Clinical application of the RONNA G4 system - preliminary validation of 23 robotic frameless brain biopsies Dlaka, Domagoj; Švaco, Marko; Chudy, Darko; Jerbić, Bojan; Šekoranja, Bojan; Šuligoj, Filip; Vidaković, Josip; Almahariq, Fadi; Romić, Dominik; Raguž, Marina Source / Izvornik: Croatian Medical Journal, 2021, 62, 318 - 327 Journal article, Published version Rad u časopisu, Objavljena verzija rada (izdavačev PDF) https://doi.org/10.3325/cmj.2021.62.318 Permanent link / Trajna poveznica: https://urn.nsk.hr/urn:nbn:hr:105:648475 Rights / Prava: Attribution-NonCommercial-NoDerivatives 4.0 International Download date / Datum preuzimanja: 2022-01-13 Repository / Repozitorij: Dr Med - University of Zagreb School of Medicine Digital Repository
Transcript
Clinical application of the RONNA G4 system -preliminary validation of 23 robotic frameless brainbiopsies
Aims To report the outcomes of robot-assisted brain biop-sies performed using a novel RONNA G4 system. The sys-tem was developed by a research group from the Faculty of Mechanical Engineering and Naval Architecture and a team of neurosurgeons from Dubrava University Hospital, University of Zagreb School of Medicine.
Methods This prospective study included 49 biopsies analyzed during one year: 23 robotic frameless and 26 frame-based Leksell stereotactic biopsies. We analyzed the presenting symptoms, tumor range and location, postop-erative complications, pathohistological diagnosis, diag-nostic yield, as well as operation and hospitalization du-ration. The target point error was calculated to assess the accuracy of the RONNA system.
Results No postoperative mortality, morbidity, or in-fections were observed. In the frameless robotic biopsy group, only one pathohistological diagnosis was incon-clusive. Therefore, the diagnostic yield was 95.6% (22/23), similar to that of the framebased Leksell stereotactic biop-sy group (95.1% or 25/26). The average target point error in the frameless robotic biopsy group was 2.15 ± 1.22 mm (range 0.39-5.85).
Conclusion The RONNA G4 robotic system is a safe and accurate tool for brain biopsy, although further research warrants a larger patient sample, comparison with other robotic systems, and a systematic analysis of the entry and target point errors.
Received: April 3, 2020
Accepted: January 14, 2021
Correspondence to: Marina Raguž Department of Neurosurgery Dubrava University Hospital Avenija Gojka Šuška 6 10 000 Zagreb, Croatia [email protected]
Domagoj Dlaka1, Marko Švaco2, Darko Chudy1,3, Bojan Jerbić2, Bojan Šekoranja2, Filip Šuligoj2, Josip Vidaković2, Fadi Almahariq1, Dominik Romić1, Marina Raguž1
1Department of Neurosurgery, Dubrava University Hospital, Zagreb, Croatia
2Faculty of Mechanical Engineering and Naval Architecture, University of Zagreb, Zagreb, Croatia
3University of Zagreb School of Medicine, Zagreb, Croatia
Clinical application of the RONNA G4 system – preliminary validation of 23 robotic frameless brain biopsies
319Dlaka et al: Clinical application of the RONNA G4 system
www.cmj.hr
Neurosurgery is one of the most demanding branches of medicine given the need for precision and limitations re-lated to the anatomical area of interest and activity. Since the brain is a specific symmetrical organ enclosed in bone armor, precise localization of a target point within the skull is often challenging. Sophisticated technological innova-tions in neurosurgery, such as automated robot-assisted systems, offer a unique combination of precision, spatial accuracy, and dexterity. Several decades ago, the introduc-tion of stereotactic frame into neurosurgery (1) established new standards in targeting and localization accuracy. The stereotactic frame is still widely used for brain biopsy pro-cedures (2). The first robotic system used in neurosurgery was industrial robot PUMA 200 (3), after which a number of robotic systems have been developed (4-9). In compar-ison with humans, robotic systems have increased surgi-cal accuracy, stability, non-fatigue, steadiness and endur-ance, accurate spatial positioning, quantitative analysis, extension of the visual and manual dexterity of neurosur-geons etc. Possible disadvantages include an inability to handle unexpected situations and required manual labor (10-12). Robotic systems are used in several neurosurgical
