57
Clinical Examination for Splinting Somaya Malkawi, PhD University of Jordan Occupational Therapy Department
| Date post: | 29-Dec-2015 |
| Category: |
Documents |
| Upload: | martha-watkins |
| View: | 214 times |
| Download: | 0 times |

Clinical Examination for Splinting
Somaya Malkawi, PhD
University of Jordan
Occupational Therapy Department
History, interviews, chart review, reportsPart 1
04/19/23

Obtaining a history
You should obtain the history from medical charts, surgical, radiologic reports
Physician’s referral or prescriptionAge, gender, diagnosis Past medical history and dates of occurrenceOccupation Pertinent medical history (e.g. diabetes, epilepsy, kidney, gout)UE dysfunction is due to orthopedic or neurological or trauma affecting soft tissue such as burn, tendon laceration)Anatomic structure involved at surgeryProtocol : different and decide on the rehabilitation program and timing
04/19/23

Interview
Impact of condition on functioning, family, economic status, social/emotional wellbeing
Co-histories from family, parents, friends, caregivers
Check questions page 77
Habits, stress, obesity
observation
In the initial process of evaluation while interviewing your client, use your observation skills!
Nonverbal communication (facial expressions and body language) mood, emotions, and motivation.Use of the involved UE and trunk: some clients may exaggerate their impairment (guarding or less AROM) Check points to observe on (page 77) or (form 5-1)Posture of whole UE.. Asymmetry Resting hand posture: 10 – 15 wrist flex/ 10 UD / 15—20 MCP flexSlight flexion and abd of thumb
04/19/23

palpation
Muscle tone (PROM) ask pt to relax muscles
Muscle symmetry (compare right and left)
Scar density
Tendon nodules
Masses (ganglia)
Skin temperature
Wear sterile gloves

AssessmentsPart 2
04/19/23

Pain
No equipment is necessary.
During initial evaluation; use a pain scale.Numeric analogue scale (1, 2, 3,… 10).Visual analogue scale (10 cm vertical line).Verbal rating scale (no pain, mild, moderate…).Graphic representation (point out pain on a body chart) (fig 5-3)Pain questionnaires (e.g. McGill pain questionnaire) usually used by pain management centers.
04/19/23

Methods
Obtain a written description of the pain including the following factors:
Level of pain: see previous slide.Location of pain: have the client point out his or her pain on a body chart and rate them (referred pain: palpation of one area results in pain in another area).Type of pain: throbbing (نابض), aching, sharp, stabbing, shooting, burning, or hypersensitivity to light touch.Frequency of pain: constant or intermittent! What seem to cause the pain? What is pain associated with (e.g. AROM). Children’s report of pain (table 5-3)
04/19/23
SkinColor Temperature Texture Muscle atrophy Scarring EdemaHair pattern Sweating Watch for Fragile skin ..older people , steroids, diabetes)Skin allergies (bandages , adhesive, latexMonitor rashes after prescription
Wound assessment
If the wound is closed; skip to scar assessment, if the wound is open, assess the following:
Size: length and width using a ruler, do not touch the wound by the ruler except was sterile. What about future measurements?Depth: use sterile cotton swap only if pt is comfortable Color: wound are red, yellow, black, or any of them together. We love the red wound!
1.1. RedRed: uninfected, definite borders, granulation tissue present, apparent revascularization
04/19/23

Wound assessment2.2. YellowYellow: wound may have odor, draining and
purulent, semi-liquid slough, usually in the late inflammatory stage, epithelialization will be delayed due to infection.dominant cellular activity is the macrophage (Pac Man),
3.3. BlackBlack: Presence of Escher (necrotic tissue) will increase the work required by the macrophage and delay healing.
04/19/23

Wound assessment
Drainage: mild, moderate, or heavy? 1. Serous: clear, white or slightly yellow,
indicator of healthy open wound. If infection is suspected, refer client back to
the referring physician.
04/19/23

