DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1962, 4, 270-278 Chronic Progressive Communicating Hydrocephalus due to Protein Transudates from Brain and Spinal Tumours Phillip Harris CHRONIC progressive ‘communicating’ hydrocephalus occasionally occurs as a complication of brain or spinal neoplasms, it sometimes presents as a primary clinical syndrome in a patient with these lesions, or, it may occur secondarily to the commoner type of syndrome resulting directly from the brain or spinal tumour. In the first instance, the diagnosis of the neoplasm sometimes proves very difficult, as will be brought out in some of the examples discussed below. I t will be shown that the hydrocephalus is often due to chronic adhesive arachnoiditis and that this may result from an inflammatory reaction secondary to protein transudate from the neoplasm. case 1 A woman, aged 44 years. Dimness of vision and headache for 5 weeks. Referred by ophthalmologist because of bilateral papilloedema. No other neurological ab- normalities. Cerebrospinal fluid (CSF) : pressure 240 mm. of water, protein 222 mg./100 ml. Air ventriculography and lumbar air encephalography showed a marked degree of hydrocephalus with a large cisterna magna, and interpeduncular and chiasmatic cisterns; no air otherwise in subarachnoid spaces; no tumour demon- strated (Figs. 1 and 2). Air myelography, no evidence of spinal tumour. Operation, 6.10.55, theco-peritoneal CSF shunt. Dis- charged home on 8.11.55, when CSF protein was 180 mg./100 ml. Some months later re-admitted because of symptoms suggestive of intermittent raised intra- cranial pressure, but CSF pressure normal on lumbar puncture, with protein 220 mg./ 100 ml. Well until June 1959, when developed headaches, dizziness, ataxia, nystagmus and bilateral papilloedema. Lumbar air encephalography unsuccessful. A ‘Myodil‘ ventriculogram showed internal hydrocephalus and obstruction of intracranial subarachnoid pathways. Theco -peritoneal CSF shunt revised. Then developed low pressure headaches, and Spitz-Holter valve was therefore incor- porated in the theco-peritoneal shunt (1.10.59). Eventually developed evidence of raised intracranial pressure and deafness and nystagmus; new X-ray films of the skull showed enlargement of the left internal acoustic meatus. At operation on 27.10.59, a left acoustic neurilemmoma was totally excised. Thirty-six hours later Consultant Neurosurgeon, Department of Surgical Neurology, Western General Hospital, and Royal Infirmary, Edinburgh. 270
Transcript
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1962, 4, 270-278
Chronic Progressive Communicating Hydrocephalus due to Protein Transudates from
Brain and Spinal Tumours Phillip Harris
CHRONIC progressive ‘communicating’ hydrocephalus occasionally occurs as a complication of brain or spinal neoplasms, it sometimes presents as a primary clinical syndrome in a patient with these lesions, or, it may occur secondarily to the commoner type of syndrome resulting directly from the brain or spinal tumour. In the first instance, the diagnosis of the neoplasm sometimes proves very difficult, as will be brought out in some of the examples discussed below. It will be shown that the hydrocephalus is often due to chronic adhesive arachnoiditis and that this may result from an inflammatory reaction secondary to protein transudate from the neoplasm.
