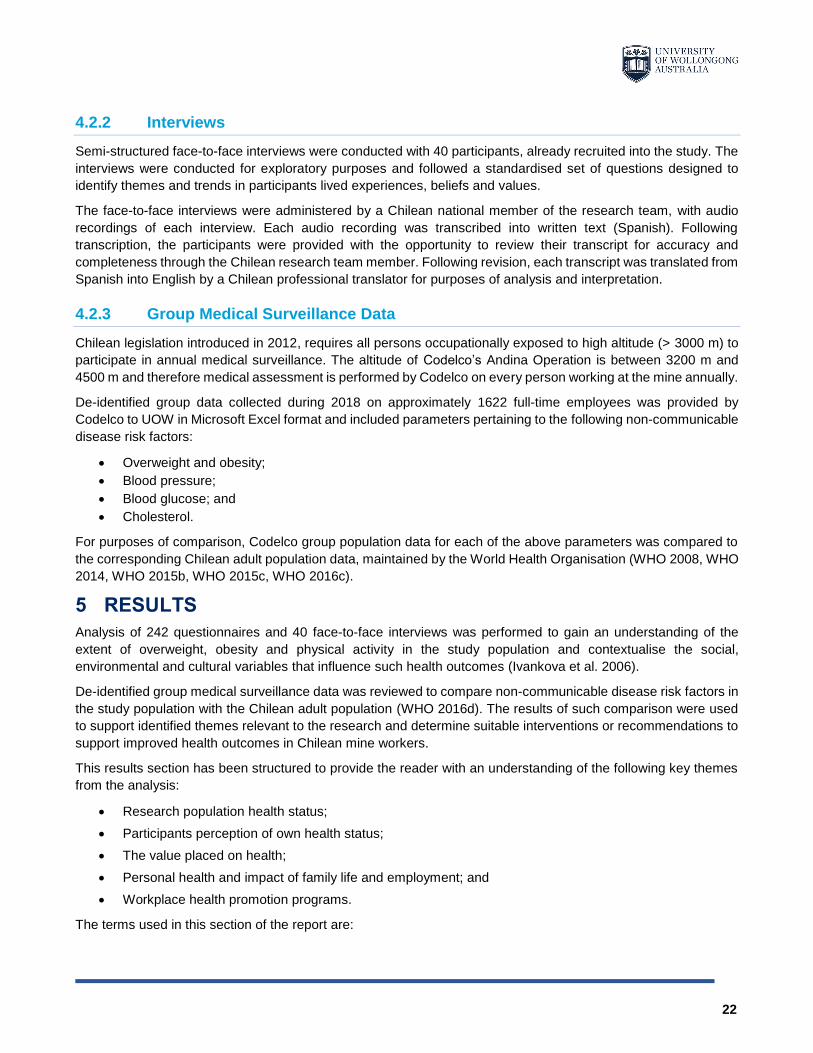
Other non-communicable disease risk factors in Codelco’s Andina population were compared to the general
Chilean adult population including blood pressure, fasting blood glucose and total cholesterol.
Comparison of all parameters indicated Codelco’s Andina population had a reduced prevalence of elevated blood
pressure (Figure 8), elevated fasting glucose (Figure 9) and elevated cholesterol (Figure 10) when compared to
the general Chilean adult population. Additionally, the mean systolic blood pressure in Codelco’s Andina
population (116 mmHg) is lower than the general Chilean adult population (124 mmHg) (Figure 11).
0.70%8.20%
63.1%
28.0%
0.6%
18.90%
56.2%
24.4%
U N D E R W EI G H T( B MI < 1 8 )
N O R MA L( B MI 1 8 - 2 4 . 9 )
O V E R W EI G H T ( B MI ≥ 2 5 )
O B E S E ( B MI ≥ 3 0 )
PO
PU
LA
TIO
N P
RE
VE
LA
NC
E (
%)
PREVALENCE OF OVERWEIGHT AND OBESITY
Chilean Population Codelco Andina
26
Figure 8 – Prevalence of Raised Blood Pressure
(WHO 2015c)
Figure 9 – Elevated Fasting Blood Glucose
(WHO 2014)
Figure 10 – Prevalence of Elevated Cholesterol
(WHO 2008)
Figure 11 – Mean Systolic Blood Pressure
(WHO 2015b)
20.9
%
4.9
%
R AI S E D B P ( S B P ≥ 1 4 0 O R D B P ≥ 9 0 )
PO
PU
LA
TIO
N P
RE
VE
LA
NC
E (
%)
PREVALENCE OF RAISED BLOOD PRESSURE
(SYSTOLIC AND DIASTOLIC)
Chilean Population Codelco Andina
10.5
%
2.8
%
E L E V ATE D F AS TI N G B L O O D G L U C O S E ( ≥ 1 2 6 M G / D L )
PO
PU
LA
TIO
NP
RE
VE
LA
NC
E(%
)
ELEVATED FASTING BLOOD GLUCOSE
Chilean Population Codelco Andina
48.6
%
12.9
0%2
8.3
%
3.1
%
E L E V ATE D TO TAL C H O L E S TE R O L ( ≥ 5 . 0 M M O L /L )
E L E V ATE D TO TAL C H O L E S TE R O L ( ≥ 6 . 2 M M O L /L )
PO
PU
LA
TIO
N P
RE
VE
LA
NC
E (
%)
PREVALENCE OF ELEVATED TOTAL CHOLESTEROL
Chilean Population Codelco Andina
124 m
mH
g
116 m
mH
g
M E AN S YS TO L I C B P ( M M H G )
MEAN SYSTOLIC BLOOD PRESSURE
Chilean Population Codelco Andina
27
5.3 Perceived Health
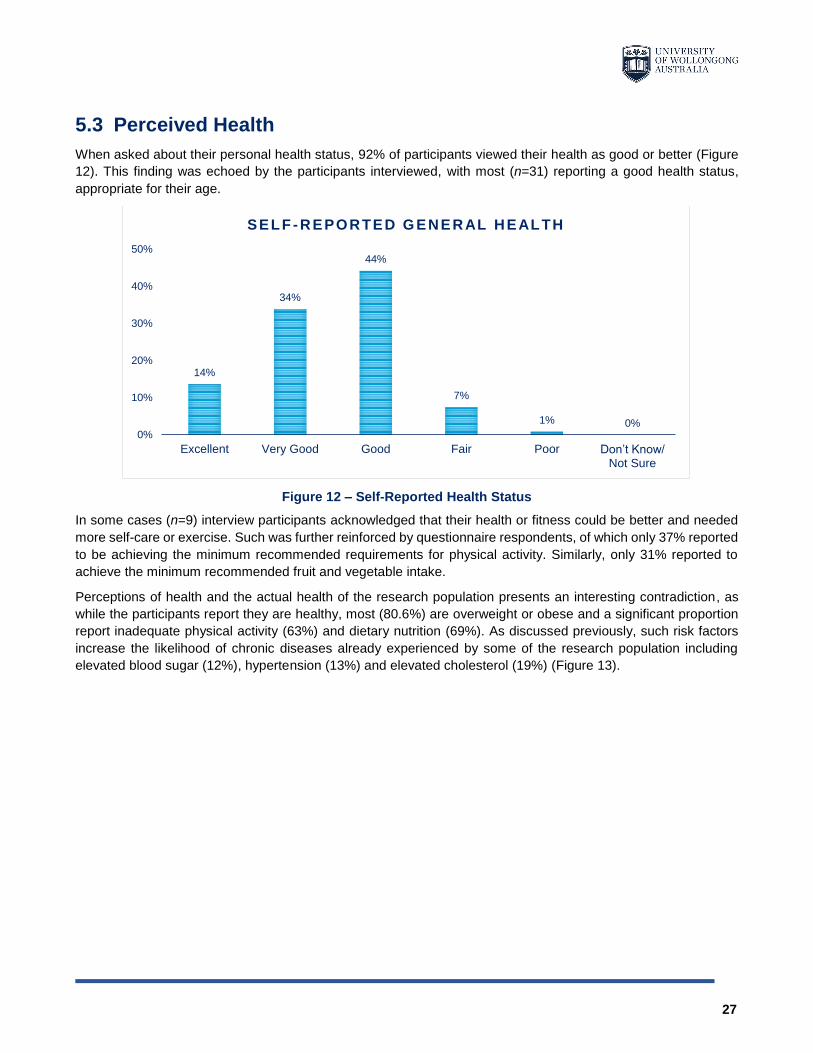
When asked about their personal health status, 92% of participants viewed their health as good or better (Figure
