28
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 1 of 28 Client Information Packet
| Date post: | 21-Aug-2018 |
| Category: |
Documents |
| Upload: | doannguyet |
| View: | 220 times |
| Download: | 0 times |

The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 1 of 28
Client Information Packet

Kali’s Initial Information Worksheet
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 2 of 28
Your Name CYS Worker
Child's Information1 Case Number 12342 Full Name Kali3 Sex Female4 SSN 333-33-33335 DOB 1/1/19936 Date of Removal 6/10/20007 Date of Return Home8 Citizenship US Citizen9 Race WH-WHITE
10 Type of Placement Substitute Care11 Removed from home of: Martha12 Address: full 123 State Street, PA 13 Relationship to Child: Mother14 SSN 111-11-111115 Is child of Hispanic Origin? No16 Telephone # (888) 888-888817 School District?18 Grade19 Has child ever been diagnosed with a disability
If yes, what disability?20 Has child ever been adopted?
If yes, at what age?21 Was child's mother married at time of child's birth?22 County and hospital where birth occurred23 Family structure removed from24 Does child have an ACCESS card?
If yes, ACCESS #25 Does child have private insurance?
If yes, Company name, address, policy #26 Does child have available income/resources?
If yes, specify cash, child support, SS, SSI, Auto , savings, VA benfits, unemploym, and $$
Parent Information:1 Father's Name unknown2 Father's Address unknown3 Father's DOB unknown4 Father's SS# unknown5 Father's phone #6 Is father employed?
If yes, where?7 Full -time or part-time?8 Father's gross monthly income
1 Mother's Name Martha2 Mother's Address 123 State Street, PA3 Mother's DOB 12/12/19694 Mother's SS# 111-11-11115 Mother's phone # (888) 888-88886 Is mother employed?
If yes, where?7 Full -time or part-time?8 Mother's gross monthly income9 Mother's maiden name
Initial Information Worksheet
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO

Kali’s Initial Information Worksheet, Cont’d
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 3 of 28
Step-parent Information
1 Step-parent name Doug2 Step-parent address 123 State Street, PA3 Step-parent SS# 3/3/19664 Step-parent DOB 222-22-22225 Step-parent phone # (888) 888-88886 Is step-parent employed?
If yes, where?7 Full-time or part-time?8 Step-parent Gross monthly income?
Household Information1 List household members, relationship to child, DOB, and SS number
Martha, Mother 12/12/1969, 111-11-1111
Doug, Step - Father 03/03/1966, 222-22-2222
Kali, Child 01/01/1993, 333-33-3333
Angela, Sister 05/16/1995, 444-44-4444
Jade, Sister 02/11/1986, 555-55-5555
Steven, Stepbrother 06/06/1988, 666-66-6666
2 Does anyone in the family receive Cash assistance,SSI, Foodstamps, or Medicaid? FS - $400.00/month, Cash - $350.00/monthIf yes, specify benefit, amount and case #'s Medicaid
3 Does anyone in the family receive Child Support?If yes, specify child's name and monthly amount
4 Do you own a vehicle?If yes, what make, model and year?
Placement InformationProvider Name Families that CareProvider Address 121 Main StreetCounty CountyDate of court order with CTW/BI and RE language?or date of VPA placing child 6/10/2000Placement type Foster family home(Non-relative)
Placing County County Children & Youth
All information recorded herein was reported to me and verified by the responsible parent/guardian
Signature of CYS worker Date
YES NO
YES NO
YES NO
YES NO

Kali’s CY-60
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 4 of 28
COUNTY CASE #
1234
1. CHILD'S NAME: 2. RACE 3. SOCIAL SECURITY NO: 4. DATE OF BIRTH: WH-WHITE
5. SEX: 6. DOES CCYA/JPO HAVE AN 7. ACCESS # 8. DOES THE CHILD HAVE ACCESS CARD FOR THE CHILD ANY PERSONAL INCOME
9. SPECIFY MONTHLY GROSS INCOME AND TYPE:
A. NOTICE OF CHILD'S INITIAL REMOVAL 1.Date of Initial Removal ( Constructive) 2 Date of Initial Placement 6/10/2000 3. Relative/Caretaker From Whom Child Was Removed: RELATIVE/CARETAKER'S NAME (LAST, FIRST, MI) SOCIAL SECURITY # RELATIONSHIP TO CHILD
B. CHILD IS IN SUBSTITUTE CARE PLACEMENT: 1. Substitute Care Provider: NAME OF SUBSTITUTE CARE PROVIDER ADDRESS
3. Effective Date of Placement 2. County Code Where Placed 4. Placement Facility Code 06/10/00 County
C. CHILD IS NO LONGER IN SUBSTITUTE CARE PLACEMENT 1. Name, Address and Relationship of the Caretaker to Whom Child was Returned RELATIVE/CARETAKER NAME AND ADDRESS SOCIAL SECURITY # RELATIONSHIIP TO CHILD
2. Effective Date 3. County Code Where Child Was Returned D. CCYA/JPO INFORMATION AND AUTHORIZATION
NAME: (PLEASE PRINT) SIGNATURE: DATE PHONE 06/07/2000
A. INITIAL ACTION 1. CHILD IS FROM A HOUSEHOLD THAT RECEIVES: 2. CHILD RECEIVING SSI? 3. AUTOMATIC MEDICAID ENROLLMENT AUTHORIZATION: RECIPIENT # (10 DIGITS) CARD ISSUE # (2 DIGITS) 4. Child is Currently Enrolled in HEALTHCHOICES And/Or has Private Insurance: Name of Insurance: Policy #:
B. MEDICAID REDETERMINATION NON-IVE CHILDREN Redeterm Date
Reason C. CONFIRM ADDITIONAL INFORMATION/UPDATES OR CHANGES ON CIS RECORD:
D. CAO INFORMATION/AUTHORIZATION DATE NAME(PLEASE PRINT): SIGNATURE DATE PHONE
CY-60 1/1/02
CCYA/JPO REQUEST FOR CAO ACTION County Children & Youth CCYA/JPO FILL OUT FORM WITH AS MUCH INFORMATION AS AVAILABLE AND FORWARD TO CAO WITHIN 5 DAYS
OF CHILD'S PLACEMENT, OR A CHANGE IN CHILD INFORMATION CCYA/JPO CY-60 MCI # 999999999 I. ACTION REQUESTED (COMPLETED BY CCYA/JPO - CHECK ALL THAT APPLY
II. IDENTIFYING INFORMATION (COMPLETED BY CCYA/JPO) Kali 333-33-3333 1/1/1993
Female
III. PLACEMENT INFORMATION (COMPLETED BY CCYA/JPO)
Martha 111-11-1111 Mother
(814) 432-9743 IV. CAO - COMPLETED BY CAO
Families that Care 121 Main Street
MONTHLY AMOUNT
CYS Worker
Notification of Change in Placement/Discharge Notification of "Age Out" Automatic Enrollment in Medicaid
YES NO
MCI # County Where Placed
NO
Child is Medicaid Eligible Child is Not Medicaid Eligible
Facility Placement Code
Medicaid Non-IVE Rederterm-TPL form attached Notification of Change or Additional Information Subsidized Permanent Legal Custodianship Release
UNKNOWN YES NO UNKNOWN
TANF Food Stamps Medicaid No Maintenance Income Benefits YES