procedures requiring exceptional spatial accuracy such as stereotactic biopsy, deep brain stimulation (DBS), stereo-encephalography, external ventricular drainage, and en-doscopy (6-8,13,14). Here, we present a new robotic neu-ronavigation system RONNA G4 developed by a research group from the Faculty of Mechanical Engineering and Naval Architecture, University of Zagreb, and a team of neurosurgeons from Dubrava University Hospital and the University of Zagreb School of Medicine (15-18). Active re-search and development within the RONNA project start-ed in 2010 (Figure 1) with an aim to create more precise and intuitive stereotactic neuronavigation procedures. The RONNA system has four generations. In the first genera-tion, we developed a prototype localization device with a precisely calibrated camera and a laser triangulation sen-sor for the localization of a polymer reference localization marker (18). In 2012, the first-generation system was used in preclinical trials on phantoms. The second-generation system was a refined version of the first generation. As the master (navigation) robot we used KUKA Agilus KR6R900 sixx (16), which is still used in the fourth generation of the RONNA system. The mechanical pose repeatability of the
FiguRe 1. RONNA historical development.
RESEARCH ARTICLE320 Croat Med J. 2021;62:318-27
www.cmj.hr
Kuka Agilus KR6 R900 sixx robot arm with respect to the ISO 9283 is ±0.03 mm. In comparison, the mechanical ac-curacy of the ROSA system is ±0.1 mm (19).
On the second-generation localization marker, we devel-oped a novel stereovision system for a precise localization of the spherical fiducials (20). The third-generation system,
FiguRe 2. RONNA g4 surgical workflow. Before operation, the bone-attached screws are fixed to the patient’s head under local anesthesia (A). The patient undergoes a contrast-enhanced preoperative computed tomography and magnetic resonance imaging according to a standard head protocol (B,C). in the preparation phase, the robot is positioned in an optimal position near the patient. An optical tracking system is used to coarsely position the robot with respect to the patient (D). The trajectory is visualized using a non-sterile probe (E). in the operation phase, after anesthesia induction, the operating field is prepared, and a sterile cover is put on the patient and the robot (F). using the RONNAplan, the neurosurgeon selects the preoperatively planned trajectory following the tool guide positioning by the robot. Skin incision and burr hole drilling are performed manually by the neurosurgeon (G). A biopsy needle is advanced manually by the neurosurgeon to the target point in order to obtain the tissue for pathohistological analysis (H, I).
321Dlaka et al: Clinical application of the RONNA G4 system
www.cmj.hr
the RONNA G3, had a mobile platform with dedicated mechanical and electrical components (17,18). The RON-NA G4 system includes multiple novel hardware and soft-ware improvements, which are described in detail by Jer-bic et al (18). Currently, the RONNA G4 is clinically used as an important neurosurgical tool for preoperative planning and precise frameless neuronavigation (Figure 1). The first brain biopsy on an actual patient using the RONNA was performed at Dubrava University Hospital, Department for Neurosurgery in Zagreb, in May 2016 (17). Since then, the RONNA has been regularly used for stereotactic brain bi-opsies.
The RONNA G4, is currently in the clinical trial phase, and numerous laboratory tests and extensive preclinical trials were performed before clinical application (15,16,21).
The clinical procedure, ie RONNA G4 workflow is performed in three stages (Figure 2). The procedure starts with the pre-operative phase. Specially developed self-drilling and self-tapping screws are attached to the cranial bone under lo-cal anesthesia to allow precise localization and navigation. For frameless robotic system biopsies, screws are inserted percutaneously while the patient lies comfortably in his or her bed. In contrast, frame mounting requires a forced sit-ting position and patient’s collaboration to keep his or her head still. Feeling the frame tightening around the head may cause considerable discomfort to the patient. In addi-tion, the frame is carried until the end of biopsy, while the percutaneous screws mostly cannot be seen or felt. Several articles (22,23) report on better tolerance of percutaneous screw placement in patients undergoing frameless robotic system biopsies, supporting our protocol (22,23).
