10/11/16 1 Post-Stroke Acupuncture: a manual for diagnosis and treatment at acute, subacute and chronic stages Claudia Citkovitz PhD, LAc Director of Acupuncture Services NYU Lutheran Medical Center, Brooklyn NY Purpose of this Talk • PM - To provide a straightforward reference manual for how to help a patient, friend or loved one who suffers a stroke or intracranial hemorrhage
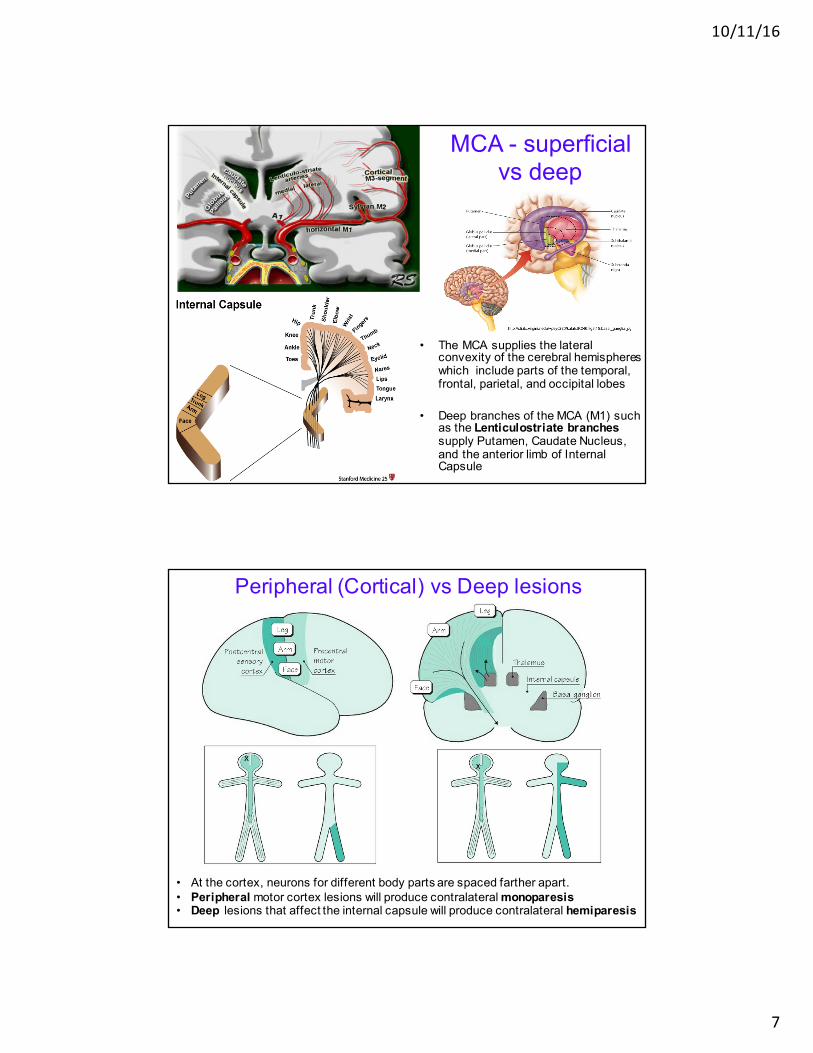
• The MCA supplies the lateral convexity of the cerebral hemispheres which include parts of the temporal, frontal, parietal, and occipital lobes
• Deep branches of the MCA (M1) such as the Lenticulostriate branches supply Putamen, Caudate Nucleus, and the anterior limb of Internal Capsule
Peripheral (Cortical) vs Deep lesions
• At the cortex, neurons for different body parts are spaced farther apart.• Peripheral motor cortex lesions will produce contralateral monoparesis• Deep lesions that affect the internal capsule will produce contralateral hemiparesis
10/11/16
8
Posterior Cerebral Artery
Branches of the PCA supply :• most of (1) midbrain (2) thalamus, and (3) subthalamic nucleus.• Anterior, posterior temporal, and parietooccipital branches, supply:
temporal lobes, medial and inferior occipital lobes of the cerebral cortex. • Calcarine artery supplies the primary visual cortex
Posterior Vessel Stroke Symptoms • Visual symptoms are a prominent feature:
– Sudden onset of bilateral signs, including ptosis, pupillary asymmetry or lack of reaction to light, and somnolence.
– Visual field loss, visual agnosia, disorders of color vision
• Memory impairment• Motor dysfunction
– Hemiballisumus is unique to PCA stroke• Central post-stroke pain syndrome
– Thalamus generates pain signal over entire affected side – excruciating
More Detail• Posterior Inferior Cerebellar Artery (PICA - blue)• Superior Cerebellar Artery (SCA - grey)
– superior and tentorial surface of the cerebellum.• Branches from vertebral and basilar artery supply
– medulla oblongata (light blue) – pons (green).
• Anterior Choroideal artery (AchA - aqua)– part of the hippocampus, – posterior limb of the internal capsule – extends upwards to an area lateral to the posterior part of the cella
media. • Lenticulo-striate arteries (LSA’s):
– lateral LSA’s (orange) = deep penetrating arteries of the middle cerebral artery (MCA): basal ganglia
– medial LSA' s (dark red) arise from anterior cerebral artery (usually the A1-segment).
• Anterior cerebral artery (ACA - red)– medial part of frontal and parietal lobe– anterior portion of corpus callosum, basal ganglia and internal
capsule.• Middle cerebral artery (MCA - yellow)
– cortical branches of MCA supply the lateral surface of the hemisphere, except for inferior part of the temporal lobe (pca).
• Posterior cerebral artery (PCA - light green)– Posterior thalamoperforating arteries branch off P1 segment and
supply blood to midbrain and thalamus.– Cortical branches of the PCA supply the inferomedial part of the
temporal lobe, occipital pole, visual cortex, and splenium of the corpus callosum.
10/11/16
10
Visual Fields
• An injury on one side of the brain will cause deficits in both eyes.– Eg MCA -> contralateral homonymous hemianopia
• Monocular visual loss suggests an injury anterior to the optic chiasm.
Thalamus• “The major way station
of incoming sensation.” (Melvin Konner)
• Sensory information such as: visual input, touch, pressure, heat, cold, and pain all enter the thalamus, then is directed to its appropriate area in the cortex.
The cerebellum controls many of our reflexes and much of our balance and coordination. A stroke that takes place in the cerebellum can cause:
•Coordination and balance problems, thus Dizziness, nausea and vomiting.•Alcohol affects cerebellar function. Cerebellar problems mimic movement of a drunk person•Nystagmus•Dysarthria: muscles of voice production and speech lack coordination so sudden irregular changes in volume and timing occur, i.e. scanning or staccato speech (words are broken into syllables).•Upper limbs: ataxia and intention tremor - best seen in movement directed towards a restricted target e.g. the finger–nose test•Dysdiadochokinesia i.e. slow, inaccurate, rapid alternating movements•Lower limbs: ataxia -best seen in the heel–knee–shin test.•Gait and stance ataxia- especially if the patient is asked to walk heel to toe, or to stand still on one leg.
Brain Stem or Vertebrobasilar Artery Stroke
• Strokes here are especially devastating. Controls all our involuntary, "life-support" functions, eg breathing rate, blood pressure, heartbeat. also controls eye movements, hearing, speech and swallowing.
• Since impulses generated in the brain's hemispheres must travel through the brain stem on their way to arms and legs, patients with a brain stem stroke may also develop paralysis in one or both sides of the body.