Kali’s CY-61
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 5 of 28
1. Did the Child Have any Income/Resources in Eligibility Month or Month Child Lived with Relative?2. Specify the Type and Amount of Income/Resources Available to the Child:
CY 61
OTHER, SpecifyRSDI
OTHER, Specify
VI. INCOME AND RESOURCES OF ONLY THE CHILD
TYPE AMOUNT TYPE
BANK ACCOUNT
AMOUNT
CERTIF OF DEPOSIT
WAGESSSI
AUTOMOBILE
No Deprivation
Yes NoYes
COUNTY
CASE #1234
1. Child's Name 2. DOB 3. SS# 4. SexFemale
5. Father's Name and Address 6. DOB 7. SS#
8. Mother's Name and Address (If different from above) 9. DOB 10. SS#
11. Citizenship
1. Date of Initial Removal (Constructive Removal): 2. Date of Initial Placement
3. Date of Juvenile Court Petition or Voluntary Placement Agreement Signed by All Parties
4. Initial Custody/Removal Court Order That Contains the CTW/BI Language: 5. Effective Date of Order
6. Court Order That Contains the Reasonable Efforts to Prevent Removal 7. Effective Date of Order Language Within 60 Days of Child's Removal:8. JPO Court Order that Contains Shared Case Management Language: 9. Effective Date of Order
1. Child Removed From the Home of:Adoptive Parent than Parent) Runaway, etc.)
2. If C, Other (Above) is Checked, Then 6 mos Prior to Plcmt Did Child Live With: Adoptive Parent than Parent) Runaway, etc.)3. Person From Whom Child Was Removed:
RELATIVE/CARETAKER'S NAME (LAST, FIRST, MI) SOCIAL SECURITY # RELATIONSHIP TO CHILD
1. Was the Child Deprived of Care and Support of One or Both Parents?
1/1/1993
US Citizen
APPLICATION FOR INITIAL DETERMINATION FOR TITLE IV-E
MotherMartha
12. Age Requirement
1. Does Child Have Private Medical Insurance
I. IDENTIFYING INFORMATION
III. COURT ORDER OR VOLUNTARY PLACEMENT AGREEMENT (COMPLETED BY CCYA/JPO)
IV. REMOVAL HOME
V. DEPRIVATION FACTORS
Kali
unknown
123 State Street, PA
unknown
333-33-3333
expected to Graduate By Age 19
unknown
Martha
II. MEDICAL INSURANCE INFORMATION
12/12/69 111-11-1111
unknown
6/10/2000
County Children & Youth
CCYA/JPOCAO
PLACEMENT MAINTENANCE AND MEDICAID DETERMINATION
CCYA/JPO COMPLETES FORM AND FORWARDS TO CAOCY-61
WITHIN 60 WORKING DAYS OF CHILD'S INITIAL PLACEMENT
6/10/2000
6/10/2000
111-11-1111
A. Parent Or B. Relative (Other C. Other (Unrelated Person,
Deprivation - Check The Deprivation Factor(s) Below Death
Absence (Separation, Divorce)
Unemployment of Primary Wage Earner
Incapacity/Disablity, Explain
Child is Under Age 18
Child is Under Age 19, Enrolled in a Secondary School And
NoYes, Attach Third Party Liability (TPL) Data Entry Worksheet
VPA, Continue to Section IVPetition, Complete Section III
A. Parent Or B. Relative (Other C. Other (Unrelated Person,
Underemployment of Primary Wage Earner
YesNo
YesNo
YesNo

Kali’s CY-61, Cont’d
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 6 of 28

