OBSTETRICS Clinical experience and follow-up with large scale single-nucleotide polymorphismebased noninvasive prenatal aneuploidy testing Pe’er Dar, MD; Kirsten J. Curnow, PhD; Susan J. Gross, MD; Megan P. Hall, PhD; Melissa Stosic, MS; Zachary Demko, PhD; Bernhard Zimmermann, PhD; Matthew Hill, PhD; Styrmir Sigurjonsson, PhD; Allison Ryan, PhD; Milena Banjevic, PhD; Paula L. Kolacki, MS; Susan W. Koch, MS; Charles M. Strom, MD, PhD; Matthew Rabinowitz, PhD; Peter Benn, DSc OBJECTIVE: We sought to report on laboratory and clinical experience following 6 months of clinical implementation of a single-nucleotide polymorphismebased noninvasive prenatal aneuploidy test in high- and low-risk women. STUDY DESIGN: All samples received from March through September 2013 and drawn 9 weeks’ gestation were included. Samples that passed quality control were analyzed for trisomy 21, trisomy 18, tri- somy 13, and monosomy X. Results were reported as high or low risk for fetal aneuploidy for each interrogated chromosome. Relationships between fetal fraction and gestational age and maternal weight were analyzed. Follow-up on outcome was sought for a subset of high-risk cases. False-negative results were reported voluntarily by providers. Positive predictive value (PPV) was calculated from cases with an available prenatal or postnatal karyotype or clinical evaluation at birth. RESULTS: Samples were received from 31,030 patients, 30,705 met study criteria, and 28,739 passed quality-control metrics and received a report detailing aneuploidy risk. Fetal fraction correlated positively with gestational age, and negatively with maternal weight. In all, 507 patients received a high-risk result for any of the 4 tested conditions (324 trisomy 21, 82 trisomy 18, 41 trisomy 13, 61 monosomy X; including 1 double aneuploidy case). Within the 17,885 cases included in follow-up analysis, 356 were high risk, and outcome information revealed 184 (51.7%) true positives, 38 (10.7%) false positives, 19 (5.3%) with ultrasound findings suggestive of aneuploidy, 36 (10.1%) spontaneous abortions without karyotype confirmation, 22 (6.2%) terminations without karyotype confirmation, and 57 (16.0%) lost to follow-up. This yielded an 82.9% PPV for all aneuploidies, and a 90.9% PPV for trisomy 21. The overall PPV for women aged 35 years was similar to the PPV for women aged <35 years. Two patients were reported as false negatives. CONCLUSION: The data from this large-scale report on clinical application of a commercially available noninvasive prenatal test suggest that the clinical performance of this single-nucleotide polymorphismebased noninvasive prenatal test in a mixed high- and low-risk population is consistent with performance in validation studies. Key words: low-risk, noninvasive prenatal testing, single-nucleotide polymorphism, trisomy 21 Cite this article as: Dar P, Curnow KJ, Gross SJ, et al. Clinical experience and follow-up with large scale single-nucleotide polymorphism—based noninvasive prenatal aneuploidy testing. Am J Obstet Gynecol 2014;211:527.e1-17. S ince becoming clinically available in late 2011, cell-free DNA (cfDNA)- based noninvasive prenatal testing (NIPT) for fetal aneuploidy has seen an unprecedented rapid adoption into clinical care. 1 This followed multiple publications on methodologies, val- idation, and test performance, 2-14 all demonstrating improved sensitivities From the Division of Fetal Medicine, Department of Obstetrics and Gynecology and Women’s Health, Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, NY (Dr Dar); Natera Inc, San Carlos (Drs Curnow, Gross, Hall, Demko, Zimmermann, Hill, Sigurjonsson, Ryan, Banjevic, and Rabinowitz and Ms Stosic), and Quest Diagnostics, Nichols Institute, San Juan Capistrano (Ms Kolacki, Ms Koch, and Dr Strom), CA; and Division of Human Genetics, Department of Genetics and Developmental Biology, University of Connecticut Health Center, Farmington, CT (Dr Benn). Received April 5, 2014; revised June 30, 2014; accepted Aug. 6, 2014. This study was supported by Natera Inc. K.J.C., S.J.G., M.P.H., M.S., Z.D., B.Z., M.H., S.S., A.R., M.B., and M.R. are employees of Natera Inc. P.D. participated in a multicenter clinical trial sponsored by Natera Inc and received research funding, but did not personally receive any funding. P.B. is a paid consultant and member of an advisory board for Natera Inc. P.L.K., S.W.K., and C.M.S. report no conflict of interest. Presented at the European Human Genetics Conference 2014 of the European Society of Human Genetics, Milan, Italy, May 31-June 3, 2014, and at the 2014 Annual Clinical Genetics Meeting of the American College of Medical Genetics and Genomics, Nashville, TN, March 25-29, 2014. Corresponding author: Peter Benn, DSc. [email protected]0002-9378/$36.00 ª 2014 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.ajog.2014.08.006 NOVEMBER 2014 American Journal of Obstetrics & Gynecology 527.e1 Research ajog.org
Transcript
Research ajog.org
OBSTETRICS
Clinical experience and follow-up with largescale single-nucleotide polymorphismebasednoninvasive prenatal aneuploidy testingPe’er Dar, MD; Kirsten J. Curnow, PhD; Susan J. Gross, MD; Megan P. Hall, PhD;Melissa Stosic, MS; Zachary Demko, PhD; Bernhard Zimmermann, PhD; Matthew Hill, PhD;Styrmir Sigurjonsson, PhD; Allison Ryan, PhD; Milena Banjevic, PhD; Paula L. Kolacki, MS;Susan W. Koch, MS; Charles M. Strom, MD, PhD; Matthew Rabinowitz, PhD; Peter Benn, DSc
OBJECTIVE:We sought to report on laboratory and clinical experience (324 trisomy 21, 82 trisomy 18, 41 trisomy 13, 61 monosomy X;
following 6 months of clinical implementation of a single-nucleotidepolymorphismebased noninvasive prenatal aneuploidy test in high-and low-risk women.