case 1 A woman, aged 44 years. Dimness of
vision and headache for 5 weeks. Referred by ophthalmologist because of bilateral papilloedema. No other neurological ab- normalities. Cerebrospinal fluid (CSF) : pressure 240 mm. of water, protein 222 mg./100 ml. Air ventriculography and lumbar air encephalography showed a marked degree of hydrocephalus with a large cisterna magna, and interpeduncular
and chiasmatic cisterns; no air otherwise in subarachnoid spaces; no tumour demon- strated (Figs. 1 and 2). Air myelography, no evidence of spinal tumour. Operation, 6.10.55, theco-peritoneal CSF shunt. Dis- charged home on 8.11.55, when CSF protein was 180 mg./100 ml. Some months later re-admitted because of symptoms suggestive of intermittent raised intra- cranial pressure, but CSF pressure normal on lumbar puncture, with protein 220 mg./ 1 0 0 ml. Well until June 1959, when developed headaches, dizziness, ataxia, nystagmus and bilateral papilloedema. Lumbar air encephalography unsuccessful. A ‘Myodil‘ ventriculogram showed internal hydrocephalus and obstruction of intracranial subarachnoid pathways. Theco -peritoneal CSF shunt revised. Then developed low pressure headaches, and Spitz-Holter valve was therefore incor- porated in the theco-peritoneal shunt (1.10.59). Eventually developed evidence of raised intracranial pressure and deafness and nystagmus; new X-ray films of the skull showed enlargement of the left internal acoustic meatus. At operation on 27.10.59, a left acoustic neurilemmoma was totally excised. Thirty-six hours later
Consultant Neurosurgeon, Department of Surgical Neurology, Western General Hospital, and Royal Infirmary, Edinburgh.
270
PHILLIP HARRIS
Fig. I . Combined air encephalogram and ventri- culogram showing communicating hydro- cephalus; lateral view.
Fig. 2. Combined air encephalogram and ventri- culogram showing communicating hydro- cephalus; A.P. view.
she developed bulbar nerve palsies and apnoea and she eventually died from bronchopneumonia. At autopsy no obvious cause for death was found on examination of the central nervous system. There was a terminal bronchopneumonia. The men- inges were thickened over the anterior aspect of the brain stem, cerebello-pontine angles and interpeduncular fossa. There was meningeal fibrosis and obstruction of the 4th ventricle exit foramina (Dr. J. W. Black).
Case 2 A woman, aged 51 years. Eight weeks’
history of typical features of right-sided acoustic neurilemmoma, with early papill- oedema. CSF: pressure 140 mm. water, total protein 160 mg./100 ml. A subtotal intracapsular excision of the neoplasm was performed. A month after operation the patient showed evidence of raised intra- cranial pressure. This was controlled initially by repeated lumbar punctures
and, two months after the craniectomy, by a thecoperitoneal CSF shunt. Seven months later, there was evidence of recurrence of raised intracranial pressure and she was studied by Myodil ventriculo- gram. This showed a marked degree of ‘communicating’ hydrocephalus, but there was no evidence of recurrence of neoplasm. At operation the tube for the theco-peritoneal anastomosis was found to be obstructed and was replaced. However, soon after this her condition steadily deteriorated and she died 9 months after the first operation. Autopsy showed evidence of basal leptomeningeal fibrosis, with hydrocephalus and there was brain stem impaction. The residium of the neoplasm was seen.
Comment. Case 1 illustrates that a patient with an acoustic neurilemmoma may present with a syndrome of ‘com- municating’ hydrocephalus. Case 2 demon- strates the point that these neoplasms
27 1
DEVELOPMENTAL MEDICINE AND
should, if at all possible, be completely excised because of the danger of the de- velopment of a chronic progressive hydro- cephalus from leptomeningeal fibrosis and also, of course, from regrowth of the neo- plasm. In 1954 Gardner et ul. discussed the production of increased intracranial pres- sure as a result of increased protein content in the CSF, in association with certain small intracranial and intraspinal tumours, and in the Guillain-BarrC syn- drome. They considered that in the production of papilloedema in their patients the chronicity of the process was more significant than the level of the protein concentration, and felt that the increased pressure was due to the piling up of the protein molecules against a blood-brain barrier, rather than to the increased osmotic tension of the protein- rich fluid. They subsequently attempted to produce papilloedema in a dog by repeated cisternal injections of human albumin and gamma globulin, but failed, they thought because the injected protein disappeared very rapidly from the CSF. In another experiment they showed that, in a test animal, the addition of autologous serum protein caused the rate of absorption of Ringer’s solution from the subarachnoid spaces to fall to approximately a quarter of the rate under control. No comment was made in their paper on the appearance of the arachnoid at suboccipital crani- ectomy. Shephard and Wadia (1956), when discussing atypical features in patients with acoustic neurilemmomas, des- cribe chronic progressive hydrocephalus in 6 patients. The main features were that the history was long (average 5 years) and the patients were in an old age group. The syndromes simulated a ‘frontal lobe lesion’. A study of the case-records shows that several of these patients had chronic adhesive arachnoiditis, which may have accounted for their chronic progressive hydrocephalus. See also Dott (1958).