Steven’s Initial Information Worksheet
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 7 of 28
Your Name JPO Worker
Child's Information Case Number 1234 Full Name Steven Sex Male SSN 666-66-6666 DOB 6/6/1988 Date of Removal 6/10/2000 Date of Return Home Citizenship US Citizen Race WH-WHITE Type of Placement Substitute Care Removed from home of: Doug Address: full 123 State Street, PA Relationship to Child: Father SSN 222-22-2222 Is child of Hispanic Origin? No Telephone # (888) 888-8888 School District? Grade Has child ever been diagnosed with a disability If yes, what disability? Has child ever been adopted? If yes, at what age? Was child's mother married at time of child's birth? County and hospital where birth occurred Family structure removed from Does child have an ACCESS card? If yes, ACCESS # Does child have private insurance? If yes, Company name, address, policy # Does child have available income/resources? If yes, specify cash, child support, SS, SSI, Auto , savings, VA benfits, unemploym, and $$
Parent Information: Father's Name Doug Father's Address 123 State Street, PA Father's DOB 3/3/1966 Father's SS# 222-22-2222 Father's phone # (888) 888-8888 Is father employed? If yes, where?
Initial Information Worksheet
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO

Steven’s Initial Information Worksheet, Cont’d
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 8 of 28
Full -time or part-time?Father's gross monthly income
Mother's Name unknownMother's Address unknownMother's DOB unknownMother's SS# unknownMother's phone #Is mother employed?If yes, where?Full -time or part-time?Mother's gross monthly incomeMother's maiden name
YES NO
Steven’s Initial Information Worksheet, Cont’d
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 9 of 28
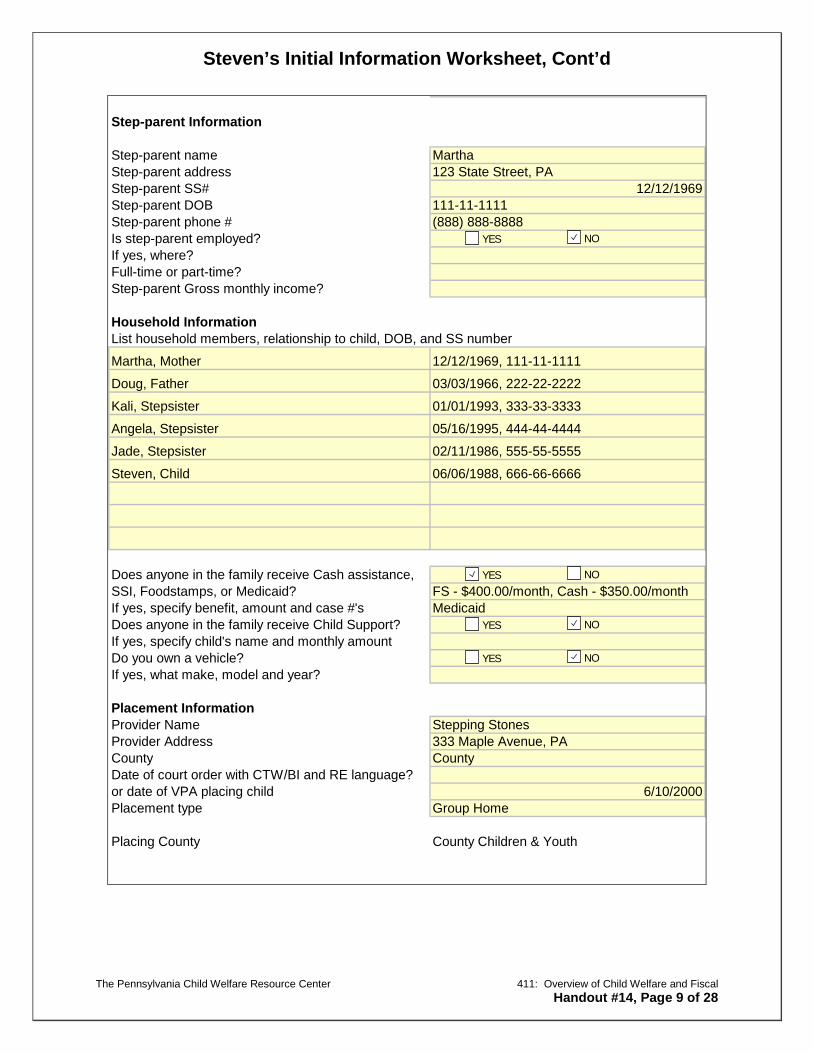
Step-parent Information
Step-parent name MarthaStep-parent address 123 State Street, PA Step-parent SS# 12/12/1969Step-parent DOB 111-11-1111Step-parent phone # (888) 888-8888Is step-parent employed?If yes, where?Full-time or part-time?Step-parent Gross monthly income?
Household InformationList household members, relationship to child, DOB, and SS number
Martha, Mother 12/12/1969, 111-11-1111
Doug, Father 03/03/1966, 222-22-2222
Kali, Stepsister 01/01/1993, 333-33-3333
Angela, Stepsister 05/16/1995, 444-44-4444
Jade, Stepsister 02/11/1986, 555-55-5555
Steven, Child 06/06/1988, 666-66-6666
Does anyone in the family receive Cash assistance,SSI, Foodstamps, or Medicaid? FS - $400.00/month, Cash - $350.00/monthIf yes, specify benefit, amount and case #'s MedicaidDoes anyone in the family receive Child Support?If yes, specify child's name and monthly amountDo you own a vehicle?If yes, what make, model and year?
Placement InformationProvider Name Stepping StonesProvider Address 333 Maple Avenue, PACounty CountyDate of court order with CTW/BI and RE language?or date of VPA placing child 6/10/2000Placement type Group Home
Placing County County Children & Youth
YES NO
YES NO
YES NO
YES NO