STUDY DESIGN: All samples received from March through September2013 and drawn �9 weeks’ gestation were included. Samples thatpassed quality control were analyzed for trisomy 21, trisomy 18, tri-somy 13, and monosomy X. Results were reported as high or low riskfor fetal aneuploidy for each interrogated chromosome. Relationshipsbetween fetal fraction and gestational age and maternal weight wereanalyzed. Follow-up on outcome was sought for a subset of high-riskcases. False-negative results were reported voluntarily by providers.Positive predictive value (PPV) was calculated from cases with anavailable prenatal or postnatal karyotype or clinical evaluation at birth.
RESULTS: Samples were received from 31,030 patients, 30,705 metstudy criteria, and 28,739 passed quality-control metrics and receiveda report detailing aneuploidy risk. Fetal fraction correlated positivelywith gestational age, and negatively with maternal weight. In all, 507patients received a high-risk result for any of the 4 tested conditions
From the Division of Fetal Medicine, Department of Obstetrics and Gynecologof Medicine, Bronx, NY (Dr Dar); Natera Inc, San Carlos (Drs Curnow, GrossRabinowitz and Ms Stosic), and Quest Diagnostics, Nichols Institute, San JuHuman Genetics, Department of Genetics and Developmental Biology, Univ
Received April 5, 2014; revised June 30, 2014; accepted Aug. 6, 2014.
This study was supported by Natera Inc.
K.J.C., S.J.G., M.P.H., M.S., Z.D., B.Z., M.H., S.S., A.R., M.B., and M.R. arsponsored by Natera Inc and received research funding, but did not personalboard for Natera Inc. P.L.K., S.W.K., and C.M.S. report no conflict of interes
Presented at the European HumanGenetics Conference 2014 of the Europea2014 Annual Clinical Genetics Meeting of the American College of Medical G
0002-9378/$36.00 � ª 2014 Elsevier Inc. All rights reserved. � http://dx.doi.org/10.1
including 1 double aneuploidy case). Within the 17,885 cases includedin follow-up analysis, 356 were high risk, and outcome informationrevealed 184 (51.7%) true positives, 38 (10.7%) false positives, 19(5.3%) with ultrasound findings suggestive of aneuploidy, 36 (10.1%)spontaneous abortions without karyotype confirmation, 22 (6.2%)terminations without karyotype confirmation, and 57 (16.0%) lost tofollow-up. This yielded an 82.9% PPV for all aneuploidies, and a90.9% PPV for trisomy 21. The overall PPV for women aged�35 yearswas similar to the PPV for women aged<35 years. Two patients werereported as false negatives.
CONCLUSION: The data from this large-scale report on clinicalapplication of a commercially available noninvasive prenatal testsuggest that the clinical performance of this single-nucleotidepolymorphismebased noninvasive prenatal test in a mixed high-and low-risk population is consistent with performance in validationstudies.
Cite this article as: Dar P, Curnow KJ, Gross SJ, et al. Clinical experience and follow-up with large scale single-nucleotide polymorphism—based noninvasive prenatalaneuploidy testing. Am J Obstet Gynecol 2014;211:527.e1-17.
ince becoming clinically available in
S late 2011, cell-free DNA (cfDNA)-based noninvasive prenatal testing
(NIPT) for fetal aneuploidy has seen anunprecedented rapid adoption intoclinical care.1 This followed multiple
y andWomen’s Health, M, Hall, Demko, Zimmermaan Capistrano (Ms Kolackersity of Connecticut Heal
e employees of Natera Incly receive any funding. P.Bt.
n Society of HumanGeneenetics and Genomics, N
016/j.ajog.2014.08.006
NOVEMBER 2014 Ameri
publications on methodologies, val-idation, and test performance,2-14 alldemonstrating improved sensitivities
ontefiore Medical Center, Albert Einstein Collegenn, Hill, Sigurjonsson, Ryan, Banjevic, andi, Ms Koch, and Dr Strom), CA; and Division ofth Center, Farmington, CT (Dr Benn).
. P.D. participated in a multicenter clinical trial
. is a paid consultant and member of an advisory
tics, Milan, Italy, May 31-June 3, 2014, and at theashville, TN, March 25-29, 2014.