272
CHILD NEUROLOGY. 1962, 4
Case 3 A man, aged 17 years. Six months’
history of headache, ataxia, diplopia and vomiting. Poor body and gonadal develop- ment, papilloedema, right facial palsy and inco-ordination of all limbs. CSF: pressure 300 mm. of water, total protein 70 mg./ 100 ml. Investigated further by air and Myodil ventriculography, and at opera- tion on 11.2.60 a large cystic glioma in the right cerebellar hemisphere was subtotally excised. The patient’s post- operative state was satisfactory except that he developed evidence of a ‘com- municating’ hydrocephalus. This required repeated lumbar puncture and then repeated lumbar drainage, and 2 months after the craniectomy a theco-peritoneal CSF anastomosis was carried out, incor- porating a Spitz-Holter valve to control intracranial pressure. The patient remains well.
The communicating hydrocephalus here may be a direct result of the neoplasm, or it could, in addition, be related to the operative procedure for excision of this tumour.
Case 4 A girl, aged 8 months. Normal birth.
Progressive hydrocephalus, right pupil dilated, right external rectus palsy, tone and reflexes increased in right limbs. CSF:
pressure 300mm. of water, total protein 75 mg./100 ml. Ventricular drainage. Ventricular CSF: total protein 47 mg./ I 0 0 ml. Very drowsy, rapidly became decerebrate and died within 48 hours of admission. Autopsy (Dr. K. Rhaney) showed marked basal leptomeningeal thickening and fibrosis; a few isolated small foci of choroid papilloma cells but no special leptomeningeal thickening in relation to these cells; symmetrical en- largement of the whole ventricular system. Papilloma of right choroid plexus in trigone region. Striking enlargement of
PHILLIP HARRIS
middle cerebral, interpeduncular, cere- bello-medullary and ambiens cisterns.
Case 5 A girl, aged 1 1 months. Progressive
hydrocephalus for several weeks. Early papilloedema, trunk ataxia, slight weak- ness or inco-ordination of limbs on left side and left abducent nerve palsy. CSF: total protein, 156 mg./100 ml. Posterior fossa exploratory operation showed marked distension of the cerebello-medul- lary cistern, and this was opened and eliminated. The child was well for a month, when the hydrocephalus recurred, necessitating ventricular drainage and ventriculography (Fig. 3), which showed
Fig. 3. Air ventriculogram, lateral view, showing severe degree of communicating hydro- cephalus.
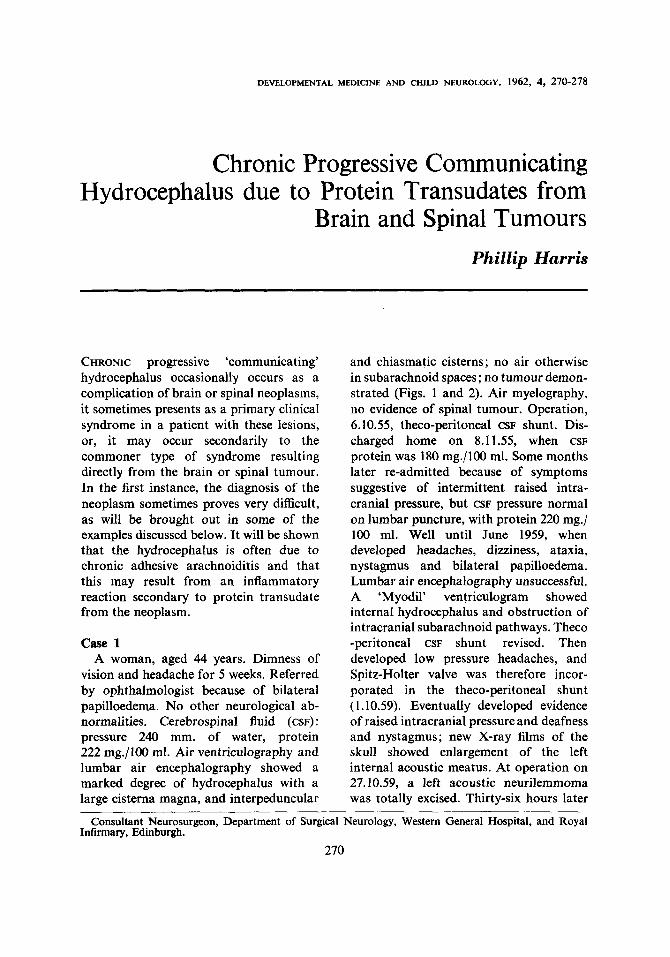
complete blockage of the basal sub- arachnoid spaces at the level of the inter- peduncular cistern, with severe hydro- cephalus. At operation on 30.1.55 a theco- peritoneal CSF shunt was carried out and the hydrocephalus was controlled for several weeks, but the child then began to vomit frequently, there was electrolyte imbalance and drowsiness, and she died on March 20, 1955. Autopsy (Dr. A. Le Roux) showed diffuse fibrous thickening of the basal leptomeninges (Figs. 4 and 5). There
Fig. 4. Base of brain showing severe lepto-
was a choroid plexus papilloma in the left lateral ventricle, 5 cm. in diameter but not obstructing the ventricular pathways. It lay in the occipital and trigonal areas (Fig. 6). The theco-peritoneal tube was patent. There were some very small groups of papilloma seedlings in the leptomeninges.
