51
In the name of ALLAH, the Beneficent the Merciful

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 1/51
In the name of ALLAH, the Beneficent the Merciful
8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 2/51
CPC
with
Thomas Ruenger MDP
hd
Muhammad Khawar Nazir
2nd Feb. 2009

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 3/51
History
15 years old boy,
PC: Brown big itchy and painful bumps on facesince last 1 year
h/o trauma with lead pencil on left hand
1 month after trauma, lesions started at facewhich are spreading
No family h/o skin diseases No past medical history
Review of systems : Insignificant

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 4/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 5/51
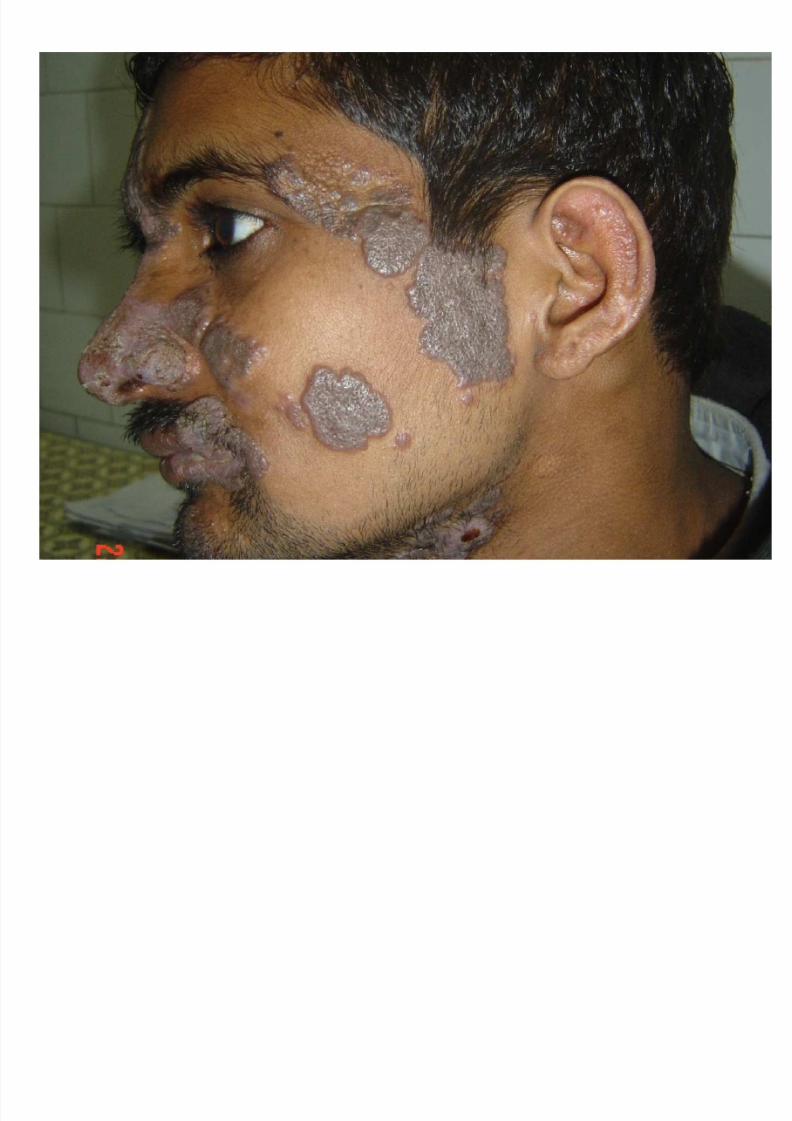
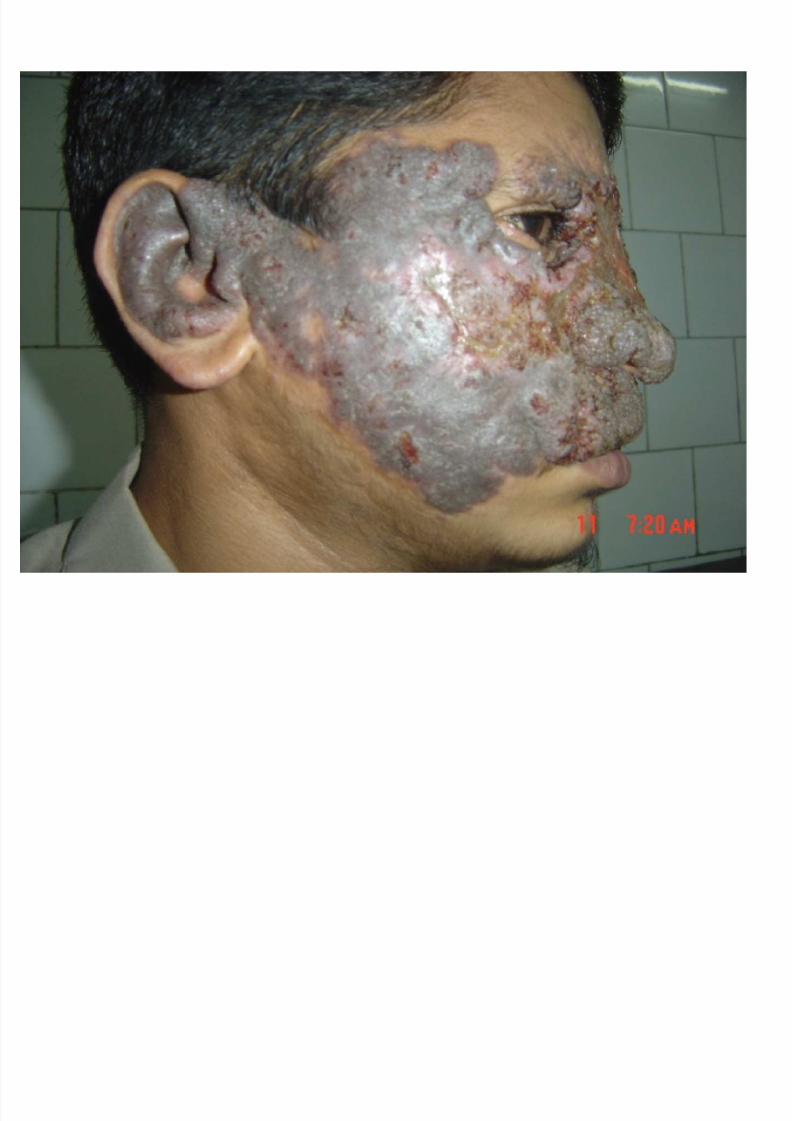
Examination
Face, almost whole central face sparing eyesand chin
Hyperpigmented verrucous induratedplaques, firm, well defined, mild erythema,few erosions
Peripheral borders are elevated, centralscarring