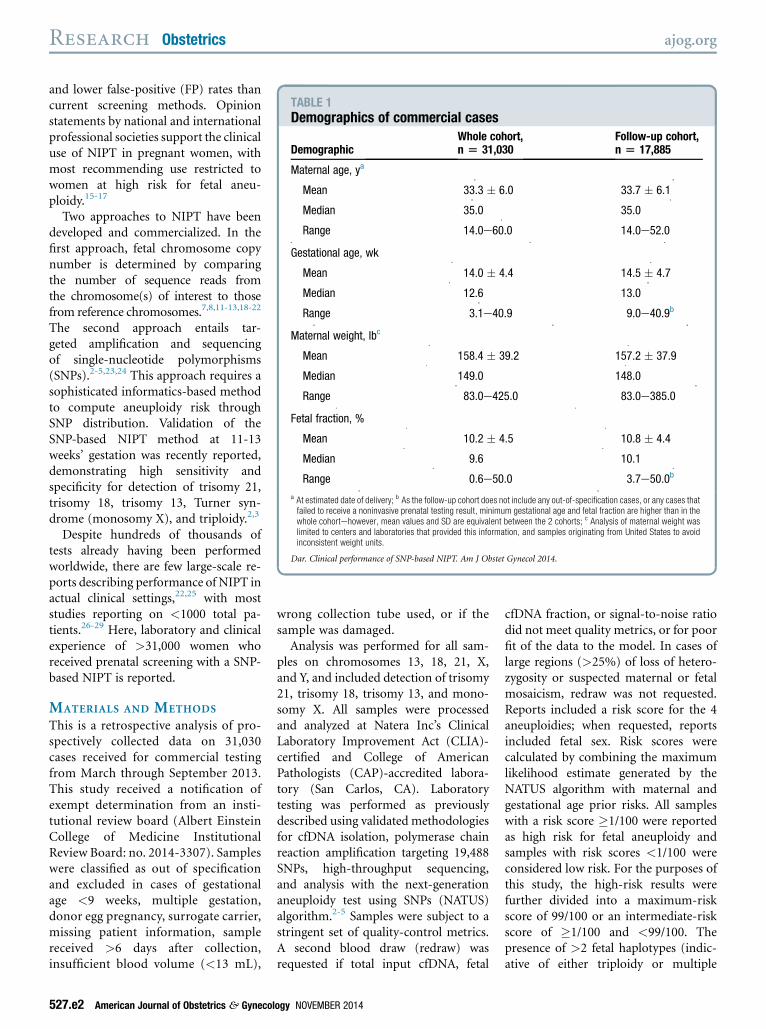
a At estimated date of delivery; b As the follow-up cohort does not include any out-of-specification cases, or any cases thatfailed to receive a noninvasive prenatal testing result, minimum gestational age and fetal fraction are higher than in thewhole cohortehowever, mean values and SD are equivalent between the 2 cohorts; c Analysis of maternal weight waslimited to centers and laboratories that provided this information, and samples originating from United States to avoidinconsistent weight units.
Dar. Clinical performance of SNP-based NIPT. Am J Obstet Gynecol 2014.
Research Obstetrics ajog.org
and lower false-positive (FP) rates thancurrent screening methods. Opinionstatements by national and internationalprofessional societies support the clinicaluse of NIPT in pregnant women, withmost recommending use restricted towomen at high risk for fetal aneu-ploidy.15-17
Two approaches to NIPT have beendeveloped and commercialized. In thefirst approach, fetal chromosome copynumber is determined by comparingthe number of sequence reads fromthe chromosome(s) of interest to thosefrom reference chromosomes.7,8,11-13,18-22
The second approach entails tar-geted amplification and sequencingof single-nucleotide polymorphisms(SNPs).2-5,23,24 This approach requires asophisticated informatics-based methodto compute aneuploidy risk throughSNP distribution. Validation of theSNP-based NIPT method at 11-13weeks’ gestation was recently reported,demonstrating high sensitivity andspecificity for detection of trisomy 21,trisomy 18, trisomy 13, Turner syn-drome (monosomy X), and triploidy.2,3
Despite hundreds of thousands oftests already having been performedworldwide, there are few large-scale re-ports describing performance of NIPT inactual clinical settings,22,25 with moststudies reporting on <1000 total pa-tients.26-29 Here, laboratory and clinicalexperience of >31,000 women whoreceived prenatal screening with a SNP-based NIPT is reported.
