Circulating CD21 low B cells in common variable immunodeficiency resemble tissue homing, innate-like B cells Mirzokhid Rakhmanov a,b , Baerbel Keller a,b,1 , Sylvia Gutenberger a,b,1 , Christian Foerster a,b , Manfred Hoenig c , Gertjan Driessen d , Mirjam van der Burg d , Jacques J. van Dongen d , Elisabeth Wiech e , Marcella Visentini f , Isabella Quinti f , Antje Prasse g , Nadine Voelxen a,b , Ulrich Salzer b , Sigune Goldacker b , Paul Fisch e , Hermann Eibel b , Klaus Schwarz h , Hans-Hartmut Peter a,b , and Klaus Warnatz a,b,2 a Centre of Chronic Immunodeficiency and b Division of Rheumatology and Clinical Immunology, University Medical Center Freiburg, 79106 Freiburg, Germany; c Children’s Hospital, University Hospital Ulm, 89075 Ulm, Germany; d Department of Immunology, Erasmus University Medical Center, 3015 GE Rotterdam, The Netherlands; e Institute for Pathology, University Medical Center Freiburg, 79106 Freiburg, Germany; f Department of Clinical Immunology, University of Rome La Sapienza, 00185 Rome, Italy; g Department of Pneumology, University Medical Center Freiburg, 79106 Freiburg, Germany; and h Institute for Transfusion Medicine, University of Ulm and Institute of Clinical Transfusion Medicine and Immunogenetics Ulm, 89081 Ulm, Germany Edited by Dennis A. Carson, University of California at San Diego School of Medicine, La Jolla, CA, and approved June 23, 2009 (received for review February 24, 2009) The homeostasis of circulating B cell subsets in the peripheral blood of healthy adults is well regulated, but in disease it can be severely disturbed. Thus, a subgroup of patients with common variable immunodeficiency (CVID) presents with an extraordinary expan- sion of an unusual B cell population characterized by the low expression of CD21. CD21 low B cells are polyclonal, unmutated IgM IgD B cells but carry a highly distinct gene expression profile which differs from conventional naı ¨ve B cells. Interestingly, while clearly not representing a memory population, they do share several features with the recently defined memory-like tissue, Fc receptor-like 4 positive B cell population in the tonsils of healthy donors. CD21 low B cells show signs of previous activation and proliferation in vivo, while exhibiting defective calcium signaling and poor proliferation in response to B cell receptor stimulation. CD21 low B cells express decreased amounts of homeostatic but increased levels of inflammatory chemokine receptors. This might explain their preferential homing to peripheral tissues like the bronchoalveolar space of CVID or the synovium of rheumatoid arthritis patients. Therefore, as a result of the close resemblance to the gene expression profile, phenotype, function and preferential tissue homing of murine B1 B cells, we suggest that CD21 low B cells represent a human innate-like B cell population. B cell differentiation CVID O nly certain subsets of B cells can be found in the peripheral blood of healthy human adults. Usually, between 5080% of the circulating B cells belong to the CD27 negative pool, including naı ¨ve B cells and up to 4% transitional B cells. The remaining B cells comprise CD27 IgM IgD marginal zone (MZ)-like B cells, very few CD27 IgM IgD (‘‘IgM-only’’) B cells, and CD27 IgM IgD class switched memory B cells (1). This peripheral B cell homeostasis is severely disturbed in patients with common variable immunodeficiency (CVID) (2– 4). Flow cytometric analysis identified the expansion of an unusual B cell subset in CVID patients characterized by its very low expression of CD21 (complement receptor 2, CR2) (5). Since it was difficult to assign this unusual population to a known stage of B cell differentiation, we designated them as CD21 low B cells (5). CD21 low B cells are surface IgM positive, express elevated levels of CD19 (5), low levels of CD38 (3), chemokine receptors CXCR5 and CCR7, and no CD23 (6); this marker profile clearly discriminates them from other B cell subpopula- tions. The expansion of CD21 low B cells correlates well with the presence of splenomegaly and granulomatous disease in CVID (2). In addition, expanded numbers of CD21 low B cells have been found in patients with systemic lupus erythematosus (SLE) (7) and in viremic HIV patients but not in HIV patients without viremia (8). So far, the origin and role of these B cells has remained elusive. A new facet was added to the context when CD21 low B cells in HIV patients were identified as an Fc receptor-like 4 (FCRL4 ) dysfunctional memory B cell population (9). Originally, FCRL4, also named immunoreceptor superfamily translocation- associated 1 (IRTA1) was identified as a marker for a CD27 positive (10) or negative (11) memory B cell population in the human tonsil. This B cell subset was assigned to the memory fraction because it lacks IgD and CD38 expression, has a high proportion of class switched B cells and an increase in somatic hypermutation (11). It consists of large lymphocytes expressing increased levels of activation markers CD69, CD80, and CD86. Recently, Ehrhardt et al. (12) found by microarray analysis a distinct gene expression profile in FCRL4 B cells compared to conventional memory B cells. Here we report the extended phenotype, function and gene expression profile of CD21 low B cells in patients with CVID revealing a resemblance to innate-like B cells in mice. Results Phenotypic Characterization of CD21 low B Cells Reveals a Distinct IgM IgD Activated B Cell Subset. The relative expansion of CD21 low B cells above 20% of the total B cell count has been used in the Freiburg classification to classify CVID patients as type Ia (2). The analysis of 81 CVID patients (supporting information (SI) Table S1) of the Freiburg cohort showed an increase of CD21 low B cells both percentage-wise and in absolute numbers in CVID Ia patients compared to non-Ia patients and healthy donors (HD) (30 30 cells/l vs. 4 4 cells/l, P 0.0004). To more precisely define the phenotype of this expanded Author contributions: H.-H.P. and K.W. designed research; M.R., B.K., S. Gutenberger, C.F., M.H., G.D., M.v.d.B., E.W., M.V., N.V., and U.S. performed research; M.R., J.J.v.D., I.Q., A.P., U.S., S. Goldacker, P.F., H.E., K.S., and K.W. analyzed data; and M.R. and K.W. wrote the paper. The authors declare no conflict of interest. This article is a PNAS Direct Submission. Data deposition: The data reported in this paper have been deposited in the Gene Expression Omnibus (GEO) database, www.ncbi.nlm.nih.gov/geo (accession no. GSE17269). 1 B.K. and S.G. contributed equally to this work. 2 To whom correspondence should be addressed. E-mail: klaus.warnatz@uniklinik- freiburg.de. This article contains supporting information online at www.pnas.org/cgi/content/full/ 0901984106/DCSupplemental. www.pnas.orgcgidoi10.1073pnas.0901984106 PNAS August 11, 2009 vol. 106 no. 32 13451–13456 IMMUNOLOGY