12). This finding was echoed by the participants interviewed, with most (n=31) reporting a good health status,
appropriate for their age.
Figure 12 – Self-Reported Health Status
In some cases (n=9) interview participants acknowledged that their health or fitness could be better and needed
more self-care or exercise. Such was further reinforced by questionnaire respondents, of which only 37% reported
to be achieving the minimum recommended requirements for physical activity. Similarly, only 31% reported to
achieve the minimum recommended fruit and vegetable intake.
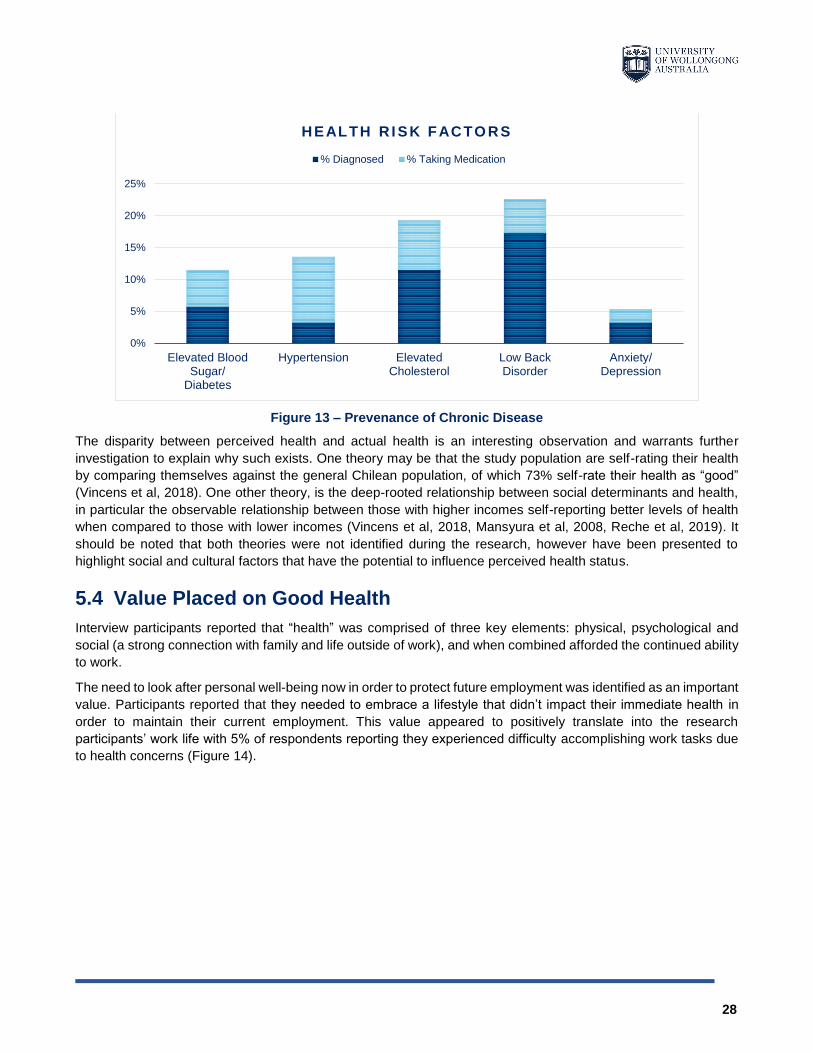
Perceptions of health and the actual health of the research population presents an interesting contradiction, as
while the participants report they are healthy, most (80.6%) are overweight or obese and a significant proportion
report inadequate physical activity (63%) and dietary nutrition (69%). As discussed previously, such risk factors
increase the likelihood of chronic diseases already experienced by some of the research population including
elevated blood sugar (12%), hypertension (13%) and elevated cholesterol (19%) (Figure 13).
14%
34%
44%
7%
1% 0%0%
10%
20%
30%
40%
50%
Excellent Very Good Good Fair Poor Don’t Know/ Not Sure
SELF - REPORTED G ENERAL HEALTH
28
Figure 13 – Prevenance of Chronic Disease
The disparity between perceived health and actual health is an interesting observation and warrants further
investigation to explain why such exists. One theory may be that the study population are self-rating their health
by comparing themselves against the general Chilean population, of which 73% self-rate their health as “good”
(Vincens et al, 2018). One other theory, is the deep-rooted relationship between social determinants and health,
in particular the observable relationship between those with higher incomes self-reporting better levels of health
when compared to those with lower incomes (Vincens et al, 2018, Mansyura et al, 2008, Reche et al, 2019). It
should be noted that both theories were not identified during the research, however have been presented to
highlight social and cultural factors that have the potential to influence perceived health status.
