CLINICAL AUDIT ON THE ADHERENCE TO GUIDELINE ON SURGICAL PROPHYLAXIS FOR CHEMOPORT INSERTION PROCEDURE IN INSTITUT KANSER NEGARA Pharmacy Department National Cancer Institute, Putrajaya Team Members: Rozita binti Mohamad Nik Nuradlina binti Nik Adnan Mohd Syamir bin Mohamad Shukeri Noor Nashreen binti Mohd Sahar
Transcript
CLINICAL AUDIT ON THE ADHERENCE TO GUIDELINE ON SURGICAL PROPHYLAXIS FOR
CHEMOPORT INSERTION PROCEDURE IN INSTITUT KANSER NEGARA
Pharmacy Department
National Cancer Institute, Putrajaya
Team Members: Rozita binti Mohamad
Nik Nuradlina binti Nik Adnan
Mohd Syamir bin Mohamad Shukeri
Noor Nashreen binti Mohd Sahar
Table of Content
No. Topics
Abstract
1.0 Introduction
2.0 Methodology
3.0 Results
4.0 Remedial Measures
5.0 Re-audit Results after Implementation of Changes
6.0 Conclusion
7.0 Acknowledgments
8.0 References
9.0 Appendix
Clinical Audit on Adherence to Guideline on Surgical Prophylaxis for Chemoport Insertion
Procedure in Institut Kanser Negara.
1Nik Nuradlina N.A, 1Mohd Syamir M. S. , 1Noor Nashreen M.S., 1Rozita M.
1Pharmacy Department, National Cancer Institute, Putrajaya.
Introduction: Antibiotic prophylaxis in surgery has become the standard of care in many
departments, with little clinical data to support its wide acceptance. The rise in antibiotic-resistant
strains of organisms in all hospitals worldwide has forced every department to re-evaluate the use of
prophylactic antibiotics. Placement of central venous catheter for chemotherapy administration or
more commonly termed chemoport is a regular procedure in Institut Kanser Negara and through its
Medical Advisory Committee has established a guideline on Antibiotic Prophylaxis for Chemoport
Insertion. This guideline has listed cefazolin (a 1st generation cephalosporin) as the antibiotic of
choice for chemoport insertion procedure due to their ease of administration, low cost, and safety
profile.
Methodology: This is a two part cross-sectional study with initial audit phase (after introduction of
the guideline) will be retrospective and prospective study will be conducted in re-audit phase.
Criteria audited including antibiotics of choice for prophylaxis, the dosage according to the guideline
and also any subsequent antibiotics dose prescribed after the procedure. All in-patients registered
for the chemoport insertion that fulfil the inclusion criteria within the audit period were included.
Data collection from Electronic Medical Record (EMR) was conducted for each initial audit and re-
audit phase. After initial audit phase, all the intervention done by the in-patient pharmacist and
patient record from EMR were analysed to identify barriers. Strategies for change implemented prior
to re-audit phase include reminder, and reinforced the guideline during antibiotics screening by the
In-patient pharmacist and clinical pharmacist.
Results and Discussion: In initial phase, all three criteria did not meet the standard. 83.95% of prescription does not comply with the type of antibiotic outlined in the guideline. 70.75% of the antibiotic prescribed was amoxycillin/clavulanate injection. Of those who comply, only 11.76% does not prescribe the dose based on patient’s body weight. 10.38% of the antibiotic duration were prescribed beyond the stat dose with subsequent dose can be up to 9 days. During re-audit phase, all three criteria showed improvement after strategies for change conducted even though one standard were still not met. Conclusion: The awareness of the availability of the guideline and lack of adherence to the guideline
by the prescriber may result in unsuitable use of antibiotics and increase of antibiotics resistance
that reflect to longer ward admission and increasing treatment cost. Regular reminder, continuous
monitoring by clinical pharmacist on prescriber and stringent prescription screening by the In-
patient pharmacist for the chemoport insertion procedure is needed to enhanced adherence to the
guideline.
1.0 Introduction
Placement of central venous catheter for chemotherapy administration or more commonly
termed chemoport is a regular procedure in Institut Kanser Negara. Antibiotic prophylaxis in
surgery has become the standard of care in many departments, with little clinical data to
support its wide acceptance. The rise in antibiotic-resistant strains of organisms in all
hospitals worldwide has forced every department to re-evaluate the use of prophylactic
antibiotics. Institut Kanser Negara through its Medical Advisory Committee has established a
guideline on Antibiotic Prophylaxis for Chemoport Insertion. This guideline has listed
cefazolin (a 1st generation cephalosporin) as the antibiotic of choice for chemoport insertion
procedure. The guideline has been disseminated on May 18th 2016.