After screw placement, the patient undergoes contrast-enhanced preoperative computed tomography (CT) imag-ing (Somatom Emotion®, Siemens, Erlangen, Germany) ac-cording to our standard head protocol with the following parameters: gantry rotation time 0.6 s, helical scanning, de-tector collimation 16 mm ×0.6 mm, slice-width 0.75 mm, reconstruction increment 0.7 mm, image matrix 512 × 512 with a voxel size of 0.5 mm ×0.5 mm ×0.7 mm, no gan-try. After scanning, the images are imported into the op-eration planning software (RONNAplan) integrated as a pl-ugin for the Osirix MD medical certified software (Pixmeo, Sa’rl, Switzerland). The RONNAplan allows the automatic localization of spherical fiducial markers using our nov-el algorithm, as previously described (24). The software is non-hardware dependent and can be used as a plugin on any computer running Osirix MD. This allows the neurosur-
geon to plan the operative trajectories in a decentralized fashion even a day before the surgical procedure, without the need for a special planning station, making the plan-ning system scalable (Figure 2A-C). The final operative plan is transferred to the RONNA G4 control computer, where it is used for navigation in the operating theater.
The first phase is followed by a preparation phase. After positioning the patient in the operating theater, our nov-el robot positioning algorithm (25) calculates the opti-mal position of the robot with respect to the patient. The medical staff manually positions the robot base given the feedback from the global optical tracking system and vi-sual instructions from the RONNAplan software module (Figure 2 D,E).
In the operation phase, after anesthesia induction, the op-erating field is prepared, and the patient and the robot are covered with a sterile draping. Using the RONNAplan, the neurosurgeon selects the preoperatively planned trajec-tory following the tool guide positioning by the robot. We developed an intuitive human-robot software interface for controlling intraoperative robot actions. The robot can be easily navigated and positioned in multiple positions, such as the main biopsy position, multiple staged-biopsy po-sitions, drilling position, etc, and be adjusted to different depths of the same trajectory. In the current phase of the clinical trials, the system is used for brain-tissue biopsies. The robot uses a sterile tool holder for a twist drill and a bi-opsy needle (diameters: 3.2 mm and 2.5 mm, respectively). Skin incision and burr hole drilling are performed manually by the neurosurgeon. After the opening and electrocoagu-lation of the dura, a biopsy needle (diameter 2.5 mm) is ad-vanced manually by the neurosurgeon to the target point. If needed, the neurosurgeon commands the robot a few millimeters deeper and/or superficial with respect to the target point to perform a staged biopsy. When the biopsy is completed at the target point, the robot retracts to its home position or repositions the tool guide at another tar-get if multiple biopsy sites are planned (Figure 2 F-I).
The aim of our study was to assess efficacy and safety of ro-botic frameless and stereotactic framebased biopsies.
PATieNTS AND MeThODS
This prospective study involved two patient groups. In the first group, the brain biopsies were performed with the RONNA G4 robotic system, and in second group with a framebased stereotactic approach with a
RESEARCH ARTICLE322 Croat Med J. 2021;62:318-27
www.cmj.hr
Leksell frame (Elekta AB, Stockholm, Sweden). No clinical or other criteria make a patient more eligible for robotic or stereotactic brain biopsy. Both procedures have the same indications; stereotactic biopsy should be performed whenever open surgery with at least bulk resection is not feasible or when the lesion requires only oncological treat-ment (26,27). Since our research group is actively develop-ing the RONNA system for robotic frameless brain biopsies, we performed robotic biopsies whenever possible. Frame-based Leksell stereotactic biopsies were performed on all occasions when any part of the robotic system underwent regular maintenance and upgrade, or when an engineer was not available (the engineer presence was preferred in the first stages of development and clinical usage until the system reliability was shown and a learning curve was es-tablished). For example, when the robotic system was un-available due to a software upgrade during a three-month period, we performed only framebased Leksell stereotactic biopsies. From February 2019 till February 2020, we per-formed 49 biopsies: 23 robotic and 26 framebased Leksell stereotactic biopsies. Every patient was informed about the biopsy type and the procedure details. Only one pa-tient refused to participate; the patient was psychoorgan-ically changed due to the tumor extent and localization. The included patients underwent full both preoperative and postoperative neuroradiological examinations (MSCT and MRI) used for additional analysis. All patients or their family members signed informed consent. The ethical ap-proval was obtained from the Institutional Review Boards
of Dubrava University Hospital and the University of Za-greb School of Medicine.