Transcript
Circulating CD21low B cells in common variableimmunodeficiency resemble tissue homing,innate-like B cellsMirzokhid Rakhmanova,b, Baerbel Kellera,b,1, Sylvia Gutenbergera,b,1, Christian Foerstera,b, Manfred Hoenigc,Gertjan Driessend, Mirjam van der Burgd, Jacques J. van Dongend, Elisabeth Wieche, Marcella Visentinif, Isabella Quintif,Antje Prasseg, Nadine Voelxena,b, Ulrich Salzerb, Sigune Goldackerb, Paul Fische, Hermann Eibelb, Klaus Schwarzh,Hans-Hartmut Petera,b, and Klaus Warnatza,b,2
aCentre of Chronic Immunodeficiency and bDivision of Rheumatology and Clinical Immunology, University Medical Center Freiburg, 79106 Freiburg,Germany; cChildren’s Hospital, University Hospital Ulm, 89075 Ulm, Germany; dDepartment of Immunology, Erasmus University Medical Center, 3015 GERotterdam, The Netherlands; eInstitute for Pathology, University Medical Center Freiburg, 79106 Freiburg, Germany; fDepartment of Clinical Immunology,University of Rome La Sapienza, 00185 Rome, Italy; gDepartment of Pneumology, University Medical Center Freiburg, 79106 Freiburg, Germany;and hInstitute for Transfusion Medicine, University of Ulm and Institute of Clinical Transfusion Medicine and Immunogenetics Ulm, 89081 Ulm, Germany
Edited by Dennis A. Carson, University of California at San Diego School of Medicine, La Jolla, CA, and approved June 23, 2009 (received for reviewFebruary 24, 2009)
The homeostasis of circulating B cell subsets in the peripheral bloodof healthy adults is well regulated, but in disease it can be severelydisturbed. Thus, a subgroup of patients with common variableimmunodeficiency (CVID) presents with an extraordinary expan-sion of an unusual B cell population characterized by the lowexpression of CD21. CD21low B cells are polyclonal, unmutatedIgM�IgD� B cells but carry a highly distinct gene expression profilewhich differs from conventional naı̈ve B cells. Interestingly, whileclearly not representing a memory population, they do shareseveral features with the recently defined memory-like tissue, Fcreceptor-like 4 positive B cell population in the tonsils of healthydonors. CD21low B cells show signs of previous activation andproliferation in vivo, while exhibiting defective calcium signalingand poor proliferation in response to B cell receptor stimulation.CD21low B cells express decreased amounts of homeostatic butincreased levels of inflammatory chemokine receptors. This mightexplain their preferential homing to peripheral tissues like thebronchoalveolar space of CVID or the synovium of rheumatoidarthritis patients. Therefore, as a result of the close resemblance tothe gene expression profile, phenotype, function and preferentialtissue homing of murine B1 B cells, we suggest that CD21low B cellsrepresent a human innate-like B cell population.
B cell differentiation � CVID
Only certain subsets of B cells can be found in the peripheralblood of healthy human adults. Usually, between 50�80%
of the circulating B cells belong to the CD27 negative pool,including naı̈ve B cells and up to 4% transitional B cells. Theremaining B cells comprise CD27�IgM�IgD� marginal zone(MZ)-like B cells, very few CD27� IgM�IgD� (‘‘IgM-only’’) Bcells, and CD27�IgM�IgD� class switched memory B cells (1).This peripheral B cell homeostasis is severely disturbed inpatients with common variable immunodeficiency (CVID) (2–4). Flow cytometric analysis identified the expansion of anunusual B cell subset in CVID patients characterized by its verylow expression of CD21 (complement receptor 2, CR2) (5).Since it was difficult to assign this unusual population to a knownstage of B cell differentiation, we designated them as CD21low Bcells (5). CD21low B cells are surface IgM positive, expresselevated levels of CD19 (5), low levels of CD38 (3), chemokinereceptors CXCR5 and CCR7, and no CD23 (6); this markerprofile clearly discriminates them from other B cell subpopula-tions. The expansion of CD21low B cells correlates well with thepresence of splenomegaly and granulomatous disease in CVID(2). In addition, expanded numbers of CD21low B cells have beenfound in patients with systemic lupus erythematosus (SLE) (7)
and in viremic HIV patients but not in HIV patients withoutviremia (8).
So far, the origin and role of these B cells has remained elusive.A new facet was added to the context when CD21low B cells inHIV patients were identified as an Fc receptor-like 4 (FCRL4�)dysfunctional memory B cell population (9). Originally, FCRL4,also named immunoreceptor superfamily translocation-associated 1 (IRTA1) was identified as a marker for a CD27positive (10) or negative (11) memory B cell population in thehuman tonsil. This B cell subset was assigned to the memoryfraction because it lacks IgD and CD38 expression, has a highproportion of class switched B cells and an increase in somatichypermutation (11). It consists of large lymphocytes expressingincreased levels of activation markers CD69, CD80, and CD86.Recently, Ehrhardt et al. (12) found by microarray analysis adistinct gene expression profile in FCRL4� B cells compared toconventional memory B cells.
Here we report the extended phenotype, function and geneexpression profile of CD21low B cells in patients with CVIDrevealing a resemblance to innate-like B cells in mice.
ResultsPhenotypic Characterization of CD21low B Cells Reveals a DistinctIgM�IgD� Activated B Cell Subset. The relative expansion ofCD21low B cells above 20% of the total B cell count has beenused in the Freiburg classification to classify CVID patients astype Ia (2). The analysis of 81 CVID patients (supportinginformation (SI) Table S1) of the Freiburg cohort showed anincrease of CD21low B cells both percentage-wise and inabsolute numbers in CVID Ia patients compared to non-Iapatients and healthy donors (HD) (30 � 30 cells/�l vs. 4 � 4cells/�l, P � 0.0004).
To more precisely define the phenotype of this expanded
Author contributions: H.-H.P. and K.W. designed research; M.R., B.K., S. Gutenberger, C.F.,M.H., G.D., M.v.d.B., E.W., M.V., N.V., and U.S. performed research; M.R., J.J.v.D., I.Q., A.P.,U.S., S. Goldacker, P.F., H.E., K.S., and K.W. analyzed data; and M.R. and K.W. wrote thepaper.
The authors declare no conflict of interest.
This article is a PNAS Direct Submission.