1.1 Literature Review
Surgical wounds are classified into four categories based on its infection risk. The four
categories are clean, clean-contaminated, contaminated and dirty. Prophylactic antibiotic is
widely used in surgical and interventional radiology procedure to prevent surgical site
infection. It is generally accepted to use prophylactic antibiotic in clean-contaminated
wound. Antibiotic use prior to contaminated or dirty procedures is more correctly
categorized as therapeutic rather than prophylactic (Moon, et al., 2010).
Chemoport placement is classified as a clean procedure. Therefore, routine use of antibiotic
prophylaxis is not recommended. However, antibiotic prophylaxis is suggested to be given if
placing a totally implantable device or if the patient is immunocompromised (Moon, et al.,
2010, Venkatesan, et al., 2010).
The majority of published evidence demonstrates that antimicrobial prophylaxis after
wound closure is unnecessary, and most studies comparing single-dose prophylaxis with
multiple-dose prophylaxis have not shown benefit of additional doses. Prolonged use of
prophylactic antimicrobials is associated with emergence of resistant bacterial strains
(Bratzler & Houck, 2004).
The antibiotic should be administered in an adequate dose based on patient body weight,
adjusted dosing weight, or body mass index and administration should be repeated intra-
operatively if the operation is still in progress 2 half-lives after the first dose to ensure
adequate antimicrobial levels until wound closure (Forse, et al, 1989). In obese patients, the
pharmacokinetics of drugs may be altered; therefore, dosage adjustments based on body
weight may be warranted in these patients (Bratzler, et al, 2013).
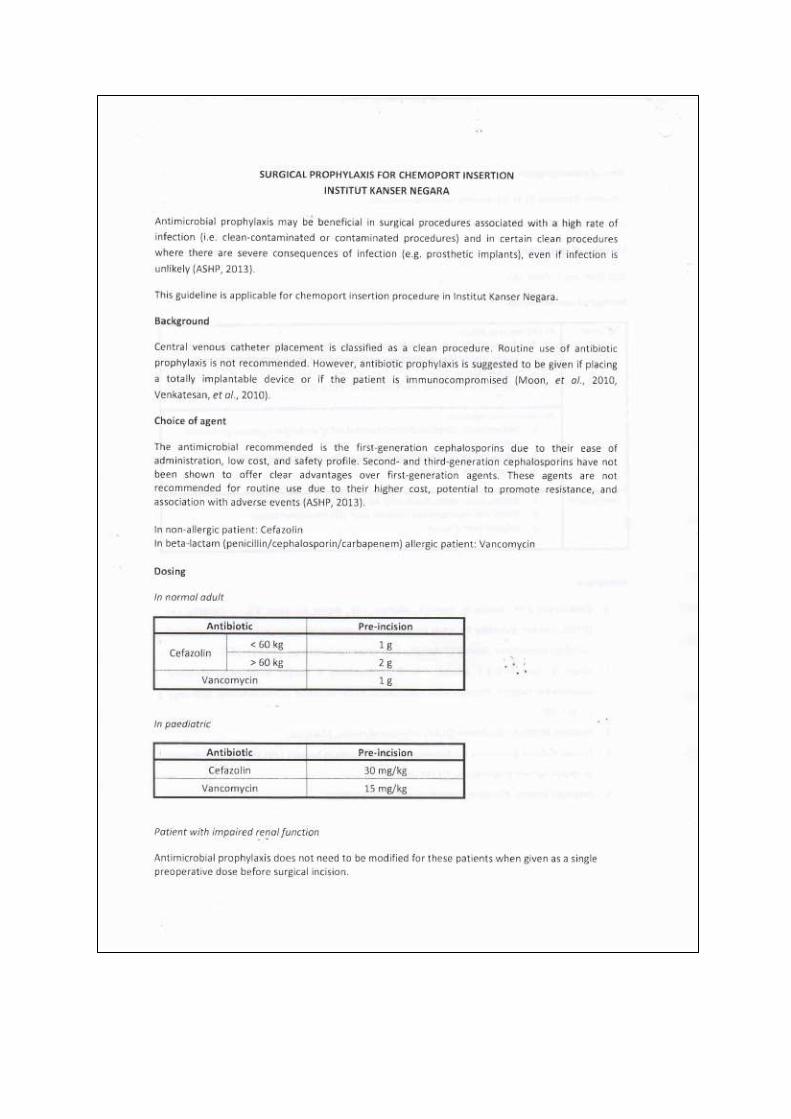
The antimicrobial recommended as surgical prophylaxis for chemoport insertion in Institut
Kanser Negara is the first-generation cephalosporins due to their ease of administration, low
cost, and safety profile. Second- and third-generation cephalosporins have not been shown
to offer clear advantages over first-generation agents. These agents are not recommended
for routine use due to their higher cost, potential to promote resistance, and association
with adverse events (ASHP, 2013).