Wound assessmentAmount of discharge Oder of discharge: means infection, if present refer client back to the referring physician.Temperature: use thermometers or temperature tapes to measure the temperature of an area near the wound and compare it with an intact area.
Always observe the wound for the cardinal signs of infection: redness, swelling, increased temperature and pain.
stages of wound healing and splinting precautions (next class) read chapter
04/19/23

Scar assessment
In assessing scar, consider the following:Color: deep red lighter with time.Size: length x width.Flat/raised: the scar itself maybe flat or raised, if raised describe it in terms of mild or moderate.
Sometimes their will be a lump under the skin which is a combination between scar and fluid, commonly it appears on the dorsum of the hand or on the wrist: describe it by location, size, and height.Adhesions: adhesions of superficial scar to underlying fascia and tendons. Can be seen during active movements. Observe and palpate and describe by mild, moderate, or sever or simply by raising the skin (the scar tissue)
04/19/23

Scar assessment
Precautions: Respect the healing of a new scar the tissue to which it may adhere.Do not move the scar if when a portion of the wound is still open.Do not aggressively attempt to move the scar within the first week after suture removal.Do not manipulate a scar strongly in the treatment or assessment of scar over a tendon in the early stages of healing.
04/19/23

ROM AssessmentPart 5
04/19/23
Vascular status assessmentPart 6
04/19/23

Vascular status assessment
Blood flow to the hand may be affected by proximal injuries or diagnoses, e.g.:
Injury to the hand itself.Conditions such as Raynaud's phenomenon.
04/19/23

Observation
Consider the following:
Color: White grayish (pallor)White grayish (pallor): arterial interruption.Congested purple blueCongested purple blue: venous blockage.Dusky blueDusky blue: chronic venous insufficiency.RedRed: venous problem or inflammatory phase of healing or infection.
04/19/23

Observation
Trophic changes (texture of the skin and nails) which can be the result of sympathetic nerve or vascular changes:
Dry/moist.Shiny/dull.Pain: in 2/3 of clients with UE vascular problems. Aching, cramping, tightness, or cold intolerance. May be associated with vibration, cold, or repetition.
04/19/23

Palpation tests of vascular status
Capillary Refill Test:
1. firmly press on the distal portion of the volar finger or finger nail.
2. Until it turns white.
3. Release and count seconds.
Normal refill time is less than 2 seconds.
04/19/23
Palpation tests of vascular status
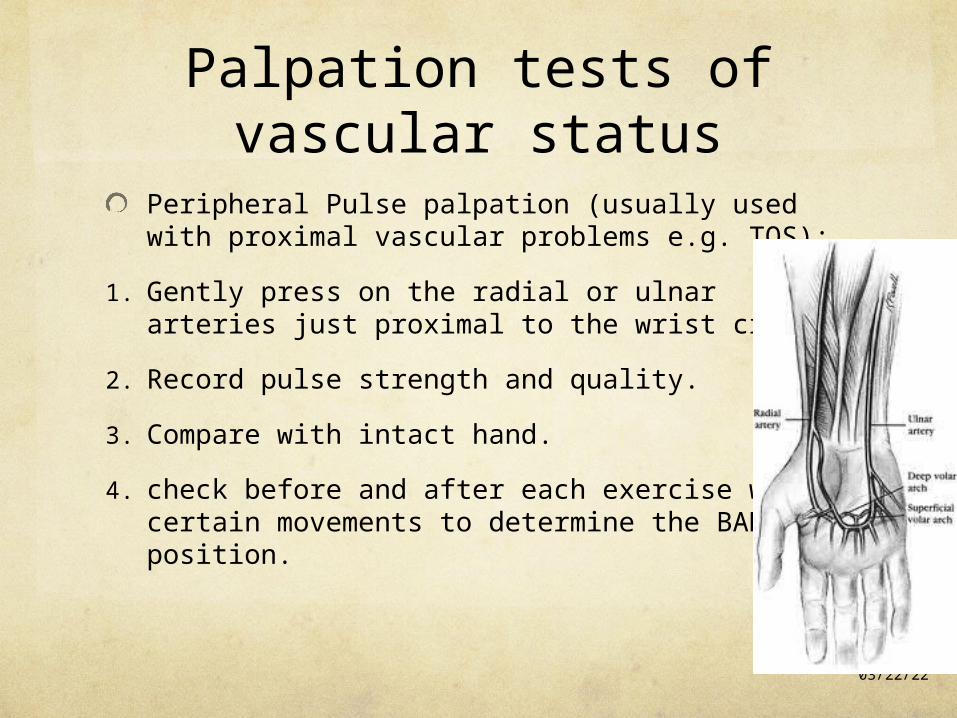
Peripheral Pulse palpation (usually used with proximal vascular problems e.g. TOS):
1. Gently press on the radial or ulnar arteries just proximal to the wrist crisis.
2. Record pulse strength and quality.
3. Compare with intact hand.
4. check before and after each exercise with certain movements to determine the BAD position.
04/19/23

