Chronic Opioid Therapy Safe Prescribing in Primary Care Nancy Wiedemer,CRNP VISN 4 Pain Management POC Pain Management Coordinator Philadelphia VA Michael Mangione, MD Chief of Anesthesia and Director of Pain Service VA Pittsburgh Health Care System
Transcript
Chronic Opioid Therapy
Safe Prescribing in Primary Care
Nancy Wiedemer,CRNP
VISN 4 Pain Management POC
Pain Management Coordinator
Philadelphia VA
Michael Mangione, MD
Chief of Anesthesia and Director of Pain Service
VA Pittsburgh Health Care System
Objectives
Facility level: Participants will identify strategies to work
toward an institutional commitment to evidence based
opioid prescribing
Pact level: Identify strategies that can be implemented in
Primary Care to promote consistent opioid prescribing
utilizing the expertise of all PACT members to their
Background- why are we still talking about OPIOIDS !!!
Briefly outline the major tenets of Chronic Opioid Therapy (VA/DOD Clinical Practice Guidelines)
Through case scenarios and audience polling, discuss specifics of practice especially hot topics:
high dose opioids
short-acting vs long-acting
decreasing /stopping opioids
methadone
Address questions and cases from the audience
Avoidance (70s to 90’s)
Total fear of
prescribing opioids
even in dying patients
No ceiling (mid 90’s – 2003-04)
Widespread use of
opioids using cancer
model of treatment
Opioid Opioid
Pendulum
Pain as the 5th VS
VHA in 98 ---- JC in 2000
Unintended outcome of Pain as the 5th Vital Sign
Epidemic of Unintentional Rx Drug Overdose and Death
CDC’s Issue Brief: Unintentional drug poisoning in the United States. Unintentional drug poisoning includes drug
overdoses resulting from drug misuse, drug abuse, and taking too much of a drug for medical reasons.
5
WHO
ANALGESIC
LADDER
5TH VITAL SIGN
Heroin
Crack
Cocaine
Rx Drugs (Opioids)
Avoidance (70s to 90’s)
Total fear of
prescribing opioids
even in dying patients
No ceiling (mid 90’s – 2003-04)
Widespread use of
opioids using cancer
model of treatment
Opioid Opioid
Pendulum
Pain as the 5th VS
VHA in 98 ---- JC in 2000
Balance/Risk
Stratification
Opioids only one part of a
comprehensive multimodal
The good news is ….
We have 15 years of experience with expert clinical
guidelines for opioid management :
VA/DOD Practice Guidelines for Management of
Opioid Therapy for Chronic Pain, May 2010
Chronic disease management guidelines: arthritis, back pain,
fibromyalgia, chronic pain syndromes
VHA Stepped Care Model for Pain Care (VHA Directive
2009)
Research identifying populations of patients at risk for
poor outcomes when prescribed opioids
Recent Research Identifies Risk for
Inadvertent Opioid Drug Overdose
Substance Use Disorders
Depression, PTSD, Anxiety Disorder
Benzodiazepine Use
Underlying lung disease
Underlying liver disease
On 100 mg or more of Morphine equivalents per day
Patients over 65
Veterans Health Administration patients had nearly twice the rate of fatal accidental poisoning compared with adults in the general US population