Although antimicrobial prophylaxis plays an important role in reducing the rate of surgical
site infections (SSI), other factors that need to be addressed such as basic infection-control
strategies, the surgeon’s experience and technique, the duration of the procedure, hospital
and operating room environments, instrument sterilization issues, preoperative preparation
(temperature and glycaemic control), and the underlying medical condition of the patient
still have a strong impact on SSI rates (Bratzler, et al, 2013).
1.2 Problem Statement
Antibiotic prophylaxis for chemoport insertion guideline has been disseminated in Institut
Kanser Negara since May 2016. However, various type and duration of antibiotics was still
being prescribed for chemoport insertion procedure. This exercise might be justified or not.
If it is not justified, it would lead to unnecessary higher budget for antibiotics and possible
antibiotic resistance. Hence, this audit is conducted to identify the reasons for non-
adherence towards the guideline and to generate strategies for guideline enforcement,
improvement in guideline adherence, and reduce cost for antibiotic use.
1.3 Objectives
This is an audit on implementation of the Guideline on surgical prophylaxis for chemoport
insertion procedure in Institut Kanser Negara with three specific aims:
1. To identify the percentage of compliance to the newly introduced antibiotic guideline for chemoport insertion in National Cancer Institute.
2. To evaluate the reason(s) and type(s) of non-compliance towards the guideline. 3. To estimate the cost reduction for antibiotic usage after guideline implementation.
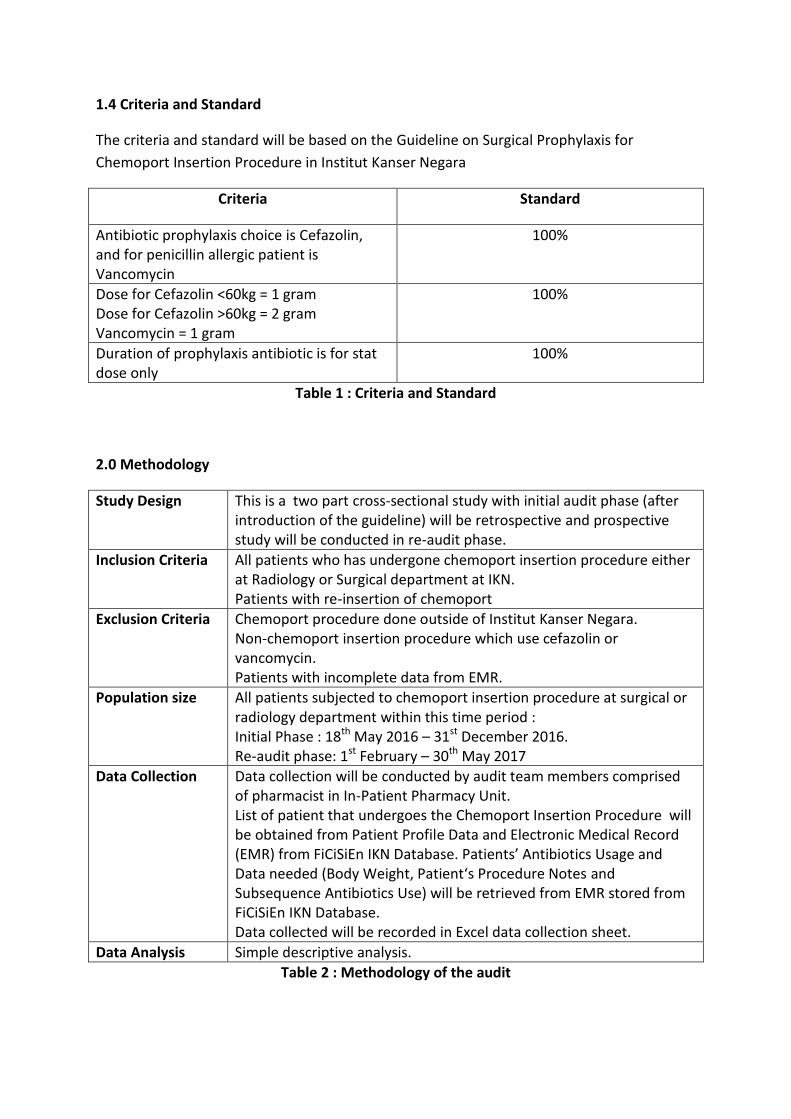
1.4 Criteria and Standard
The criteria and standard will be based on the Guideline on Surgical Prophylaxis for
Chemoport Insertion Procedure in Institut Kanser Negara
Criteria Standard
Antibiotic prophylaxis choice is Cefazolin, and for penicillin allergic patient is Vancomycin
100%
Dose for Cefazolin <60kg = 1 gram Dose for Cefazolin >60kg = 2 gram Vancomycin = 1 gram
100%
Duration of prophylaxis antibiotic is for stat dose only
100%
Table 1 : Criteria and Standard
2.0 Methodology
Study Design This is a two part cross-sectional study with initial audit phase (after introduction of the guideline) will be retrospective and prospective study will be conducted in re-audit phase.