5.4 Value Placed on Good Health
Interview participants reported that “health” was comprised of three key elements: physical, psychological and
social (a strong connection with family and life outside of work), and when combined afforded the continued ability
to work.
The need to look after personal well-being now in order to protect future employment was identified as an important
value. Participants reported that they needed to embrace a lifestyle that didn’t impact their immediate health in
order to maintain their current employment. This value appeared to positively translate into the research
participants’ work life with 5% of respondents reporting they experienced difficulty accomplishing work tasks due
to health concerns (Figure 14).
0%
5%
10%
15%
20%
25%
Elevated BloodSugar/
Diabetes
Hypertension ElevatedCholesterol
Low BackDisorder
Anxiety/Depression
HEALTH R I SK FACTO RS
% Diagnosed % Taking Medication

29
Figure 14 – Difficulty Accomplishing Work Tasks Due to Health
Interview participants were identified to be clearly “future focussed” on aspects of their ongoing health and well-
being for the benefit of both the participants and their families, such is further discussed in the following section.
When questioned in regards to balancing the demands of work with family obligations, 82% of research
participants reported low conflict when managing the demands of work with their demands of their personal lives.
Health and Impact on Family Life
Some (n=8) interview participants reported no current family issues. However, for those expressing issues, two
main concerns were identified. First, a genuine concern regarding future uncertainty, even though things were
reported to be okay at present, there was significant value placed on ensuring things were “looked after” now to
mitigate problems in the future. Second, concern associated with bringing home negative aspects of work that
obstruct short term family connection. Such negative aspects included mood and irritability, along with general
tiredness, illness and muscular issues that prevented them from physically playing with their children.
Work related issues that impacted the participants’ connection and interaction with their immediate and extended
families was identified as important to most interview participants, with a number of participants reporting their
families often worried about them being injured at work, citing such to be a psychological burden.
Employment and Impact on Health
Somewhat surprisingly after the majority of interviewed participants’ self-reported good health, was that the
majority also believed that working conditions did affect their health in some way. Upon further questioning
interview participants elaborated and described numerous factors associated with work that had affected their
health. Factors included travelling to and from work, distances covered in a work day, stress and mental fatigue,
muscular pain, silica exposure and silicosis, colds and flu, weight concerns, sedentary work, sleep problems,
allergies and skin issues.
Many interview participants noted and accepted a decline in their health and fitness with age, specifically
describing deterioration in joints, muscles, being worn out physically and issues associated with working at altitude.
Significantly, many also believed that their health has remained the same as when they started with the company.
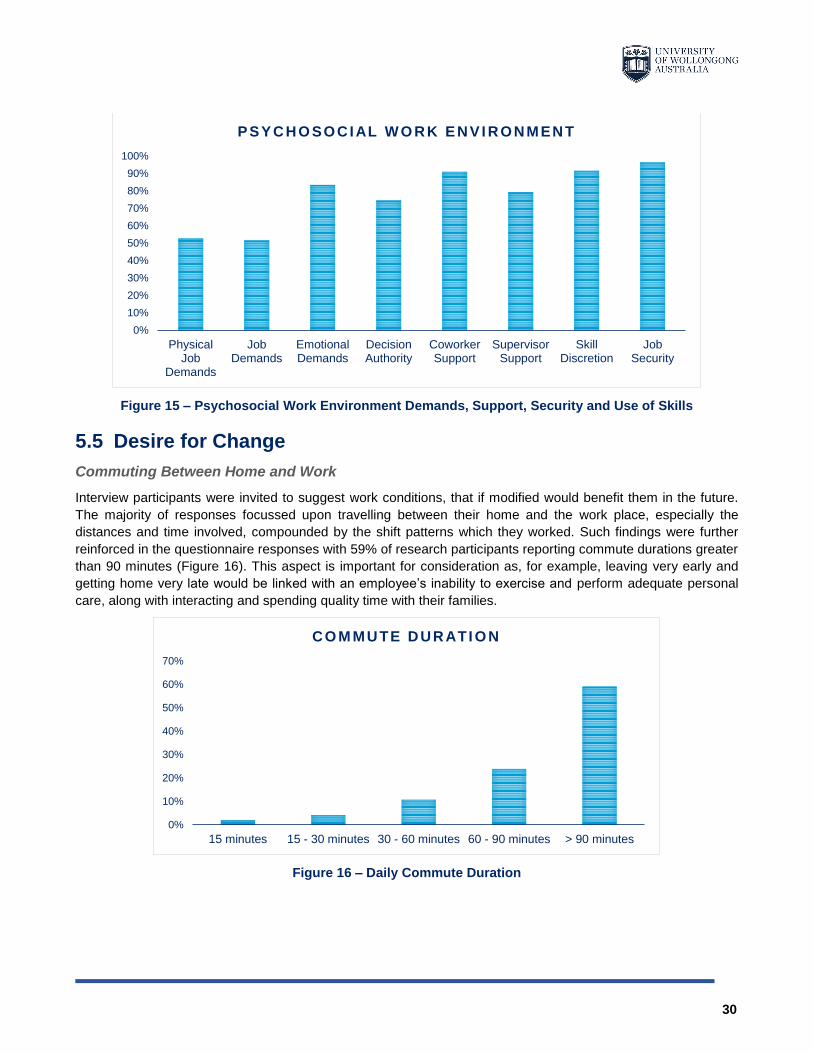
When asked about job demands, 53% of research participants reported high physical demands while 83% reported
high emotional demands. Such demands however are opposed by reported high supervisor and co-worker
support, along with high decision authority and skill discretion (Figure 15).
0%
10%
20%
30%
40%
50%
60%
70%
StronglyDisagree
Disagree Neutral Agree StronglyAgree
HEAL TH I NTERF ERENCE W I TH W O RK
30
Figure 15 – Psychosocial Work Environment Demands, Support, Security and Use of Skills
5.5 Desire for Change
Commuting Between Home and Work
Interview participants were invited to suggest work conditions, that if modified would benefit them in the future.
The majority of responses focussed upon travelling between their home and the work place, especially the
distances and time involved, compounded by the shift patterns which they worked. Such findings were further
reinforced in the questionnaire responses with 59% of research participants reporting commute durations greater
than 90 minutes (Figure 16). This aspect is important for consideration as, for example, leaving very early and
getting home very late would be linked with an employee’s inability to exercise and perform adequate personal
care, along with interacting and spending quality time with their families.