ReSulTS
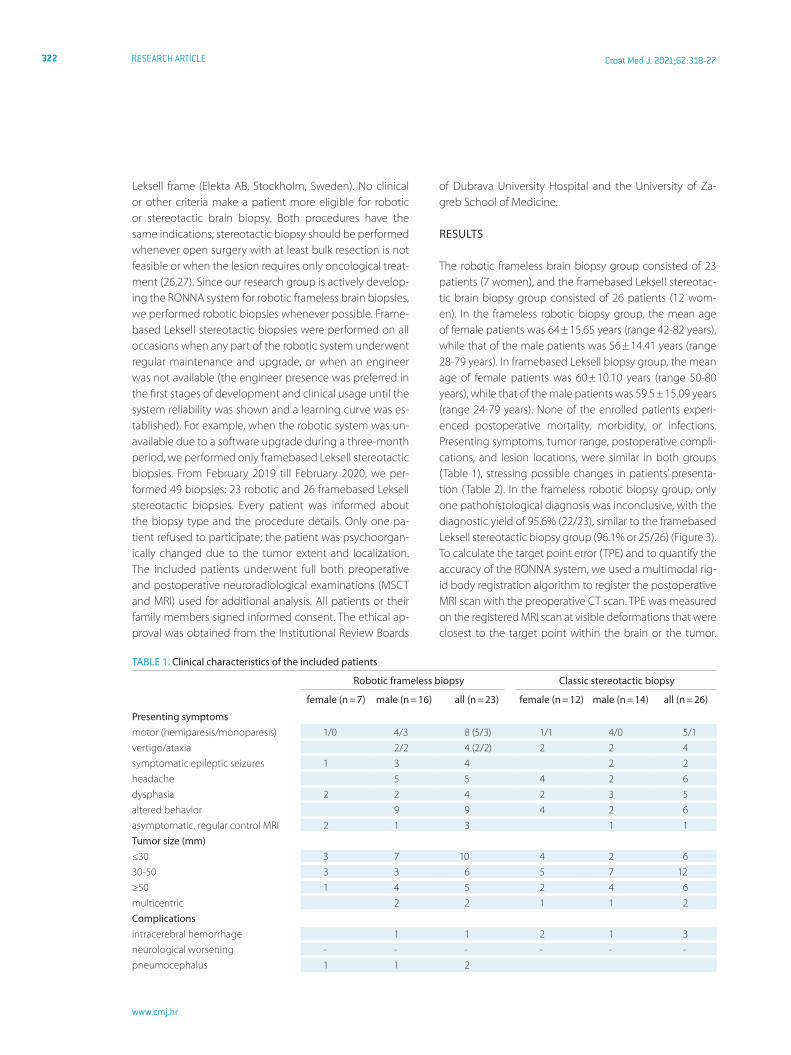
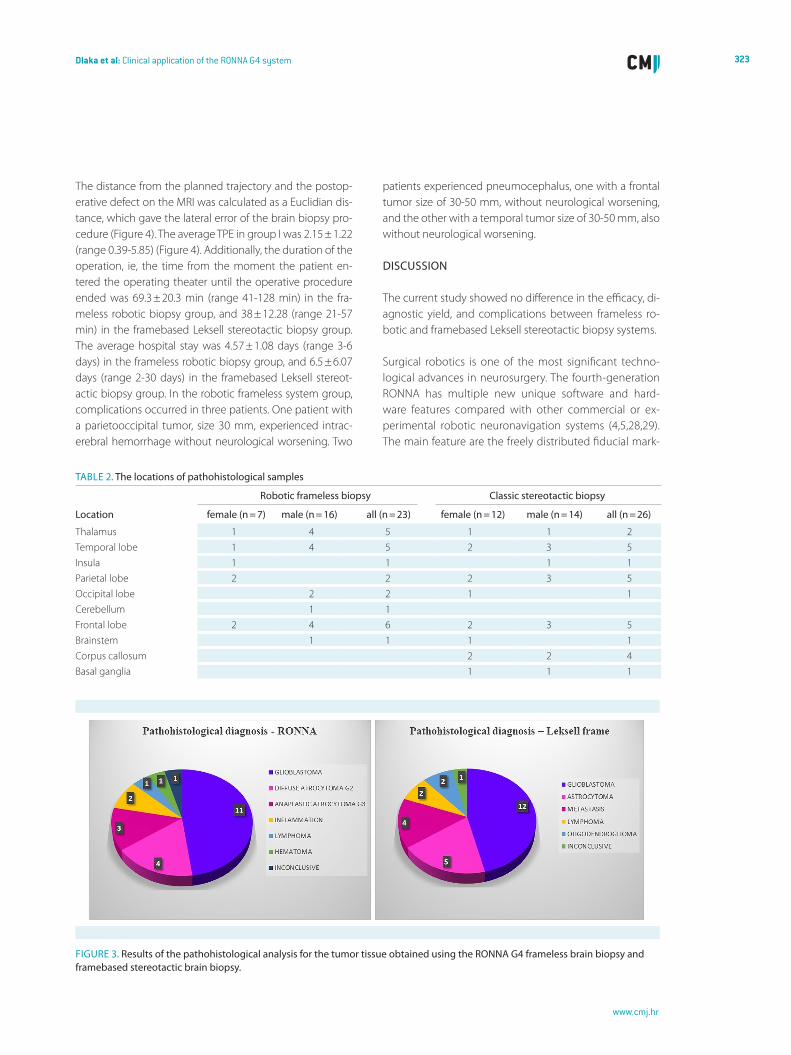
The robotic frameless brain biopsy group consisted of 23 patients (7 women), and the framebased Leksell stereotac-tic brain biopsy group consisted of 26 patients (12 wom-en). In the frameless robotic biopsy group, the mean age of female patients was 64 ± 15.65 years (range 42-82 years), while that of the male patients was 56 ± 14.41 years (range 28-79 years). In framebased Leksell biopsy group, the mean age of female patients was 60 ± 10.10 years (range 50-80 years), while that of the male patients was 59.5 ± 15.09 years (range 24-79 years). None of the enrolled patients experi-enced postoperative mortality, morbidity, or infections. Presenting symptoms, tumor range, postoperative compli-cations, and lesion locations, were similar in both groups (Table 1), stressing possible changes in patients’ presenta-tion (Table 2). In the frameless robotic biopsy group, only one pathohistological diagnosis was inconclusive, with the diagnostic yield of 95.6% (22/23), similar to the framebased Leksell stereotactic biopsy group (96.1% or 25/26) (Figure 3). To calculate the target point error (TPE) and to quantify the accuracy of the RONNA system, we used a multimodal rig-id body registration algorithm to register the postoperative MRI scan with the preoperative CT scan. TPE was measured on the registered MRI scan at visible deformations that were closest to the target point within the brain or the tumor.