Data deposition: The data reported in this paper have been deposited in the GeneExpression Omnibus (GEO) database, www.ncbi.nlm.nih.gov/geo (accession no. GSE17269).
1B.K. and S.G. contributed equally to this work.
2To whom correspondence should be addressed. E-mail: [email protected].
This article contains supporting information online at www.pnas.org/cgi/content/full/0901984106/DCSupplemental.
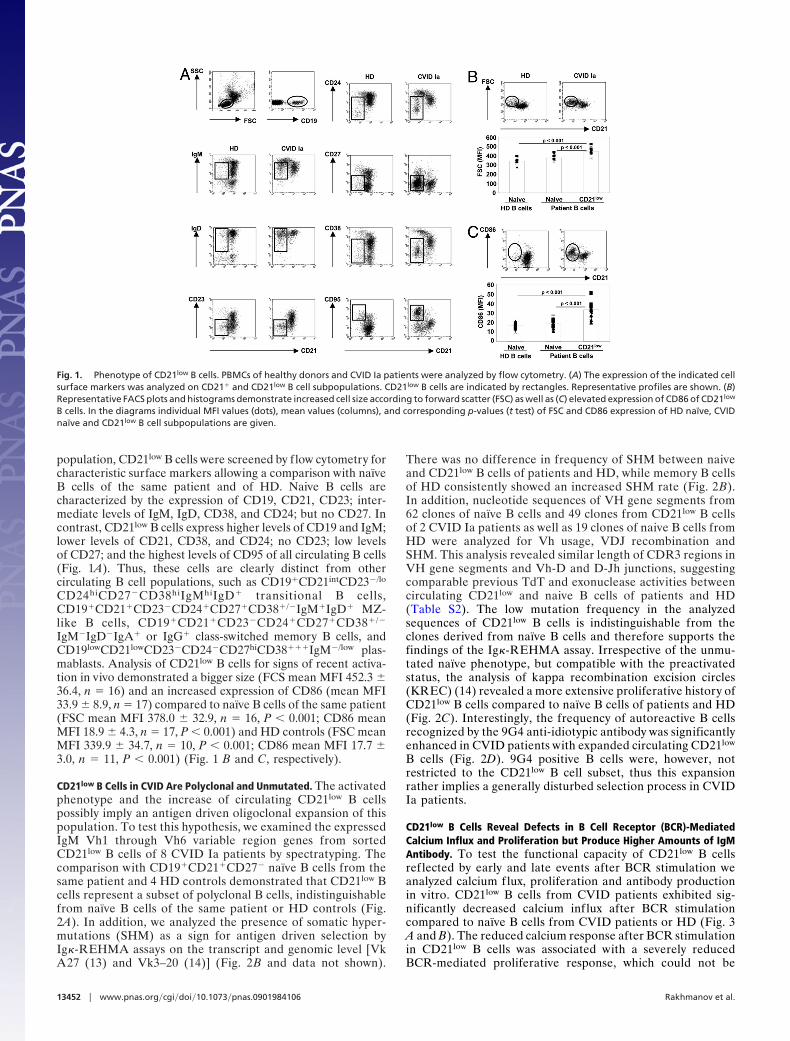
population, CD21low B cells were screened by flow cytometry forcharacteristic surface markers allowing a comparison with naı̈veB cells of the same patient and of HD. Naive B cells arecharacterized by the expression of CD19, CD21, CD23; inter-mediate levels of IgM, IgD, CD38, and CD24; but no CD27. Incontrast, CD21low B cells express higher levels of CD19 and IgM;lower levels of CD21, CD38, and CD24; no CD23; low levelsof CD27; and the highest levels of CD95 of all circulating B cells(Fig. 1A). Thus, these cells are clearly distinct from othercirculating B cell populations, such as CD19�CD21intCD23�/lo
CD24hiCD27�CD38hiIgMhiIgD� transitional B cells,CD19�CD21�CD23�CD24�CD27�CD38�/�IgM�IgD� MZ-like B cells, CD19�CD21�CD23�CD24�CD27�CD38�/�
IgM�IgD�IgA� or IgG� class-switched memory B cells, andCD19lowCD21lowCD23�CD24�CD27hiCD38���IgM�/low plas-mablasts. Analysis of CD21low B cells for signs of recent activa-tion in vivo demonstrated a bigger size (FCS mean MFI 452.3 �36.4, n � 16) and an increased expression of CD86 (mean MFI33.9 � 8.9, n � 17) compared to naı̈ve B cells of the same patient(FSC mean MFI 378.0 � 32.9, n � 16, P � 0.001; CD86 meanMFI 18.9 � 4.3, n � 17, P � 0.001) and HD controls (FSC meanMFI 339.9 � 34.7, n � 10, P � 0.001; CD86 mean MFI 17.7 �3.0, n � 11, P � 0.001) (Fig. 1 B and C, respectively).
CD21low B Cells in CVID Are Polyclonal and Unmutated. The activatedphenotype and the increase of circulating CD21low B cellspossibly imply an antigen driven oligoclonal expansion of thispopulation. To test this hypothesis, we examined the expressedIgM Vh1 through Vh6 variable region genes from sortedCD21low B cells of 8 CVID Ia patients by spectratyping. Thecomparison with CD19�CD21�CD27� naı̈ve B cells from thesame patient and 4 HD controls demonstrated that CD21low Bcells represent a subset of polyclonal B cells, indistinguishablefrom naı̈ve B cells of the same patient or HD controls (Fig.2A). In addition, we analyzed the presence of somatic hyper-mutations (SHM) as a sign for antigen driven selection byIg�-REHMA assays on the transcript and genomic level [VkA27 (13) and Vk3–20 (14)] (Fig. 2B and data not shown).
There was no difference in frequency of SHM between naiveand CD21low B cells of patients and HD, while memory B cellsof HD consistently showed an increased SHM rate (Fig. 2B).In addition, nucleotide sequences of VH gene segments from62 clones of naı̈ve B cells and 49 clones from CD21low B cellsof 2 CVID Ia patients as well as 19 clones of naive B cells fromHD were analyzed for Vh usage, VDJ recombination andSHM. This analysis revealed similar length of CDR3 regions inVH gene segments and Vh-D and D-Jh junctions, suggestingcomparable previous TdT and exonuclease activities betweencirculating CD21low and naive B cells of patients and HD(Table S2). The low mutation frequency in the analyzedsequences of CD21low B cells is indistinguishable from theclones derived from naı̈ve B cells and therefore supports thefindings of the Ig�-REHMA assay. Irrespective of the unmu-tated naı̈ve phenotype, but compatible with the preactivatedstatus, the analysis of kappa recombination excision circles(KREC) (14) revealed a more extensive proliferative history ofCD21low B cells compared to naı̈ve B cells of patients and HD(Fig. 2C). Interestingly, the frequency of autoreactive B cellsrecognized by the 9G4 anti-idiotypic antibody was significantlyenhanced in CVID patients with expanded circulating CD21low
B cells (Fig. 2D). 9G4 positive B cells were, however, notrestricted to the CD21low B cell subset, thus this expansionrather implies a generally disturbed selection process in CVIDIa patients.