Surface temperature assessmentIf forearm temperature is at least 4 degrees warmer than the fingertips
temperature then vascular problems are expected.
In testing for Raynaud’s phenomenon:
1. Test baseline temperature.
2. Test after being in a warm room for 30 minutes.
3. Record time of temperature returning to baseline.
4. Test after being immersed in ice for 20 seconds.
5. Record time of temperature returning to baseline.
Normal time is 10 minutes, Raynaud’s phenomenon patients may take 20 – 45 minutes.
04/19/23

Assessment of SwellingPart 7
04/19/23

Swelling Inflammatory swelling is a normal body response to injury, surgery or trauma, bringing good cells for healing.
Normal reduction of edema begins within 2 weeks post surgery/trauma/injury but may take months to complete.
Edema that does not decrease gradually and stays longer than 2 weeks is a problem!! it becomes more like gel interferes with joint and tendon motion UE function.
Inflammatory edema that occur after injury, surgery or insult starts as fluids spongy fibrotic!!.
So what?? Resistant to methods aimed at reducing the swelling
04/19/23

swelling
You should consider:
Amount of swelling:Volumetric displacement.Circumferential measurement.
Characteristics of edema:observation.Palpation.
04/19/23

Volumetric displacement
Equipments:Tank.Collection beaker.Graduated cylinder.
Methods:See picture next slide.
Notes:After measuring the affected hand, compare it to the intact hand, a difference of 10-ml is significant and shows a systematic increase in volume.
04/19/23

Volumetric displacement
Precautions: This method must not be used with: open wounds, unstable vascular status, casts, external fixators, etc.
Discussion:To increase test reliability, repeat the test 3 times and average.To increase test reliability, mark the forearm at the edge of water! Web-space between fingers.
04/19/23
Circumferential measurement
Equipments:Tape measure with finger loop (standardize location in relation to anatomic landmarks, standardize tension!).
Methods:Apply tape measure.Tighten.Record reading.
Discussion:To increase reliability: standardize location in relation to anatomic landmarks, standardize tension, and have the same therapist do the test all times.Compare to intact hand.
04/19/23

observation
Look for and document using a checklist including:
Shininess.Dryness.Loss of joint creases.Skin color (erythematicerythematic, cyanosiscyanosis, or pallorpallor).
04/19/23
Assessment of SensationPart 8
04/19/23

Static two-point discrimination
Measures innervation density (number of nerve endings).
Flexor zones I and II are to be tested.
Two-point discrimination relates to the clients’ ability to feel something and to know what they are feeling.
Equipments:Disk-Criminator.Boley gauge.
04/19/23

Static two-point discrimination
Methods:Ask patient to respond by “two” or “one”.Support client’s hand.Occlude the client vision.Start with 5 mm.Force must be applied to the point of blanching, in a longitudinal direction, and perpendicular to the skin.If patient recognizes 5 mm increase distance, vice versa.Begin distally and progress proximally.
04/19/23