Comment. The association of communi- cating hydrocephalus with papillomas of the choroid plexus has been reported in several papers-e.g., Kahn and Luros 1952, Russell 1954, Harris 1956, Matson and Crofton 1960. Russell (1949) described the case of a baby aged 4!7 months who had a papilloma of the choroid plexus in a lateral ventricle associated with lepto- meningeal fibrosis and severe hydro- cephalus. At that time it was thought that the changes in the meninges were related to previous upper respiratory tract infec- tion and that the tumour was a coincidental
meningeal fibrosis.
273
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1962, 4
.Fig. 5. Sagittal section of brain in third ventricle region, demonstrating the leptorneningeal fibrosis.
Fig. 6. Sagittal section of brain showing the choroid plexus papilloma.
finding. In a subsequent communication (Russell 1954), the possibility of an excessive formation of CSF by these tumours was discussed and Dr. Russell described in detail the findings in a boy aged 10 months. Autopsy on this child showed granular ependymitis. It was considered that the low-grade inflam- matory character of the reaction strongly suggested the action of an irritant in the CSF and this was supported by the high protein content of the ventricular CSF. It was also suggested that a low-grade inflammatory process may well have extended to the basal leptomeninges. Smith (1955) mentions thickening and opacity of the basal leptomeninges in one patient. However, the reports by Kahn and Luros (1952) and by Matson (1953)
274
strongly suggest that the hydrocephalus resulted from excess production of CSF by the choroid plexus papilloma. Removal of such a tumour, or indeed, as will be mentioned later, of the offending spinal or other intracranial neoplasm which is associated with a communicating type of hydrocephalus, often results in the perma- nent disappearance of the hydrocephalus.
The mechanism here is not fully under- stood but one factor may be that protein from the lesion is no longer entering the CSF pathways. The hydrodynamics of such a process are difficult to understand. Even with the help of the electron microscope, radioactive isotopes and other techniques, such as electrophoresis, we are still very ignorant about the formation, circulation, absorption and indeed also the functions of the cerebrospinal fluid. It is interesting to note that Welch and Friedman (1960) have recently revived the suggestion of cerebrospinal fluid valves, made by Cushing in 1901. Foldes and Arrowood (1948) showed that 2,000 ml. of Ringer’s solution could be safely injected into the lumbar subarachnoid space in adults within a period of 24 hours. One would expect that the absorptive apparatus for cerebrospinal fluid could cope with all but the highest increase in demand made on it. Of the 16 cases described by Matson and Crofton (1960), the CSF total protein was raised in 13 (whether from the lumbar region or a lateral ventricle), and in fact it was over 100 mg./100 ml. in 10 cases, and in some was as high as 500 mg./100 ml.