CD21low B Cells Reveal Defects in B Cell Receptor (BCR)-MediatedCalcium Influx and Proliferation but Produce Higher Amounts of IgMAntibody. To test the functional capacity of CD21low B cellsref lected by early and late events after BCR stimulation weanalyzed calcium flux, proliferation and antibody productionin vitro. CD21low B cells from CVID patients exhibited sig-nificantly decreased calcium inf lux after BCR stimulationcompared to naı̈ve B cells from CVID patients or HD (Fig. 3A and B). The reduced calcium response after BCR stimulationin CD21low B cells was associated with a severely reducedBCR-mediated proliferative response, which could not be
Fig. 1. Phenotype of CD21low B cells. PBMCs of healthy donors and CVID Ia patients were analyzed by flow cytometry. (A) The expression of the indicated cellsurface markers was analyzed on CD21� and CD21low B cell subpopulations. CD21low B cells are indicated by rectangles. Representative profiles are shown. (B)Representative FACS plots and histograms demonstrate increased cell size according to forward scatter (FSC) as well as (C) elevated expression of CD86 of CD21low
B cells. In the diagrams individual MFI values (dots), mean values (columns), and corresponding p-values (t test) of FSC and CD86 expression of HD naı̈ve, CVIDnaı̈ve and CD21low B cell subpopulations are given.
13452 � www.pnas.org�cgi�doi�10.1073�pnas.0901984106 Rakhmanov et al.
enhanced by anti-CD40 stimulation (Fig. 3C). In addition,CD21low B cells more frequently underwent apoptosis thannaı̈ve cells (Fig. S1). TLR9 stimulation also induced subnormalbut detectable proliferation of CD21low B cells (Fig. 3C). Incontrast, CD21low B cells produced significantly more IgM
than naı̈ve B cells of HD after stimulation with CD40L, IL2,and IL10 (Fig. 3D).
Gene Expression Profiles of CD21low B Cells in CVID Patients.Comparison of gene expression profiles of sortedCD19�CD27�CD38�/lowCD21low B cells of 4 CVID patients,CD19�CD27�CD38�CD21� naı̈ve B cells of the same patientsand of 4 HD identified 321 probe sets for known functionallyannotated genes, unknown expressed sequence tags (ESTs), orgene sequences for hypothetical proteins, which are at least3-fold up- or down-regulated when comparing CD21low B cellsfrom CVID patients with naı̈ve B cells from HD (316 genes)or CVID patients (21 genes) (P value of P � 0.01 and falsediscovery rate (FDR) of 2.2%). The previously identifiedderegulation of CD19, CD21, CD23, CD38, CD86, and CD95was reproduced at the transcriptional level (Fig. 1 and Fig. S2).
The transcription factor sex determining region Y (SRY)-box5 (SOX5) stood out as one of the highest up-regulated genes inCD21low B cells. qRT-PCR confirmed a 10-fold up-regulationcompared to naı̈ve B cells of HD and over 2-fold up-regulationcompared to naive B cells of CVID patients (Fig. S3A). Note-worthy, SOX5 had also been identified as one of the differen-tially regulated genes in FCRL4� B cells (12). We thereforecompared the expression of other markers characterizingFCRL4� B cells. CVID derived CD21low B cells express in-creased levels of FCRL4 transcript (Fig. S3A) and protein (Fig.S3B) and share the reported phenotype with regard to CD20,CD62L, and CD11c expression (Fig. S3B) (12). Also, severaltranscripts of other FCRL family members (15), like FCRL2,FCRL3, FCRL5, FCRLM1, and FCRLM2 were up-regulated(Fig. S2).
CD21low B Cells Express Inflammatory Chemokine Receptors andConstitute the Main B-Cell Population in Peripheral Tissue Like theBronchoalveolar Space. Usually, the homeostatic chemokinereceptors CXCR5 and CCR7 are highly expressed on allcirculating B cell populations and allow homing to B cell and
Fig. 2. CD21low B cells of CVID are polyclonal, unmutated B cells with an increased replication history and autoreactive specificity. (A) Sorted naı̈ve B cells of4 HD and 8 CVID patients as well as CD21low B cells of 8 CVID patients were spectratyped for the expression of Vh1 through Vh6 regions of IgM. Representativeplots for each Vh gene family show the typical Gaussian distribution of polyclonal cells. (B) SHM rates in Vk A27 transcript were determined by Ig�-REHMA assayin sorted HD naive and memory as well as CVID naive and CD21low B cells (n � 5 CVID Ia patients, n � 5 HD). Individual Ig� SHM indices were calculated as theratio of the SHM rate in the sample against the mean baseline rate of SHM in HD naive B cells. The plot indicates individual values (dots) and mean values (columns)of Ig� SHM index. (C) Replication history of CD21low B cells was assessed by KREC assay. The plot indicates individual values (dots) and mean values (columns) ofnumbers of cell divisions of sorted B cell subpopulations (4 HD and 4 CVID samples). (D) B cells of 6 HD and 5 CVID Ia patients were stained with the anti-idiotypicantibody 9G4. The plot indicates individual values (dots) and mean values (columns) of the percentage of 9G4 positive B cells. Kruskal-Wallis (pKW), Mann-Whitney(pMW), and t test p-values are indicated.
Fig. 3. Altered response of CD21low B cells to B cell receptor stimulation. (A)The increase in intracellular calcium concentration in B lymphocytes upon BCRstimulation was measured. An overlay of representative plots for a CVID Iapatient and a HD control is shown. Time points of adding the respectivestimulus are indicated. (B) The plot demonstrates individual values (dots) andmean values (columns) of maximum fluorescence ratio after IgM stimulationof B cell subpopulations of 5 HD and 5 CVID samples. (C) Proliferative responsesof sorted B cells were evaluated by 3H Thymidin incorporation on day 3 and(D) IgM production in supernatants after 7 days of stimulation as indicated.Plots depict individual values (dots) and mean values (columns). P-valuesaccording to Kruskal-Wallis (pKW), Mann-Whitney (pMW), Wilcoxon (pW), andt tests (pt) are indicated.