Static two-point discrimination
Scoring:7 out of 10 correct response in one area are required for a correct responses.
04/19/23
Distance Score
1 – 5 mmNormal
6 – 10 mmFair
11 -15 mmPoor
One point perceived Protective sensation only
No points perceivedAnesthetic

Moving two-point discrimination
Always returns earlier than static two-point discrimination.
Measures progress in return of sensation following nerve injury.
Equipments:Disk-Criminator.Boley gauge.
04/19/23

Moving two-point discrimination
Methods:Ask patient to respond by “two” or “one”.Support client’s hand.Occlude the client vision.Start with 5 mm.Moving force must be applied to the point of blanching, in a longitudinal direction, and perpendicular to the skin, along the finger tip only.Begin proximally and progress distally.Begin with 5 – 8 mm and increase or decrease as needed.
04/19/23

Moving two-point discrimination
Scoring:7 out of 10 correct response in one area are required for a correct responses.2 mm is considered normal moving two-point discrimination.
04/19/23
Touch/Pressure Threshold Test
Recovers earlier than two-point discrimination sensation.
Effective in identifying sensory impairments due to nerve compressions.
Equipments:The Semmes-Weinstein Pressure Aesthesiometer kit of 20 monofilaments (5-monofilaments kit is also available).
04/19/23
Touch/Pressure Threshold Test
Equipments:The Semmes-Weinstein Pressure Aesthesiometer kit of 20 monofilaments (5-monofilaments kit is also available).
04/19/23
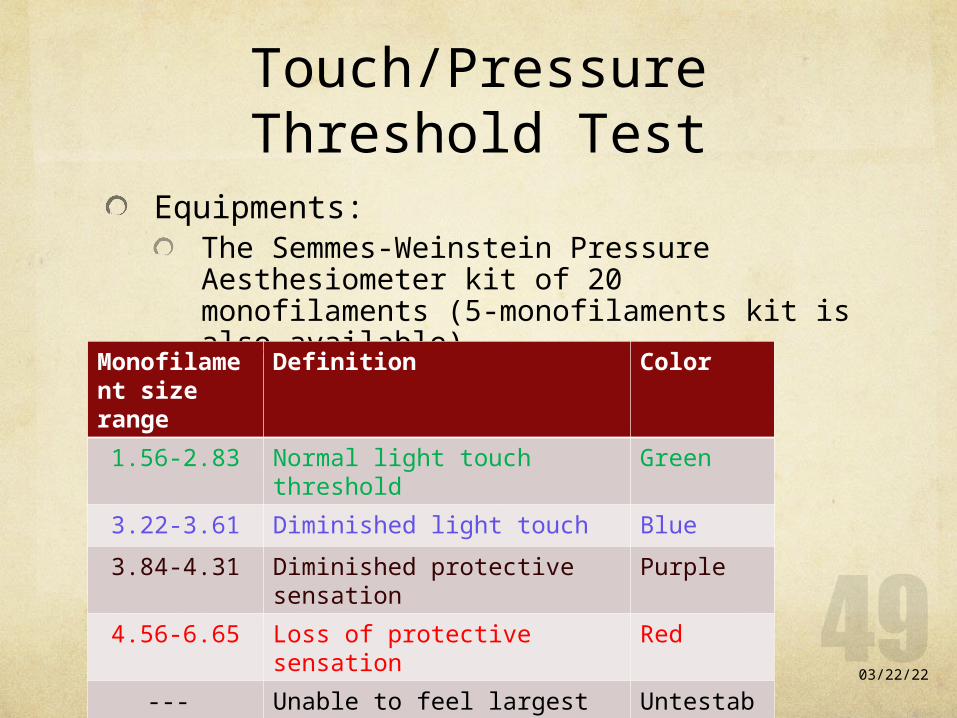
Color Definition Monofilament size range
GreenNormal light touch threshold1.56-2.83
BlueDiminished light touch3.22-3.61
PurpleDiminished protective sensation
3.84-4.31
RedLoss of protective sensation 4.56-6.65
Untestable
Unable to feel largest MF---