TABle 1. Clinical characteristics of the included patients
323Dlaka et al: Clinical application of the RONNA G4 system
www.cmj.hr
The distance from the planned trajectory and the postop-erative defect on the MRI was calculated as a Euclidian dis-tance, which gave the lateral error of the brain biopsy pro-cedure (Figure 4). The average TPE in group I was 2.15 ± 1.22 (range 0.39-5.85) (Figure 4). Additionally, the duration of the operation, ie, the time from the moment the patient en-tered the operating theater until the operative procedure ended was 69.3 ± 20.3 min (range 41-128 min) in the fra-meless robotic biopsy group, and 38 ± 12.28 (range 21-57 min) in the framebased Leksell stereotactic biopsy group. The average hospital stay was 4.57 ± 1.08 days (range 3-6 days) in the frameless robotic biopsy group, and 6.5 ± 6.07 days (range 2-30 days) in the framebased Leksell stereot-actic biopsy group. In the robotic frameless system group, complications occurred in three patients. One patient with a parietooccipital tumor, size 30 mm, experienced intrac-erebral hemorrhage without neurological worsening. Two
patients experienced pneumocephalus, one with a frontal tumor size of 30-50 mm, without neurological worsening, and the other with a temporal tumor size of 30-50 mm, also without neurological worsening.
DiSCuSSiON
The current study showed no difference in the efficacy, di-agnostic yield, and complications between frameless ro-botic and framebased Leksell stereotactic biopsy systems.
Surgical robotics is one of the most significant techno-logical advances in neurosurgery. The fourth-generation RONNA has multiple new unique software and hard-ware features compared with other commercial or ex-perimental robotic neuronavigation systems (4,5,28,29). The main feature are the freely distributed fiducial mark-
TABle 2. The locations of pathohistological samples
FiguRe 3. Results of the pathohistological analysis for the tumor tissue obtained using the RONNA g4 frameless brain biopsy and framebased stereotactic brain biopsy.
RESEARCH ARTICLE324 Croat Med J. 2021;62:318-27
www.cmj.hr
ers, ie, bone fiducials, which consist of a bone screw and a special screw cap with interchangeable spherical ret-roreflective fiducials. The RONNA G4 bone screw set con-sists of a milled aluminum instrument tray holding eight screws and eight screw caps, and a specially designed screwdriver (Eonex Medical, Trnovec, Croatia) (Figure 5). The whole set is sterilized before surgery in the auto-clave. To minimize the effect of metallic artifacts in CT
images, the screw caps are made of polyether ether ketone, a medical-grade polymer. The screw caps
have a mechanical interface for standard medical retrore-flective snap-fit spherical markers (NDI – Northern Digital Inc., Waterloo, Canada). When it comes to software fea-tures, RONNA G4 uses a new and improved algorithm for
FiguRe 4. The methodology used for target point error measurement; tissue defect of tumor sampling site superimposed with a preoperative plan (A). A range of measured target point error values presented a mean ± standard deviation (B).
FiguRe 5. The RONNA bone screw set consisting of a milled aluminum instrument tray that holds eight screws, eight screw caps, and a specially designed screwdriver.
FiguRe 6. Trajectory cross-section of an inconclusive frameless robotic biopsy presenting target point on the tumor margin.
325Dlaka et al: Clinical application of the RONNA G4 system
www.cmj.hr
autonomous localization of fiducial markers in the image space (24), an algorithm for robot position planning with respect to the patient in the physical space (25), a nov-el pair-point correspondence algorithm for the patient registration from the image space to the physical space (30), and a novel method for determining an optimal ro-bot localization strategy in the physical space (31). Other major features that differentiate the RONNA G4 from the current state of-the-art robotic neuronavigation systems are a specifically designed universal mobile platform (32) and a new and accurate non-contact localization system (18). The universal mobile platform can be used for differ-ent robot arms and is not limited to a unique robot mod-el. The high-precision non-contact localization system RONNAstereo is used for accurate patient localization in the image space. For safety reasons, RONNA G4 has an uninterruptible power supply and 20-minute autonomy in case of power failure. It is also equipped with numerous built-in software and hardware safety measures. A speed limiter is used for all linear and joint movements to limit speeds to 30 mm/s or 5°/s. An emergency stop button (manual shutoff button) is incorporated both as a hard-ware and software option. All robot motions are planned before the execution, and collisions between the robot, its tools, and the patient are continuously checked.