Steven’s Initial Information Worksheet, Cont’d
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 10 of 28
All information recorded herein was reported to me and verified by the responsible parent/guardian
Signature of CYS worker Date

Steven’s CY-60
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 11 of 28
COUNTY
CASE # 1234
1. CHILD'S NAME: 2. RACE 3. SOCIAL SECURITY NO: 4. DATE OF BIRTH: WH-WHITE
5. SEX: 6. DOES CCYA/JPO HAVE AN 7. ACCESS # 8. DOES THE CHILD HAVE ACCESS CARD FOR THE CHILD ANY PERSONAL INCOME
9. SPECIFY MONTHLY GROSS INCOME AND TYPE:
A. NOTICE OF CHILD'S INITIAL REMOVAL 1.Date of Initial Removal ( Constructive) 2 Date of Initial Placement 6/10/2000 3. Relative/Caretaker From Whom Child Was Removed: RELATIVE/CARETAKER'S NAME (LAST, FIRST, MI) SOCIAL SECURITY # RELATIONSHIP TO CHILD
B. CHILD IS IN SUBSTITUTE CARE PLACEMENT: 1. Substitute Care Provider: NAME OF SUBSTITUTE CARE PROVIDER ADDRESS
3. Effective Date of Placement 2. County Code Where Placed 4. Placement Facility Code 06/10/00 County
C. CHILD IS NO LONGER IN SUBSTITUTE CARE PLACEMENT 1. Name, Address and Relationship of the Caretaker to Whom Child was Returned RELATIVE/CARETAKER NAME AND ADDRESS SOCIAL SECURITY # RELATIONSHIIP TO CHILD
2. Effective Date 3. County Code Where Child Was Returned D. CCYA/JPO INFORMATION AND AUTHORIZATION
NAME: (PLEASE PRINT) SIGNATURE: DATE PHONE
A. INITIAL ACTION
CCYA/JPO REQUEST FOR CAO ACTION County Children & Youth CCYA/JPO FILL OUT FORM WITH AS MUCH INFORMATION AS AVAILABLE AND FORWARD TO CAO WITHIN 5 DAYS
OF CHILD'S PLACEMENT, OR A CHANGE IN CHILD INFORMATION CCYA/JPO CY-60 MCI# 999999999 I. ACTION REQUESTED (COMPLETED BY CCYA/JPO - CHECK ALL THAT APPLY
II. IDENTIFYING INFORMATION (COMPLETED BY CCYA/JPO) Steven 666-66-6666 6/6/1988
Male 1234567890
III. PLACEMENT INFORMATION (COMPLETED BY CCYA/JPO)
Doug 222-22-2222 Father
IV. CAO - COMPLETED BY CAO
Stepping Stones 03- Substitute Care Plcmt to a county
333 Maple Avenue, PA
CYS Worker
Notification of Change in Placement/Discharge Notification of "Age Out" Automatic Enrollment in Medicaid
YES NO
Medicaid Non-IVE Rederterm-TPL form attached Notification of Change or Additional Information Subsidized Permanent Legal Custodianship Release
UNKNOWN YES NO UNKNOWN
TANF Food Stamps Medicaid No Maintenance Income Benefits