Figure 16 – Daily Commute Duration
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
PhysicalJob
Demands
JobDemands
EmotionalDemands
DecisionAuthority
CoworkerSupport
SupervisorSupport
SkillDiscretion
JobSecurity
PSYCHO SOCIAL W O RK ENVI RONMENT
0%
10%
20%
30%
40%
50%
60%
70%
15 minutes 15 - 30 minutes 30 - 60 minutes 60 - 90 minutes > 90 minutes
CO M MUTE DURATI O N

31
Workloads and the Work Environment
Modifying workloads and experiences at work was suggested by a small number of interviewee’s (n=7), and
therefore was not a strong and reoccurring theme. With regards to shift patterns and shift duration, issues
associated with such were related to travel and the distances between home and work, rather than the roster
arrangement itself.
Interestingly and of note, 89% of research participants reported satisfaction with their job (Figure 17), which is an
important aspect as it significantly influences emotional wellbeing and commitment to work. However, 10% of
research participants reported they intended to leave their job, indicating disengagement and potential negative
impact on wellbeing and productivity (Figure 17).
Figure 17 – Job Satisfaction and Intention to Leave
Concern specifically associated with being female in a male dominated workplace was raised (n=2), however due
to the low proportion of female interview participants (8%), such concern was not repeated however has been
included in this research report as mutual respect and regard for others influence the quality of work life. Such was
further reflected by the research participants with less than half (45%) reporting a fair and just workplace2 (Figure
18) while 63% reported the workplace to be civil3 and respectful.
2 Justice – refers to employee perceptions of fairness in how organisational procedures which affect employee wellbeing and quality of work life are applied. 3 Civil Norms – refers to tolerance of behaviors that violate unspoken rules of mutual respect, courtesy, regard for others.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Job Satisfaction Intention to Leave
JO B SATI SFACTI O N

32
Figure 18 – Justice and Civil Norms
Desire to Change
Interview participants were asked about their future health intentions. Most (n=28) reported a desire to change
their diet, meal quality, nutrition and weight. Such desire to adopt a healthier lifestyle was reflected in the
questionnaire responses where a significant proportion of the research participants indicated they had considered
or were ready to change a range of health behaviours, in particular weight loss (70%), physical activity (71%)
eating habits (73%) and stress reduction (70%) (Figure 19).
Figure 19 – Motivation to Adopt Healthier Lifestyles
Participant interviews (n=16) revealed that Codelco Andina had addressed the issue of eating habits through
targeted programs that included consultation and employee input into the meals provided at work, however the
participant responses with respect to their desire to change was indicated to be a desire to take charge of their
own outcomes, rather than that provided by the company.
0%
10%
20%
30%
40%
50%
60%
70%
Justice Civil Norms
W O RKPLACE AUTO NO M Y
0%
20%
40%
60%
80%
100%
PhysicalActivity
EatingHabits
Tobacco Use Lose Weight ReduceStress
ImproveSleep
ReduceAlcohol
READI NESS FO R CHANG E
Actively Changing Ready Considered

33
5.6 Organisational Support
Interview participants were questioned with regards to the commitment of the company and its leadership towards
workers health. Participants generally believed their supervisors demonstrated a commitment to their health, with
the caveat that the focus was on work-related safety rather than on the broader implications of physical and
psychological well-being. Questionnaire responses further reinforced such findings with 83% of research
participants reporting a safe workplace, including safety initiatives targeted at safe work practices, while only 21%
of respondents reported organisational support4 for initiatives that target healthy behaviours. There is a genuine
opportunity for Codelco to be more pro-active by embedding health initiatives in conjunction with existing safety
programs.
Opportunities provided by Codelco Andina for employees to maintain or improve their health at work indicated a
priority for tobacco control (56%), followed by healthy eating (49%), physical activity (37%) and stress
management (23%) (Figure 20).
Figure 20 – Health Opportunities at Work
Participants generally had some awareness of health-related company policies and programs, especially in the
areas of drugs and alcohol, diet and weight loss. However, many (n=16) reported that they chose not to participate,
primarily due to the timing of the program delivery, citing long work days, particularly when travel was involved, or
because they didn’t feel the need for such programs at the time.
Worker Consultation
Interview participants were questioned regarding worker consultation and involvement in identifying opportunities
to improve workplace conditions that affect health outcomes. Responses differed as some participants believed
while employees were consulted (n=10), such consultation failed to include any follow up (n=5). Almost half of
participants were of the opinion that employees were not consulted (n=19), while a significant proportion believed
the company only acted through the unions (n=22).
4 Organisational Support – refers to company initiatives implemented to support healthy behaviors in employees.
0%
10%
20%
30%
40%
50%
60%
Physical Activity Healthy Eating Tabacco Control StressManagement
HEALTH O PPO RTUNIT I ES AT W O RK
34
Questionnaire responses regarding a supportive health climate5 indicated 46% of respondents believed Codelco
Andina provided opportunities and resources to be healthy, indicating a similar differing awareness of systems
intended to facilitate the improvement of health outcomes.
Interview participants indicated interventions targeting employee diet and exercise is understood to have mixed
results, regardless considerable employee goodwill was observed and could contribute to successful outcomes if
applied towards a well-designed intervention. The observation that some of the company interventions have not
necessarily been well supported or received may be because of design and implementation rather than a lack of
employee desire.
Interview participants reported that more could be done by the company in terms of employee involvement to
identify opportunities for improvements, citing that sometimes ideas were collected but not acted upon, and in
some cases participants felt that they were informed rather than consulted.
Supervisor Resources
Mixed findings were recorded regarding the interview participants’ perception of resources available to supervisors
to be effective in protecting and promoting the safety, health, and welfare of workers. Again, there was a general
consensus that resources made available to supervisors were focused on workplace safety and accident
prevention, rather than an intention for use to improve employee health and well-being. It was acknowledged that
supervisors often were occupied with matters related to work and therefore prevented attention given to worker
health outcomes.
6 CONCLUSIONS
This research project comprises of two main components. Firstly, a review of the current body of knowledge on
the effectiveness of workplace health promotion interventions. Secondly, population data that was collected and
analysed from a representative Chilean mine operation.
This section of the report outlines the findings of those research activities.