Conventional frame-based procedures still represent the gold standard for brain biopsies. Although stereotactic frames such as Leksell, Cosman-Brown-Wells (Integra, May-field Cranial Stabilization System, Plainsboro, NJ, USA), and/or other frames are widely used (2), frameless biopsy has several advantages over stereotactic frame-based biopsies. One of the main advantages is less patient discomfort. Fur-thermore, frameless biopsies allow making preoperative scans a day before surgery, enabling a more flexible plan-ning strategy. More time is available for a detailed operative plan analysis, allowing the planning of better trajectories. An advantage of the RONNA G4 robotic neuronavigation system and a head holder (such as a Mayfield clamp – Inte-gra, Mayfield Cranial Stabilization System) in a frameless set-up allows the creation of both lateral and posterior trajec-tories without hardware limitations, which is not the case in frame-based biopsies (17). In addition, frameless systems allow multiple trajectory planning and switching between trajectories within seconds, thus simplifying and speeding-up the procedure for multiple biopsy locations.
Several points should be discussed when comparing our study with previously published frame-based, frameless, and robotic biopsy studies (2,5,28,29,33). In other studies,
the sample size varied from fewer than ten to more than 200 patients. Thus, we believe our preliminary results from a sample of 23 patients to be valid, considerable, and com-parable with other studies in the field of stereotactic brain biopsies. In frame-based and frameless biopsy studies, the mortality ranged from around 1% to 4% and morbidity from 1% to more than 20%, and in robotic brain biopsies the mor-tality and morbidity rates were less than 10%. In our study, no postoperative mortality or morbidity were observed. Complications included intracerebral hemorrhage in only one patient and pneumocephalus in two patients, visible on postoperative CT and/or MRI scan, without neurological worsening. In the available frame-based and frameless bi-opsy studies, both hemorrhage and neurological deficit oc-curred in 1% to 20% of patients. In robotic brain biopsies, hemorrhage and neurological deficit occurred in approxi-mately 4% to 28% of patients. The average procedure time ranges from 56.3 ± 23.6 to 185 ± 6 min for frameless biopsy studies and 54.2 ± 31.9 to 149 ± 32 min for frame-based stud-ies, while the average operation duration in our study was 71 ± 20.7 min. Still, we believe that the average procedure time will shorten as neurosurgeons become more experi-enced. The diagnostic yield in our sample was 95.6% (22/23). In the literature, the diagnostic yield for various frameless bi-opsy cohorts ranged from 86.6% to 100%, for frame-based biopsy cohorts it ranged from 84% to 100%, and for robotic brain biopsies it ranged from 75% to 100% (2,5,28,29,33).
The single inconclusive sample was located at the level of the crura cerebri and mesencephalon. Usually, tissue sam-ples obtained during brain biopsies are not sent for intraop-erative pathohistological diagnosis. The reasons are short operation duration, a few small tissue samples obtained during biopsy (tissue cylinder), and the time needed to perform intraoperative pathological analysis. Tissue sam-pling during biopsy may lead to malignant tumor bleed-ing causing intracerebral hemorrhage in 5% to more than 20% of the cases (34). Thus, to avoid possible complica-tions when performing deep-seated brain tumor biopsies with neuroradiological signs of malignancies, especially at the level of the crura cerebri as was the case in this patient, the target for tissue sampling is set on the tumor margin. We repeated the biopsy with Leksell frame; the pathohis-tological diagnosis was glioblastoma, and the patient un-derwent oncological treatment. On the repeated biopsy, based on our previous experience, we planned a riskier target point in the middle of the tumor since pathohis-tological diagnosis was mandatory for oncological treat-ment, which was the only treatment option for the pa-tient (26,27). In addition, postoperative MRI did not
RESEARCH ARTICLE326 Croat Med J. 2021;62:318-27
www.cmj.hr
show mistargeting (Figure 6). The obtained tissue was the tumor-surrounding tissue, as we planned due to the above mentioned reasons. In addition, several factors, such as high coronal trajectory angle, a long trajectory, and espe-cially minimal bending of the biopsy probe due to passing through the sulci, ie, tissues of different resistance, as well as the planned marginal area contributed to an unsuccess-ful pathohistological diagnosis.
