Classification and Endovascular Management of Pediatric Cerebral Vascular Malformations Timo Krings, MD, PhD, FRCP(C) a,b,c, *, Sasikhan Geibprasert, MD d,e , Karel terBrugge, MD, FRCP(C) a Before treating pediatric vascular malformation, 2 basic principles have to be taken into account that may seem trivial but still have an effect on management strategies. The first principle is that the understanding of a disease should precede its treatment. In vascular malformations, little is known about their cause, pathophysiology, or natural history, and the numerous different classi- fication schemes that should aid in the under- standing of arteriovenous (AV) shunts testify to this lack of knowledge. In addition, advances in diagnostic tools for pretreatment risk assessment as well as continuously improved treatment modalities are likely to further change the way these vascular malformations are managed. The second basic principle is that children are not small adults; vascular malformations in the pedi- atric population differ significantly from the adult population. Therefore, classification schemes used for and derived from the experience in treat- ing adults are not likely to be compatible with the treatment protocols in children. As a particular example, the adult-based classification of AV shunting lesions that is related to the expected surgical outcome of AV malformations is particu- larly inappropriate in children, in whom (1) cere- bral eloquence is difficult to assess because of the remodeling potential, particularly in the first few years of life, (2) most lesions are fistulas or multifocal, (3) the drainage usually affects the entire venous system, and (4) the potential for recovery is different. In addition, the anatomic and physiologic characteristics of the neonatal and infant brain (including hydrovenous peculiari- ties and immaturity of myelination) create a specific group of nonhemorrhagic symptoms and therapeutic challenges that are not encoun- tered in adults. a Division of Neuroradiology, Department of Medical Imaging, Toronto Western Hospital, University of Toronto, 399 Bathurst Street, 3MCL – 429, Toronto, ON M5T 2S8, Canada b Department of Neuroradiology, University Hospital Aachen, Pauwelsstraße 30, Aachen 52074, Germany c Service de Neuroradiologie Diagnostique et Therapeutique, CHU Le-Kremlin-Bicetre, 78, rue du Ge ´ ne ´ ral Leclerc, Cedex, Paris 94275, France d Department of Diagnostic Imaging, The Hospital for Sick Children, University of Toronto, 555 University Avenue, Toronto, ON M5G 1X8, Canada e Department of Radiology, Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Ratchatewi, Bangkok 10400, Thailand * Corresponding author. Division of Neuroradiology, Department of Medical Imaging, Toronto Western Hospital, University of Toronto, 399 Bathurst Street, 3MCL – 429, Toronto, ON M5T 2S8, Canada. E-mail address: [email protected]KEYWORDS Endovascular management Pediatric cerebral vascular malformations Classification Neurosurg Clin N Am 21 (2010) 463–482 doi:10.1016/j.nec.2010.03.010 1042-3680/10/$ – see front matter ª 2010 Elsevier Inc. All rights reserved. neurosurgery.theclinics.com
Before treating pediatric vascular malformation, 2basic principles have to be taken into accountthat may seem trivial but still have an effect onmanagement strategies. The first principle is thatthe understanding of a disease should precedeits treatment. In vascular malformations, little isknown about their cause, pathophysiology, ornatural history, and the numerous different classi-fication schemes that should aid in the under-standing of arteriovenous (AV) shunts testify tothis lack of knowledge. In addition, advances indiagnostic tools for pretreatment risk assessmentas well as continuously improved treatmentmodalities are likely to further change the waythese vascular malformations are managed. Thesecond basic principle is that children are notsmall adults; vascular malformations in the pedi-atric population differ significantly from the adultpopulation. Therefore, classification schemes
a Division of Neuroradiology, Department of MedicalToronto, 399 Bathurst Street, 3MCL – 429, Toronto, ON Mb Department of Neuroradiology, University Hospital Aac Service de Neuroradiologie Diagnostique et TherapeuLeclerc, Cedex, Paris 94275, Franced Department of Diagnostic Imaging, The Hospital forAvenue, Toronto, ON M5G 1X8, Canadae Department of Radiology, Ramathibodi Hospital, MBangkok 10400, Thailand* Corresponding author. Division of Neuroradiology,Hospital, University of Toronto, 399 Bathurst Street, 3MCE-mail address: [email protected]
Neurosurg Clin N Am 21 (2010) 463–482doi:10.1016/j.nec.2010.03.0101042-3680/10/$ – see front matter ª 2010 Elsevier Inc. All
used for and derived from the experience in treat-ing adults are not likely to be compatible with thetreatment protocols in children. As a particularexample, the adult-based classification of AVshunting lesions that is related to the expectedsurgical outcome of AV malformations is particu-larly inappropriate in children, in whom (1) cere-bral eloquence is difficult to assess because ofthe remodeling potential, particularly in the firstfew years of life, (2) most lesions are fistulas ormultifocal, (3) the drainage usually affects theentire venous system, and (4) the potential forrecovery is different. In addition, the anatomicand physiologic characteristics of the neonataland infant brain (including hydrovenous peculiari-ties and immaturity of myelination) createa specific group of nonhemorrhagic symptomsand therapeutic challenges that are not encoun-tered in adults.
Imaging, Toronto Western Hospital, University of5T 2S8, Canada
chen, Pauwelsstraße 30, Aachen 52074, Germanytique, CHU Le-Kremlin-Bicetre, 78, rue du General
Sick Children, University of Toronto, 555 University
ahidol University, 270 Rama VI Road, Ratchatewi,
Department of Medical Imaging, Toronto WesternL – 429, Toronto, ON M5T 2S8, Canada.
This article discusses different approaches toclassifying pediatric vascular malformations anddescribes the endovascular management options.The difficulty in classifying pediatric cerebralvascular malformations is reflected by the largevariety of different approaches that have beenused for these rare diseases. These classificationsmay be based on symptoms, pathomechanisms,patient’s age, or morphologic features. Each ofthese classifications may have specific advan-tages, but the fact that no uniform classificationhas yet been decided on testifies to their specificdrawbacks.
PATHOMECHANICAL CLASSIFICATION
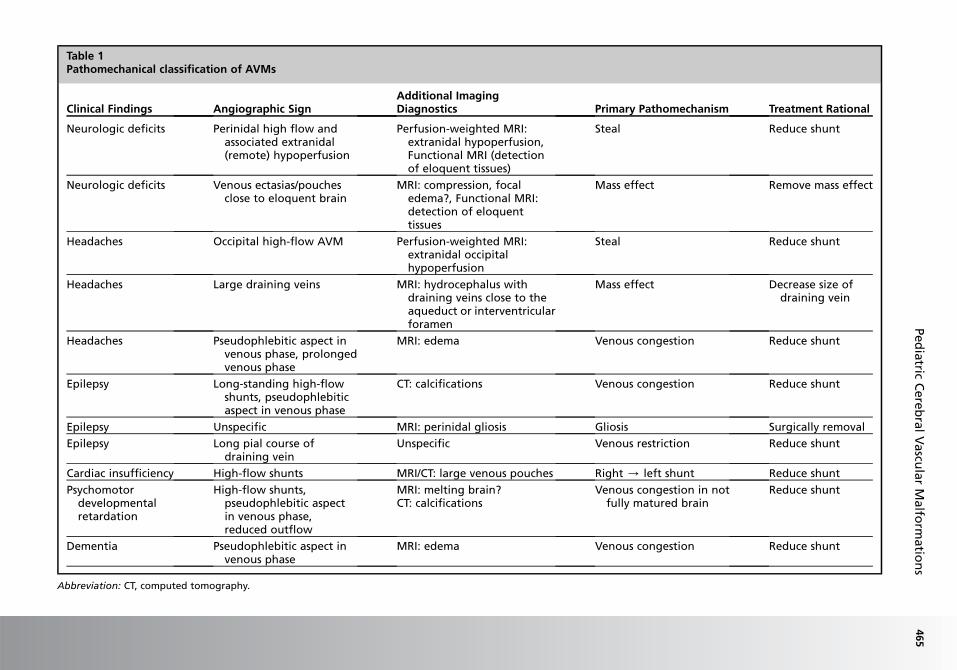
A clinical and pathomechanical classification canlead to the following subcategories: certain high-flow shunts (ie, fistulous pial AV malformations)can lead to macrocrania, hydrocephalus, andpsychomotor developmental retardation asa result of hydrovenous disorders, and cardiacinsufficiency caused by cardiac overload. Venouscongestion that can be caused by a high input(fistulous lesions) or a reduced outflow(secondary stenosis of the outflow pattern) maylead to cognitive decline or epilepsy. Even if signsof venous congestion are not present, a long pialcourse of the draining vein may indicate thatvenous drainage restriction is present in a largearea, increasing the risk of venous congestionand subsequent epilepsy.1 Conversely, a shortvein that drains almost directly into a dural sinusis unlikely to interfere with the normal pialdrainage. If epilepsy was present in a patientwith this kind of angioarchitecture, the magneticresonance imaging (MRI) should be scrutinizedfor signs of perinidal gliosis or hemosiderosis asthe cause of the patient’s symptoms. Mass effectis a rare pathomechanism that may result fromlarge venous ectasias or the nidus proper com-pressing critical structures and may lead toepilepsy, neurologic deficits, and even hydro-cephalus.2 Arterial steal has been associatedwith clinical findings such as migraine and focalneurologic symptoms that most often are transi-tory in nature.3 With the advent of new imagingmodalities such as functional MRI and perfu-sion-weighted MRI it has now become possibleto visualize whether or not the symptoms ofa patient can be attributed to a true steal. Hemor-rhage in AV shunting lesions may be caused byangioarchitectural risk factors such as venousoutlet stenoses or intranidal aneurysms(Table 1).4,5 One advantage of this classificationis that it may be used to guide therapies,because it relates the pathomechanism to the
clinical findings. Therefore, in patients with high-flow shunts and problems that indicate venouscongestion or in patients with arterial steal, treat-ment should be aimed to reduce the AV shuntingvolume, which can be achieved by endovasculartechniques. In patients with epilepsy from perifo-cal gliosis, or in patients presenting with masseffect, endovascular treatment may be less indi-cated. Surgical resection or decompression withpossible preoperative embolization are likely tobe more beneficial in these cases.