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 6/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 7/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 8/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 9/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 10/51
Differenital Diagnosis
Cutaneous tuberculosis
Blastomycosis
Leishmaniasis
Atypical Mycobacterial Infection

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 11/51
Diagnosis
Biopsy
CHROMOBLASTOMYCOSIS

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 12/51
TREATMENT
Terbinafin
Fluoconazol
Cryotherapy
Psychological help
Plastic Surgery

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 13/51
CHROMOBLASTOMYCOSIS
8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 14/51
Synonyms:
Chromomycosis
Cladosporiosis
Verrucous dermatitis
Phaeosporotrichosis
Pedroso's disease
Fonseca's disease

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 15/51
INTRODUCTION
verrucous dermatosis caused by several
genera of dematiaceous, or pigmented, fungi
Typically chronic in nature, an expandingverrucous plaque on the lower, or occasionally
upper, extremity is the classic presentation

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 16/51
INTRODUCTION
6 fungi are responsible for the vast majority of cases:
Fonsecaea pedrosoi ,
Phialophora verrucosa,
C ladosporium carrionii , Fonsecaea compacta,
Fonsecaea monophora and
Rhinocladiella aquaspera.
The clinical presentation and colonial morphologies of each of these fungi are very similar, and differentiation is based onmicroscopic and conidial characteristics

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 17/51
HISTORY
Pedroso first recognized chromoblastomycosis
in 1911
Four years later, Medlar & Lane reported the
first case in the US (in Boston)