Rakhmanov et al. PNAS � August 11, 2009 � vol. 106 � no. 32 � 13453
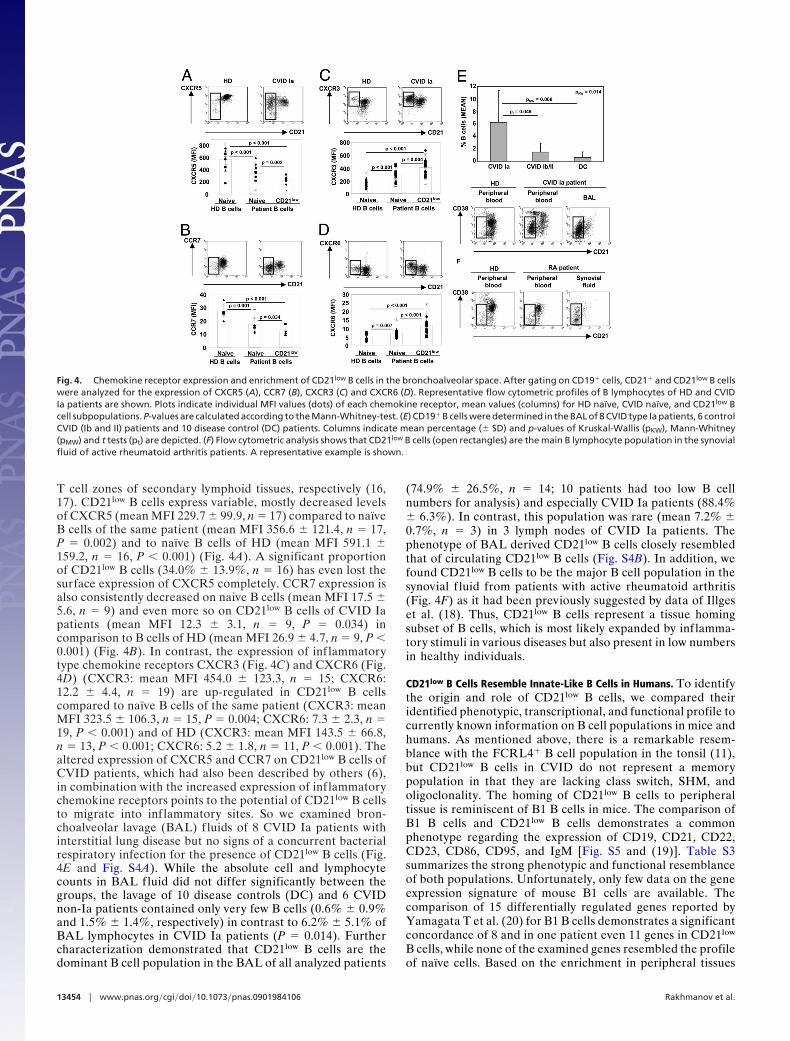
T cell zones of secondary lymphoid tissues, respectively (16,17). CD21low B cells express variable, mostly decreased levelsof CXCR5 (mean MFI 229.7 � 99.9, n � 17) compared to naı̈veB cells of the same patient (mean MFI 356.6 � 121.4, n � 17,P � 0.002) and to naı̈ve B cells of HD (mean MFI 591.1 �159.2, n � 16, P � 0.001) (Fig. 4A). A significant proportionof CD21low B cells (34.0% � 13.9%, n � 16) has even lost thesurface expression of CXCR5 completely. CCR7 expression isalso consistently decreased on naive B cells (mean MFI 17.5 �5.6, n � 9) and even more so on CD21low B cells of CVID Iapatients (mean MFI 12.3 � 3.1, n � 9, P � 0.034) incomparison to B cells of HD (mean MFI 26.9 � 4.7, n � 9, P �0.001) (Fig. 4B). In contrast, the expression of inf lammatorytype chemokine receptors CXCR3 (Fig. 4C) and CXCR6 (Fig.4D) (CXCR3: mean MFI 454.0 � 123.3, n � 15; CXCR6:12.2 � 4.4, n � 19) are up-regulated in CD21low B cellscompared to naı̈ve B cells of the same patient (CXCR3: meanMFI 323.5 � 106.3, n � 15, P � 0.004; CXCR6: 7.3 � 2.3, n �19, P � 0.001) and of HD (CXCR3: mean MFI 143.5 � 66.8,n � 13, P � 0.001; CXCR6: 5.2 � 1.8, n � 11, P � 0.001). Thealtered expression of CXCR5 and CCR7 on CD21low B cells ofCVID patients, which had also been described by others (6),in combination with the increased expression of inf lammatorychemokine receptors points to the potential of CD21low B cellsto migrate into inf lammatory sites. So we examined bron-choalveolar lavage (BAL) f luids of 8 CVID Ia patients withinterstitial lung disease but no signs of a concurrent bacterialrespiratory infection for the presence of CD21low B cells (Fig.4E and Fig. S4A). While the absolute cell and lymphocytecounts in BAL fluid did not differ significantly between thegroups, the lavage of 10 disease controls (DC) and 6 CVIDnon-Ia patients contained only very few B cells (0.6% � 0.9%and 1.5% � 1.4%, respectively) in contrast to 6.2% � 5.1% ofBAL lymphocytes in CVID Ia patients (P � 0.014). Furthercharacterization demonstrated that CD21low B cells are thedominant B cell population in the BAL of all analyzed patients
(74.9% � 26.5%, n � 14; 10 patients had too low B cellnumbers for analysis) and especially CVID Ia patients (88.4%� 6.3%). In contrast, this population was rare (mean 7.2% �0.7%, n � 3) in 3 lymph nodes of CVID Ia patients. Thephenotype of BAL derived CD21low B cells closely resembledthat of circulating CD21low B cells (Fig. S4B). In addition, wefound CD21low B cells to be the major B cell population in thesynovial f luid from patients with active rheumatoid arthritis(Fig. 4F) as it had been previously suggested by data of Illgeset al. (18). Thus, CD21low B cells represent a tissue homingsubset of B cells, which is most likely expanded by inf lamma-tory stimuli in various diseases but also present in low numbersin healthy individuals.