6.1 Literature
A significant amount of research reported in the literature has been conducted on workplace interventions targeting
overweight and obesity among employees. However, most of these studies have been conducted in developed
countries and in workplaces with reliable support systems, therefore, findings may not be applicable to developing
countries (Mattke et al. 2013).
Evidence of Intervention Effectiveness
Evidence for actual effectiveness of health promotion interventions demonstrated positive effects on diet and
exercise, smoking, alcohol use and health care costs. There was limited impact on absenteeism and mental
health.
However, the usefulness of this ‘evidence’ has been criticised as anecdotal and inconclusive as many interventions
lacked rigorous evaluation (Mattke et al. 2012). Any positive effects observed were more likely to be associated
with the intensity of the intervention itself (Mattke et al. 2012).
5 Supportive Health Climate – refers to the extent of which employees are aware of social support networks and practices that promote and maintain improved health behaviors.

35
Additionally, the abundance of literature only encompassed a minor proportion of interventions and prompted
questions regarding the generalisability of reported findings, particularly in developing countries and in
subpopulations (Mattke et al. 2012).
Studies relevant to the effectiveness of health promotion interventions implemented in the mining industry were
not identified in any of the sources, nor were studies relevant to the Chilean working population, therefore
reinforcing the priority for research efforts.
Intervention Strategies
The literature review identified a need to evaluate the impact of workplace health interventions in “real world”
settings to better inform decision making and improve health outcomes at workplaces.
The “Total Worker Health” (TWH) framework and supporting theoretical knowledge aims for successful and
sustainable interventions by integrating health promotion into exisiting workplace policies, programs and practices
(Seabury et al. 2005). The suitability of the framework in ‘real world’ settings is appropriate as it can be adapted
to accommodate the social norms and cultural influences relevant to the target country (Sorensen et al. 2016a).
The TWH framework was identified as a method suitable for use in the occupational environment to improve
worker’s nutrition and physical activity-related behaviours and decrease musculoskeletal injuries in Chilean mine
workers.
A summary and conclusion regarding current literature is provided in Table 9.
Table 9 – Conclusion: Literature Regarding the Effectiveness of Health Promotion Interventions
SUMMARY:
The majority of literature has been published by developed countries.
The literature only covers a small proportion of interventions, preventing the translation
of results, particularly in developing countries and in subpopulations.
Intervention intensity was identified as a confounder, influencing intervention
effectiveness.
Conclusive health promotion research requires greater rigorous evaluation, such that
policymakers are informed when making decisions and to improve health outcomes.
The Total Worker Health framework can be applied to guide research methods to
evaluate the impact of workplace health interventions in “real world” settings.
CONCLUSION:
Conclusive health promotion literature, particularly regarding the Chilean working
population is deficient. Therefore, research regarding the design, testing and evaluation
of workplace interventions relevant in the Chilean context should be prioritised.
The Total Worker Health framework is suggested for use to guide such research.
6.2 Research Population
Results of the research demonstrated a significant proportion of the research population is overweight or obese
(80.6%) and is consistent with prevalence in the general Chilean adult population (91%).
Comparison of other non-communicable disease risk factors demonstrated the research population had a reduced
prevalence of elevated blood pressure, elevated fasting glucose and elevated cholesterol when compared to the
general Chilean adult population. Additionally, the mean systolic blood pressure in the research population is
slightly lower than the general Chilean adult population. It should be noted that although the results of such risk
factors are considered marginally better, they are not statistically significant.
36
One possible explanation for this observation is the requirement for all persons who work at the Andina Mine to
comply with established medical criteria and demonstrate on an annual basis that they are fit for their role and
continued occupational altitude exposure (Chilean Ministry of Health, 2020). It should be noted that this
relationship was not identified during the research, however is suggested to highlight a potential positive
relationship between occupational fitness requirements and preventing the progression of non-communicable
disease risk factors over time.
The perceived health and the actual health of the research population presented an interesting contradiction, as
the research population believe they are healthy, although the majority are overweight or obese and report
inadequate physical activity and dietary nutrition. This perception is incongruent with measured health outcomes,
in particular those risk factors that promote non-communicable disease.
Such a contradiction was an interesting study observation and warrants further investigation to explain why. One
supposition may be that the study population are self-rating their health by comparing themselves against their
peers in the general Chilean population. Alternately, this could be due to the deep-rooted relationship between
social determinants and health, in particular the observable relationship between those with higher incomes self-
reporting better levels of health when compared to those with lower incomes (Vincens et al, 2018, Mansyura et al,
2008, Reche et al, 2019). While neither of these suppositions were tested or identified during the research, they
have been presented to highlight social and cultural factors that have the potential to influence perceived health
status.
A summary and conclusion regarding the health status of the research population is provided in Table 10.
Table 10 – Conclusion: Health Status of the Research Population
SUMMARY:
Majority of the research population believe they are healthy, despite a significant
proportion being overweight or obese and reporting inadequate physical activity and
dietary nutrition.
The prevalence of overweight and obesity in the research population is commensurate
with the general Chilean adult population.
Non-communicable disease risk factors were observed to be slightly lower in the
research population when compared to the general Chilean adult population.
CONCLUSION: The perceived health of the research population is incongruent with measured non-
communicable disease risk factors.
6.2.1 Health Beliefs and Attitudes
Value Placed on Health and Desire to be Healthy
Good health was observed to be valued significantly as it is believed to be a fundamental and inherent enabler for
continued participation in work. This observation ironically mirrors the underpinning principle of the Ottawa Charter,
that is health is a “resource for everyday life, not the object of living” (WHO 2016c).
The research population were clearly “future focussed” citing the ability to work afforded both themselves and their
families’ greater benefits and an ability to prepare for future uncertainty. This value and belief translates into a
genuine desire to be healthy.
The strong connection between “being healthy” and protecting future employment was contrasted by the
identification of numerous work related factors that had impacted the health of the research population. Factors
included travelling to and from work, distances covered in a work day, stress and mental fatigue, muscular pain,

37
silica exposure and silicosis, colds and flu, weight concerns, sedentary work, sleep problems, allergies and skin
issues.
Maintaining a connection with immediate and extended family members was identified as an important value.
Issues compromising this desired connection were identified to include mood and irritability, along with general
tiredness, illness and muscular issues that prevented physical play with children.
A summary and conclusion regarding the health beliefs and attitude of the research population is provided in Table
11.
Table 11 – Conclusion: Health Beliefs and Attitudes
SUMMARY:
The research population are focused on the future of themselves and their families
Health is believed to be a fundamental and inherent enabler for continued participation
in work
Work related factors were identified to impact both health and family connection
CONCLUSION: The research population genuinely desire to be healthy and place great value on the
benefits of being healthy.