The type of hydrocephalus described above accompanies only about 50 per cent of choroid plexus papillomas in the lateral ventricle (Braunstein and Martin 1952); and so far there is no histological criterion for distinguishing the over-active type from the more inert type of choroid plexus papilloma. Full X-ray and pathological studies, including investigations of the leptomeninges, are not yet available for a
PHILLIP HARRIS
large number of patients with these tumours and we have much to learn from them. If they occur in the 3rd or 4th ventricles and cause an ‘obstructive’ type of hydrocephalus, should hydrocephalus also develop distal to the tumour because of excess formation of cerebrospinal fluid? Mortensen and Weed (1933) showed that the rate of absorption of the CSF is directly proportional to its pressure, so long as pathways by which absorption takes place remain patent. (CSF pressure is eventually regulated by the absorption of CSF.) Hassin (1930) described a child with absence of the choroid plexuses who had an occluded aqueduct, and who developed hydrocephalus. In the patient described by Kahn and Luros (1952) there was a symmetrical dilatation of the ven- tricles and an enlarged cisterna magna, and air extended as far forwards as the cisterna interpeduncularis, which was small, but there was no air beyond this. It is possible that haemorrhage might occur from neoplasms, either spontaneously or/ and as a result of operative treatment, and this might incite some degree of lepto- meningeal fibrosis (Bagley 1929, Russell 1949, Dott 1950, Kibler et af. 1961). However, one would presumably expect microscopic changes showing incorpora- tion of haemosiderin in the thickened leptomeninges in these patients. Matson (1953) and Bering (1955) felt that a choroid plexus papilloma might produce dilatation of the ventricular system by the presence of a large pulsating intraventricular mass.