MATERIALS AND METHODS
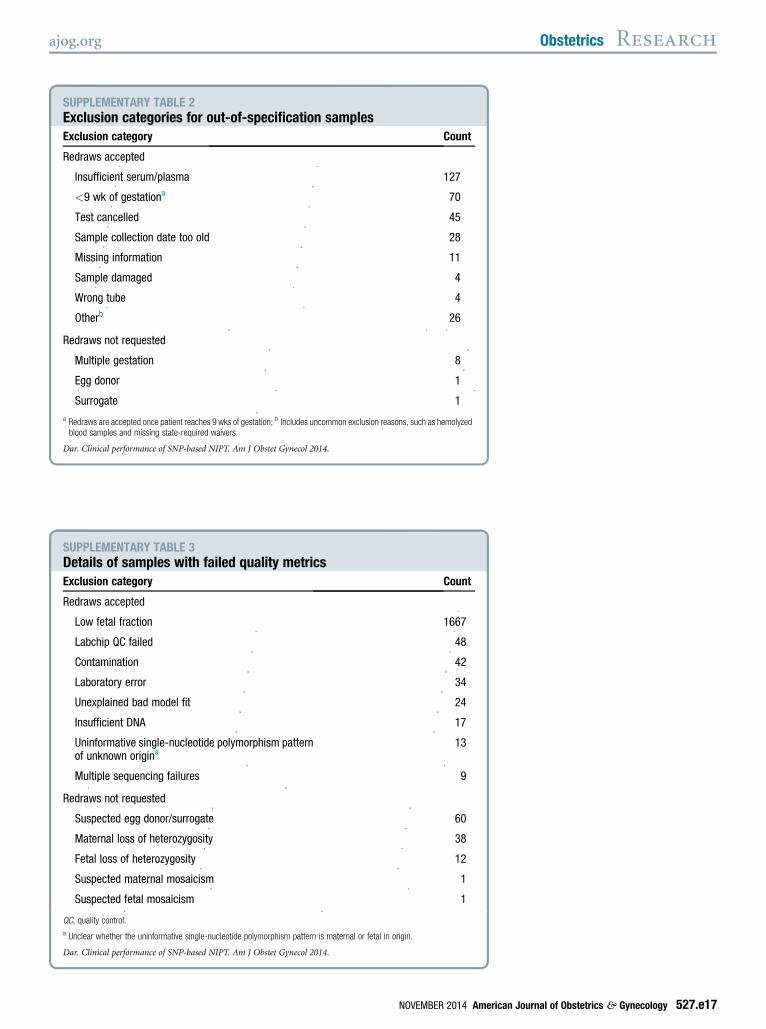
This is a retrospective analysis of pro-spectively collected data on 31,030cases received for commercial testingfrom March through September 2013.This study received a notification ofexempt determination from an insti-tutional review board (Albert EinsteinCollege of Medicine InstitutionalReview Board: no. 2014-3307). Sampleswere classified as out of specificationand excluded in cases of gestationalage <9 weeks, multiple gestation,donor egg pregnancy, surrogate carrier,missing patient information, samplereceived >6 days after collection,insufficient blood volume (<13 mL),
527.e2 American Journal of Obstetrics & Gynecol
wrong collection tube used, or if thesample was damaged.Analysis was performed for all sam-
ples on chromosomes 13, 18, 21, X,and Y, and included detection of trisomy21, trisomy 18, trisomy 13, and mono-somy X. All samples were processedand analyzed at Natera Inc’s ClinicalLaboratory Improvement Act (CLIA)-certified and College of AmericanPathologists (CAP)-accredited labora-tory (San Carlos, CA). Laboratorytesting was performed as previouslydescribed using validated methodologiesfor cfDNA isolation, polymerase chainreaction amplification targeting 19,488SNPs, high-throughput sequencing,and analysis with the next-generationaneuploidy test using SNPs (NATUS)algorithm.2-5 Samples were subject to astringent set of quality-control metrics.A second blood draw (redraw) wasrequested if total input cfDNA, fetal
ogy NOVEMBER 2014
cfDNA fraction, or signal-to-noise ratiodid not meet quality metrics, or for poorfit of the data to the model. In cases oflarge regions (>25%) of loss of hetero-zygosity or suspected maternal or fetalmosaicism, redraw was not requested.Reports included a risk score for the 4aneuploidies; when requested, reportsincluded fetal sex. Risk scores werecalculated by combining the maximumlikelihood estimate generated by theNATUS algorithm with maternal andgestational age prior risks. All sampleswith a risk score �1/100 were reportedas high risk for fetal aneuploidy andsamples with risk scores <1/100 wereconsidered low risk. For the purposes ofthis study, the high-risk results werefurther divided into a maximum-riskscore of 99/100 or an intermediate-riskscore of �1/100 and <99/100. Thepresence of >2 fetal haplotypes (indic-ative of either triploidy or multiple
Dar. Clinical performance of SNP-based NIPT. Am J ObstetGynecol 2014.
FIGURE 2Father sample and clinicallaboratory experience reducesredraw rate
3%
4%
5%
6%
7%
8%
9%
Mar-May June-July August September
Perc
ent o
f sam
ples
Overall
With Father
Decrease in redraw rates overall and for patients
including a paternal sample during the reporting
period (March through September 2013) for
samples �10 weeks of gestation.
Dar. Clinical performance of SNP-based NIPT. Am J ObstetGynecol 2014.
ajog.org Obstetrics Research
gestation) was reported only when theconfidence was >99.9%. Additional sexchromosome aneuploidies (XXX, XXY,and XYY) were reported from June 2013.The following patient characteristicswere requested for each sample:maternal date of birth, maternal weight,gestational age, and whether a paternalsample was included.