Reference: # 1,2,3,4,5
Association of Mental Health Disorders With
Prescription Opioids and High-Risk Opioid Use in
US Veterans of Iraq and Afghanistan
Veterans with mental health issues were more likely to receive
opioids, about 3X as likely with PTSD, about 2X as likely with
other mental health issues
Veterans with PTSD were more likely to receive higher-dose
opioids, 2 or more opioids, sedative hypnotics, and get early
refills
Receiving opioids was associated with an adverse clinical
outcome for all veterans, more pronounced in veterans with
PTSD
Reference # 5
(N= 291,205 soldiers who entered VA 2005-2008)
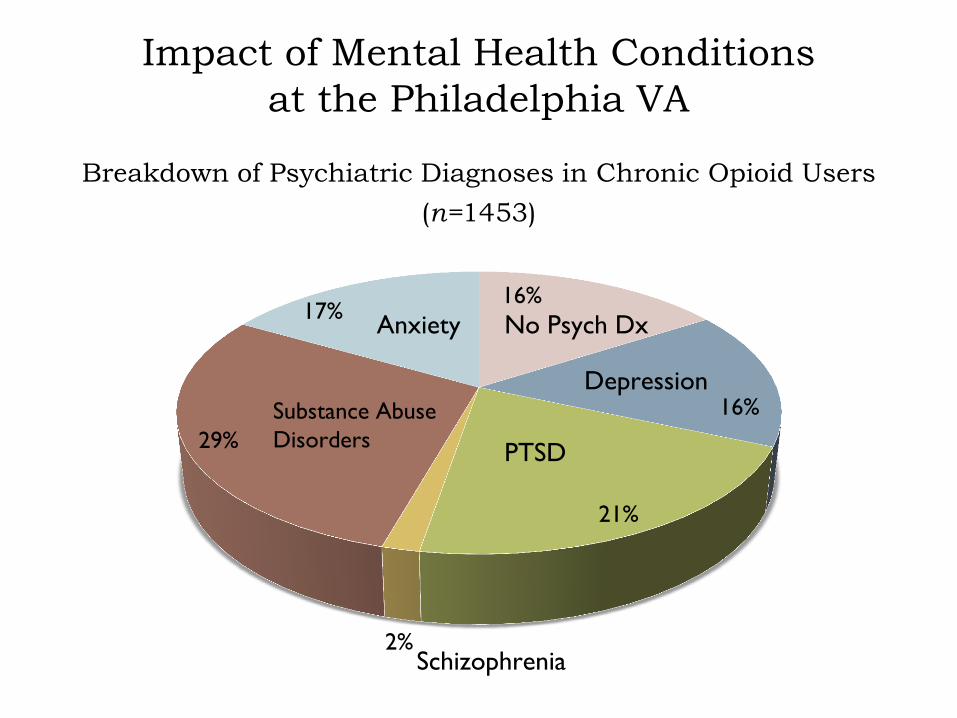
Impact of Mental Health Conditions
at the Philadelphia VA
Breakdown of Psychiatric Diagnoses in Chronic Opioid Users
(n=1453)
16%
16%
21%
2%
29%
17%
Substance Abuse
Disorders PTSD
Schizophrenia
No Psych Dx Anxiety
Depression
The good news is ….
CDC, FDA, DEA focus on Opioid Risk Mitigation Strategies
State Prescription Monitoring Programs
Functioning in NJ,WV, Ohio
PA: still 100% Law Enforcement;
Delaware: not fully operational yet
VHA
OIG will be examining VA facilities for policies for opioid prescribing. Focus is on protection from risks of long-term opioid therapy and misuse of opioids
Joint Commission Sentinel Event Alert
“Safe Opioid Prescribing in Hospitals” Issue 49, 8/8/12
Solutions for VISN 4
Opioid Risk Mitigation Strategies
≠ just decreasing opioids
GOAL to provide the best possible pain care
with opioids if indicated and
with safeguards against harm and abuse
Minimal to no
opioids
prescribed
Develop strategies in PC to
promote Consistent opioid
prescribing based on Expert
Guidelines
Strategies to standardize
and ease the workload
for opioid renewals
Prescribing
without
assessment of
risk factors
Continuing
opioids
without
monitoring
High dose
short-acting
opioids
#240 # 360
As a VISN/Facility/Individual prescriber,
we have to work together to move to the middle of the bell curve
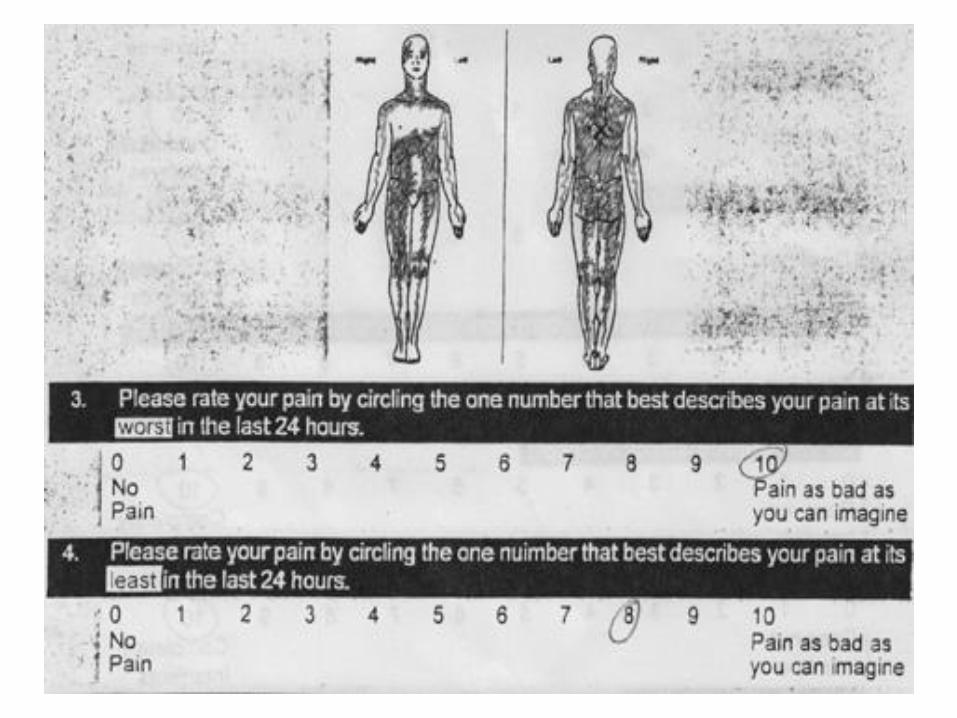
Routine screening for presence & intensity of pain
Comprehensive pain assessment
Management of common pain conditions
Support from MH-PC Integration, OEF/OIF, &
Post-Deployment Teams
Expanded care management
Opioid Renewal Pain Care Clinics
Pain Medicine
Rehabilitation Medicine
Behavioral Pain Management
Multidisciplinary Pain Clinics
SUD Programs
Mental Health Programs
Advanced pain medicine
diagnostics & interventions
CARF accredited pain
rehabilitation
STEP 1
STEP 2
STEP 3
VA Stepped Pain
Care
Complexity
Treatment Refractory
Comorbidities
RISK RISK
Surgical
Interventions
Advanced
Interventional
Long-Term Opioid
Therapy
Short-term / Short –acting Opioids
Non-opioid Pharmacological Therapy
Non-pharmacologic Therapy
Physical Therapy
Psychological/Activating Interventions
Lifestyle Change / Self-Management
Patient Education/Activation
Comprehensive Assessment - - - - - Identification/Treatment of Comorbidities