Case 6 A woman, aged 31 years. Seven years’
history of backache and leg pains. De- veloped foot-drop after lumbar puncture. Memory defect for one year. Four months history of headaches, dizziness and occas- ional vomiting. Examination showed papilloedema, right abducent nerve palsy and fine nystagmus on looking to the left.
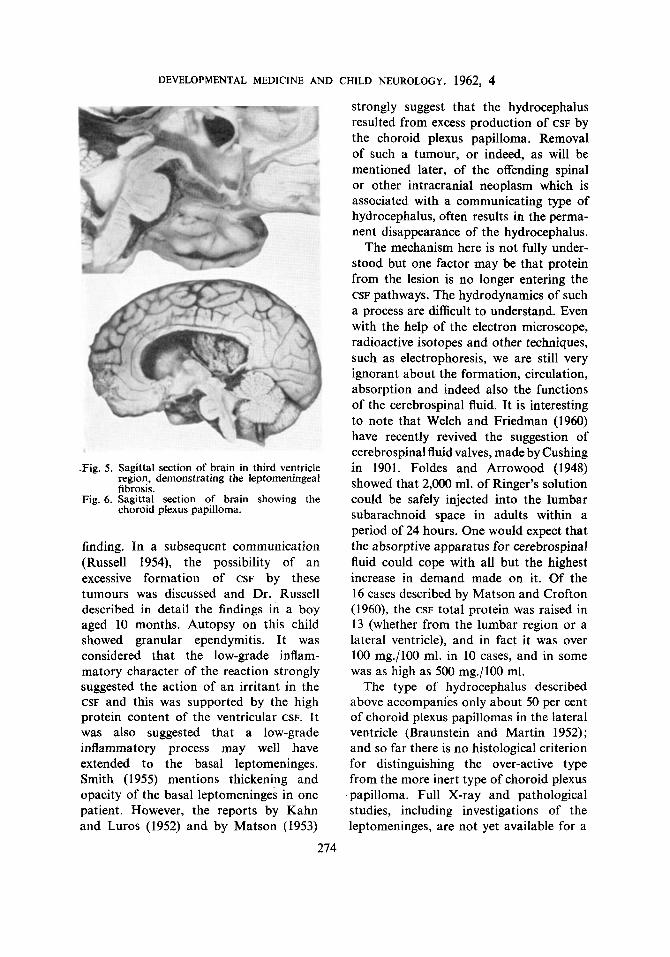
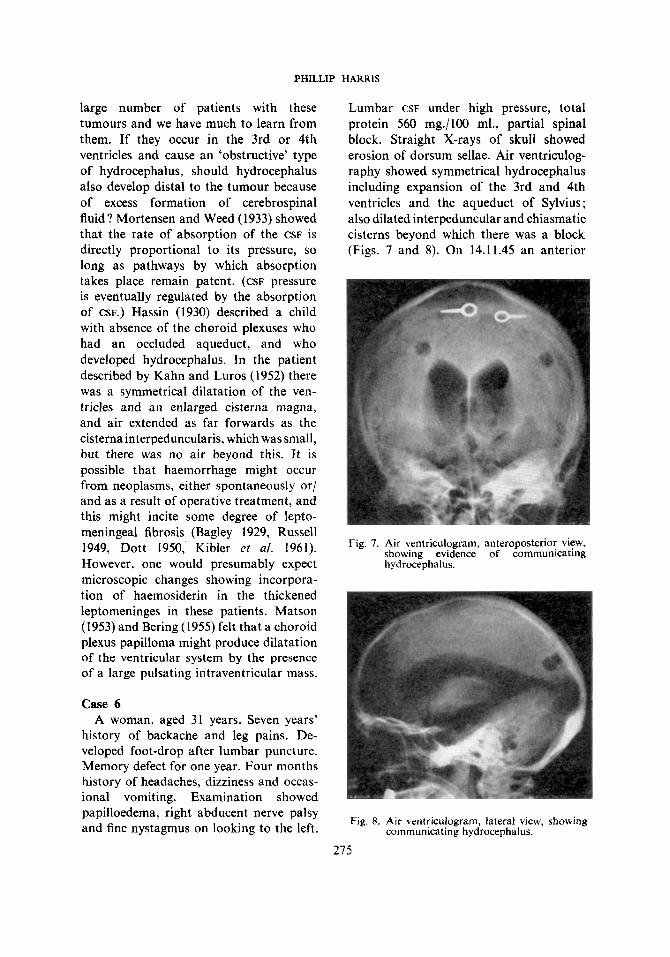
Lumbar CSF under high pressure, total protein 560 mg./100 ml., partial spinal block. Straight X-rays of skull showed erosion of dorsum sellae. Air ventriculog- raphy showed symmetrical hydrocephalus including expansion of the 3rd and 4th ventricles and the aqueduct of Sylvius; also dilated interpeduncular and chiasmatic cisterns beyond which there was a block (Figs. 7 and 8). On 14.11.45 an anterior
Fig. 7. Air ventriculogram, anteroposterior view, showing evidence of communicating hydrocephalus.
Fig. 8. Air ventriculogram, lateral view, showing communicating hydrocephalus.
215
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1962, 4
3rd ventriculostomy was performed. How- ever, the hydrocephalus continued, and on 10.12.45 a subtemporal decompression was done on both sides. The brain bulged and the arachnoid was thickened. The patient remained drowsy and confused and died on 31.12.45. Autopsy (Dr. W. Blackwood) showed a chronic inflam- matory basal adhesive arachnoiditis with chronic hydrocephalus. The 3rd ventricu- lostomy appeared to be patent. There was a spinal conus medullaris ependyrnoma measuring 74 x 28 x 20 mm., centred at about L5 level (Fig. 9). Microscopic
Fig. 9. Conus medullaris and cauda equina, s h o w i n g t h e e p e n d y m o m a (bisected).
examination showed haemosiderin in phagocytes and thickened arachnoid in- corporated in the layers of surface cerebral leptomeninges and in the superficial layers of the cortex.