Inclusion Criteria All patients who has undergone chemoport insertion procedure either at Radiology or Surgical department at IKN. Patients with re-insertion of chemoport
Exclusion Criteria Chemoport procedure done outside of Institut Kanser Negara. Non-chemoport insertion procedure which use cefazolin or vancomycin. Patients with incomplete data from EMR.
Population size All patients subjected to chemoport insertion procedure at surgical or radiology department within this time period : Initial Phase : 18th May 2016 – 31st December 2016. Re-audit phase: 1st February – 30th May 2017
Data Collection Data collection will be conducted by audit team members comprised of pharmacist in In-Patient Pharmacy Unit. List of patient that undergoes the Chemoport Insertion Procedure will be obtained from Patient Profile Data and Electronic Medical Record (EMR) from FiCiSiEn IKN Database. Patients’ Antibiotics Usage and Data needed (Body Weight, Patient‘s Procedure Notes and Subsequence Antibiotics Use) will be retrieved from EMR stored from FiCiSiEn IKN Database. Data collected will be recorded in Excel data collection sheet.
Data Analysis Simple descriptive analysis.
Table 2 : Methodology of the audit
3.0 Results
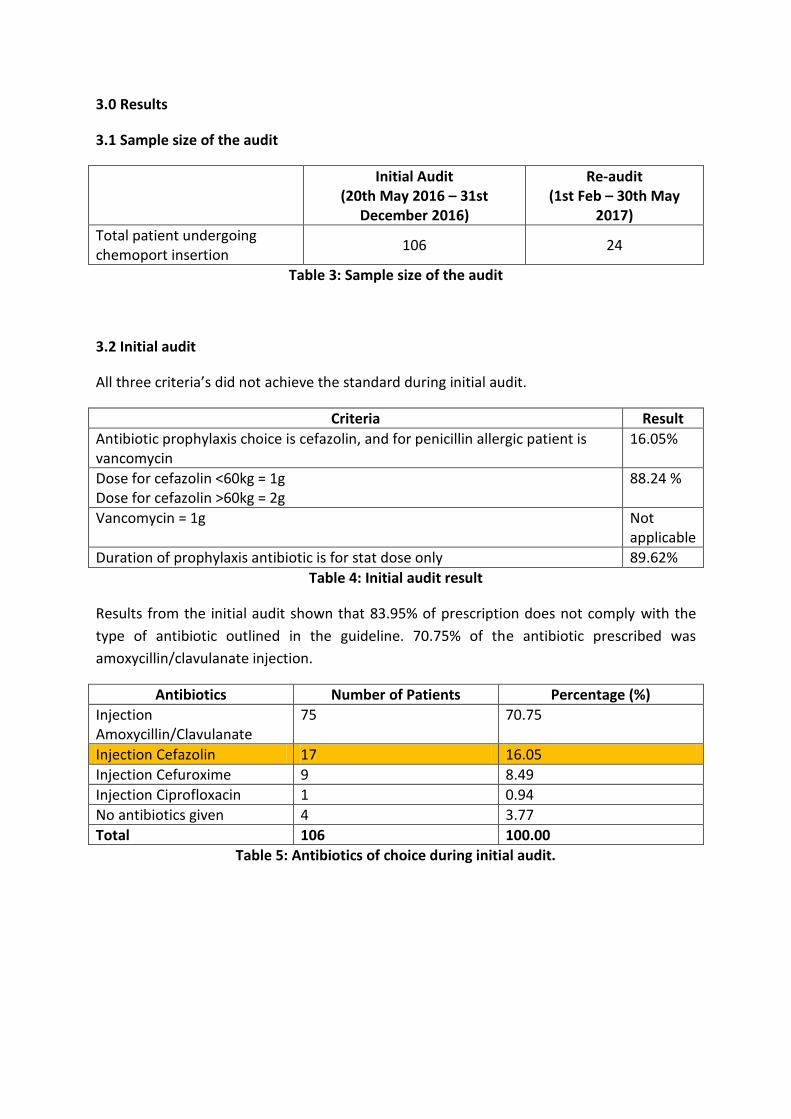
3.1 Sample size of the audit
Initial Audit (20th May 2016 – 31st
December 2016)
Re-audit (1st Feb – 30th May
2017)
Total patient undergoing chemoport insertion
106 24
Table 3: Sample size of the audit
3.2 Initial audit
All three criteria’s did not achieve the standard during initial audit.