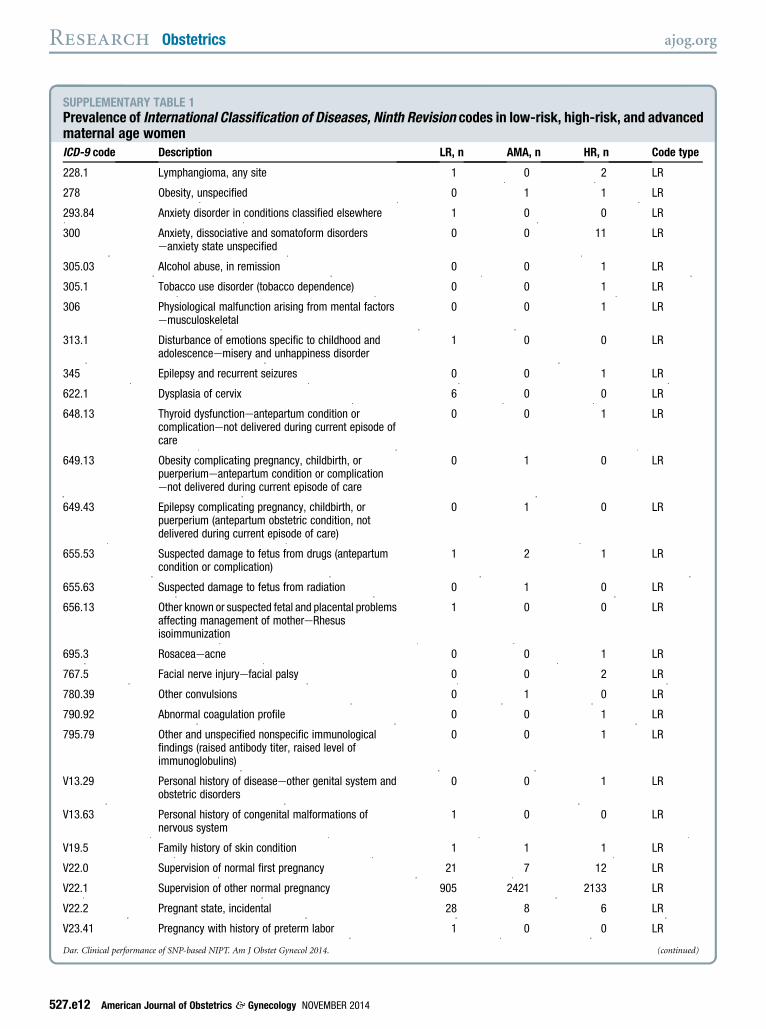
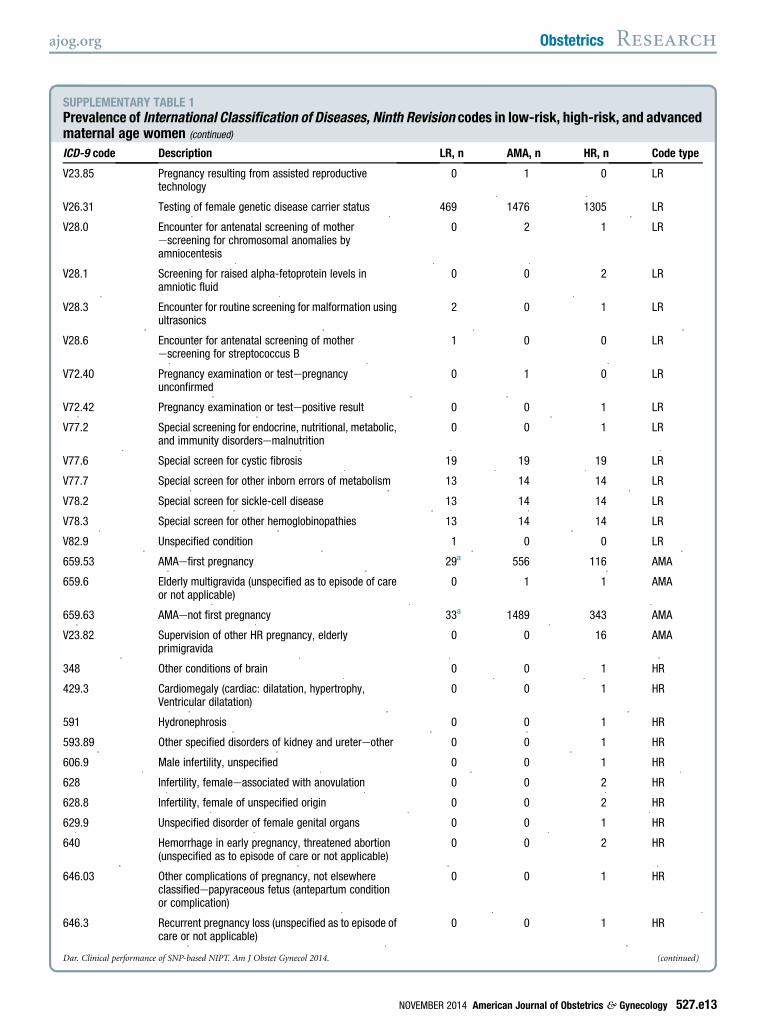
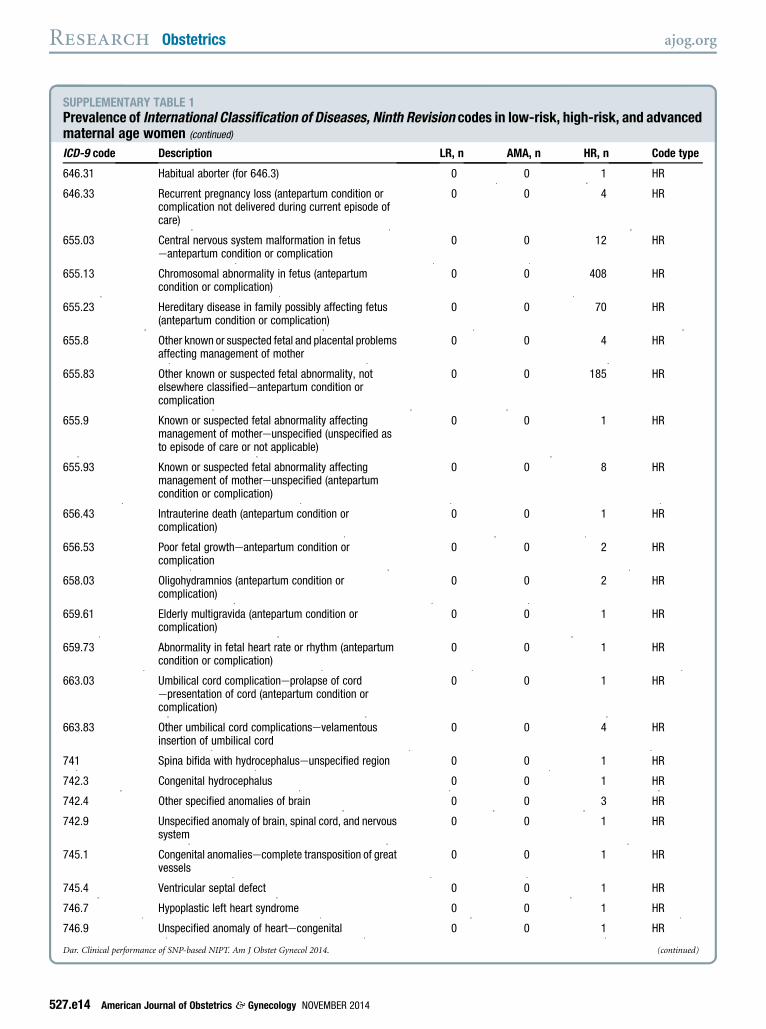
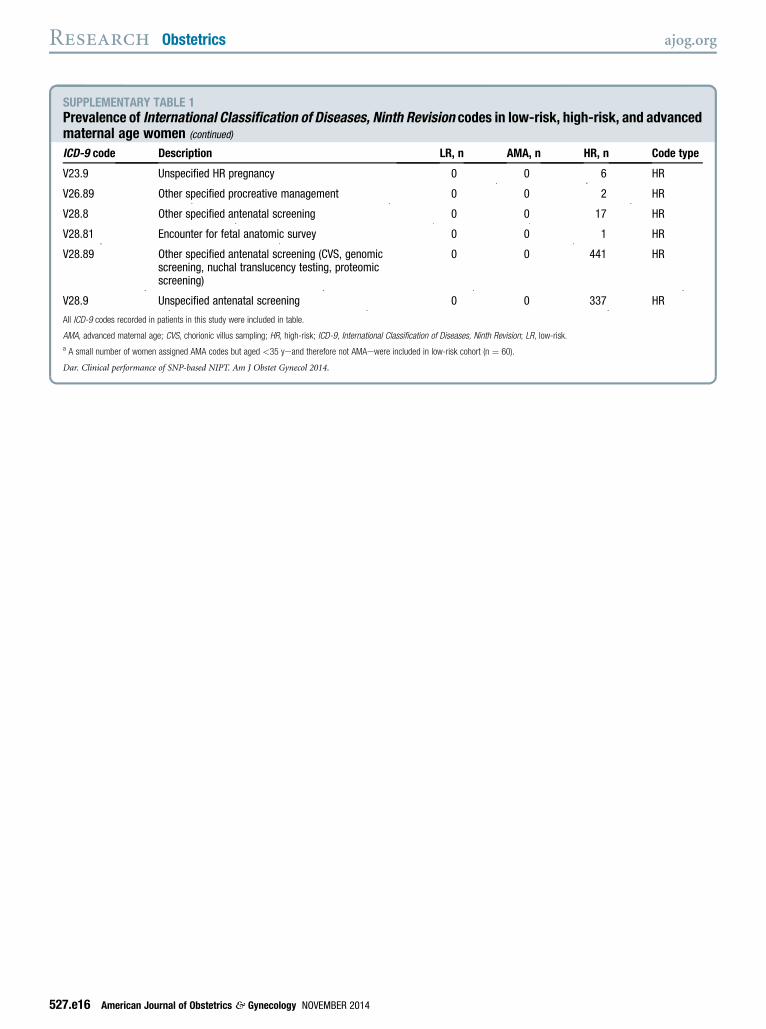
Patients with available InternationalClassification of Diseases, Ninth Revision(ICD-9) codes (Appendix; SupplementaryTable 1) were categorized into 3 sub-cohorts: (1) “low risk” if aged <35 yearsand no aneuploidy-related high-riskcodes; (2) “at risk” for fetal aneuploidybased solely onmaternal age�35 years; or(3) “high risk” for fetal aneuploidy byICD-9 code, regardless of maternal age.High-risk indications included positivescreening tests, ultrasound anomalies, andrelevant family history. Patients withoutreported ICD-9 codes were categorized bymaternal age as low risk (<35 years) orhigh risk (�35 years).