AGE-RELATED CLASSIFICATION
A classification of pediatric vascular malforma-tions according to the patient’s age is helpful inpredicting what type of vascular malformationswill be encountered, but does not explain whythe predominance of specific vascular malforma-tions in specific age-groups exists. However, themajor advantage of this classification is the abilityto predict symptoms that are specific for eachpediatric age-group.6
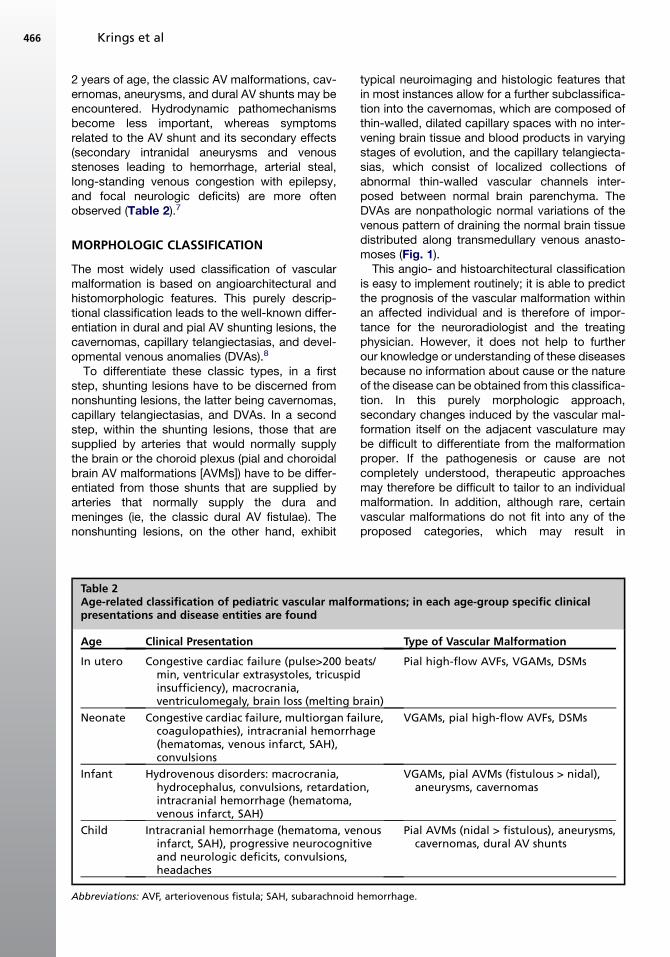
In the fetal age, prenatal MRI or ultrasound maydetect high-flow fistulous lesions, vein of Galen AVmalformations (VGAMs) or dural sinus malforma-tions (DSMs). Systemic manifestations such asmacrocrania with or without encephalomalacia(melting brain syndrome) and cardiac manifesta-tions may be clinically present and point towarda bad prognosis. Similar to the fetal period, in theneonatal period, VGAMs, DSMs, and pial AVshunts are the predominant lesions; however,albeit rarer, cavernomas and arterial aneurysmshave also been observed in this age-group.Systemic pathomechanisms as described earlierand hydrovenous pathomechanisms (hydroceph-alus, maturation delay) are found more often inthis period. Neurologic manifestations (seizures,focal deficits) point toward a hemorrhagic infarctor venous congestion. During infancy, VGAMs,pial AV shunts (more often fistulous than glomer-ular), DSMs, aneurysms, and cavernomas maybe present. In shunting lesions, hydrodynamicdisorders are the predominant pathomechanisms:the cerebrospinal fluid (CSF) reabsorption in thisage-group is solely dependent on the venous(transparenchymal) drainage because the arach-noid granulations are not yet fully functional.Therefore, an increased pressure within thevenous system (caused by an AV shunt) leads toretention of CSF within the ventricles witha concomitant increase in ventricular size andtransependymal pressure gradient until a newequilibrium is found. Macrocrania, cognitive delay,hydrocephalus, and cerebellar tonsillar prolapseare the clinical manifestations at this stage. After
2 years of age, the classic AV malformations, cav-ernomas, aneurysms, and dural AV shunts may beencountered. Hydrodynamic pathomechanismsbecome less important, whereas symptomsrelated to the AV shunt and its secondary effects(secondary intranidal aneurysms and venousstenoses leading to hemorrhage, arterial steal,long-standing venous congestion with epilepsy,and focal neurologic deficits) are more oftenobserved (Table 2).7
MORPHOLOGIC CLASSIFICATION
The most widely used classification of vascularmalformation is based on angioarchitectural andhistomorphologic features. This purely descrip-tional classification leads to the well-known differ-entiation in dural and pial AV shunting lesions, thecavernomas, capillary telangiectasias, and devel-opmental venous anomalies (DVAs).8
To differentiate these classic types, in a firststep, shunting lesions have to be discerned fromnonshunting lesions, the latter being cavernomas,capillary telangiectasias, and DVAs. In a secondstep, within the shunting lesions, those that aresupplied by arteries that would normally supplythe brain or the choroid plexus (pial and choroidalbrain AV malformations [AVMs]) have to be differ-entiated from those shunts that are supplied byarteries that normally supply the dura andmeninges (ie, the classic dural AV fistulae). Thenonshunting lesions, on the other hand, exhibit
Table 2Age-related classification of pediatric vascular malfopresentations and disease entities are found
Age Clinical Presentation
In utero Congestive cardiac failure (pulse>200 bemin, ventricular extrasystoles, tricuspidinsufficiency), macrocrania,ventriculomegaly, brain loss (melting b
typical neuroimaging and histologic features thatin most instances allow for a further subclassifica-tion into the cavernomas, which are composed ofthin-walled, dilated capillary spaces with no inter-vening brain tissue and blood products in varyingstages of evolution, and the capillary telangiecta-sias, which consist of localized collections ofabnormal thin-walled vascular channels inter-posed between normal brain parenchyma. TheDVAs are nonpathologic normal variations of thevenous pattern of draining the normal brain tissuedistributed along transmedullary venous anasto-moses (Fig. 1).
This angio- and histoarchitectural classificationis easy to implement routinely; it is able to predictthe prognosis of the vascular malformation withinan affected individual and is therefore of impor-tance for the neuroradiologist and the treatingphysician. However, it does not help to furtherour knowledge or understanding of these diseasesbecause no information about cause or the natureof the disease can be obtained from this classifica-tion. In this purely morphologic approach,secondary changes induced by the vascular mal-formation itself on the adjacent vasculature maybe difficult to differentiate from the malformationproper. If the pathogenesis or cause are notcompletely understood, therapeutic approachesmay therefore be difficult to tailor to an individualmalformation. In addition, although rare, certainvascular malformations do not fit into any of theproposed categories, which may result in
rmations; in each age-group specific clinical
Type of Vascular Malformation
ats/
rain)
Pial high-flow AVFs, VGAMs, DSMs
ilure,ge
VGAMs, pial high-flow AVFs, DSMs
n,VGAMs, pial AVMs (fistulous > nidal),
aneurysms, cavernomas
ousive
Pial AVMs (nidal > fistulous), aneurysms,cavernomas, dural AV shunts
hemorrhage.
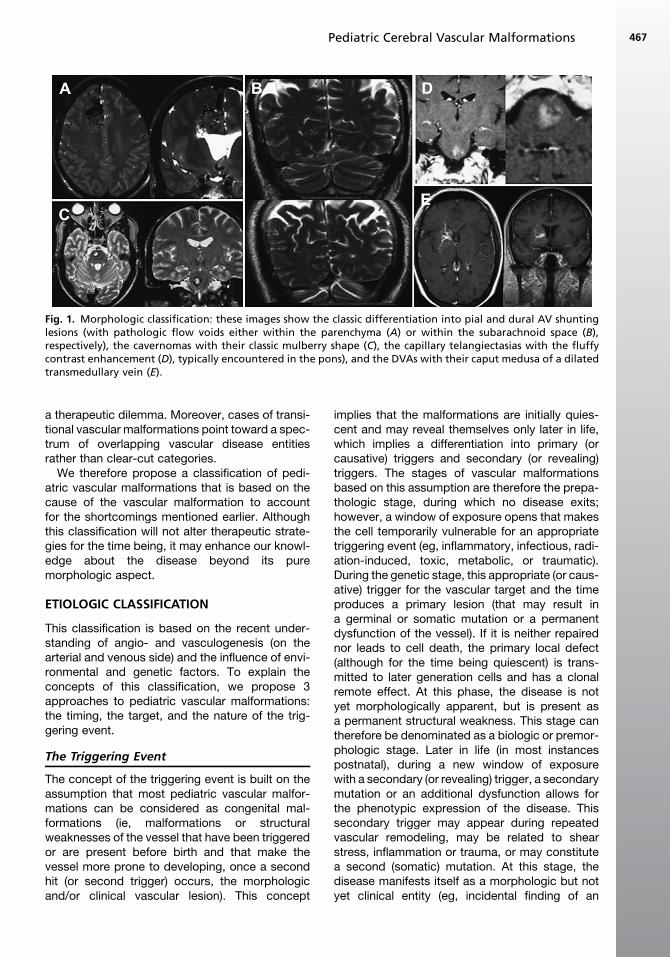
Fig. 1. Morphologic classification: these images show the classic differentiation into pial and dural AV shuntinglesions (with pathologic flow voids either within the parenchyma (A) or within the subarachnoid space (B),respectively), the cavernomas with their classic mulberry shape (C), the capillary telangiectasias with the fluffycontrast enhancement (D), typically encountered in the pons), and the DVAs with their caput medusa of a dilatedtransmedullary vein (E).