Criteria Result
Antibiotic prophylaxis choice is cefazolin, and for penicillin allergic patient is vancomycin
16.05%
Dose for cefazolin <60kg = 1g Dose for cefazolin >60kg = 2g
88.24 %
Vancomycin = 1g Not applicable
Duration of prophylaxis antibiotic is for stat dose only 89.62%
Table 4: Initial audit result
Results from the initial audit shown that 83.95% of prescription does not comply with the
type of antibiotic outlined in the guideline. 70.75% of the antibiotic prescribed was
amoxycillin/clavulanate injection.
Antibiotics Number of Patients Percentage (%)
Injection Amoxycillin/Clavulanate
75 70.75
Injection Cefazolin 17 16.05
Injection Cefuroxime 9 8.49
Injection Ciprofloxacin 1 0.94
No antibiotics given 4 3.77
Total 106 100.00
Table 5: Antibiotics of choice during initial audit.
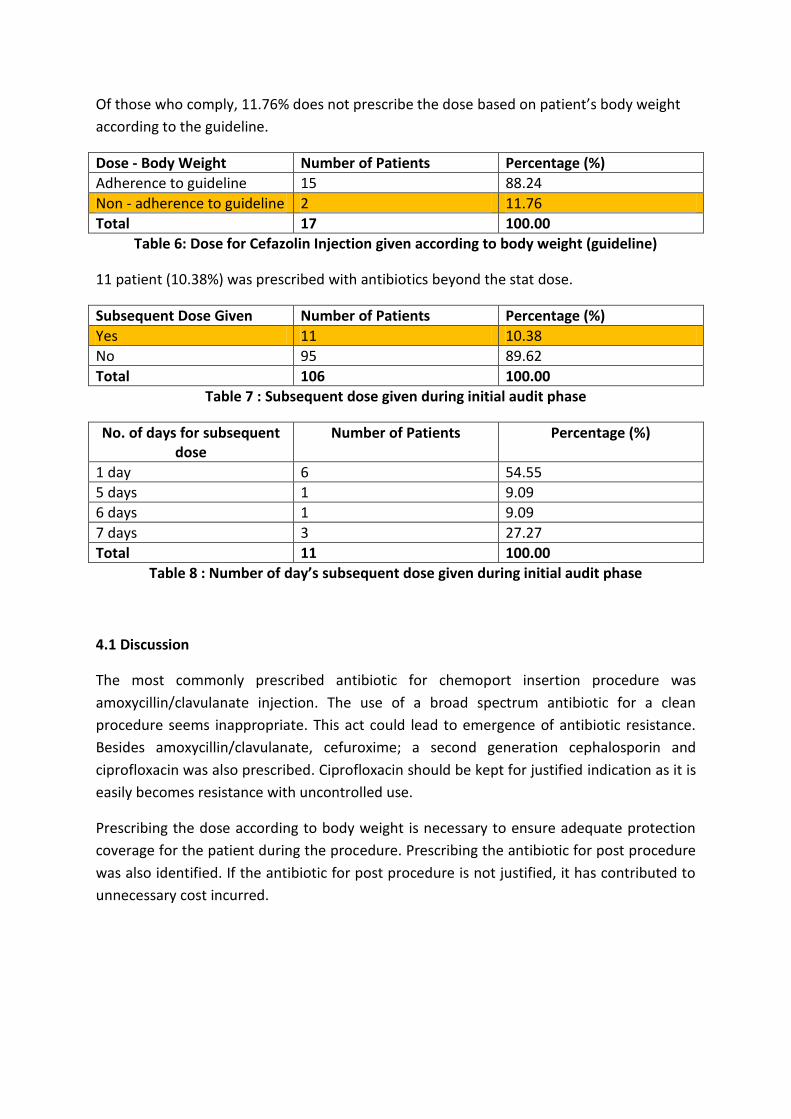
Of those who comply, 11.76% does not prescribe the dose based on patient’s body weight
according to the guideline.
Dose - Body Weight Number of Patients Percentage (%)
Adherence to guideline 15 88.24
Non - adherence to guideline 2 11.76
Total 17 100.00
Table 6: Dose for Cefazolin Injection given according to body weight (guideline)
11 patient (10.38%) was prescribed with antibiotics beyond the stat dose.
Subsequent Dose Given Number of Patients Percentage (%)
Yes 11 10.38
No 95 89.62
Total 106 100.00
Table 7 : Subsequent dose given during initial audit phase
No. of days for subsequent dose
Number of Patients Percentage (%)
1 day 6 54.55
5 days 1 9.09
6 days 1 9.09
7 days 3 27.27
Total 11 100.00
Table 8 : Number of day’s subsequent dose given during initial audit phase
4.1 Discussion
The most commonly prescribed antibiotic for chemoport insertion procedure was
amoxycillin/clavulanate injection. The use of a broad spectrum antibiotic for a clean
procedure seems inappropriate. This act could lead to emergence of antibiotic resistance.