Follow-up information on high-riskresults was obtained by telephone andrecorded in an internal database. Clinicalfollow-up was completed on June 14,2014, at which time all pregnancies werecompleted. Two partner laboratories
accounting for 38.1% of the total 31,030cases were responsible for their ownfollow-up efforts and were excludedfrom outcome calculations. Providerswere encouraged to share informationabout false-negative (FN) results. Sam-ples were categorized as follows: (1)“true positive” (TP) included high-risksamples that were confirmed by prena-tal or postnatal diagnostic testing, orbased on clinical evaluation at birth; (2)“FP” included high-risk samples thatwere shown to be euploid by follow-uptesting or based on clinical evaluationat birth; (3) “suggestive” included sam-ples where prenatal ultrasound detectedat least 1 structural anomaly and 1 softsonographic marker consistent withNIPT findings, but karyotype confir-mationwas not obtained; (4) “pregnancyloss” where the patient experiencedspontaneous abortion and karyotypeconfirmation was not obtained; (5)“termination” where the patient electedto end the pregnancy without karyotypeconfirmation; (6) “no follow-up”included samples where informationwasunavailable; and (7) “FN” includedNIPT low-risk samples that were re-ported as aneuploid by the provider.When placental and fetal karyotypeswere both available and determined to bediscordant, NIPT findings were consid-ered TP if they matched the fetal kar-yotype, and FP if they did not match thefetal karyotype. Pregnancies wereconsidered mosaic when chromosomeanalysis revealed either placental or fetalmosaicism or there was discordance be-tween placental and fetal karyotypes.Patient and sample characteristics
were expressed as means, SD, medians,and ranges. Linear regression analysiswas used to determine the relationshipbetween fetal fraction and gestationalage, between fetal fraction and maternalweight, and between fetal/maternalcfDNA and maternal weight; a recip-rocal model was used when determiningthe relationship between fetal fractionand gestational age or maternal weight.For comparison of euploid and aneu-ploid calls, fetal fractions were expressedas multiples of the median (MoM)relative to low-risk calls weightedby week of gestation, and significance
NOVEMBER 2014 Ameri
determined using aMann-Whitney ranksum test. The 2 FN results were includedin the appropriate aneuploid category,and FP calls were excluded from aneu-ploidy fetal fraction analyses. Thebenefit of a paternal sample on redrawrates and differences in aneuploidyincidence between the a priori riskgroups were determined using a c2 test.The Kruskal-Wallis 1-way analysis ofvariance on ranks test was used to eval-uate maternal age and gestational agedifferences for the different risk groups.Positive predictive value (PPV) ([TP]/[TPþ FP]) was calculated for cases withknown cytogenetic analyses. SigmaPlot12.5 (Systat Software, San Jose, CA) wasused for all statistical analyses. P < .05was considered statistically significant.
RESULTS
Patients and samplesPatient and sample characteristics for the31,030 cases received during the studyperiod are detailed in Table 1. Meanmaternal age was 33.3 years, with 51.4%(15,952) aged�35 years at the estimateddate of delivery. Mean gestational agewas 14.0 weeks, with 64.5% (20,001) ofsamples drawn in first trimester and33.8% (10,479) in the second trimester.
Figure 1 depicts the study flowchart. Samples from 325 (1.0%) patientswere excluded as being outside of the
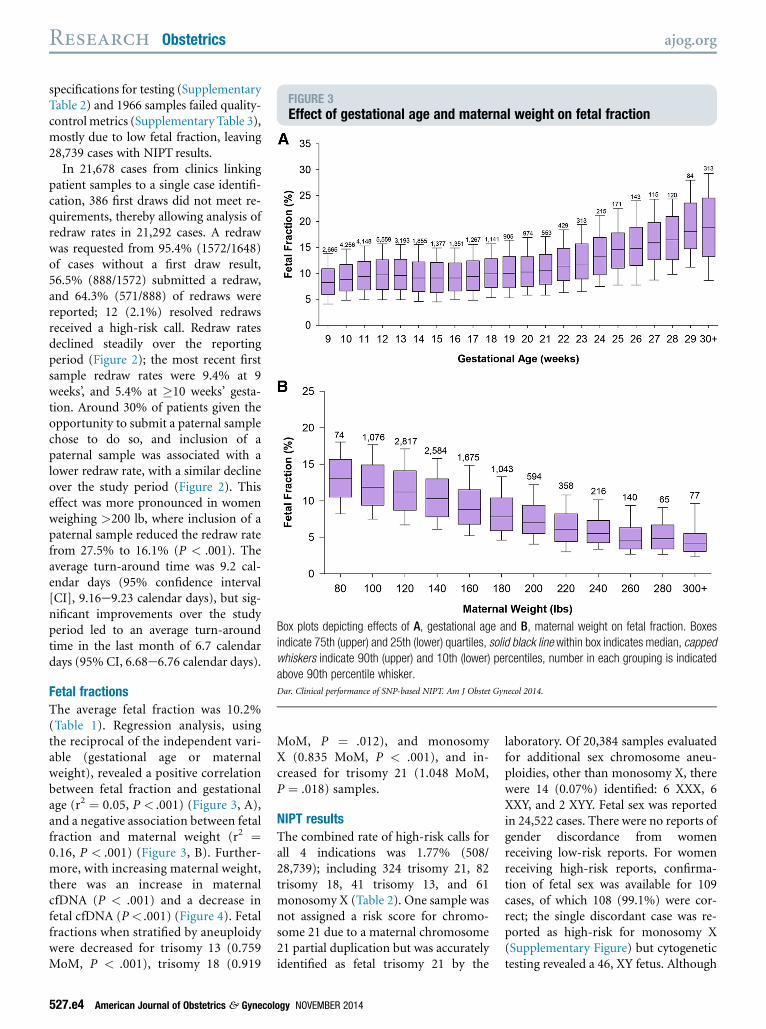
FIGURE 3Effect of gestational age and maternal weight on fetal fraction
Box plots depicting effects of A, gestational age and B, maternal weight on fetal fraction. Boxes
indicate 75th (upper) and 25th (lower) quartiles, solid black line within box indicates median, capped
whiskers indicate 90th (upper) and 10th (lower) percentiles, number in each grouping is indicated
above 90th percentile whisker.