Pediatric Cerebral Vascular Malformations 467
a therapeutic dilemma. Moreover, cases of transi-tional vascular malformations point toward a spec-trum of overlapping vascular disease entitiesrather than clear-cut categories.
We therefore propose a classification of pedi-atric vascular malformations that is based on thecause of the vascular malformation to accountfor the shortcomings mentioned earlier. Althoughthis classification will not alter therapeutic strate-gies for the time being, it may enhance our knowl-edge about the disease beyond its puremorphologic aspect.
ETIOLOGIC CLASSIFICATION
This classification is based on the recent under-standing of angio- and vasculogenesis (on thearterial and venous side) and the influence of envi-ronmental and genetic factors. To explain theconcepts of this classification, we propose 3approaches to pediatric vascular malformations:the timing, the target, and the nature of the trig-gering event.
The Triggering Event
The concept of the triggering event is built on theassumption that most pediatric vascular malfor-mations can be considered as congenital mal-formations (ie, malformations or structuralweaknesses of the vessel that have been triggeredor are present before birth and that make thevessel more prone to developing, once a secondhit (or second trigger) occurs, the morphologicand/or clinical vascular lesion). This concept
implies that the malformations are initially quies-cent and may reveal themselves only later in life,which implies a differentiation into primary (orcausative) triggers and secondary (or revealing)triggers. The stages of vascular malformationsbased on this assumption are therefore the prepa-thologic stage, during which no disease exits;however, a window of exposure opens that makesthe cell temporarily vulnerable for an appropriatetriggering event (eg, inflammatory, infectious, radi-ation-induced, toxic, metabolic, or traumatic).During the genetic stage, this appropriate (or caus-ative) trigger for the vascular target and the timeproduces a primary lesion (that may result ina germinal or somatic mutation or a permanentdysfunction of the vessel). If it is neither repairednor leads to cell death, the primary local defect(although for the time being quiescent) is trans-mitted to later generation cells and has a clonalremote effect. At this phase, the disease is notyet morphologically apparent, but is present asa permanent structural weakness. This stage cantherefore be denominated as a biologic or premor-phologic stage. Later in life (in most instancespostnatal), during a new window of exposurewith a secondary (or revealing) trigger, a secondarymutation or an additional dysfunction allows forthe phenotypic expression of the disease. Thissecondary trigger may appear during repeatedvascular remodeling, may be related to shearstress, inflammation or trauma, or may constitutea second (somatic) mutation. At this stage, thedisease manifests itself as a morphologic but notyet clinical entity (eg, incidental finding of an
Krings et al468
unruptured aneurysm). This stage is the morpho-logic or preclinical stage. Only after failure of bio-logic compensation mechanisms (intrinsic repairmechanisms), or during secondary angiopathicchanges (extrinsic risk factors: hemodynamicdisequilibrium, shear stresses), the alreadymorphologically fragile disease will get symptom-atic and enter the clinical, symptomatic stage(Fig. 2).9
Target of the Trigger
Development of blood vessels from differentiatingendothelial cells (EC) is called vasculogenesis,whereas sprouting of new blood vessels from thepreexisting ones is termed angiogenesis. Vascularendothelial growth factor (VEGF) and its receptorVEGFR2 are the most critical drivers of embryonicvessel formation. During vasculogenesis lateraland posterior mesodermal cells migrate towardthe yolk sac. During their migration, the precursorsaggregate to clusters, termed hemangioblasticaggregates. The peripheral cells of these aggre-gates flatten to differentiate into EC, whereas thecentrally located cells differentiate to hematopoi-etic cells of the blood islands. Following this differ-entiation, EC surrounding these blood islandsanastomose to form a capillary meshwork, whichserves as a scaffold for the beginnings of circula-tion, before the heart starts beating.10 It is onlyafter the onset of heartbeat and of blood flowthat the yolk sac capillary plexus is remodeledinto arteries and veins in the now ongoing processof angiogenesis. Historically, it was believed thatthe EC of the primary capillary plexus constituteda homogenous group of cells and that further
Fig. 2. The congenital nature of vascular malformations a
differentiation into arteries and veins occurredbecause of hemodynamic forces. However, inrecent years, several signaling molecules werediscovered, which labeled arterial or venous ECfrom early developmental stages onward, beforethe assembly of a vascular wall. Arterial EC selec-tively express ephrin-B2, neuropilin-1, andmembers of the Notch pathway, whereas othermolecules are specifically expressed in the venoussystem only; some molecules (such as the neuro-pilin-2 receptor) are expressed in early stages byveins and, at later developmental stages, becomerestricted to lymphatic vessels.10 These observa-tions led to the hypothesis that the embryonicvascular system could be predetermined to anarterial, venous, or lymphatic fate from early devel-opmental stages onward (ie, before angiogenesisand after vasculogenesis).11 Arteries, veins, andlymphatic vessels are therefore different, molecu-larly defined targets. It can therefore be easily en-visioned that triggering events are specific foreither the arterial or the venous site. Diseasesthat strike only on the arterial site (aneurysms,dissections) can therefore be differentiated fromdiseases that are targeted against the capillary,venous, or lymphatic vessels.12
Timing of the Trigger
The endothelium and the media of blood vesselsare derived from the mesoderm and the neuralcrest, respectively, with the exception of themesencephalic region and the spinal levels, bothof which originate from mesoderm. These neuralcrest or para-axial mesoderm cells are migratinggroups of cells starting from the segmented
nd the role of triggering events.
Pediatric Cerebral Vascular Malformations 469
regions.13 They course along predetermined pathsin which daughter cells are seeded. When a defectin this migrating cell is present, the defect is trans-mitted to the daughter cells along its migratingpath. The effect, size, area, and severity of thedefect produced by the causative trigger aretherefore related to the timing of the event in rela-tion to the migration; the earlier the hit, the largerthe effect on the vessels with a more widespreadand severe vascular lesion. Vice versa, the laterthe hit, the more focal the effect and the moreconfined the vascular lesion. Although a germinalmutation is present in all cells, an early somaticmutation may lead to various stages of metameri-cally arranged defects, whereas a postnatal muta-tion affects only a small cluster of cells. Althoughcongenital, some of these mutations may be re-vealed only later in life (such as in a failed remod-eling during vascular renewal).
In the early embryonic vessel configuration (ie,during the early stages of angiogenesis and afterthe heart started beating) not all capillaries areintegrated into the primitive circulation. In thisperiod, the primitive circulation consists of directtransitions of arteries into veins; arterial andvenous blood can flow through the same vascularchannel.10 This embryonic circulation is thereforedifferent from the adult situation (in which bloodflows through arteries into arterioles, a capillarybed, and through successively larger veins backto the heart). If this embryonic arterial-venousvessel configuration persists, large arterial-venousshunts will develop (which may be the case incertain fistulous malformations of the brain andspine). With further development of the vascula-ture (ie, in later embryonic and fetal stages), thearea of the shunt may become more confined,again revealing the importance of the timing of
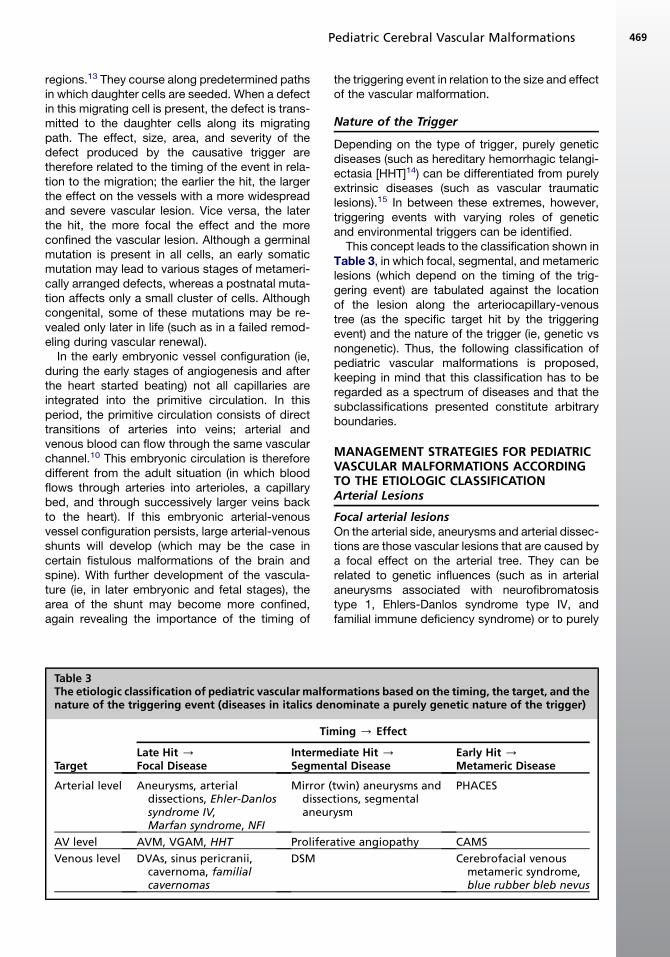
Table 3The etiologic classification of pediatric vascular malfonature of the triggering event (diseases in italics den
the triggering event in relation to the size and effectof the vascular malformation.