Besides amoxycillin/clavulanate, cefuroxime; a second generation cephalosporin and
ciprofloxacin was also prescribed. Ciprofloxacin should be kept for justified indication as it is
easily becomes resistance with uncontrolled use.
Prescribing the dose according to body weight is necessary to ensure adequate protection
coverage for the patient during the procedure. Prescribing the antibiotic for post procedure
was also identified. If the antibiotic for post procedure is not justified, it has contributed to
unnecessary cost incurred.
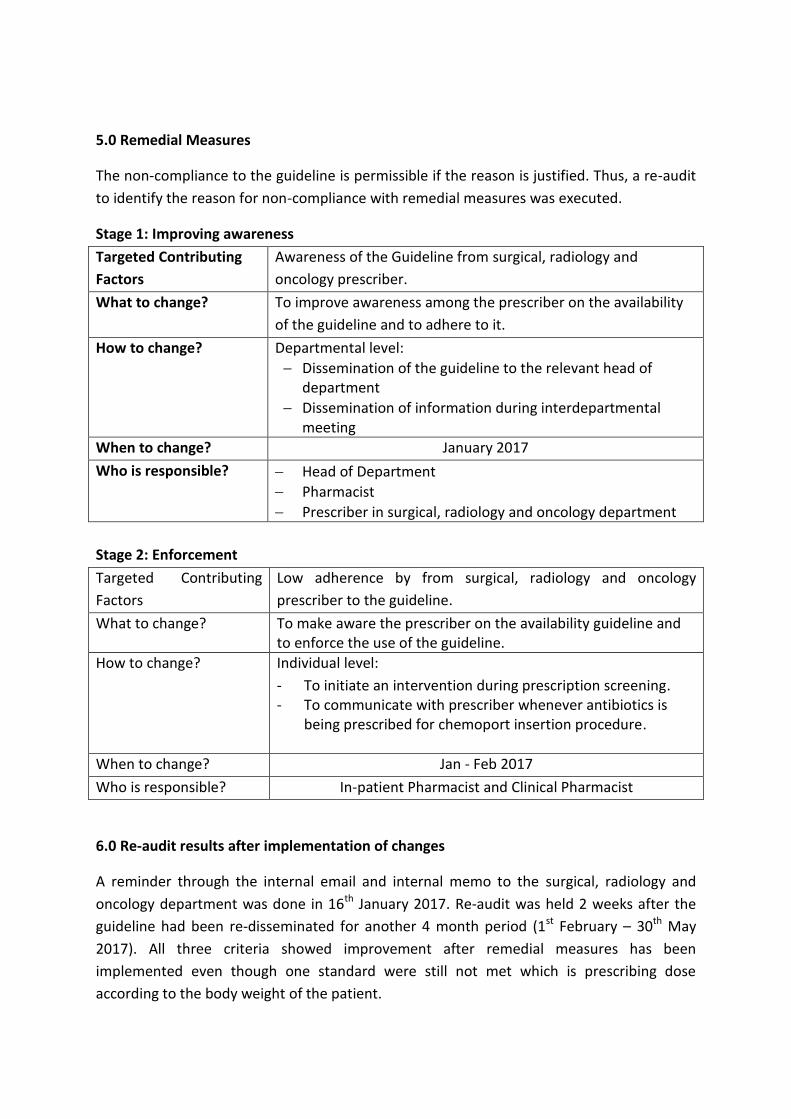
5.0 Remedial Measures
The non-compliance to the guideline is permissible if the reason is justified. Thus, a re-audit
to identify the reason for non-compliance with remedial measures was executed.
Stage 1: Improving awareness
Targeted Contributing
Factors
Awareness of the Guideline from surgical, radiology and
oncology prescriber.
What to change? To improve awareness among the prescriber on the availability
of the guideline and to adhere to it.
How to change? Departmental level:
Dissemination of the guideline to the relevant head of department
Dissemination of information during interdepartmental meeting
When to change? January 2017
Who is responsible? Head of Department
Pharmacist
Prescriber in surgical, radiology and oncology department
Stage 2: Enforcement
Targeted Contributing
Factors
Low adherence by from surgical, radiology and oncology
prescriber to the guideline.
What to change? To make aware the prescriber on the availability guideline and to enforce the use of the guideline.
How to change? Individual level:
- To initiate an intervention during prescription screening. - To communicate with prescriber whenever antibiotics is
being prescribed for chemoport insertion procedure.
When to change? Jan - Feb 2017
Who is responsible? In-patient Pharmacist and Clinical Pharmacist
6.0 Re-audit results after implementation of changes
A reminder through the internal email and internal memo to the surgical, radiology and
oncology department was done in 16th January 2017. Re-audit was held 2 weeks after the
guideline had been re-disseminated for another 4 month period (1st February – 30th May
2017). All three criteria showed improvement after remedial measures has been
implemented even though one standard were still not met which is prescribing dose
according to the body weight of the patient.