Thus, the obtained RONNA G4 diagnostic yield values are comparable and higher than the average diagnostic yield in other studies (2,5,28,29,33). One of the challenges to the widespread acceptance of robotics in neurosurgery is the ability to train neurosurgeons to use these new technolo-gies. An increase in neurosurgeon’s experience over time is associated with shorter procedure duration, length of postoperative hospitalization, and the incidence of compli-cations. In neurosurgery, technical advancements will con-tinue to improve the speed, accuracy, and tactile ability in computer-assisted surgeries. Completely autonomous neu-rosurgical procedures are still a long way off, but robotics is already progressively changing the face of neurosurgery.
Our results should be interpreted with several limitations in mind. First, the number of participants is relatively small, and the results need to be confirmed in a larger cohort. In addition, an in-depth accuracy system analysis with includ-ed errors of measurement should be conducted, as was previously described in the literature (2,4,5,8,22). All other factors that considerably affect the accuracy and diagnos-tic yield should be investigated, and in vitro studies should be conducted (35). Different planning software programs and platforms prevented us from comparing the accuracy measurement between robotic frameless and framebased Leksell stereotactic biopsies.
In conclusion, the RONNA G4 robotic system is a safe and accurate tool for performing brain biopsy. Further studies need to enroll a larger patient sample for comparison with other robotic systems, to systematically analyze the entry and target point errors, and to investigate a wider applica-tion of robotic systems (DBS, SEEG, catheter placement). As the research on robotic brain biopsies is limited, our prospective study adds to the knowledge on robotic ste-reotactic brain biopsies. We plan to perform more detailed studies on robotic frameless and framebased Leksell ste-reotactic biopsies and their application accuracy.
Funding This research was supported by the Adris Foundation Grant “Appli-cation Analysis of a Robotic System for Stereotactic Neuronavigation” to DC.
ethical approval given the Institutional Review Boards of Dubrava Univer-sity Hospital and the Zagreb University School of Medicine (641-01/13-02).
Declaration of authorship DD, MŠ, and MR conceived and designed the study; DC, BJ, BŠ, FŠ, JV, FA, and DR acquired the data; DD, MŠ, and MR ana-lyzed and interpreted the data; DD, MŠ, and MR drafted the manuscript; ; DC, BJ, BŠ, FŠ, JV, FA, and DR critically revised the manuscript for important intellectual content; all authors gave approval of the version to be submit-ted; all authors agree to be accountable for all aspects of the work.
Competing interests All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organi-zation for the submitted work; no financial relationships with any organiza-tions that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influ-enced the submitted work.
References1 Spiegel eA, Wycis hT, Marks M, lee AJ. Stereotaxic apparatus for
operations on the human brain. Science. 1947:10;106(2754):349-50.
2 Dhawan S, he Y, Bartek J, Alattar AA, Chen CC. Comparison of frame-
based versus frameless intracranial stereotactic biopsy: systematic
review and meta-analysis. World Neurosurg. 2019;127:607-616.e4.
Medline:30974279 doi:10.1016/j.wneu.2019.04.016
3 Kwoh YS, hou J, Jonckheere eA, hayati S. A robot with improved
absolute po-sitioning accuracy for CT guided stereotactic brain
surgery. ieee Trans Biomed eng. 1988;35:153-60. Medline:3280462
doi:10.1109/10.1354
4 Fomenko A, Serletis D. Robotic stereotaxy in cranial neurosurgery:
a qualitative systematic review. Neurosurgery. 2018;83:642-50.
Medline:29253265 doi:10.1093/neuros/nyx576
5 Marcus hJ, Vakharia VN, Ourselin S, Duncan J, Tisdall M, Aquilina
K. Robot-assisted stereotactic brain biopsy: systematic review
and bibliometric analysis. Childs Nerv Syst. 2018;34:1299-309.