Nature of the Trigger
Depending on the type of trigger, purely geneticdiseases (such as hereditary hemorrhagic telangi-ectasia [HHT]14) can be differentiated from purelyextrinsic diseases (such as vascular traumaticlesions).15 In between these extremes, however,triggering events with varying roles of geneticand environmental triggers can be identified.
This concept leads to the classification shown inTable 3, in which focal, segmental, and metamericlesions (which depend on the timing of the trig-gering event) are tabulated against the locationof the lesion along the arteriocapillary-venoustree (as the specific target hit by the triggeringevent) and the nature of the trigger (ie, genetic vsnongenetic). Thus, the following classification ofpediatric vascular malformations is proposed,keeping in mind that this classification has to beregarded as a spectrum of diseases and that thesubclassifications presented constitute arbitraryboundaries.
MANAGEMENT STRATEGIES FOR PEDIATRICVASCULAR MALFORMATIONS ACCORDINGTO THE ETIOLOGIC CLASSIFICATIONArterial Lesions
Focal arterial lesionsOn the arterial side, aneurysms and arterial dissec-tions are those vascular lesions that are caused bya focal effect on the arterial tree. They can berelated to genetic influences (such as in arterialaneurysms associated with neurofibromatosistype 1, Ehlers-Danlos syndrome type IV, andfamilial immune deficiency syndrome) or to purely
rmations based on the timing, the target, and theominate a purely genetic nature of the trigger)
environmental factors (such as vascular trauma).Presumably most arterial aneurysms and dissec-tions in the pediatric age-group are related to envi-ronmental and genetic influences with intrinsicpredisposing factors such as segmental vulnera-bility, wall matrix failure, and altered repair mecha-nisms on the one hand, and extrinsic triggeringfactors such as inflammation, (minor) trauma,and autoimmune-related causes on the other(Fig. 3).16,17 Although the complete description oftreatment strategies in pediatric aneurysms isbeyond the scope of this article, their (dissecting,traumatic, or infectious) nature often leads to thenecessity of parent vessel occlusion with the riskof subsequent stroke. Because the diseaseprocess (given its cause) is in most cases locatedin the vessel wall, a purely endoluminal treatment(ie, coiling of the aneurysm) is successful only inpatients in whom true saccular aneurysms arepresent. Most aneurysms, however, area symptom rather than the disease itself and there-fore require a more thorough evaluation of theircause before treatment (Fig. 4).
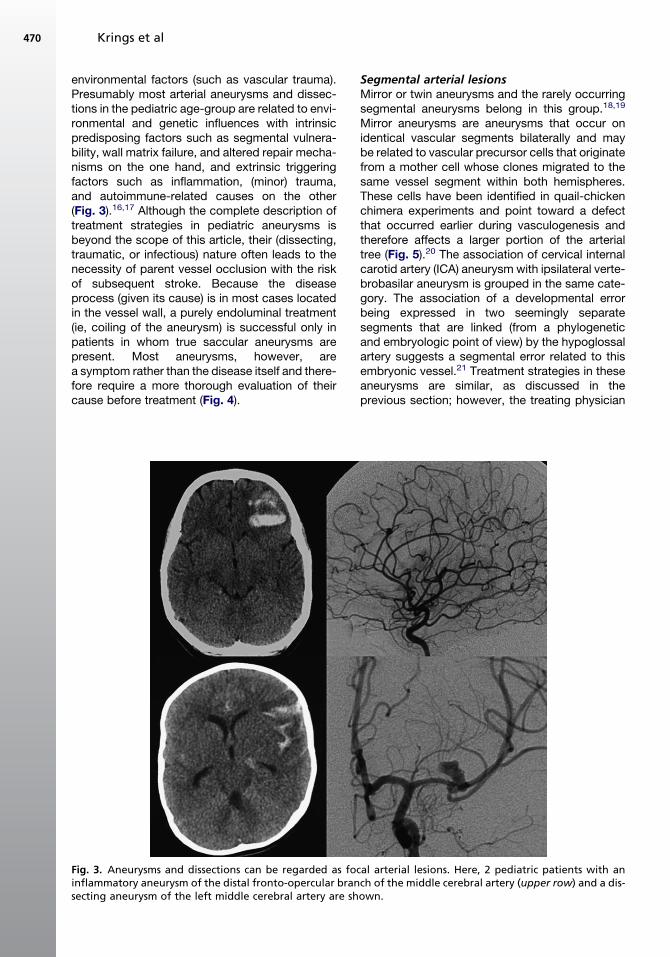
Fig. 3. Aneurysms and dissections can be regarded as focinflammatory aneurysm of the distal fronto-opercular bransecting aneurysm of the left middle cerebral artery are sh
Segmental arterial lesionsMirror or twin aneurysms and the rarely occurringsegmental aneurysms belong in this group.18,19
Mirror aneurysms are aneurysms that occur onidentical vascular segments bilaterally and maybe related to vascular precursor cells that originatefrom a mother cell whose clones migrated to thesame vessel segment within both hemispheres.These cells have been identified in quail-chickenchimera experiments and point toward a defectthat occurred earlier during vasculogenesis andtherefore affects a larger portion of the arterialtree (Fig. 5).20 The association of cervical internalcarotid artery (ICA) aneurysm with ipsilateral verte-brobasilar aneurysm is grouped in the same cate-gory. The association of a developmental errorbeing expressed in two seemingly separatesegments that are linked (from a phylogeneticand embryologic point of view) by the hypoglossalartery suggests a segmental error related to thisembryonic vessel.21 Treatment strategies in theseaneurysms are similar, as discussed in theprevious section; however, the treating physician
al arterial lesions. Here, 2 pediatric patients with anch of the middle cerebral artery (upper row) and a dis-own.
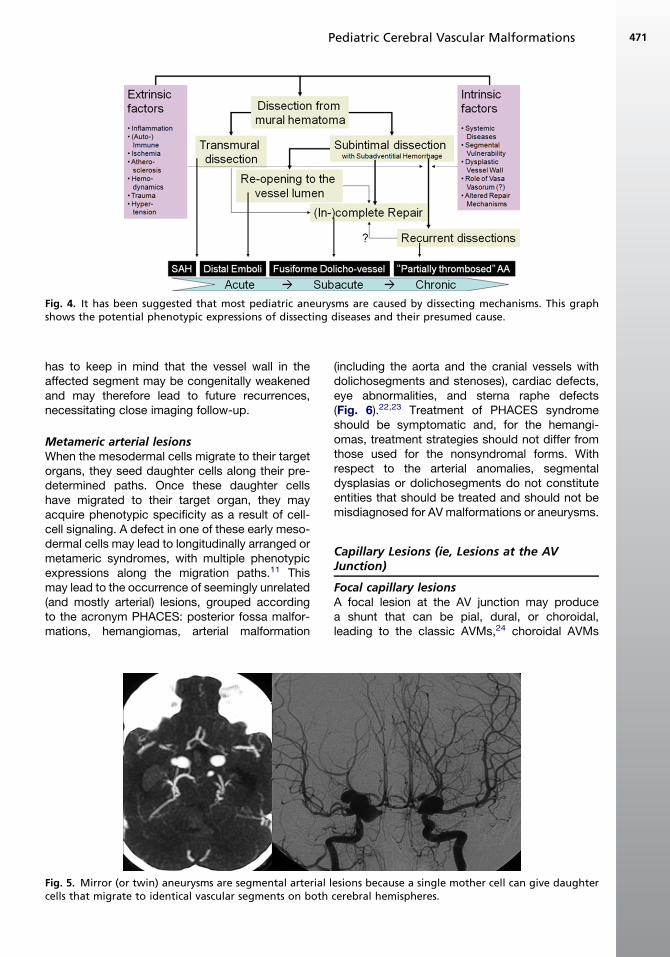
Fig. 4. It has been suggested that most pediatric aneurysms are caused by dissecting mechanisms. This graphshows the potential phenotypic expressions of dissecting diseases and their presumed cause.
Pediatric Cerebral Vascular Malformations 471
has to keep in mind that the vessel wall in theaffected segment may be congenitally weakenedand may therefore lead to future recurrences,necessitating close imaging follow-up.
Metameric arterial lesionsWhen the mesodermal cells migrate to their targetorgans, they seed daughter cells along their pre-determined paths. Once these daughter cellshave migrated to their target organ, they mayacquire phenotypic specificity as a result of cell-cell signaling. A defect in one of these early meso-dermal cells may lead to longitudinally arranged ormetameric syndromes, with multiple phenotypicexpressions along the migration paths.11 Thismay lead to the occurrence of seemingly unrelated(and mostly arterial) lesions, grouped accordingto the acronym PHACES: posterior fossa malfor-mations, hemangiomas, arterial malformation
Fig. 5. Mirror (or twin) aneurysms are segmental arterial lcells that migrate to identical vascular segments on both
(including the aorta and the cranial vessels withdolichosegments and stenoses), cardiac defects,eye abnormalities, and sterna raphe defects(Fig. 6).22,23 Treatment of PHACES syndromeshould be symptomatic and, for the hemangi-omas, treatment strategies should not differ fromthose used for the nonsyndromal forms. Withrespect to the arterial anomalies, segmentaldysplasias or dolichosegments do not constituteentities that should be treated and should not bemisdiagnosed for AV malformations or aneurysms.