Steven’s CY-60, Cont’d
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 12 of 28
1. CHILD IS FROM A HOUSEHOLD THAT RECEIVES:
2. CHILD RECEIVING SSI?
3. AUTOMATIC MEDICAID ENROLLMENT AUTHORIZATION: RECIPIENT # (10 DIGITS) CARD ISSUE # (2 DIGITS)
4. Child is Currently Enrolled in HEALTHCHOICES And/Or has Private Insurance: Name of Insurance: Policy #:
B. MEDICAID REDETERMINATION NON-IVE CHILDRENRedeterm Date
Reason
C. CONFIRM ADDITIONAL INFORMATION/UPDATES OR CHANGES ON CIS RECORD:
D. CAO INFORMATION/AUTHORIZATION DATENAME(PLEASE PRINT): SIGNATURE DATE PHONE
CY-60 1/1/02
MONTHLY AMOUNT
Other
County Where Placed
NO
Child is Medicaid Eligible
Child is Not Medicaid Eligible
Facility Placement Code
TANF Food Stamps Medicaid No Maintenance Income Benefits
YES
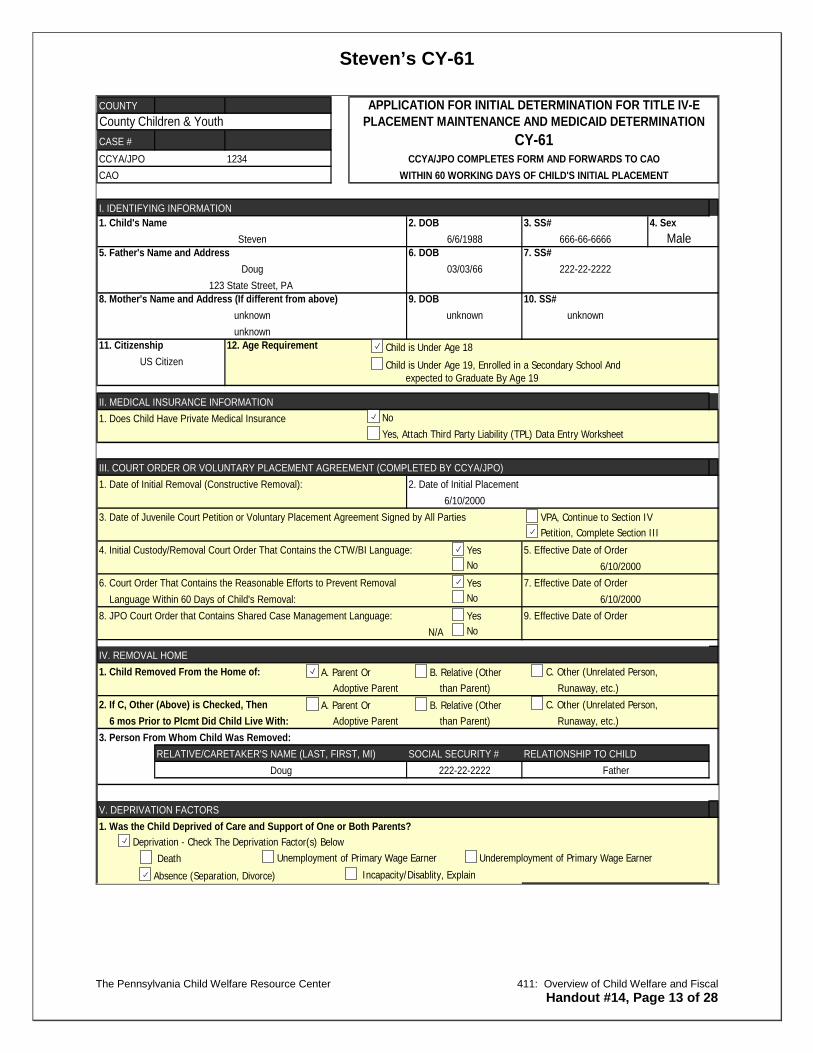
Steven’s CY-61
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 13 of 28
COUNTY
CASE #1234
1. Child's Name 2. DOB 3. SS# 4. SexMale
5. Father's Name and Address 6. DOB 7. SS#
8. Mother's Name and Address (If different from above) 9. DOB 10. SS#
11. Citizenship
1. Date of Initial Removal (Constructive Removal): 2. Date of Initial Placement
3. Date of Juvenile Court Petition or Voluntary Placement Agreement Signed by All Parties
4. Initial Custody/Removal Court Order That Contains the CTW/BI Language: 5. Effective Date of Order
6. Court Order That Contains the Reasonable Efforts to Prevent Removal 7. Effective Date of Order Language Within 60 Days of Child's Removal:8. JPO Court Order that Contains Shared Case Management Language: 9. Effective Date of Order
N/A
1. Child Removed From the Home of:Adoptive Parent than Parent) Runaway, etc.)
2. If C, Other (Above) is Checked, Then 6 mos Prior to Plcmt Did Child Live With: Adoptive Parent than Parent) Runaway, etc.)3. Person From Whom Child Was Removed:
RELATIVE/CARETAKER'S NAME (LAST, FIRST, MI) SOCIAL SECURITY # RELATIONSHIP TO CHILD
1. Was the Child Deprived of Care and Support of One or Both Parents?
6/6/1988
US Citizen
APPLICATION FOR INITIAL DETERMINATION FOR TITLE IV-E
FatherDoug
12. Age Requirement
1. Does Child Have Private Medical Insurance
I. IDENTIFYING INFORMATION
III. COURT ORDER OR VOLUNTARY PLACEMENT AGREEMENT (COMPLETED BY CCYA/JPO)
IV. REMOVAL HOME
V. DEPRIVATION FACTORS
Steven
Doug
unknown
222-22-2222
666-66-6666
expected to Graduate By Age 19
123 State Street, PA
unknown
II. MEDICAL INSURANCE INFORMATION
unknown unknown
03/03/66
6/10/2000
County Children & Youth
CCYA/JPOCAO
PLACEMENT MAINTENANCE AND MEDICAID DETERMINATION
CCYA/JPO COMPLETES FORM AND FORWARDS TO CAOCY-61
WITHIN 60 WORKING DAYS OF CHILD'S INITIAL PLACEMENT
6/10/2000
6/10/2000
222-22-2222
A. Parent Or B. Relative (Other C. Other (Unrelated Person,
Deprivation - Check The Deprivation Factor(s) Below Death
Absence (Separation, Divorce)
Unemployment of Primary Wage Earner
Incapacity/Disablity, Explain
Child is Under Age 18
Child is Under Age 19, Enrolled in a Secondary School And
NoYes, Attach Third Party Liability (TPL) Data Entry Worksheet
VPA, Continue to Section IVPetition, Complete Section III
A. Parent Or B. Relative (Other C. Other (Unrelated Person,
Underemployment of Primary Wage Earner
YesNo
YesNo
YesNo