6.3 Organisation Health Promotion
Worker Consultation and Input
Codelco Andina have implemented a number of health promotion programs, in particular those that target tobacco
use, drugs, alcohol, diet and weight loss. The design of such programs however, involved less than desired worker
consultation and subsequently once implemented, were not well supported or received, primarily due to the due
to the timing of the program delivery, not because of the intervention itself.
Balancing the demands of long work days against a willingness to participate in health improvement activities is
not only the challenge, however presents an opportunity. Considerable goodwill was observed in the research
population which may result in successful outcomes if applied to an intervention designed with worker consultation
and input.
Commuting Between Home and Work
Daily commute durations between home and work, and vice-versa was identified as the most significant issue for
the majority of the research population, particularly where such was compounded by 12 hour shift patterns. This
issue is important when considering the impact on worker health. While the research recognises commute
activities inherently do not directly cause adverse health, it does however influence the workers opportunity to
participate in health promoting activities such as exercise, personal care and spending quality time with their family.
The relationship between long work days (particularly where travel is involved) and each workers opportunity to
rest and recover provides greater context for the less than desirable participation in company health promotion
programs and was reinforced by the research.
Organisational Support
The company and its supervisors demonstrate a genuine commitment to the health of its workers, however such
is caveated by a focus on work-related safety rather than on the broader implications of physical and psychological
well-being.
The research population are mature in their understanding of the relationship between their work environment and
their physical and psychological well-being. They demonstrate genuine support for their supervisors and a
38
willingness to be involved in programs that suit both their needs and their availability, taking into account the
peculiar challenges of working at altitude and some distance from their homes. This should allow the company to
integrate all of this into a comprehensive system that looks at both the present, with an emphasis on safety, and
the future, with an emphasis on long term health and well-being.
A summary and conclusion regarding company health promotion programs is provided in Table 12.
Table 12 – Conclusion: Organisational Health Promotion
SUMMARY:
The support of historical company interventions may be because of the design and
implementation rather than a lack of employee desire.
Long commute durations significantly encroach workers opportunity to participate in
health promoting activities
Health programs are eclipsed by workplace safety programs and are therefore not
considered to be a priority
CONCLUSION:
Existing and well-known issues are actually opportunities for company improvement,
however such improvements fundamentally rely on genuine company consultation with
its workforce to seek input and collectively identify solutions appropriate to both parties.
6.4 Recommendations
The research revealed opportunities for improvement that can be targeted at the local research site, the wider
Codelco Company and nationally and are presented below:
Codelco Andina
Communicate the results of this research with workers and Codelco Andina;
Apply the results of this research to identify existing systems of work that can be tailored to include
health promotion interventions, rather than establishing stand-alone health programs;
Establish standardised methods for worker consultation and input into health promotion programs such
that programs are co-designed and co-implemented;
Continue to collect de-identified medical surveillance data; and
Analyse and review such data periodically to better understand the health of the research population
over time.
Codelco
Communicate the results of this research in Codelco;
If not already performed, centralise the de-identified medical surveillance data for the entire Codelco
working population; and
If not already performed, analyse and review such data periodically to better understand the health of
the Codelco working population over time and to identify opportunities for companywide improvement.
Chile
Communicate the results of this research for purposes of promoting knowledge of methods that can be
applied to identify suitable workplace health promotion interventions;
Develop and validate instruments for use by Chilean employers that facilitate the identification of suitable
health promotion interventions; and

39
Prioritise research regarding the design, testing and evaluation of workplace interventions relevant in the
Chilean context.
6.5 Limitations
Research interviews are a small sample (n=40) of the total research participant (n=242) sample. The number of
interviews, although smaller than the number of research participants, is still considered sufficiently large to have
addressed the main issues and themes relevant to the research population (Saunders et al., 2018). The interview
questions were mostly followed and then elaborated upon, however, there were instances where the wording was
slightly changed in order to make meaning for the interviewee, and also a few instances where certain questions
were omitted. None of these instances are thought to have detracted from the overall body of results generated.
40
7 REFERENCES
ABS 2008, Overweight and Obesity in Adults, Australia, 2004-05, Australian Bureau of Statistics, viewed
October 2 2016, http://www.abs.gov.au/ausstats/[email protected]/Latestproducts/4719.0Main%20Features32004-
05?opendocument&tabname
Agampodi, T.C., Agampodi, S.B., Glozier, N. and Siribaddana, S., 2015. Measurement of social capital in
relation to health in low and middle income countries (LMIC): a systematic review. Social Science &
Medicine, 128, pp.95-104.
Albala, C., Vio, F., Kain, J. & Uauy, R. 2002, ‘Nutrition transition in Chile: determinants and consequences’,
Public Health Nutrition, vol. 5, no. 1a, pp. 123-128.
Anandacoomarasamy, A., Caterson, I., Sambrook, P., Fransen, M. & March, L. 2008, ‘The impact of
obesity on the musculoskeletal system’, International Journal of Obesity, vol. 32, no. 2, pp. 211-222.
Anger, W.K., Elliot, D.L., Bodner, T., Olson, R., Rohlman, D.S., Truxillo, D.M., Kuehl, K.S., Hammer, L.B. &
Montgomery, D. 2015, ‘Effectiveness of Total Worker Health interventions’, Journal of Occupational Health
Psychology, vol. 20, no. 2, pp. 226-247.
Batt, M.E. 2009, ‘Physical activity interventions in the workplace: the rationale and future direction for
workplace wellness’, British Journal of Sports Medicine, vol. 43, no. 1, pp. 47-48.
Baum, F. 2008, The New Public Health, 3 edn, Oxford University Press, South Melbourne, Victoria.
Baum, F. 2011, ‘From Norm to Eric: avoiding lifestyle drift in Australian health policy’, Australian and New
Zealand Journal of Public Health, vol. 35, no. 5, pp. 404-406.
Baum, F. & Sanders, D. 1995, ‘Can health promotion and primary health care achieve health for all without
a return to their more radical agenda?’, Health Promotion International, vol. 10, no. 2, pp. 149-160.
Berelson, B. (1952). Content analysis in communication research. New York: Hafner.
Bully, P., Sánchez, Á., Zabaleta-del-Olmo, E., Pombo, H. & Grandes, G. 2015, ‘Evidence from
interventions based on theoretical models for lifestyle modification (physical activity, diet, alcohol and
tobacco use) in primary care settings: A systematic review’, Preventive Medicine, vol. 76, Supplement, pp.