Biopsychosocial care: help the patient to make the connection
between psychosocial factors and physical pain
Treatment Approaches: the evidence
Evidence supports that there is a greater chance for
successful outcomes when the psychological components
of pain are treated with CBT, fear avoidance training and
interdisciplinary rehabilitation compared with
conventional medical interventions (IASP, January 2011)
Evidence that the attitude and message delivered by the
provider has a substantial effect on reports of pain relief
(Moerman & Jonas, Lancet,2003)
The message to your patient about
prolonged opioid treatment….
It was appropriate that your acute injury was treated with opioids BUT there is strong evidence that prolonged opioid therapy has significant long-term negative effects:
1. Endocrine dysfunction:
Decreased testosterone levels
Osteoporosis, fractures
Decreased libido
Decreased size of testes
Erectile dysfunction
Increased prolactin levels: Gynecomastia
Opioid-induced menopause
References: 7, 8
2. Tolerance develops overtime and increasing doses to high dose opioids is risky and has resulted in worse outcomes (Ballantyne,2003)
3. Opioid induced hyperalgesia – opioids can actually be a cause of increased pain
4. You are dependent on living your life around 30 day renewals which will affect you freedom in going away on vacations
5. Strong evidence that high doses increase risk of overdose, increase in health services utilization encounters for withdrawal, intoxication, overdose (Krebs et al, 2011; Bohnert et al, 2011;Gomes et al, 2011)
As the Primary Care Provider although it is difficult and likely not to be received well by the patient, you are emphasizing long term
treatment & the welfare of your patient
Case # 2
PMH: Type 2 Diabetes, HTN, Stage 2 Chronic Kidney Disease, ETOH abuse in sustained remission for 15 years, no psychiatric history, has had one prior back surgery, failed epidural injections
Social History: Worked as a police officer, retired at age 55, active in community, lives with wife and 2 daughters
Description of pain: achy throbbing pain in low back with episodic radiation of burning and numbness and tingling down backs of both legs
Pain diagnosis and pain generators: Spinal stenosis with episodic neurogenic claudication secondary to facet arthropathy and ligamentum flavum hypertophy causing central canal stenosis at L4-5 & L5-S1
62 yo male with chronic low back pain that started after being
thrown out a jeep in Viet Nam
Case # 2 Pain Management Regimen
PCP prescribed appropriate multimodal treatment
including:
Gabapentin, nortriptylline, capsaicin, TENS, follows HEP
from physical therapy, avoids NSAIDs due to CKD
Spine injections are no longer helpful
Percocet 5/325 for 3 years- has escalated to 8-10 tabs a
day(40-50 mg oxycodone /day)is no longer effective.
Patient states that it is not relieving his pain as well as in the
past and is only providing 2-3 hours of relief.