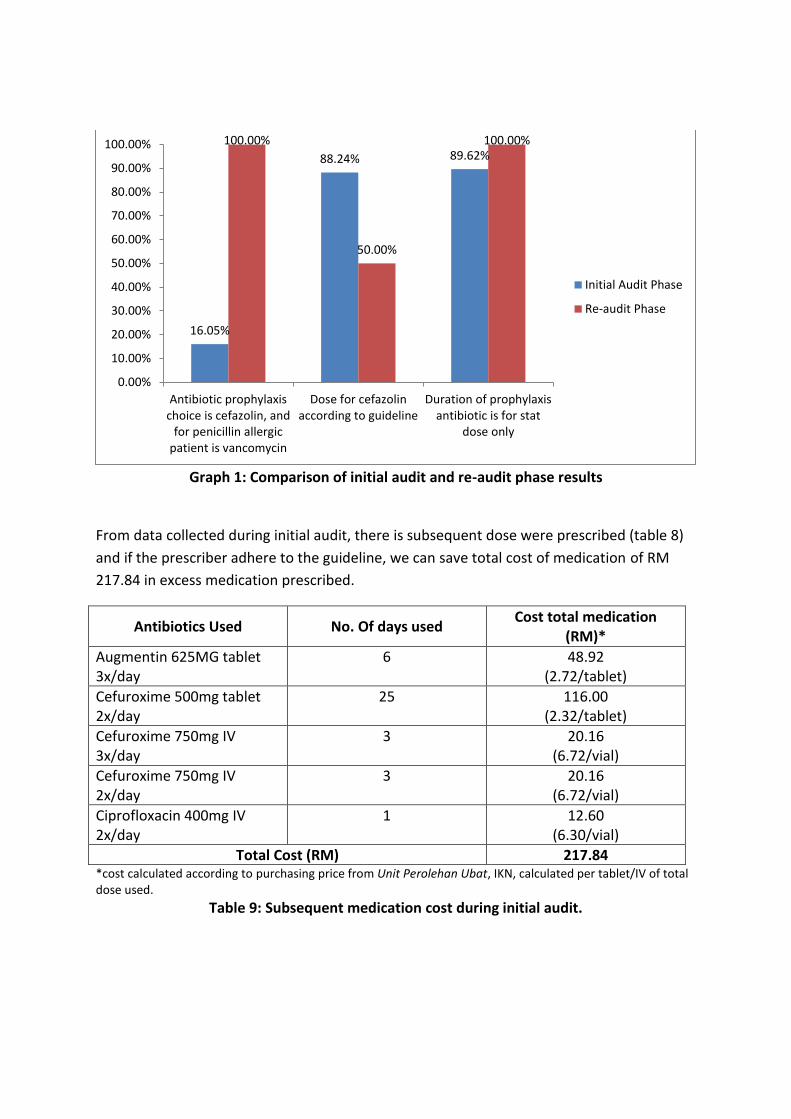
Graph 1: Comparison of initial audit and re-audit phase results
From data collected during initial audit, there is subsequent dose were prescribed (table 8)
and if the prescriber adhere to the guideline, we can save total cost of medication of RM
217.84 in excess medication prescribed.
Antibiotics Used No. Of days used Cost total medication
(RM)*
Augmentin 625MG tablet 3x/day
6 48.92 (2.72/tablet)
Cefuroxime 500mg tablet 2x/day
25 116.00 (2.32/tablet)
Cefuroxime 750mg IV 3x/day
3 20.16 (6.72/vial)
Cefuroxime 750mg IV 2x/day
3 20.16 (6.72/vial)
Ciprofloxacin 400mg IV 2x/day
1 12.60 (6.30/vial)
Total Cost (RM) 217.84 *cost calculated according to purchasing price from Unit Perolehan Ubat, IKN, calculated per tablet/IV of total dose used.
Table 9: Subsequent medication cost during initial audit.
16.05%
88.24% 89.62% 100.00%
50.00%
100.00%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Antibiotic prophylaxischoice is cefazolin, and
for penicillin allergicpatient is vancomycin
Dose for cefazolinaccording to guideline
Duration of prophylaxisantibiotic is for stat
dose only
Initial Audit Phase
Re-audit Phase
7.0 Conclusion
This audit revealed several weaknesses in guideline implementation on chemoport insertion
procedure. Lack of enforcement of the guideline during initial phase and low awareness
from the staff leading to unnecessary use and duration of antibiotic, which in turn may
contribute to the increased risk of antibiotic resistance and also increased the budget spent
on subsequent antibiotics. Even though there is stringent prescription screening from the
pharmacist on duty of In-Patient Pharmacy and Clinical Pharmacist; continuous audit,
routine reminders, support and monitoring from head of department, prescriber and also
clinical pharmacist in ward were necessary to facilitate improvements in adherence of the
guideline.