Capillary Lesions (ie, Lesions at the AVJunction)
Focal capillary lesionsA focal lesion at the AV junction may producea shunt that can be pial, dural, or choroidal,leading to the classic AVMs,24 choroidal AVMs
esions because a single mother cell can give daughtercerebral hemispheres.
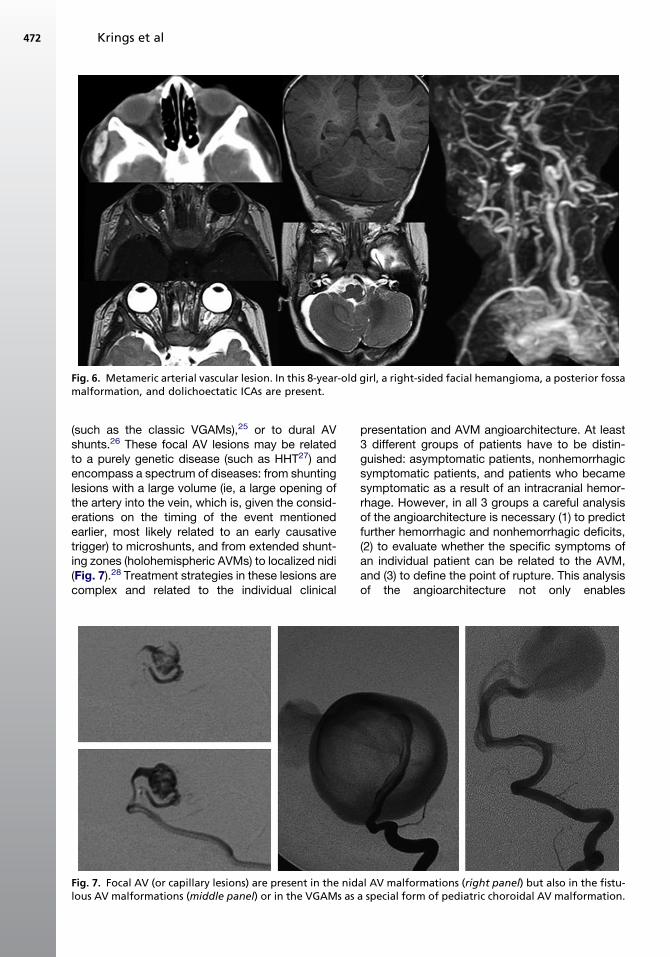
Fig. 6. Metameric arterial vascular lesion. In this 8-year-old girl, a right-sided facial hemangioma, a posterior fossamalformation, and dolichoectatic ICAs are present.
Krings et al472
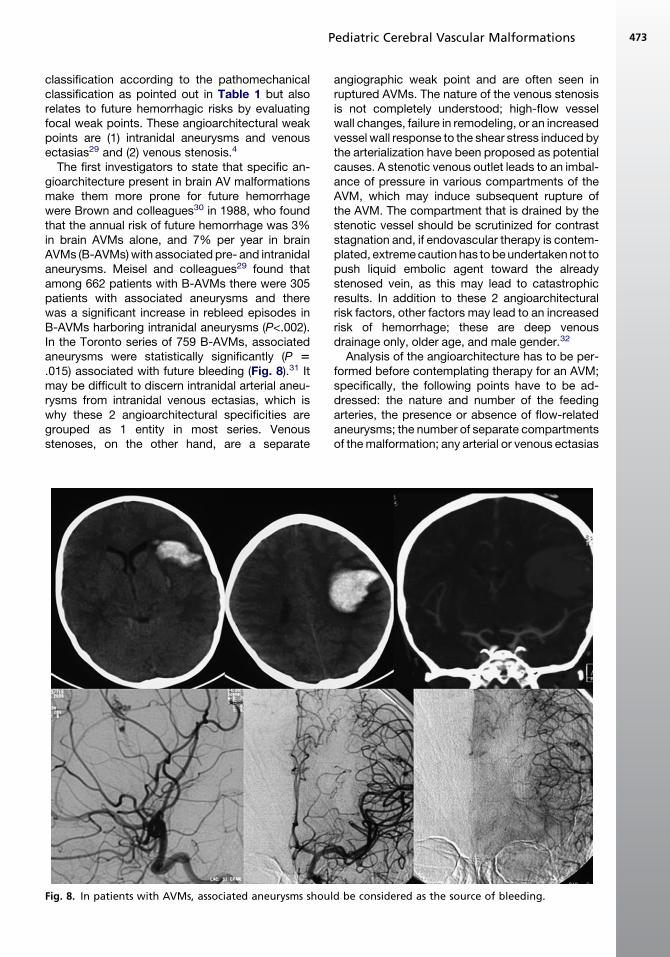
(such as the classic VGAMs),25 or to dural AVshunts.26 These focal AV lesions may be relatedto a purely genetic disease (such as HHT27) andencompass a spectrum of diseases: from shuntinglesions with a large volume (ie, a large opening ofthe artery into the vein, which is, given the consid-erations on the timing of the event mentionedearlier, most likely related to an early causativetrigger) to microshunts, and from extended shunt-ing zones (holohemispheric AVMs) to localized nidi(Fig. 7).28 Treatment strategies in these lesions arecomplex and related to the individual clinical
Fig. 7. Focal AV (or capillary lesions) are present in the nidlous AV malformations (middle panel) or in the VGAMs as
presentation and AVM angioarchitecture. At least3 different groups of patients have to be distin-guished: asymptomatic patients, nonhemorrhagicsymptomatic patients, and patients who becamesymptomatic as a result of an intracranial hemor-rhage. However, in all 3 groups a careful analysisof the angioarchitecture is necessary (1) to predictfurther hemorrhagic and nonhemorrhagic deficits,(2) to evaluate whether the specific symptoms ofan individual patient can be related to the AVM,and (3) to define the point of rupture. This analysisof the angioarchitecture not only enables
al AV malformations (right panel) but also in the fistu-a special form of pediatric choroidal AV malformation.
Pediatric Cerebral Vascular Malformations 473
classification according to the pathomechanicalclassification as pointed out in Table 1 but alsorelates to future hemorrhagic risks by evaluatingfocal weak points. These angioarchitectural weakpoints are (1) intranidal aneurysms and venousectasias29 and (2) venous stenosis.4
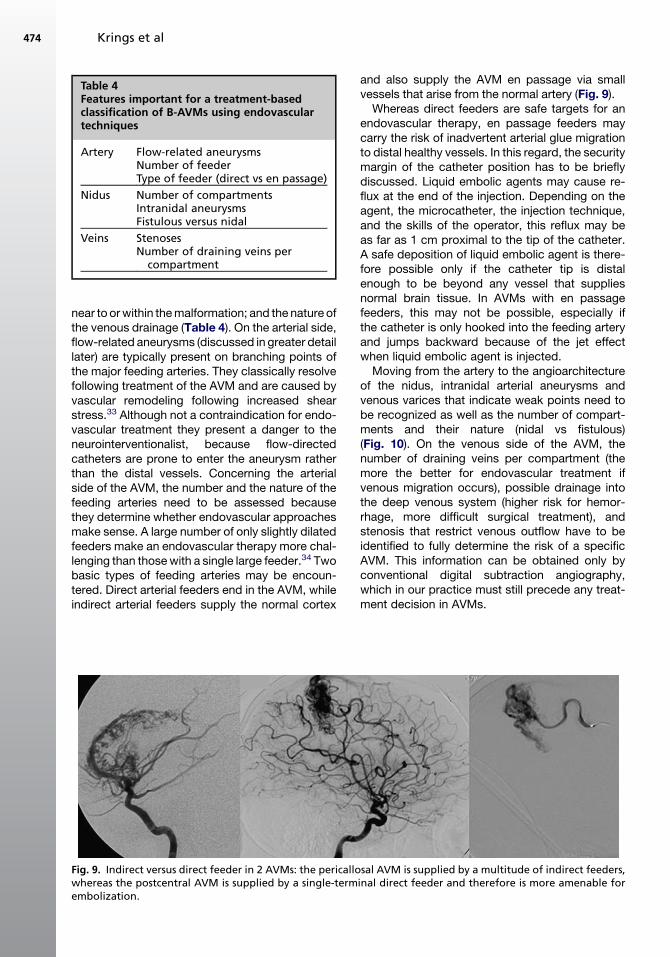
The first investigators to state that specific an-gioarchitecture present in brain AV malformationsmake them more prone for future hemorrhagewere Brown and colleagues30 in 1988, who foundthat the annual risk of future hemorrhage was 3%in brain AVMs alone, and 7% per year in brainAVMs (B-AVMs) with associated pre- and intranidalaneurysms. Meisel and colleagues29 found thatamong 662 patients with B-AVMs there were 305patients with associated aneurysms and therewas a significant increase in rebleed episodes inB-AVMs harboring intranidal aneurysms (P<.002).In the Toronto series of 759 B-AVMs, associatedaneurysms were statistically significantly (P 5.015) associated with future bleeding (Fig. 8).31 Itmay be difficult to discern intranidal arterial aneu-rysms from intranidal venous ectasias, which iswhy these 2 angioarchitectural specificities aregrouped as 1 entity in most series. Venousstenoses, on the other hand, are a separate
Fig. 8. In patients with AVMs, associated aneurysms shou
angiographic weak point and are often seen inruptured AVMs. The nature of the venous stenosisis not completely understood; high-flow vesselwall changes, failure in remodeling, or an increasedvessel wall response to the shear stress induced bythe arterialization have been proposed as potentialcauses. A stenotic venous outlet leads to an imbal-ance of pressure in various compartments of theAVM, which may induce subsequent rupture ofthe AVM. The compartment that is drained by thestenotic vessel should be scrutinized for contraststagnation and, if endovascular therapy is contem-plated, extreme caution has to be undertaken not topush liquid embolic agent toward the alreadystenosed vein, as this may lead to catastrophicresults. In addition to these 2 angioarchitecturalrisk factors, other factors may lead to an increasedrisk of hemorrhage; these are deep venousdrainage only, older age, and male gender.32
Analysis of the angioarchitecture has to be per-formed before contemplating therapy for an AVM;specifically, the following points have to be ad-dressed: the nature and number of the feedingarteries, the presence or absence of flow-relatedaneurysms; the number of separate compartmentsof the malformation; any arterial or venous ectasias
ld be considered as the source of bleeding.