Touch/Pressure Threshold Test
Methods:Explain the test to client.Support the hand in a putty.Occlude client’s vision.Ask the patient to respond with “touch” when he/she feels a touch.Begin with the largest green MF. If responded continue to smaller, if no response continue to larger MF.For green and blue MFs, apply the filament must be applied 3 times, 1 correct response is good enough. All other large MFs must be applied once for each trial.Distal to proximal.
04/19/23
Touch/Pressure Threshold Test
Filament must be applied perpendicular to the skin until it bends. Apply in 1-1.5 seconds hold for 1.5 seconds lift in 1-1.5 seconds. Record on a hand chart (MF size and color).
04/19/23

Localization of light touch
The last sensory stimulus to return.
Has a significant importance after nerve repair.
Equipments:Smallest MF recognized earlier. Determined by the previous test.Cotton ball.
04/19/23

Localization of light touch
Methods:Explain the test to client.Support the hand in a putty.Occlude client’s vision.Touch the hand somewhere and dot it on a chart.Ask the patient to respond by opening his/her eyes and point out where you’ve touch him/her.If the response was correct do not draw any thing on the chart.If the client pointed out the stimulus in another place than given, draw an arrow from the dot you’ve drawn toward the place he/she pointed out.
04/19/23

Assessment of coordinationPart 9
04/19/23

Coordination assessment
O’Connor dexterity test.
Nine-hole Peg test.
Jebsen-Taylor hand function test.
Minnesota rate of manipulation test.
Crawford small parts dexterity test.
Purdue peg board.
04/19/23

Assessment of strengthPart 10
04/19/23

contraindications
As simple as this: is the testing going to damage a healing process (fracture, ligament repair, tendon laceration, tendon transfer, etc)?
So do not perform strength testing except when resistance is approved by referring physician.
04/19/23

Grip strength testAlways use the Jamar grip dynamometer.
Do not ignore calibration!
Testing setting: Client seated.Shoulder adducted.Elbow flexed to 90 degrees.Forearm neutral.Place dynamometer in the client’s hand.Provide gentle support at the base of the dynamometer.Instruct client squeeze smoothly not jerkily.Allow wrist extension during grip.
04/19/23

Grip strength test
Methods and procedures: Standard grip test: 3 trials on the 2nd handle setting.Five-level grip test: 1 trial on each handle setting, when curve is a flat line or shows up/down/up/down waves lack of maximal efforts. Rapid change grip test: therapist alternate the dynamometer between hands for 10 trials for each hand. Thought to prevent client from self-limiting his grip strength!!!!!!!!!
There are normative data, BUT compare to the intact hand if possible.
04/19/23

Pinch strength test
Use the pinchmeter.
Testing setting: Client seated.Shoulder adducted.Elbow flexed to 90 degrees.Forearm neutral.Place pinchmeter in the client’s hand.Instruct client to squeeze smoothly not jerkily.
04/19/23
Pinch strength test
Methods and procedures, proceed as following: Lateral pinch (key pinch): pinchmeter between radial side of the index and the thumb.Three-point pinch (three jaw chuck pinch): pinchmeter between the pulp of the thumb and the pulps of the index and middle fingers. Two-point pinch (tip to tip pinch): between the tip of the index and the tip of the thumb.
Ask the patient to pinch as hard as possible.
04/19/23

MMT
You’ve already learned that.
Note: thumb and fingers tendon repairs are sufficiently strong to test until after 14 weeks after surgery.
04/19/23

Splinting precautionsPart 11
04/19/23
Splint precautions
Form 5-2 Check off sheet
04/19/23

Assessment of functional usePart 11
04/19/23

Functional use
DASH
04/19/23

