( Morphine is listed in allergy section “ cognitive impairment
and hallucination”)
Poll Question #2
Starting Methadone
Can cause QT prolongation at high doses but precaution with patients with concomitant cardioarrhythmic meds (i.e. TCAs) and history of arrhythmia or syncope
Protocol
EKG
before starting methadone
once the dose is stabilized
annually thereafter
additional monitoring if dose > 100mg /day or if unexplained syncope or seizures
QTc
If the QTc is > 450 but < 500 re-evaluate and discuss with the patient the potential risks and benefits of therapy and need for monitoring QTc more frequently
If QTc is > 500 don’t start discontinue (with a taper)
1.Methadone Guidelines from National Pain Management Strategy Committee Pharmacy Workgroup;
2.VA/DOD Guidelines,2010
Start low and go slow: 2.5 – 5 mg q 8 hours
If elderly or opioid naïve: q 12 or even q day
Increase dose as tolerated every 7 days
With close telephone contact
Provide short-acting opioids when starting if pain is severe
Instill FEAR: Patients must take exactly as prescribed, caution
them NOT to increase even if they think it is not working
Explain that methadone takes time, don’t expect that it will
relieve pain at starting dose
** Methadone is the only long-acting opioid that can be crushed
Starting Methadone
Methadone Cheat Sheet ☺ Start Low Go Slow
Opioid Tolerant Converting PO Morphine to Methadone:
Morphine < 200mg/day-use Methadone 5mg q 8 hours
Morphine 200-500mg/day-Use 7% of the Morphine equivalent divided doses q 8hrs
Determination of etiology requires thorough evaluation by
provider
VA/DOD Chronic Opioid Therapy CPG, 2010
ADRBs defined by VA/DOD CPG: Level I
Minor variations in adherence to prescribed med schedules
and other recommended treatments
Calling for early refills
Misplacing medications
Lending borrowing medications from friends/family
Marijuana, isolated nonprescribed opioid or benzo, isolated cocaine
with no or remote history of substance abuse
Management of Level 1 ADRBs in Primary Care
Education, re-review Treatment Agreement
Increase clinical structure for renewals – Opioid Renewal Clinic
Behavioral interventions
ADRBs defined by VA/DOD CPG: Level II
Behaviors that persistently demonstrate deviation from treatment agreement Frequently calling in for early refills, frequent reports of lost
prescriptions
Persistence of aberrant behaviors despite education and warnings
Represent serious co-morbidities Mood disorder
Personality disorder
PTSD
Addiction
Psychosis
Cognitive dysfunction
Management requires consultation or co-management with one or more specialists: pain management, mental health, addiction or may require discontinuation of opioids
ADRBs defined by VA/DOD CPG: Level III
Addiction: compulsive use of a substance resulting in physical, psychological and social harm to the user and continued use despite that harm (Rinaldi, RC JAMA 1988:259)
Illegal Criminal or dangerous behaviors
Management
Document, and offer referral to addiction treatment
Discuss nonopioid pharmacotherapy options
If there is clear unsafe or illegal behaviors, opioid prescribing should stop immediately and withdrawal should be addressed
In the setting of clear addiction, continuation of opioids for noncancer chronic pain will most likely be contraindicated
Minimal to no
opioids
prescribed
Develop strategies in PC to
promote Consistent opioid
prescribing based on Expert
Guidelines
Strategies to standardize
and ease the workload
for opioid renewals
Prescribing
without
assessment of
risk factors
Continuing
opioids
without
monitoring
High dose
short-acting
opioids
#240 # 360
As a VISN/Facility/Individual prescriber,
we have to work together to move to the middle of the bell curve
References
1.Dunn et al, Opioid Prescriptions for Chronic Pain and Overdose. Ann Int Med, 2010;152:85-92.
2. Gomes, et al Opioid Dose and Drug Related Mortality in Patients with Nonmalignant Pain. Arch Int Med, 2011;171(7):686-691.
3. Bohnert AS, Ilgen MA, Galea S et al. Accidental poisoning mortality among patients in the Department of
Veterans Affairs Health System. Med Care 2011;49:3936 4. Bohnert AS, Ilgen MA, Ignacio RV et al. Risk of death from accidental
overdose associated with psychiatric and substance use disorders. Am J Psychiatry 2012;169:64-70.
5.Bohnert AS, Valenstein M, Bair MJ et al. Association between opioid prescribing patterns and opioid overdose-related deaths. Jama 2011;305:1315-21
6.Seal, K et al. JAMA. 2012;307(9):940-947
References 7Rhodin, A., Stridsberg, M and Gordh, T. (2010) Opioid Endocrinopathy; A
clinical problem in patients With Chronic Pain and Longterm Oral Opioid
Treatment. Clinical Journal of Pain. 23(5), pp. 374-380.
8 Daniell, H.W. (2002) Hypogonadism in Men Consuming Sustained-
Action Oral Opioids. The Journal of Pain, 3(5), pp. 377-384.