Table 4Features important for a treatment-basedclassification of B-AVMs using endovasculartechniques
Artery Flow-related aneurysmsNumber of feederType of feeder (direct vs en passage)
Nidus Number of compartmentsIntranidal aneurysmsFistulous versus nidal
Veins StenosesNumber of draining veins per
compartment
Krings et al474
near to or within the malformation; and the nature ofthe venous drainage (Table 4). On the arterial side,flow-related aneurysms (discussed in greater detaillater) are typically present on branching points ofthe major feeding arteries. They classically resolvefollowing treatment of the AVM and are caused byvascular remodeling following increased shearstress.33 Although not a contraindication for endo-vascular treatment they present a danger to theneurointerventionalist, because flow-directedcatheters are prone to enter the aneurysm ratherthan the distal vessels. Concerning the arterialside of the AVM, the number and the nature of thefeeding arteries need to be assessed becausethey determine whether endovascular approachesmake sense. A large number of only slightly dilatedfeeders make an endovascular therapy more chal-lenging than those with a single large feeder.34 Twobasic types of feeding arteries may be encoun-tered. Direct arterial feeders end in the AVM, whileindirect arterial feeders supply the normal cortex
Fig. 9. Indirect versus direct feeder in 2 AVMs: the pericallowhereas the postcentral AVM is supplied by a single-termembolization.
and also supply the AVM en passage via smallvessels that arise from the normal artery (Fig. 9).
Whereas direct feeders are safe targets for anendovascular therapy, en passage feeders maycarry the risk of inadvertent arterial glue migrationto distal healthy vessels. In this regard, the securitymargin of the catheter position has to be brieflydiscussed. Liquid embolic agents may cause re-flux at the end of the injection. Depending on theagent, the microcatheter, the injection technique,and the skills of the operator, this reflux may beas far as 1 cm proximal to the tip of the catheter.A safe deposition of liquid embolic agent is there-fore possible only if the catheter tip is distalenough to be beyond any vessel that suppliesnormal brain tissue. In AVMs with en passagefeeders, this may not be possible, especially ifthe catheter is only hooked into the feeding arteryand jumps backward because of the jet effectwhen liquid embolic agent is injected.
Moving from the artery to the angioarchitectureof the nidus, intranidal arterial aneurysms andvenous varices that indicate weak points need tobe recognized as well as the number of compart-ments and their nature (nidal vs fistulous)(Fig. 10). On the venous side of the AVM, thenumber of draining veins per compartment (themore the better for endovascular treatment ifvenous migration occurs), possible drainage intothe deep venous system (higher risk for hemor-rhage, more difficult surgical treatment), andstenosis that restrict venous outflow have to beidentified to fully determine the risk of a specificAVM. This information can be obtained only byconventional digital subtraction angiography,which in our practice must still precede any treat-ment decision in AVMs.
sal AVM is supplied by a multitude of indirect feeders,inal direct feeder and therefore is more amenable for
Fig. 10. Whether a nidal or a fistulous transition between arteries and veins is present can in most instances beseen from the MRI alone. This factor has major implications on the pathophysiology and on the choice of treat-ment modalities.
Pediatric Cerebral Vascular Malformations 475
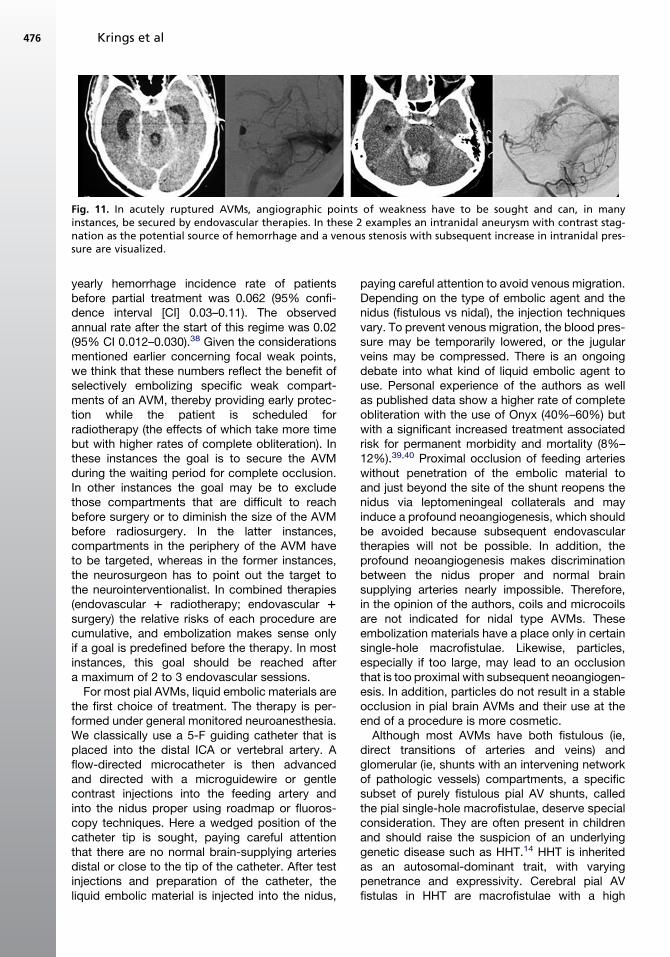
A complete cure of a pial brain AVM by endo-vascular means is possible in approximately 20%of all AVMs irrespective of their angioarchitec-ture.35–37 Those AVMs that are favorable toa complete cure are the small, single-feeder,single-compartment AVMs that have a directfeeding artery. Because these AVMs are alsogood candidates for radiosurgery and open neuro-surgery, a tailored team approach is preferable foreach specific AVM in each individual patient,respecting their wishes and taking into consider-ation the clinical presentation. In most instances,endovascular therapies are used to diminish thesize of an AVM before radiotherapy or surgery, tosecure focal weak points in the acute andsubacute stage of ruptured AVMs (Fig. 11) and inunruptured AVMs in which radiosurgery is contem-plated, or to exclude those compartments of an
AVM that may be difficult to reach during surgery.Once treatment for an AVM is decided upon,a pathway to its complete exclusion has to beagreed on by the treatment team, which shouldinclude radiosurgeons, vascular neurosurgeons,and neurointerventionalists. It does not makesense in our opinion to partially treat an AVMwithout a strategy on how to handle a possibleresidual of the AVM.
If endovascular therapy is chosen, we proceedwith a predefined goal, which may mean perform-ing what has been termed a partially targetedembolization. Such rationale is based on theoutcome of a series of more than 600 patientswith AVMs who were partially embolized andshowed a significant decrease in hemorrhageepisodes when compared with the conservativelytreated series reported in the literature.38 The
Fig. 11. In acutely ruptured AVMs, angiographic points of weakness have to be sought and can, in manyinstances, be secured by endovascular therapies. In these 2 examples an intranidal aneurysm with contrast stag-nation as the potential source of hemorrhage and a venous stenosis with subsequent increase in intranidal pres-sure are visualized.
Krings et al476
yearly hemorrhage incidence rate of patientsbefore partial treatment was 0.062 (95% confi-dence interval [CI] 0.03–0.11). The observedannual rate after the start of this regime was 0.02(95% CI 0.012–0.030).38 Given the considerationsmentioned earlier concerning focal weak points,we think that these numbers reflect the benefit ofselectively embolizing specific weak compart-ments of an AVM, thereby providing early protec-tion while the patient is scheduled forradiotherapy (the effects of which take more timebut with higher rates of complete obliteration). Inthese instances the goal is to secure the AVMduring the waiting period for complete occlusion.In other instances the goal may be to excludethose compartments that are difficult to reachbefore surgery or to diminish the size of the AVMbefore radiosurgery. In the latter instances,compartments in the periphery of the AVM haveto be targeted, whereas in the former instances,the neurosurgeon has to point out the target tothe neurointerventionalist. In combined therapies(endovascular 1 radiotherapy; endovascular 1surgery) the relative risks of each procedure arecumulative, and embolization makes sense onlyif a goal is predefined before the therapy. In mostinstances, this goal should be reached aftera maximum of 2 to 3 endovascular sessions.