S76-S93.
Celis-Morales, C., Salas, C., Alduhishy, A., Sanzana, R., Martínez, M.A., Leiva, A., Diaz, X., Martínez, C.,
Álvarez, C. & Leppe, J. 2016, ‘Socio-demographic patterns of physical activity and sedentary behaviour in
Chile: results from the National Health Survey 2009–2010’, Journal of Public Health, vol. 38, no. 2, pp. e98-
e105.
Chilean Ministry of Health. 2020, Guía Técnica: Sobre Exposición Ocupacional a Hipobaria Intermitente
Crónica Por Gran Altitud, Departamento de Salud Ocupacional, viewed May 11 2020,
https://www.minsal.cl/sites/default/files/guia_hipobaria_altitud.pdf
Christakis, N.A. & Fowler, J.H. 2007, ‘The spread of obesity in a large social network over 32 years’, New
England Journal of Medicine, vol. 357, no. 4, pp. 370-379.
CPH-NEW. 2014, Healthy Workplace All Employee Survey, Center for Promotion of Health in the New
England Workplace, viewed August 22 2019, https://www.uml.edu/docs/AES_manual_4-17-14_tcm18-
147260.pdf
41
Doiron, D., Fiebig, D.G., Johar, M. and Suziedelyte, A., 2015. Does self-assessed health measure health?.
Applied Economics, 47(2), pp.180-194.
Gazmararian, J.A., Elon, L., Newsome, K., Schild, L. & Jacobson, K.L. 2013, ‘A randomized prospective
trial of a worksite intervention program to increase physical activity’, American Journal of Health Promotion,
vol. 28, no. 1, pp. 32-40.
Grunseit, A.C., O’Hara, B.J., Chau, J.Y., Briggs, M. & Bauman, A.E. 2015, ‘Getting the Message Across:
Outcomes and Risk Profiles by Awareness Levels of the “Measure-Up” Obesity Prevention Campaign in
Australia’, PLoS One, vol. 10, no. 4.
Hancock, T. 2007, ‘Creating Environments for Health – 20 Years On’, Promotion & Education, vol. 14, no.
s2, pp. 7-8.
Health, H.S.o.P. 2016, The Nutrition Transition, Harvard School of Public Health, viewed September 30
2016, https://www.hsph.harvard.edu/obesity-prevention-source/nutrition-transition/
Hopkins, J.M., Glenn, B.A., Cole, B.L., McCarthy, W. & Yancey, A. 2012, ‘Implementing organizational
physical activity and healthy eating strategies on paid time: Process evaluation of the UCLA WORKING
pilot study’, Health Education Research, vol. 27, no. 3, pp. 385-398.
Hunt, K. & Emslie, C. 2001, ‘Commentary: The prevention paradox in lay epidemiology – Rose revisited’,
International Journal of Epidemiology, vol. 30, pp. 442-446.
ILO 2012, A comprehensive approach to improving nutrition at the workplace: A survey of Chilean
companies and tailored recommendations, International Labour Organization, Geneva, Switzerland.
Kickbusch, I. 2007, ‘The Move Towards a New Public Health’, Promotion & Education, vol. 14, no. 2, p. 9.
Kickbusch, I. 2015, ‘The imperative of public health: opportunity or trap?’, Health Promotion International,
vol. 30, no. 2, pp. 197-200.
King, E., Grunseit, A., O’Hara, B. & Bauman, A. 2013, ‘Evaluating the effectiveness of an Australian obesity
mass-media campaign: how did the ‘Measure-Up’ campaign measure up in New South Wales?’ Health
education research, vol. 28, no. 6, pp. 1029-1039.
Labonté, R. 2011, ‘Toward a post-Charter health promotion’, Health Promotion International, vol. 26, no.
suppl 2, pp. ii183-ii186.
Mansyur, C., Amick, B.C., Harrist, R.B. and Franzini, L., 2008. Social capital, income inequality, and self-
rated health in 45 countries. Social Science & Medicine, 66(1), pp.43-56.
Mattke, S., Liu, H., Caloyeras, J.P., Huang, C.Y., Van Busum, K.R., Khodyakov, D. & Shier, V. 2013,
Workplace wellness programs study.
Mattke, S., Schnyer, C. & Van Busum, K. 2012, A review of the US workplace wellness market,
083307721X, Rand Health.
Méndez, J. 2018. Health evaluation for occupational high-altitude exposure: results from a Chilean copper
mine during 2016. Occupational and Environmental Medicine, 75 (Suppl_2).
Michaels, C.N. & Greene, A.M. 2013, ‘Worksite Wellness: Increasing Adoption of Workplace Health
Promotion Programs’, Health Promotion Practice, vol. 14, no. 4, pp. 473-479.

42
NIOSH 2008, Essential elements of effective workplace programs and policies for improving worker health
and wellbeing, U.S Department of Health and Human Services, viewed September 16 2016,
http://www.cdc.gov/niosh/twh/essentials.html
Osilla, K.C., Van Busum, K., Schnyer, C., Larkin, J.W., Eibner, C. & Mattke, S. 2012, ‘Systematic review of
the impact of worksite wellness programs’, American Journal of Managed Care, vol. 18, no. 2.
Østbye, T., Stroo, M., Brouwer, R.J.N., Peterson, B.L., Eisenstein, E.L., Fuemmeler, B.F., Joyner, J.,
Gulley, L. & Dement, J.M. 2013, ‘The steps to health employee weight management randomized control
trial: Rationale, design and baseline characteristics’, Contemporary Clinical Trials, vol. 35, no. 2, pp. 68-76.
Reche, E., König, H.H. and Hajek, A., 2019. Income, Self-Rated Health, and Morbidity. A Systematic
Review of Longitudinal Studies. International Journal of Environmental Research and Public Health, 16(16),
p.2884.
Ridde, V., Guichard, A. & Houeto, D. 2007, ‘Social inequalities in health from Ottawa to Vancouver: action
for fair equality of opportunity’, Promotion & Education, vol. 14, no. S2, pp. 12-16.
Rongen, A., Robroek, S.J.W., van Lenthe, F.J. & Burdorf, A. 2013, ‘Workplace Health Promotion: A Meta-
Analysis of Effectiveness’, American Journal of Preventive Medicine, vol. 44, no. 4, pp. 406-415.