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 18/51
Confusion over the proper naming
At one point, chromoblastomycosis was thoughtto be closely related to blastomycosis; however,
cellular division does not occur via budding(blasto-) but rather via internal septation, hencethe preference for the term chromomycosis
Nonetheless, some authors have argued thatchromomycosis is also confusing, because it hasthe same meaning as phaeohyphomycosis, andso they prefer the term chromoblastomycosis

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 19/51
EPIDEMIOLOGY
Most commonly found in tropical and subtropical climates
Occasionally in temperate zones such as the US, Europeand Canada
Farmers, miners and others working in rural areas are athigher risk than the general population
Men 20 to 60 years of age are more often affected,probably due to their increased occupational exposure
Up to 90% of cases result from occupational exposure

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 20/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 21/51
CLINICAL FEATURES
Usually presents as a papule or nodule on the leg,which progresses to form a verrucous orgranulomatous plaque
Lesion may appear annular as the central portionresolves with scarring
Several lesions may coalesce to form amultinodular mass, or multiple lesions may existas discrete islands scattered within unaffectedskin

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 22/51
CLINICAL FEATURES
It is thought that autoinoculation, fromscratching, may be responsible for the spread of infection
Only one extremity is typically affected.Sometimes, a subcutaneous nodule or tumor isthe presenting lesion
Local or constitutional symptoms are not typical.

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 23/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 24/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 25/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 26/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 27/51
8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 28/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 29/51
Annular and figurate
plaques due to central
clearing and scarringwith a verrucous surface
on the arm (A) and a
more granulomatous
appearance on the leg
(B
).
C Brown-colored
sclerotic body within a
mixed granulomatous
and neutrophilic dermalinfiltrate.
C, C ourtesy of Jennifer
McNiff MD.

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 30/51
Pathology
Pseudoepitheliomatous hyperplasia, intraepidermal abscesses, andsuppurative and granulomatous inflammation within the dermis arethe typical histologic findings
Round, pigmented bodies, which are said to resemble copperpennies (6 to 12 mm), are present in the dermis, bothextracellularly and within giant cells
These are unique to chromoblastomycosis and are also known as
Medlar bodies or sclerotic bodies
Detection of organisms via PCR of tissue samples has been reportedfor the more common species.

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 31/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 32/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 33/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 34/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 35/51
Differential Diagnosis
Biopsy is indicated to exclude other granulomatousinfectious diseases such as
Cutaneous tuberculosis,
Tertiary syphilis, Blastomycosis or
Leishmaniasis
that may also have associated scarring
Mycetoma is another implantation mycosis that commonlyaffects the lower extremity, but edema, draining sinusesand grains point to this diagnosis

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 36/51
If a biopsy is not feasible, a KOH examination
of scrapings from a pigmented portion of the
lesion is performed
The presence of pigmented Medlar bodies is
diagnostic (excluding diagnoses such asblastomycosis), but hyphae may also be seen
Culture growth (at 2530°C) is slow and thedifferent genera produce fairly similar colonial
morphologies

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 37/51
Major differences between genera are the microscopicfeatures, in particular the type of conidia produced inculture.
3major types
Cladosporium-like (long branching side chainswith shield cells at branch points)
Phialophora-like (conidia resemble overflowing
buds in a vase)
Rhinocladiella-like (overall configuration similar toa mascara brush).

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 38/51
Treatment
Therapeutic options are limited
Some authors have advocated heat therapy based on evidence that thecausative organisms will not grow at high temperatures
For small lesions, surgical excision (plus systemic antifungal treatment) can beattempted
5-Flucytosine combined with either oral thiabendazole, intravenousamphotericin B or an oral triazole has been reported to be efficacious.
Itraconazole alone (200-400 mg/day) administered for at least 6 months hasproved promising, with up to 80-90% cure rates according to one author
.

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 39/51
Treatment
The newest triazole, voriconazole, may also proveto be beneficial
In a small series, oral terbinafine (500 mg/day) given for at least 7 months was described aseffective
Cryosurgery and the addition of antibiotics if thelesion is secondarily infected

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 40/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 41/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 42/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 43/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 44/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 45/51
8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 46/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 47/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 48/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 49/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 50/51

8/8/2019 Chromo Blas to Mycosis
http://slidepdf.com/reader/full/chromo-blas-to-mycosis 51/51
THANK YOU

