For most pial AVMs, liquid embolic materials arethe first choice of treatment. The therapy is per-formed under general monitored neuroanesthesia.We classically use a 5-F guiding catheter that isplaced into the distal ICA or vertebral artery. Aflow-directed microcatheter is then advancedand directed with a microguidewire or gentlecontrast injections into the feeding artery andinto the nidus proper using roadmap or fluoros-copy techniques. Here a wedged position of thecatheter tip is sought, paying careful attentionthat there are no normal brain-supplying arteriesdistal or close to the tip of the catheter. After testinjections and preparation of the catheter, theliquid embolic material is injected into the nidus,
paying careful attention to avoid venous migration.Depending on the type of embolic agent and thenidus (fistulous vs nidal), the injection techniquesvary. To prevent venous migration, the blood pres-sure may be temporarily lowered, or the jugularveins may be compressed. There is an ongoingdebate into what kind of liquid embolic agent touse. Personal experience of the authors as wellas published data show a higher rate of completeobliteration with the use of Onyx (40%–60%) butwith a significant increased treatment associatedrisk for permanent morbidity and mortality (8%–12%).39,40 Proximal occlusion of feeding arterieswithout penetration of the embolic material toand just beyond the site of the shunt reopens thenidus via leptomeningeal collaterals and mayinduce a profound neoangiogenesis, which shouldbe avoided because subsequent endovasculartherapies will not be possible. In addition, theprofound neoangiogenesis makes discriminationbetween the nidus proper and normal brainsupplying arteries nearly impossible. Therefore,in the opinion of the authors, coils and microcoilsare not indicated for nidal type AVMs. Theseembolization materials have a place only in certainsingle-hole macrofistulae. Likewise, particles,especially if too large, may lead to an occlusionthat is too proximal with subsequent neoangiogen-esis. In addition, particles do not result in a stableocclusion in pial brain AVMs and their use at theend of a procedure is more cosmetic.
Although most AVMs have both fistulous (ie,direct transitions of arteries and veins) andglomerular (ie, shunts with an intervening networkof pathologic vessels) compartments, a specificsubset of purely fistulous pial AV shunts, calledthe pial single-hole macrofistulae, deserve specialconsideration. They are often present in childrenand should raise the suspicion of an underlyinggenetic disease such as HHT.14 HHT is inheritedas an autosomal-dominant trait, with varyingpenetrance and expressivity. Cerebral pial AVfistulas in HHT are macrofistulae with a high
Pediatric Cerebral Vascular Malformations 477
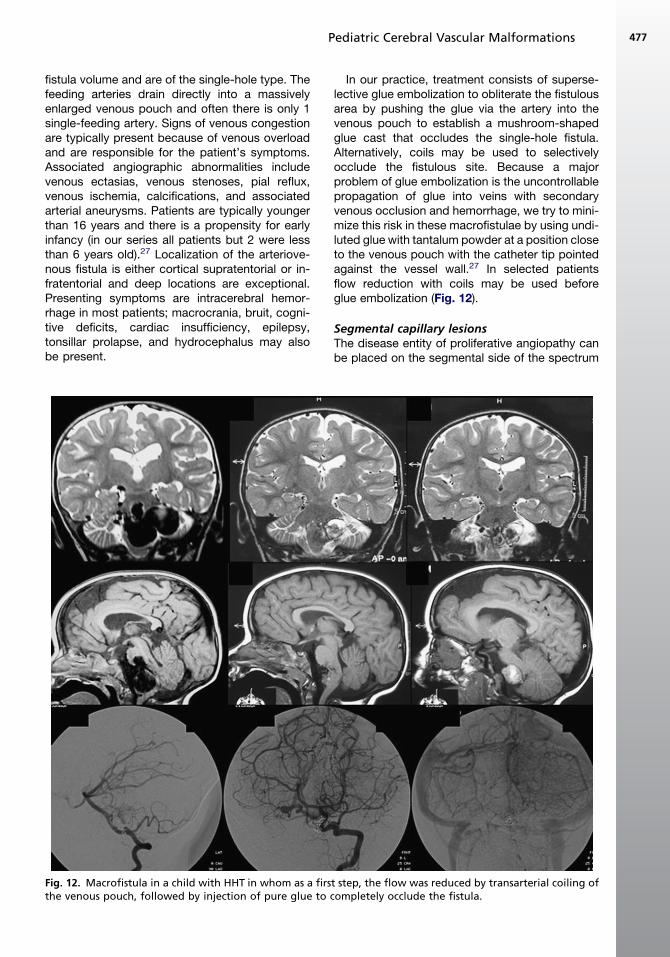
fistula volume and are of the single-hole type. Thefeeding arteries drain directly into a massivelyenlarged venous pouch and often there is only 1single-feeding artery. Signs of venous congestionare typically present because of venous overloadand are responsible for the patient’s symptoms.Associated angiographic abnormalities includevenous ectasias, venous stenoses, pial reflux,venous ischemia, calcifications, and associatedarterial aneurysms. Patients are typically youngerthan 16 years and there is a propensity for earlyinfancy (in our series all patients but 2 were lessthan 6 years old).27 Localization of the arteriove-nous fistula is either cortical supratentorial or in-fratentorial and deep locations are exceptional.Presenting symptoms are intracerebral hemor-rhage in most patients; macrocrania, bruit, cogni-tive deficits, cardiac insufficiency, epilepsy,tonsillar prolapse, and hydrocephalus may alsobe present.
Fig. 12. Macrofistula in a child with HHT in whom as a firsthe venous pouch, followed by injection of pure glue to
In our practice, treatment consists of superse-lective glue embolization to obliterate the fistulousarea by pushing the glue via the artery into thevenous pouch to establish a mushroom-shapedglue cast that occludes the single-hole fistula.Alternatively, coils may be used to selectivelyocclude the fistulous site. Because a majorproblem of glue embolization is the uncontrollablepropagation of glue into veins with secondaryvenous occlusion and hemorrhage, we try to mini-mize this risk in these macrofistulae by using undi-luted glue with tantalum powder at a position closeto the venous pouch with the catheter tip pointedagainst the vessel wall.27 In selected patientsflow reduction with coils may be used beforeglue embolization (Fig. 12).
Segmental capillary lesionsThe disease entity of proliferative angiopathy canbe placed on the segmental side of the spectrum
t step, the flow was reduced by transarterial coiling ofcompletely occlude the fistula.
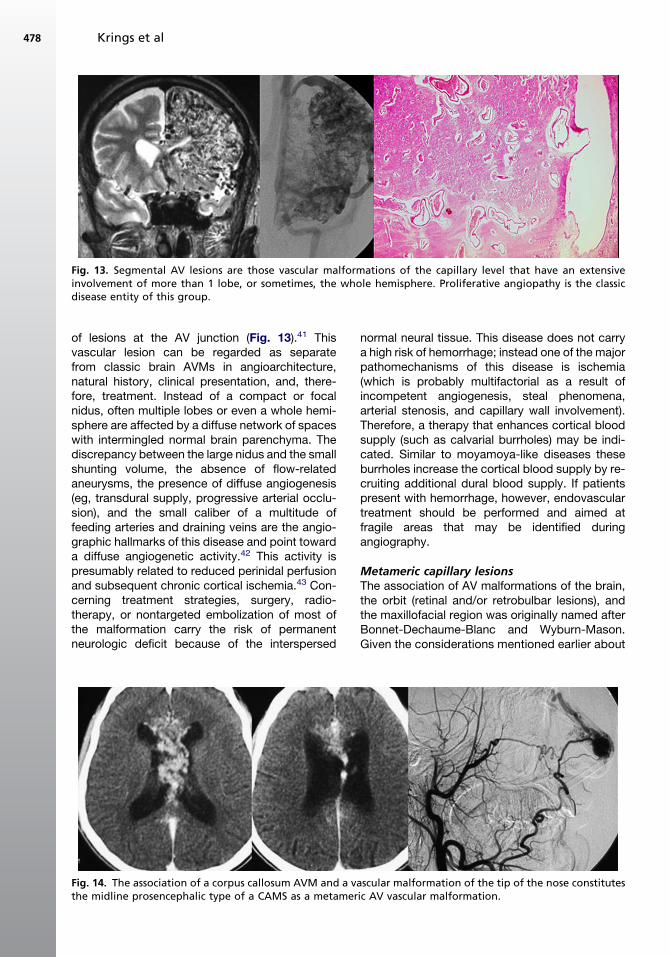
Fig. 13. Segmental AV lesions are those vascular malformations of the capillary level that have an extensiveinvolvement of more than 1 lobe, or sometimes, the whole hemisphere. Proliferative angiopathy is the classicdisease entity of this group.
Krings et al478
of lesions at the AV junction (Fig. 13).41 Thisvascular lesion can be regarded as separatefrom classic brain AVMs in angioarchitecture,natural history, clinical presentation, and, there-fore, treatment. Instead of a compact or focalnidus, often multiple lobes or even a whole hemi-sphere are affected by a diffuse network of spaceswith intermingled normal brain parenchyma. Thediscrepancy between the large nidus and the smallshunting volume, the absence of flow-relatedaneurysms, the presence of diffuse angiogenesis(eg, transdural supply, progressive arterial occlu-sion), and the small caliber of a multitude offeeding arteries and draining veins are the angio-graphic hallmarks of this disease and point towarda diffuse angiogenetic activity.42 This activity ispresumably related to reduced perinidal perfusionand subsequent chronic cortical ischemia.43 Con-cerning treatment strategies, surgery, radio-therapy, or nontargeted embolization of most ofthe malformation carry the risk of permanentneurologic deficit because of the interspersed
Fig. 14. The association of a corpus callosum AVM and a vathe midline prosencephalic type of a CAMS as a metamer
normal neural tissue. This disease does not carrya high risk of hemorrhage; instead one of the majorpathomechanisms of this disease is ischemia(which is probably multifactorial as a result ofincompetent angiogenesis, steal phenomena,arterial stenosis, and capillary wall involvement).Therefore, a therapy that enhances cortical bloodsupply (such as calvarial burrholes) may be indi-cated. Similar to moyamoya-like diseases theseburrholes increase the cortical blood supply by re-cruiting additional dural blood supply. If patientspresent with hemorrhage, however, endovasculartreatment should be performed and aimed atfragile areas that may be identified duringangiography.