Steven’s CY-61, Cont’d
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 14 of 28
1. Did the Child Have any Income/Resources in Eligibility Month or Month Child Lived with Relative?2. Specify the Type and Amount of Income/Resources Available to the Child:
CY 61
1. Please list All Members of the Household Living with the Child in the Removal Home(Attach Additional Sheet if Needed)
GROSS INCOME AND FREQUENCY
$400.00/month$350.00/month
None
None
None
None
None2. Parent is Paying Child Support For 3. Name of Child(ren) 4. Total Amount Child(ren) Out of the Home5. Parent is Receiving Child Support For 6. Name of Child(ren) 7. Total Amount Child(ren) In the Home8. CCYA Information and Authorization:
NAME: (PLEASE PRINT) SIGNATURE: DATE PHONE
1. INSUFFICIENT INFORMATION, SPECIFY:2 This Child (Check One)
MEETS AFDC CRITERIA AND IS CATEGORICALLY MEDICAID ELIGIBLE
DOES NOT MEET AFDC CRITERIA, REASON:
ELIGIBLE FOR MEDICAID BENEFITS ONLYNOT ELIGIBLE FOR MEDICAID BENEFITS
3. CAO Information and AuthorizationNAME: (PLEASE PRINT) SIGNATURE: DATE PHONE
1. Pending, IV-E Eligibility Cannot be Determined ReasonDate Placed in Pending File Date of Resolution
Steven, Child
Angela, Stepsister01/01/1993, 333-33-3333 None None None
Kali, Stepsister03/03/1966, 222-22-2222 None None None
Doug, Father
IX. CCYA IV-E DETERMINATION
OTHER, SpecifyRSDI
CAO Returns Completed Form to CCYA
OTHER, Specify
VI. INCOME AND RESOURCES OF ONLY THE CHILD
TYPE AMOUNT TYPE
BANK ACCOUNT
CCYA/JPO Forward Completed Form to CAOVIII. COUNTY ASSISTANCE OFFICE CERTIFICATION
CYS Worker
Martha, Step-Mother12/12/1969, 111-11-1111
05/16/1995, 444-44-4444
VII. INCOME AND RESOURCES OF THE HOUSEHOLD
HOUSEHOLD MEMBER NAME(INCLUDE NAME,
RELATION TO CHILD: SS#, DOB)
DEPENDENT CARE EXPENSES TYPE,
AMOUNT
INCOME SOURCE
Foodstamps
RESOURCES AND AMOUNT (FOR VEHICLES, INCLUDE MAKE, MODEL
AND YEAR)
None
None
Jade, Stepsister02/11/1986, 555-55-5555 None
06/06/1988, 666-66-6666 None None
Cash
None
AMOUNT
CERTIF OF DEPOSIT
WAGESSSI
AUTOMOBILE
None
None
None
None
None
No Deprivation
Excess IncomeExcess ResourcesLack of DeprivationAgeCitizenship
Yes No
Child Did Not Live With Specified Relative Within 6 Months
YesNoYes
No
Yes
Steven’s CY-61, Cont’d
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 15 of 28
2. IV-E Eligibility (Check One)
3. CCYA Information and Authorization
NAME: (PLEASE PRINT) SIGNATURE: DATE PHONE
1. CAO/JPO Notified of Child's Eligibility By: Code:
2. CCYA Authorization: 3. Date:
CY61 1/1/02
X. CCYA NOTIFICATION OF IV-E ELIGIBILITY TO CAO/JPO
Child is IV-E Eligible
Child is Not IV-E Eligible, Reason:
Mail E-mail Fax

Kali’s
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 16 of 28
APPLICATION FOR CHILD SUPPORT SERVICES
I, Child Welfare Services Agency request the Domestic Relations Section to
provide CHILD/SPOUSAL SUPPORT services to which I am entitled to upon application
under Federal Law and the Child Support Enforcement Program of Pennsylvania.
If necessary, I request use of the Parent Locator Services, and help if necessary
in establishing paternity.
My case began 6/10/2000. This confirms that any child support services I
requested before this form was available, were sought and applied for under the Child
Support Enforcement Program, described in Public Law 93-647.
Date: 6/12/2000
Signature
Printed Name: Child Welfare Representative
Plaintiff’s Attorney Defendant’s Attorney

The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 17 of 28
: IN THE COURT OF COMMON PLEAS OF PLAINTIFF : COUNTY ________________________ VS Martha DEFENDANT : DR# ____________________________
COMPLAINT FOR SUPPORT
1. Plaintiff resides at 123 State Street, , Pennsylvania, County ________________________ Phone _______________________ Date of Birth: 12/12/69 Social Security #: 111-11-1111 . 2. Defendant resides at 123 State Street, , Pennsylvania, County ________________________ Phone (888) 888-888 Date of Birth 12/12/69 Social Security# 111-11-1111 3. (a) Plaintiff and Defendant were married on (Date), at . (City &State) (b) Plaintiff and Defendant were separated on (Date) (c) Plaintiff and Defendant were divorced on (Date) at . (City & State) 4. Plaintiff and Defendant are the parents of the following children:
(a) Born of Marriage: NAME SS# DOB AGE RESIDENCE Kali 333-33-3333 1/1/93 7 123 State Street, PA

The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 18 of 28
Born out of Wedlock: NAME SS# DOB AGE RESIDENCE Plaintiff seeks support for the following persons: 6. (a) Plaintiff is (not) receiving public assistance in the amount of $ 65.00 per
day for the support of (Names): Kali .
(b) Plaintiff is receiving additional income of $ per month from
employment.