276
Comment. It is known that chronic progressive hydrocephalus occasionally appears as a complication of certain spinal tumours. Love et al. (1951), describing this association in two patients who had a cauda equina ependymoma, noted that a t cervico-dorsal exploration there was fibrous thickening of the arachnoid. Teng et af. (1960) described 11 cases from the literature and added one of their own. The total protein of the ventricular or cisternal CSF was raised in four of these patients. Eleven of the neoplasms were glial, seven being ependymomas, and one was a neurofibroma. The main clinical features were impaired visual acuity, papilloedema, headache, vertigo and vomiting. Eight of the tumours were in the dorso-lumbar region. The increased protein content of the CSF was thought to play an important part in the production of hydrocephalus in these patients (see also Gardner et a/. 1954 and Schaltenbrand 1953).
It is of interest and importance to consider certain other conditions where raised intracranial pressure and papill- oedema may develop and where the CSF protein is raised. For example, the Guillain-Barrt syndrome, peripheral neuritis and poliomyelitis (Drew and Magee 1951, Weinman et a/. 1951, Denny-Brown 1952, Gardner et af. 1954). Joynt (1958) does not accept the view that excessive protein in the CSF blocks its absorption by the arachnoidal villi. He suggests that papilloedema may occur in the Guillain-Barre syndrome as a result of cerebral oedema similar to that occur- ring in ‘pseudo-tumour cerebri’. However, it is necessary to take into account the findings obtained on lumbar air encephal- ography and ventriculography, the response to repeated lumbar punctures and lumbar drainage in many of these patients, and the response to such procedures as spinal theco-peritoneal shunts.
PHILLIP HARRIS
Conclusions Chronic progressive communicating
hydrocephalus is a rare complication of certain brain and spinal tumours but the diagnosis should always be considered in patients such as those described above. That is, with certain intracranial neoplasms and in particular acoustic neuromas and choroid plexus papillomas; and in certain spinal tumours, in particular ependy- momas in the dorso-lumbar region. In this respect there are certain investigations which are particularly valuable, especially lumbar air encephalography and myelog- raphy. Careful audiometry and caloric tests may pick up an early acoustic neurilemmoma. Electrophoretic examina- tion of CSF proteins may provide some information in the future regarding the possible aetiology of this syndrome. Every opportunity should be taken to examine the leptomeninges at operation in these cases and certainly very careful studies should be made of the spine and head if any of these patients come to autopsy.
Regarding possible causation, it is felt that protein transudates from these neo- plasms may cause an inflammatory reac- tion, particularly involving the basal leptomeninges. This appears to be an individual response, possibly allergic. Others feel that the blood-brain barrier may become clogged with the protein molecules, or with the increased viscosity of the CSF there will be less tendency for
this fluid to be absorbed. Certain papil- lomas of the choroid plexus may cause excess production of cerebrospinal fluid. Some of these neoplasms may bleed into the subarachnoid spaces and cause lepto- meningeal fibrosis and communicating hydrocephalus. This may also happen in ‘spontaneous’ subarachnoid haemorrhage (Foltz and Ward 1956, Kibler et al. 1961, Harris 1961). Rarely, carcinomatosis of the meninges (Heathfield and Williams 1956) may result in a communicating type of hydrocephalus; and it is possible that a tumour may produce this syndrome by blockage or deformation or thrombosis of the larger venous sinuses in the head.
Regarding treatment, in the first place, the complication may be prevented by early and complete excision of these tumours; secondly, it is possible that the early use of corticosteroids may prevent or limit the development of communicating hydrocephalus with these neoplasms. The condition may respond wellin some patients to repeated lumbar punctures or to lumbar drainage, while others, as are described above, require short-circuiting procedures such as spinal theco peritoneal CSF shunts so that the CSF may be diverted and absorbed outside the cranial and spinal cavities.