CD21low B Cells Resemble Innate-Like B Cells in Humans. To identifythe origin and role of CD21low B cells, we compared theiridentified phenotypic, transcriptional, and functional profile tocurrently known information on B cell populations in mice andhumans. As mentioned above, there is a remarkable resem-blance with the FCRL4� B cell population in the tonsil (11),but CD21low B cells in CVID do not represent a memorypopulation in that they are lacking class switch, SHM, andoligoclonality. The homing of CD21low B cells to peripheraltissue is reminiscent of B1 B cells in mice. The comparison ofB1 B cells and CD21low B cells demonstrates a commonphenotype regarding the expression of CD19, CD21, CD22,CD23, CD86, CD95, and IgM [Fig. S5 and (19)]. Table S3summarizes the strong phenotypic and functional resemblanceof both populations. Unfortunately, only few data on the geneexpression signature of mouse B1 cells are available. Thecomparison of 15 differentially regulated genes reported byYamagata T et al. (20) for B1 B cells demonstrates a significantconcordance of 8 and in one patient even 11 genes in CD21low
B cells, while none of the examined genes resembled the profileof naı̈ve cells. Based on the enrichment in peripheral tissues
Fig. 4. Chemokine receptor expression and enrichment of CD21low B cells in the bronchoalveolar space. After gating on CD19� cells, CD21� and CD21low B cellswere analyzed for the expression of CXCR5 (A), CCR7 (B), CXCR3 (C) and CXCR6 (D). Representative flow cytometric profiles of B lymphocytes of HD and CVIDIa patients are shown. Plots indicate individual MFI values (dots) of each chemokine receptor, mean values (columns) for HD naı̈ve, CVID naı̈ve, and CD21low Bcell subpopulations. P-values are calculated according to the Mann-Whitney-test. (E) CD19� B cells were determined in the BAL of 8 CVID type Ia patients, 6 controlCVID (Ib and II) patients and 10 disease control (DC) patients. Columns indicate mean percentage (� SD) and p-values of Kruskal-Wallis (pKW), Mann-Whitney(pMW) and t tests (pt) are depicted. (F) Flow cytometric analysis shows that CD21low B cells (open rectangles) are the main B lymphocyte population in the synovialfluid of active rheumatoid arthritis patients. A representative example is shown.
13454 � www.pnas.org�cgi�doi�10.1073�pnas.0901984106 Rakhmanov et al.
and the great similarity to B1 B cells we suggest an innate-likeorigin of CD21low B cells.
DiscussionWe and others have described the unusual expansion ofCD21low B cells in the peripheral blood of patients with CVID(2), viremic HIV infection (8) and systemic lupus erythema-tosus (7). This population is clearly distinct from all othercirculating B cell populations. The low expression of CD38distinguishes these cells from both other CD21 low-expressingB cell populations and transitional B cells, as well as plasma-blasts (3). While also being different from conventional naı̈veB cells by phenotype and gene expression profile, the surfaceexpression of IgM and IgD, lack of class switched isotypes, andthe low CD27 expression are compatible with a naı̈ve-likestatus of most CD21low B cells in CVID. This is corroboratedby the polyclonality and the lack of somatic hypermutation ofthis population excluding an antigen driven origin, especiallya germinal center derived memory stage. The up-regulation ofCD86 and the increased cell size indicate recent activation,while the high surface expression of IgM and IgD argue againstan activation involving the B cell receptor. In several CVIDpatients with expanded circulating CD21low B cells, we had thechance to analyze B cells in lymph node, spleen, and bron-choalveolar lavage. While lymph nodes and spleens containedless CD21low B cells than the peripheral blood, we foundCD21low B cells to present the predominant B cell populationin the bronchoalveolar space. These cells resemble closely theircirculating counterparts. Interestingly, this local dominance ofCD21low B cells was independent of the underlying disease.Also in synovial f luid of patients with rheumatoid arthritis, aperipheral inf lammatory tissue with known B cell infiltration(21), most B cells were CD21low B cells closely resemblingCD21low B cells in BAL and peripheral blood of CVID patientssupporting the notion that CD21low B cells are enriched inperipheral tissues.
Their homing to peripheral tissue is highly reminiscent ofthe nature of innate B cells in mice (22). B1 B cells designatea specialized innate B cell population distinct from conven-tional B2 cells, including follicular (FO) B cells as well asMZ-B cells, by their origin, unique tissue distribution, poly-reactive antigen specificity, and capacity of self renewal (19).Comparison of CD21low B cells of CVID patients with con-ventional B2 and B1 B cells demonstrated a similar, partiallyactivated phenotype, with the exception of the expression ofCD5, CD38, and CD24, which seem to be differentiallyregulated in humans and mice (22–25). In human peripheralblood, CD5 is expressed on the majority of transitional B cellsand some CD21low and naı̈ve B cells, thus rendering CD5 nota marker for a specific human B cell subset. CD21low B cellsand B1 B cells have a history of higher in vivo turnover thanconventional naı̈ve B2 B cells (19). Unlike B1a B cells, CD21low
B cells show signs of previous TdT activity and thus don’t seemto derive from a fetal liver precursor population. CD21low Bcells from CVID patients are polyclonal B cells with increasedpoly- and even autoreactive specificities (E. Meffre, personalcommunication) in assays using single cell RT-PCR andexpression vector cloning of the BCR (26). In fact, thefrequency of autoreactive clones was compatible to earlyimmature B cells (27). Polyreactivity and an increased auto-reactivity is a significant trait in innate-like B cells affecting theselection into this pool (22). Finally, similar to B1 B cells andprobably associated with the partially activated, polyreactivestatus, in vitro stimulation of the BCR causes only poorcalcium inf lux and proliferative response in CD21low B cellsand increased apoptosis, even after costimulation with CD40(28, 29). This attenuated response might be the result ofincreased levels of several inhibitory receptors like CD22 (30),
Siglecs (28) and FCRLs (only human) in CD21low B cells aswell as B1 B cells. Also the response to CpG stimulation isreduced in CD21low B cells and murine B1 B cells comparedto their respective naı̈ve counterparts (31). On the contrary, Igsynthesis is even enhanced in CD21low B cells, suggesting apreferential differentiation into antibody secreting cells.
Partial anergy referring to a functional nonresponsiveness ofmature lymphocytes seems to be a common tolerogenic traitamong innate-like B cells (32). Thus, signaling in innate-like Bcells resembles the signaling in classical anergy (33) as de-scribed in the soluble HEL model (34). Innate-like B cellsincluding CD21low B cells, however, differ from the classicalform of anergy in several important aspects. Anergic anti-HELB cells require constant BCR occupancy (35) and thereforeexpress low IgM receptors. They fail to up-regulate CD86 (36)and do not produce antibody on stimulation in vitro. Bothfunctions are preserved in CD21low B cells and in murineinnate-like B cells, rendering these cells a potential threat ofautoimmunity, which in fact is increased in CVID Ia patients.