Steven’s
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 19 of 28
APPLICATION FOR CHILD SUPPORT SERVICES
I, Child Welfare Service Agency request the Domestic Relations Section to
provide CHILD/SPOUSAL SUPPORT services to which I am entitled to upon application
under Federal Law and the Child Support Enforcement Program of Pennsylvania.
If necessary, I request use of the Parent Locator Services, and help if necessary
in establishing paternity.
My case began 6/10/2000. This confirms that any child support services I
requested before this form was available, were sought and applied for under the Child
Support Enforcement Program, described in Public Law 93-647.
Date: 6/12/2000
Signature
Printed Name: Child Welfare Representative
Plaintiff’s Attorney Defendant’s Attorney

The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 20 of 28
: IN THE COURT OF COMMON PLEAS OF PLAINTIFF : COUNTY ________________________ VS Doug DEFENDANT : DR# ____________________________
COMPLAINT FOR SUPPORT
1. Plaintiff resides at 123 State Street, , Pennsylvania, County ________________________ Phone (888) 888-888 . Date of Birth 3/3/66 Social Security # 222-22-2222 2. Defendant resides at 123 State Street, , Pennsylvania, County ________________________ Phone (888) 888-888 . Date of Birth 3/3/66 Social Security# 222-22-2222 3. (a) Plaintiff and Defendant were married on (Date), at . (City &State) (b) Plaintiff and Defendant were separated on .(Date) (c) Plaintiff and Defendant were divorced on .(Date) at . (City & State) 4. Plaintiff and Defendant are the parents of the following children:
(b) Born of Marriage: NAME SS# DOB AGE RESIDENCE Steven 666-66-6666 6/6/88 12 123 State Street, PA

The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 21 of 28
Born out of Wedlock: NAME SS# DOB AGE RESIDENCE Plaintiff seeks support for the following persons: Steven 6. (a) Plaintiff is (not) receiving public assistance in the amount of $140.00 per
day for the support of (Names): Steven .
(b) Plaintiff is receiving additional income of $ 0 per month from
employment.

Kali’s
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 22 of 28
Social Security Administration Inquiry June 12, 2000 Social Security Administration Inquiry Pennsylvania Child’s Name: Kali Social Security Number: 333-33-3333 Please verify if the above named child is in receipt of Social Security benefits. Your cooperation in this matter is greatly appreciated.
Thank you, Employee Signature: Date: 6/12/00 _______________________________