Ackno~ledger~zeiits. I wish to thank Professor Dott for allowing me to include some of his cases as examples in this paper, and Dr. David Lees for his help in assembling the material.
REFERENCES
Bagley, C. Jr. (1929) ‘Functional and organic alterations following the introduction of blood into the
Bering, E. A. Jr. (1955) ‘Choroid plexus an darterial pulsation of cerebrospinal fluid.’ Arch. Neitrol. fsychiar.
Braunstein, H. , Martin, F. Jr. (1952) ‘Congenital papilloma of choroid plexus.’ Arch. NeitroI. Psychjar.
Denny-Brown, D. E. (1952) ‘Shattuck lecture: changing pattern of neurclagic medicine.’ N e w Engl. J . Med.,
Dott, N. M. (1950) ‘A contribution to the surgery of hydrocephalus in childhood.’ 6th. Internat. Congr.
~ (1958) ‘Chronic arachnoiditis and hydrocephalus in the surgical management of acoustic tumours. A
Drew, A. L., Magce, K . R . (I95 I ) ‘Papilledema in Guilhin-Bdrrk syndrome.‘ Arch. N e i t r d . f ~ y c h i u t . (Chic.),
277
cerebrospinal fluid.’ In: Res. Pub/. Ass. nerv. ment. Dis., 8,217-244.
(Chic.), 73, 165-172.
(Chic.), 68, 475480.
246,839-846.
Pediat. Zurich, 1950, Summaries of communications. Vol. IT, p. 191.
plea for early operation.’ froc. roy. Soc. Med., 51, 897-898.
66,744-75 I .
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1962, 4
Foldes, F. R., Arrowood, J. G. (1948) ‘Changes in cerebrospinal fluid pressure under influence of continuous subarachnoid infusion of normal saline.’J. clin. Invest., 27,346-351.
Foltz, E. L., Ward, A. A. Jr. (1956) ‘Communicating hydrocephalus from subarachnoid bleeding.’ J. Neuro- surg., 13,546566.
Gardner, W. J., Spitler, D. K., Whitten, C. (1954) ‘Increased intracranial pressure caused by increased protein content in cerebrospinal fluid: explanation of papilledema in certain cases of small intracranial and intraspinal tumors, and in Guillain-Barre syndrome.’ New Engl. J. Med., 250,932-936.
Harris, P. (1956) ‘Hydrocephalus associated with small papillomas of the choroid plexus.’ Paper read at Royal Society of Medicine Neurology Section. May 3, 1956.
Harris, P. (1961) Cincinn. J. Med., 42, 1 . Hassin, G. B. (1930) ‘Hydrocephalus; studies of pathology and pathogenesis, with remarks on cerebrospinal
fluid.’ Arch. Neurol. Psychiat. (Chic.), 24,1164-1186. Heathfield, K. W. G., Williams, J. R. B. (1956) ‘Carcinomatosis of the meninges: some clinical and patho-
logical aspects. Brir. med. J., 1,328-330. Joynt, R. J. (1958) ‘Mechanism of production of papilledema in the Guillain-Barre syndrome.’ Neurology, 8,
Kahn, E. A., Luros, J. T. (1952) ‘Hydrocephalus from over-production of cerebrospinal fluid (and experiences
Kibler, R. F., Couch, R. S. C., Crompton, M. R. (1961) ‘Hydrocephalus in the adult following spontaneous
Love, J. G., Wagener, H. P., Woltman, H. W. (1951) ‘Tumors of spinal cord associated with choking of
Matson, D. D. (1953) ‘Hydrocephalus in premature infant caused by papilloma of choroid plexus with
- Crofton, F. D. L., (1960) ‘Papilloma of the choroid plexus in childhood.’ J . Neurosurg., 17, 1002-1027. Mortensen. 0. A.. Weed. L. H. (1934) ‘Absorption of isotonic fluids from subarachnoid space.’ Amer. J.
8-12.
with other papillomas of choroid plexus.)’ J. Neurosurg., 9,59-67.