7.1 Recommendations
Guideline implementation could be enhanced by the following measures:
1. Regular monitoring by clinical pharmacist on prescriber for the chemoport insertion
procedure.
2. Continuous stringent prescription screening by the In-patient pharmacist.
3. Monthly reports on cefazolin injection usage with chemoport insertion procedure to the
department involved.
8.0 Acknowledgement
We would like to express our gratitude to doctors in radiology, surgical and oncology
department and AMS team that are involved directly and indirectly in this audit.
9.0 References
W. Bratzler, Dale and M. Houck, Peter, Antimicrobial Prophylaxis for Surgery: An Advisory
Statement from the National Surgical Infection Prevention Project .Surgical Infection
Forse,RA, Karam,B, MacLean,LD, Christou, NV. Antibiotic prophylaxis for surgery in
morbidly obese patients, Surgery , 1989, vol. 106 (pg. 750-6)
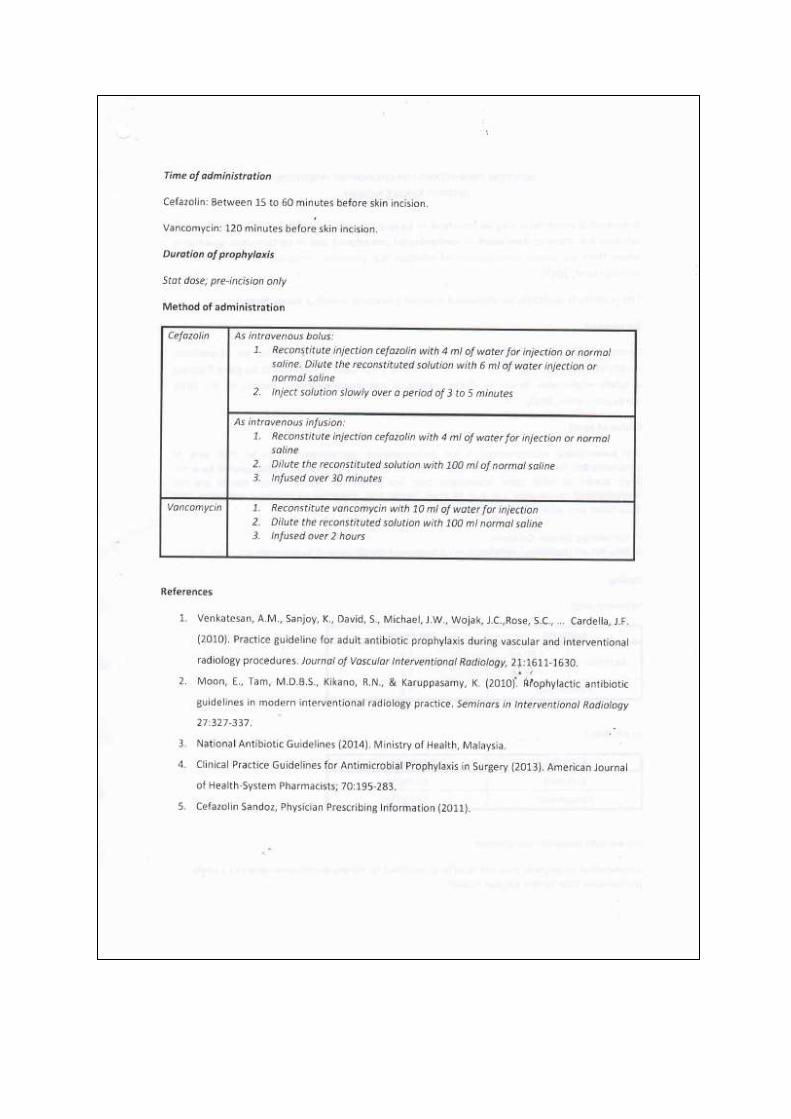
Venkatesan, A.M., Sanjoy, K., David, S., Michael, J.W., Wojak, J.C.,Rose, S.C., … Cardella, J.F. (2010). Practice guideline for adult antibiotic prophylaxis during vascular and interventional radiology procedures. Journal of Vascular Interventional Radiology, 21:1611-1630.
Moon, E., Tam, M.D.B.S., Kikano, R.N., & Karuppasamy, K. (2010). Prophylactic antibiotic guidelines in modern interventional radiology practice. Seminars in Interventional Radiology 27:327-337.
National Antibiotic Guidelines (2014). Ministry of Health, Malaysia.
Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery (2013). American Journal of Health-System Pharmacists; 70:195-283.
Cefazolin Sandoz, Physician Prescribing Information (2011).