Kali’s
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 23 of 28
Social Security Denial Letter June 2000 Attention: Fiscal Officer County Children & Youth Services PA
Kali 333-33-3333 Child’s Name Social Security Number
SS benefit received: _____________________ Signature of SS employee verifying suspension: ____________________________________ Title of SS Employee: ________________________ Date: ____________________________
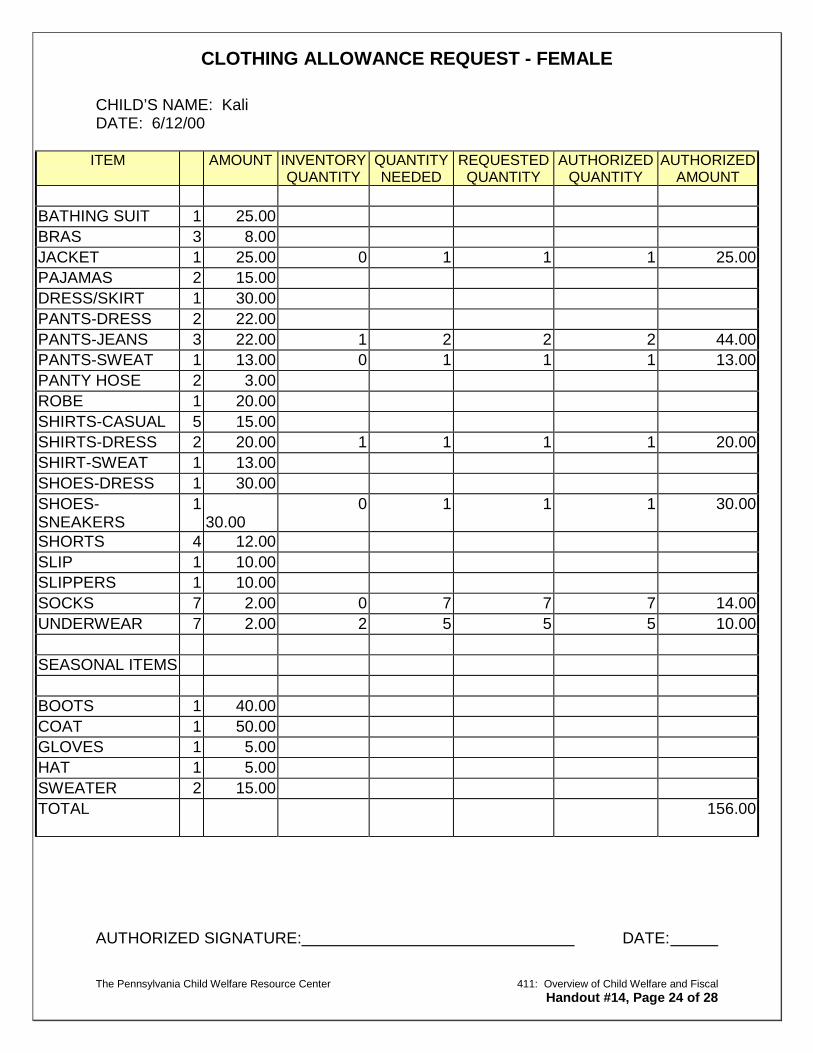
CLOTHING ALLOWANCE REQUEST - FEMALE
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 24 of 28
CHILD’S NAME: Kali DATE: 6/12/00
ITEM AMOUNT INVENTORY QUANTITY
QUANTITY NEEDED
REQUESTED QUANTITY
AUTHORIZED QUANTITY
AUTHORIZED AMOUNT
BATHING SUIT 1 25.00 BRAS 3 8.00 JACKET 1 25.00 0 1 1 1 25.00 PAJAMAS 2 15.00 DRESS/SKIRT 1 30.00 PANTS-DRESS 2 22.00 PANTS-JEANS 3 22.00 1 2 2 2 44.00 PANTS-SWEAT 1 13.00 0 1 1 1 13.00 PANTY HOSE 2 3.00 ROBE 1 20.00 SHIRTS-CASUAL 5 15.00 SHIRTS-DRESS 2 20.00 1 1 1 1 20.00 SHIRT-SWEAT 1 13.00 SHOES-DRESS 1 30.00 SHOES-SNEAKERS
1 30.00
0 1 1 1 30.00
SHORTS 4 12.00 SLIP 1 10.00 SLIPPERS 1 10.00 SOCKS 7 2.00 0 7 7 7 14.00 UNDERWEAR 7 2.00 2 5 5 5 10.00
SEASONAL ITEMS
BOOTS 1 40.00 COAT 1 50.00 GLOVES 1 5.00 HAT 1 5.00 SWEATER 2 15.00 TOTAL 156.00
AUTHORIZED SIGNATURE: DATE:
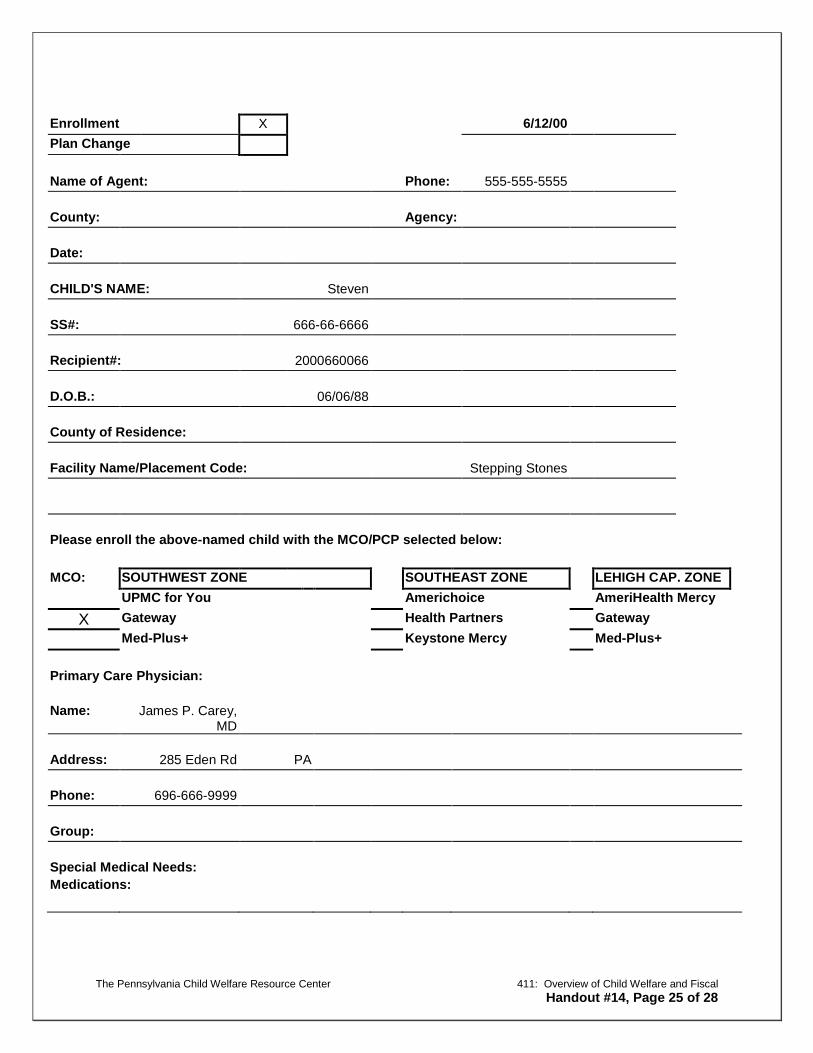
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 25 of 28
Enrollment X 6/12/00 Plan Change
Name of Agent: Phone: 555-555-5555
County: Agency:
Date:
CHILD'S NAME: Steven
SS#: 666-66-6666
Recipient#: 2000660066
D.O.B.: 06/06/88
County of Residence:
Facility Name/Placement Code: Stepping Stones
Please enroll the above-named child with the MCO/PCP selected below:
MCO: SOUTHWEST ZONE SOUTHEAST ZONE LEHIGH CAP. ZONE UPMC for You Americhoice AmeriHealth Mercy
X Gateway Health Partners Gateway Med-Plus+ Keystone Mercy Med-Plus+
Primary Care Physician:
Name: James P. Carey, MD
Address: 285 Eden Rd PA
Phone: 696-666-9999
Group:
Special Medical Needs: Medications:

Steven’s Primary Care Physician (PCP) Information
The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 26 of 28
James P. Carey, MD
285 Eden Rd PA
696-666-9999

The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 27 of 28

The Pennsylvania Child Welfare Resource Center 411: Overview of Child Welfare and Fiscal Handout #14, Page 28 of 28




![Display Advertising Windows Live Presentation to [Client Name] [Month Date, Year]](https://static.documents.pub/doc/80x56/56649ef35503460f94c050d3/display-advertising-windows-live-presentation-to-client-name-month-date.jpg)












![ONLINE BUSINESS PROPOSAL [CLIENT NAME] [MONTH] [DAY ... · ONLINE BUSINESS PROPOSAL [CLIENT NAME] [MONTH] [DAY], [YEAR] ... 2 Custom moodboard concepts ... galleries, PDF/PPT/DOC](https://static.documents.pub/doc/80x56/5e7fbf9bb930cf489b037185/online-business-proposal-client-name-month-day-online-business-proposal.jpg)