The additional resemblance of CD21low B cells withFCRL4� B cells in human tonsils (11) is remarkable, especiallyin view of the presence of FCRL4�CD21low B cells in the bloodof HIV (8) and SLE patients (7). The major differencebetween these populations is the lack of class switch, SHM andoligoclonality in CVID derived CD21low B cells, assigning theminto the nonmemory pool. This difference might be due to theunderlying defect in memory formation in CVID (2). Thusnonswitched and switched CD21low B cells might representdifferent stages of a developmental continuum. This hypoth-esis is supported by the fact that in the blood of HD, SLEpatients (7), as well as in human tonsils (10) IgM�, unmutated,naı̈ve-like FCRL4�CD21low B cells have been described along-side with the mutated memory-like FCRL4�CD21low B cells.
In conclusion, this study reveals that in CVID, CD21low Bcells are a distinct, polyclonal, preactivated, partially autore-active, functionally attenuated B cell population with prefer-ential enrichment in peripheral tissues. Thus, strongly resem-bling murine innate-like B cells, we suggest that humanCD21low B cells represent an innate-like B cell population,abnormally expanded in the peripheral blood of a subgroup ofCVID patients. Further studies will be important to shed morelight on the relation between nonswitched and switchedFCRL4�CD21low B cells in the various disease entities andtheir origin and role in the human immune system. In CVID,future work needs to address the origin and effect of thedramatic expansion of circulating innate-like B cells in thecontext of altered B cell function and selection.
Materials and MethodsDescription of Patient and Healthy Donor Cohorts. 81 CVID patients including29 Freiburg type Ia patients (Table S1) diagnosed in line with the EuropeanSociety for Immunodeficiencies criteria were classified according to theFreiburg (2) and EUROclass (3) classification. CVID patients and controls (10DC patients and 31 HD) were between 17 and 75 years of age. BAL wasperformed in 8 CVID Ia and 6 CVID Ib/II, as well as 10 DC patients for medicalindication. Informed written consent to the internal ethics review board-approved clinical study protocol (University Hospital Freiburg 239/99) wasobtained from each individual before participation in the study, in accor-dance with the Declaration of Helsinki.
Flow Cytometric Analysis and Cell Sorting. Antibodies used in flow cytometryand calcium flux assay are described in SI Material and Methods. Anti-FCRL4antibodies were a generous gift of Dr. Max Cooper (Emory UniversitySchool of Medicine, Atlanta, GA). VH4 –34 specific 9G4 antibodies werekindly provided by Dr. Freda Stevenson (University of Southampton,Southampton, United Kingdom).
Flow cytometric analysis was performed on a FACSCaliburTM or LSR II (BDBiosciences). Data were analyzed using FlowJo (Tree Star Inc.) software. For cellsorting naı̈ve and CD21low B cells of patients and HD, the cells were separated into
Rakhmanov et al. PNAS � August 11, 2009 � vol. 106 � no. 32 � 13455
CD19�CD27�CD21�CD38� cells and CD19�CD27�CD21�CD38� cells respectivelyto a purity of �95% using a MoFlow cell sorter (DakoCytomation).
Microarray Analysis. Human genome U133 plus 2.0 arrays (Affymetrix U.K.Ltd.) were used. The description of the RNA amplification and hybridizationexperiments is in SI Material and Methods.
Analysis of microarray data were performed using dChip software (37).Microarray data are available in the National Center for Biotechnology Infor-mation Gene Expression Omnibus (http://www.ncbi.nih.gov/geo/) under ac-cession no. GSE17269.
Quantitative RT-PCR. qRT-PCR for SOX5, FCRL4, hypoxanthine phosphoribo-syltransferase 1 (HPRT1) and glyceraldehyde-3-phosphate dehydrogenase(GAPDH) genes was performed using a LightCycler 480 Real-Time PCR System(Roche Diagnostics GmbH). Primer sequences and PCR conditions are providedin SI Material and Methods.
IgH CDR3 Spectratyping and Analysis of VH Gene Repertoire. IgH CDR3 spec-tratyping was performed as described by Pannetier et al. (38) for analysis ofthe TCR�-chain. We used primers as established by Kueppers et al. (39). In brief,the CDR3 regions were amplified using 35 cycles of PCR with a forward primerspecific for the V region family and the common reverse primer from theconstant region (39). In a second round, 3 cycles of a primer extension reactionwith a fluorescent (5� FAM-labeled) nested reverse primer specific for theconstant region was performed. The run-off products were then analyzed on
an ABI 3100 capillary sequencer (Applied Biosystems) to determine the lengthdistribution of the fluorescent fragments.
Multiplex PCR for VH-JH rearrangements was performed according to (40).Description of analysis of VH gene repertoire, B cell proliferation and Igsecretion assays are in SI Material and Methods.
SHM Analysis and KREC Assay. SHM in the V� A27 transcript was analyzed usingIg�-restriction enzyme-based hot-spot mutation assay (Ig�-REHMA assay) asdescribed by Andersen et al. (13). Ig�-REHMA assay for V�3–20 gene as well asKREC assay was performed as described previously (14).
Statistical Analysis. All data are expressed as mean � SD unless indicatedotherwise. Statistical comparison between groups was carried out using pairedand unpaired t tests, the Kruskal-Wallis (KW) ANOVA by ranks and in cases ofsignificant differences, the Mann-Whitney (MW) test between groups wereapplied as indicated using SigmaStat 3.1 software (Systat Software GmbH).
ACKNOWLEDGMENTS. The authors thank Dr. Jens Thiel and Dr. ManuellaGomes for patient care, Ruth Draeger, Stefanie Hahn, Sylvia Kock, Dr. MarieFollo, Klaus Geiger, Dr. Andrea Heinzmann, and Jessica Heinze for theirtechnical support and Cornelius Struck, Dr. Michael Schlesier and Dr.Anne-Marie Eades-Perner for help in preparing the manuscript. This re-search was funded by the German Research Foundation grant SFB620,projects C1 (to K.W., H.H.P.), C2 (to U.S.), and Z2 (to P.F.), 7th frameworkprograms of the European Union Grant Nr. HEALTH-F2–2008-201549 (toK.W., H.E., U.S., I.Q.) and BMBF grant CCI-01E O0803 (to K.W., H.E., U.S.).
1. Warnatz K, Schlesier M (2008) Flowcytometric phenotyping of common variableimmunodeficiency. Cytometry B Clin Cytom 74:261–271.
2. Warnatz K, et al. (2002) Severe deficiency of switched memory B cells (CD27(�)-IgM(�)IgD(�)) in subgroups of patients with common variable immunodeficiency: A newapproach to classify a heterogeneous disease. Blood 99:1544–1551.