Metameric capillary lesionsThe association of AV malformations of the brain,the orbit (retinal and/or retrobulbar lesions), andthe maxillofacial region was originally named afterBonnet-Dechaume-Blanc and Wyburn-Mason.Given the considerations mentioned earlier about
scular malformation of the tip of the nose constitutesic AV vascular malformation.
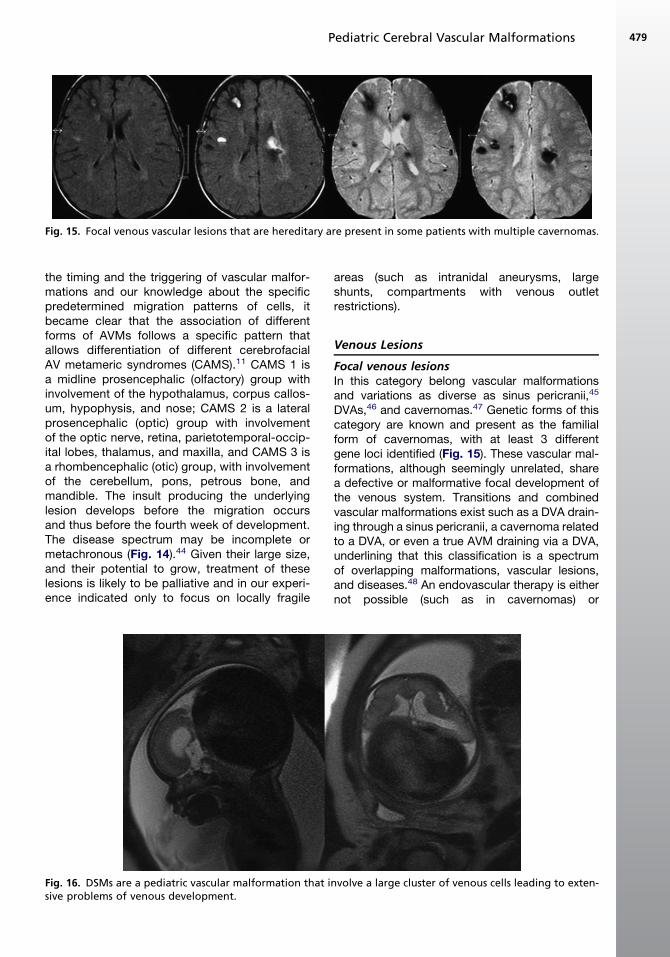
Fig. 15. Focal venous vascular lesions that are hereditary are present in some patients with multiple cavernomas.
Pediatric Cerebral Vascular Malformations 479
the timing and the triggering of vascular malfor-mations and our knowledge about the specificpredetermined migration patterns of cells, itbecame clear that the association of differentforms of AVMs follows a specific pattern thatallows differentiation of different cerebrofacialAV metameric syndromes (CAMS).11 CAMS 1 isa midline prosencephalic (olfactory) group withinvolvement of the hypothalamus, corpus callos-um, hypophysis, and nose; CAMS 2 is a lateralprosencephalic (optic) group with involvementof the optic nerve, retina, parietotemporal-occip-ital lobes, thalamus, and maxilla, and CAMS 3 isa rhombencephalic (otic) group, with involvementof the cerebellum, pons, petrous bone, andmandible. The insult producing the underlyinglesion develops before the migration occursand thus before the fourth week of development.The disease spectrum may be incomplete ormetachronous (Fig. 14).44 Given their large size,and their potential to grow, treatment of theselesions is likely to be palliative and in our experi-ence indicated only to focus on locally fragile
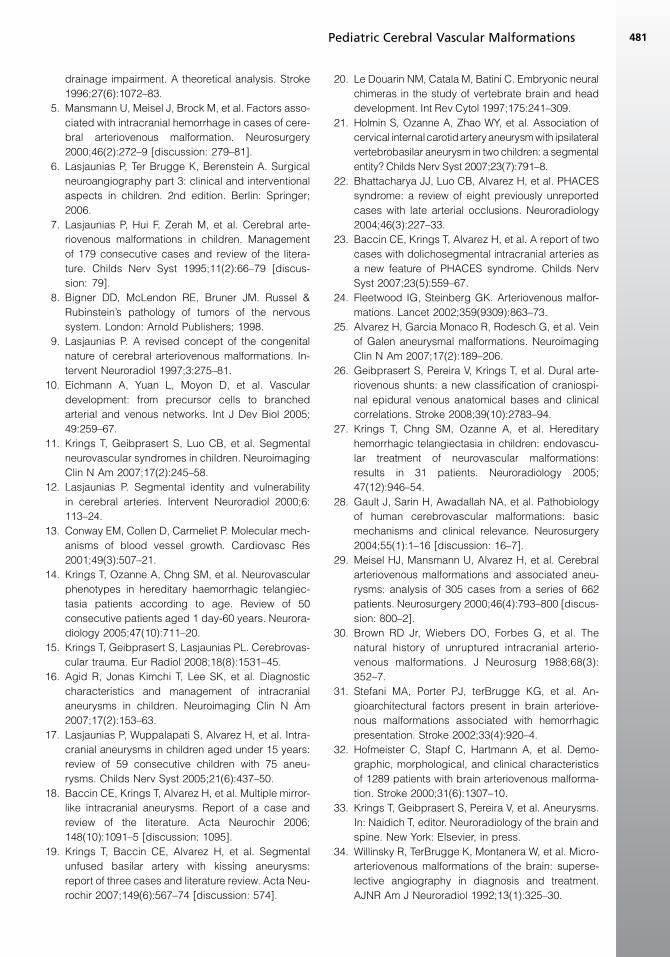
Fig. 16. DSMs are a pediatric vascular malformation that isive problems of venous development.
areas (such as intranidal aneurysms, largeshunts, compartments with venous outletrestrictions).
Venous Lesions
Focal venous lesionsIn this category belong vascular malformationsand variations as diverse as sinus pericranii,45
DVAs,46 and cavernomas.47 Genetic forms of thiscategory are known and present as the familialform of cavernomas, with at least 3 differentgene loci identified (Fig. 15). These vascular mal-formations, although seemingly unrelated, sharea defective or malformative focal development ofthe venous system. Transitions and combinedvascular malformations exist such as a DVA drain-ing through a sinus pericranii, a cavernoma relatedto a DVA, or even a true AVM draining via a DVA,underlining that this classification is a spectrumof overlapping malformations, vascular lesions,and diseases.48 An endovascular therapy is eithernot possible (such as in cavernomas) or
nvolve a large cluster of venous cells leading to exten-
Fig. 17. Sturge-Weber syndrome can be subsumed under metameric nonhereditary venous lesions given theirinvolvement of the face, the choroid plexus, and the cortical veins.
Krings et al480
contraindicated (such as in most DVAs and sinuspericranii given their role in the drainage of thebrain).
Segmental venous lesionsIf the venous lesion affects a larger cluster of cells,more severe venous defects are encountered. Theclassic example is DSMs,49 in which the develop-ment of the dural sinuses is affected (Fig. 16). Thisdisease leads not only to sinus wall overgrowthand epidural confluences of venous spaces withgiant lakes but also to cavernomas, sinus pericra-nii, DVAs, and maxillofacial malformations. The AVshunts associated with DSM add to the venouscongestion of the normal brain.50 Therefore treat-ment is targeted toward reduction of the shuntvia a transarterial approach.
Metameric venous lesionsThe encephalotrigeminal angiomatosis or Sturge-Weber syndrome is a nonfamilial disease witha skin discoloration (port wine) in the V1 territoryassociated with a calcified leptomeningeal venousmalformation of the ipsilateral supratentorial hemi-sphere, which (in relation to the CAMS mentionedearlier) may be termed cerebrofacial venous meta-meric syndrome.11 Associated with the classicfacial portwine stain are intracranial vascularanomalies that consist of cortical venous throm-bosis with capillary venous proliferation andenlargement of the transmedullary collateralvenous drainage with or without choroid plexushypertrophy (Fig. 17). A genetic disease that fallsinto the metameric venous lesion group is theblue rubber bleb nevus syndrome, which involvesmultiple venous lesions (such as DVAs).51 Endo-vascular therapies are not established for thesediseases.
SUMMARY
The proposed classification may add to our under-standing of vascular malformations because thephenotypic expression of a given vascular diseasecan shed light on the nature and timing of the trig-gering event, thereby potentially opening up treat-ment modalities that are directed against thetriggering event rather than against the clinicalmanifestations or the morphologic appearance.In addition, the proposed classification may shedlight on the prognosis and pathomechanisms ofcertain vascular malformations and may, there-fore, lead to better treatment of the child afflictedwith these rare and difficult diseases. For thetime being, treatment in many instances is stillrelated only to the symptoms of the disease, notto the disease process itself. However, with themethods at hand, most vascular diseases cannowadays be approached safely and with goodclinical results.
REFERENCES
1. Kader A, Young WL. The effects of intracranial arte-
riovenous malformations on cerebral hemody-
namics. Neurosurg Clin N Am 1996;7:767–81.
2. Geibprasert S, Pereira V, Krings T, et al. Hydroceph-