Rose, G. 2001, ‘Sick individuals and sick populations’, International Journal of Epidemiology, vol. 30, no. 3,
pp. 427-432.
Rydin, Y., Bleahu, A., Davies, M., Dávila, J., Friel, S., De Grandis, G., Groce, N., Hallal, P., Hamilton, I.,
Howden-Chapman, P., Lai, K., Lim, C., Martins, J., Osrin, D., Ridley, I., Scott, I., Taylor, M., Wilkinson, P. &
Wilson, J. 2012, ‘The Lancet Commissions: Shaping cities for health: complexity and the planning of urban
environments in the 21st century’, The Lancet, vol. 379, pp. 2079-2108.
San Martin, R., Brito, J., Siques, P. and León-Velarde, F., 2017. Obesity as a conditioning factor for high-
altitude diseases. Obesity Facts, 10(4), pp.363-372.
Saunders, B. et al. (2018). Saturation in qualitative research: exploring its conceptualization and
operationalization. Qual Quant. 2018; 52(4): 1893–1907. Published online 2017 Sep 14. doi:
10.1007/s11135-017-0574-8
Seabury, S.A., Lakdawalla, D. & Reville, R.T. 2005, The economics of integrating injury and illness
prevention and health promotion programs, RAND Institute for Civil Justice.
Sorensen, McLellan, D.L., Sabbath, E.L., Dennerlein, J.T., Nagler, E.M., Hurtado, D.A., Pronk, N.P. &
Wagner, G.R. 2016a, ‘Integrating worksite health protection and health promotion: A conceptual model for
intervention and research’, Preventative Medicine, vol. 91, pp. 188-196.
Sorensen, G., Nagler, E.M., Hashimoto, D., Dennerlein, J.T., Theron, J.V., Stoddard, A.M., Buxton, O.,
Wallace, L.M., Kenwood, C., Nelson, C.C., Tamers, S.L., Grant, M.P. & Wagner, G. 2016b, ‘Implementing
an Integrated Health Protection/Health Promotion Intervention in the Hospital Setting Lessons Learned
From the Be Well, Work Well Study’, Journal of Occupational and Environmental Medicine, vol. 58, no. 2,
pp. 185-194.
Tamers, S.L., Beresford, S.A.A., Cheadle, A.D., Zheng, Y., Bishop, S.K. & Thompson, B. 2011, ‘The
association between worksite social support, diet, physical activity and body mass index’, Preventive
Medicine, vol. 53, no. 1-2, pp. 53-56.
43
Thorndike, A.N., Sonnenberg, L., Healey, E., Myint-U, K., Kvedar, J.C. & Regan, S. 2012, ‘Prevention of
weight gain following a worksite nutrition and exercise program: A randomized controlled trial’, American
Journal of Preventive Medicine, vol. 43, no. 1, pp. 27-33.
Vartiainen, E.A., Laatikainen, T., Philpot, B., Janus, E.D., Davis-Lameloise, N. & Dunbar, J.A. 2011, ‘The
projected impact of population and high-risk strategies for risk-factor control on coronary heart disease and
stroke events’, Medical journal of Australia, vol. 194, no. 1, pp. 10-15.
Vincens, N., Emmelin, M. and Stafström, M., 2018. Social capital, income inequality and the social gradient
in self-rated health in Latin America: A fixed effects analysis. Social Science & Medicine, 196, pp.115-122.
Vio, F., Albala, C. & Kain, J. 2008, ‘Nutrition transition in Chile revisited: mid-term evaluation of obesity
goals for the period 2000–2010’, Public Health Nutrition, vol. 11, no. 4, pp. 405-412.
Wakefield, M.A., Coomber, K., Durkin, S.J., Scollo, M., Bayly, M., Spittal, M.J., Simpson, J.A. & Hill, D.
2014, ‘Time series analysis of the impact of tobacco control policies on smoking prevalence among
Australian adults, 2001? 2011’, Bulletin of the World Health Organization, vol. 92, no. 6, pp. 413-422.
WHO 2008, Mean Total Cholesterol (age-standardized estimate) (25 years +), World Health Organisation,
visited 26 Septiembre 2019, https://www.who.int/data/gho/data/indicators/indicator-details/GHO/mean-total-
cholesterol-(age-standardized-estimate)
WHO 2014, Blood Glucose. Raised fasting (≥ 7.0 mmol/L or ≥ 126 mg/dL) (age-standardized), World
Health Organisation, visited 26 Septiembre 2019, https://www.who.int/data/gho/data/indicators/indicator-
details/GHO/raised-fasting-blood-glucose-(-=7-0-mmol-l-or-on-medication)(age-standardized-estimate)
WHO 2015a, Noncommunicable diseases: Fact Sheet, World Health Organisation, visited 4 May 2016,
http://gamapserver.who.int/gho/interactive_charts/ncd/risk_factors/physical_inactivity/atlas.html?detectflash
=false
WHO 2015b, Mean Systolic Blood Pressure (age-standardized estimate), World Health Organisation,
visited 26 September 2019, https://www.who.int/data/gho/data/indicators/indicator-details/GHO/mean-
systolic-blood-pressure-(age-standardized-estimate)
WHO 2015c, Raised Blood Pressure (SBP ≥ 140 or DBP ≥ 90) (age-standardized estimate), World Health
Organisation, visited 26 September 2019, https://www.who.int/data/gho/data/indicators/indicator-
details/GHO/raised-blood-pressure-(sbp-=140-or-dbp-=90)-(age-standardized-estimate)
WHO 2016a, Global Health Observatory (GHO) data: Noncommunicable diseases (NCD), World Health
Organisation, visited 4 May 2016, http://www.who.int/gho/ncd/en/
WHO 2016b, Health promotion: The Ottawa Charter for Health Promotion, World Health Organisation,
visited 13 March 2016, http://www.who.int/healthpromotion/conferences/previous/ottawa/en/
WHO 2016c, The workplace: A priority setting for health promotion, World Health Organisation, visited
October 2 2016, http://www.who.int/occupational_health/topics/workplace/en/
WHO 2016d, Global Health Observatory (GHO) data: Prevalence of underweight among adults, BMI <
18.5, age-standardized. Estimates by country, World Health Organisation, visited 26 September 2019,
https://apps.who.int/gho/data/node.main.NCDBMILT18A?lang=en
WHO 2020, Process of Translation and Adaptation of Instruments, World Health Organisation, visited 12
May 2020, https://www.who.int/substance_abuse/research_tools/translation/en/
