3. Wehr C, et al. (2008) The EUROclass trial: Defining subgroups in common variableimmunodeficiency. Blood 111:77–85.
4. Piqueras B, et al. (2003) Common variable immunodeficiency patient classificationbased on impaired B cell memory differentiation correlates with clinical aspects. J ClinImmunol 23:385–400.
5. Warnatz K, et al. (2002) Expansion of CD19(hi)CD21(lo/neg) B cells in common variableimmunodeficiency (CVID) patients with autoimmune cytopenia. Immunobiology206:502–513.
6. Moratto D, et al. (2006) Combined decrease of defined B and T cell subsets in a groupof common variable immunodeficiency patients. Clin Immunol 121:203–214.
7. Wehr C, et al. (2004) A new CD21low B cell population in the peripheral blood ofpatients with SLE. Clin Immunol 113:161–171.
8. Moir S, et al. (2001) HIV-1 induces phenotypic and functional perturbations of B cellsin chronically infected individuals. Proc Natl Acad Sci USA 98:10362–10367.
9. Moir S, et al. (2008) Evidence for HIV-associated B cell exhaustion in a dysfunctionalmemoryBcell compartment inHIV-infectedviremic individuals. JExpMed205:1797–1805.
10. Falini B, et al. (2003) Expression of the IRTA1 receptor identifies intraepithelial andsubepithelial marginal zone B cells of the mucosa-associated lymphoid tissue (MALT)Blood 102:3684–3692.
11. Ehrhardt GR, et al. (2005) Expression of the immunoregulatory molecule FcRH4 definesa distinctive tissue-based population of memory B cells. J Exp Med 202:783–791.
12. Ehrhardt GR, et al. (2008) Discriminating gene expression profiles of memory B cellsubpopulations. J Exp Med 205:1807–1817.
13. Andersen P, et al. (2005) Deficiency of somatic hypermutation of the antibody lightchain is associated with increased frequency of severe respiratory tract infection incommon variable immunodeficiency. Blood 105:511–517.
14. van Zelm MC, Szczepanski T, van der BM, van Dongen JJ (2007) Replication history ofB lymphocytes reveals homeostatic proliferation and extensive antigen-induced B cellexpansion. J Exp Med 204:645–655.
15. Ehrhardt GR, et al. (2007) Fc receptor-like proteins (FCRL): Immunomodulators of B cellfunction. Adv Exp Med Biol 596:155–162.
16. Forster R, et al. (1996) A putative chemokine receptor, BLR1, directs B cell migration todefined lymphoid organs and specific anatomic compartments of the spleen. Cell87:1037–1047.
17. Forster R, et al. (1999) CCR7 coordinates the primary immune response by establishingfunctional microenvironments in secondary lymphoid organs. Cell 99:23–33.
18. Illges H, Braun M, Peter HH, Melchers I (2000) Reduced expression of the complementreceptor type 2 (CR2, CD21) by synovial fluid B and T lymphocytes Clin Exp Immunol122:270–276.
19. Fagarasan S, Watanabe N, Honjo T (2000) Generation, expansion, migration andactivation of mouse B1 cells. Immunol Rev 176:205–215.
20. Yamagata T, Benoist C, Mathis D (2006) A shared gene-expression signature in innate-like lymphocytes. Immunol Rev 210:52–66.
21. Kim HJ, Berek C (2000) B cells in rheumatoid arthritis Arthritis Res 2:126–131.22. Hardy RR B-1 B cell development (2006) J Immunol 177(5):2749–2754.23. Carsetti R, Rosado MM, Wardmann H (2004) Peripheral development of B cells in mouse
and man. Immunol Rev 197:179–191.24. Ridderstad A, Tarlinton DM (1998) Kinetics of establishing the memory B cell popula-
tion as revealed by CD38 expression. J Immunol 160:4688–4695.25. Liu YJ, Arpin C (1997) Germinal center development. Immunol Rev 156:111–126.26. Tiller T, et al. (2008) Efficient generation of monoclonal antibodies from single human
B cells by single cell RT-PCR and expression vector cloning. J Immunol Methods329:112–124.
27. Wardemann H, et al. (2003) Predominant autoantibody production by early human Bcell precursors Science 301:1374–1377.
28. Hoffmann A, et al. (2007) Siglec-G is a B1 cell-inhibitory receptor that controls expan-sion and calcium signaling of the B1 cell population. Nat Immunol 8:695–704.
30. Danzer CP, Collins BE, Blixt O, Paulson JC, Nitschke L (2003) Transitional and marginalzone B cells have a high proportion of unmasked CD22: Implications for BCR signaling.Int Immunol 15:1137–1147.
31. Genestier L, et al. (2007) TLR agonists selectively promote terminal plasma cell differ-entiation of B cell subsets specialized in thymus-independent responses. J Immunol178:7779–7786.
33. Goodnow CC, Brink R, Adams E (1991) Breakdown of self-tolerance in anergic Blymphocytes. Nature 352:532–536.
34. Wong SC, et al. (2002) Peritoneal CD5� B-1 cells have signaling properties similar totolerant B cells. J Biol Chem 277:30707–30715.
35. Gauld SB, Benschop RJ, Merrell KT, Cambier JC (2005) Maintenance of B cell anergyrequires constant antigen receptor occupancy and signaling. Nat Immunol 6:1160–1167.
36. Rathmell JC, Fournier S, Weintraub BC, Allison JP, Goodnow CC (1998) Repression ofB7.2 on self-reactive B cells is essential to prevent proliferation and allow Fas-mediateddeletion by CD4(�) T cells. J Exp Med 188:651–659.
37. Li C, Wong WH (2001) Model-based analysis of oligonucleotide arrays: Expression indexcomputation and outlier detection. Proc Natl Acad Sci USA 98:31–36.
38. Pannetier C, Levraud P, Lim A, Even J, Kourilsky P (1998) in The Antigen T Cell Receptor:Selected Protocols and Applications, ed Oksenberg JR (Chapman & Hall, London), pp287–325.
39. Kuppers R, Zhao M, Rajewsky K, Hansmann ML (1993) Detection of clonal B cellpopulations in paraffin-embedded tissues by polymerase chain reaction. Am J Pathol143:230–239.
40. van Dongen JJ, et al. (2003) Design and standardization of PCR primers and protocolsfor detection of clonal immunoglobulin and T-cell receptor gene recombinations insuspect lymphoproliferations: report of the BIOMED-2 Concerted Action BMH4-CT98–3936 Leukemia 17:2257–2317.
13456 � www.pnas.org�cgi�doi�10.1073�pnas.0901984106 Rakhmanov et al.