Dar. Clinical performance of SNP-based NIPT. Am J Obstet Gynecol 2014.
Research Obstetrics ajog.org
specifications for testing (SupplementaryTable 2) and 1966 samples failed quality-controlmetrics (Supplementary Table 3),mostly due to low fetal fraction, leaving28,739 cases with NIPT results.
In 21,678 cases from clinics linkingpatient samples to a single case identifi-cation, 386 first draws did not meet re-quirements, thereby allowing analysis ofredraw rates in 21,292 cases. A redrawwas requested from 95.4% (1572/1648)of cases without a first draw result,56.5% (888/1572) submitted a redraw,and 64.3% (571/888) of redraws werereported; 12 (2.1%) resolved redrawsreceived a high-risk call. Redraw ratesdeclined steadily over the reportingperiod (Figure 2); the most recent firstsample redraw rates were 9.4% at 9weeks’, and 5.4% at �10 weeks’ gesta-tion. Around 30% of patients given theopportunity to submit a paternal samplechose to do so, and inclusion of apaternal sample was associated with alower redraw rate, with a similar declineover the study period (Figure 2). Thiseffect was more pronounced in womenweighing >200 lb, where inclusion of apaternal sample reduced the redraw ratefrom 27.5% to 16.1% (P < .001). Theaverage turn-around time was 9.2 cal-endar days (95% confidence interval[CI], 9.16e9.23 calendar days), but sig-nificant improvements over the studyperiod led to an average turn-aroundtime in the last month of 6.7 calendardays (95% CI, 6.68e6.76 calendar days).
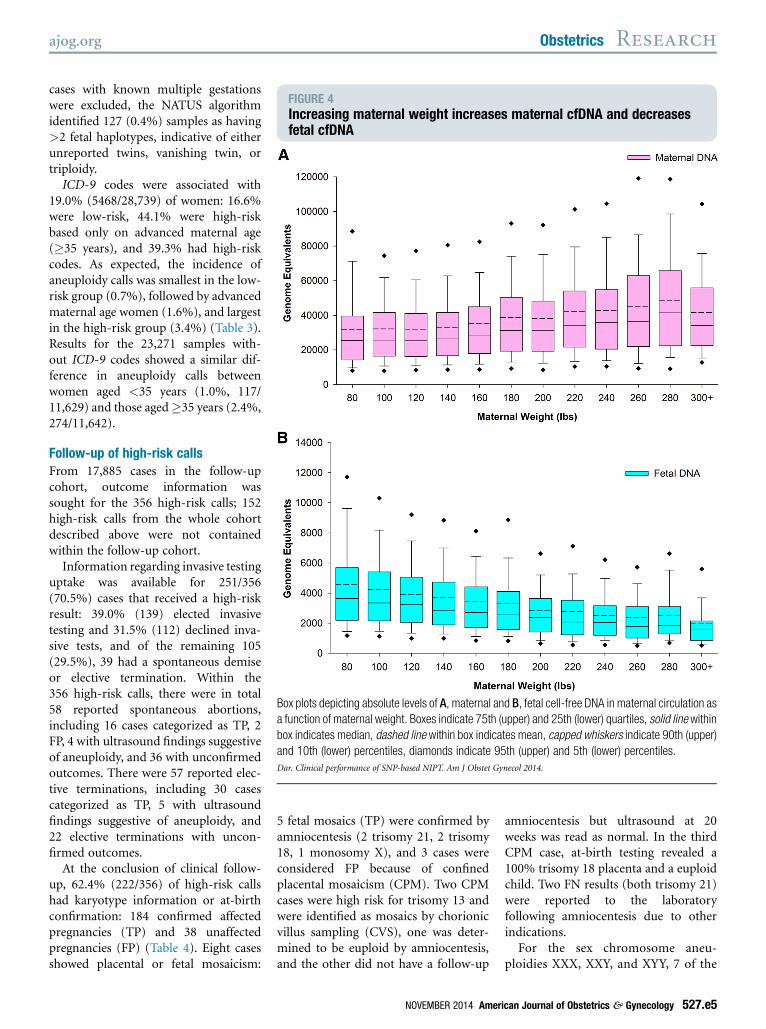
Fetal fractionsThe average fetal fraction was 10.2%(Table 1). Regression analysis, usingthe reciprocal of the independent vari-able (gestational age or maternalweight), revealed a positive correlationbetween fetal fraction and gestationalage (r2 ¼ 0.05, P < .001) (Figure 3, A),and a negative association between fetalfraction and maternal weight (r2 ¼0.16, P < .001) (Figure 3, B). Further-more, with increasing maternal weight,there was an increase in maternalcfDNA (P < .001) and a decrease infetal cfDNA (P < .001) (Figure 4). Fetalfractions when stratified by aneuploidywere decreased for trisomy 13 (0.759MoM, P < .001), trisomy 18 (0.919
527.e4 American Journal of Obstetrics & Gynecol
MoM, P ¼ .012), and monosomyX (0.835 MoM, P < .001), and in-creased for trisomy 21 (1.048 MoM,P ¼ .018) samples.
NIPT resultsThe combined rate of high-risk calls forall 4 indications was 1.77% (508/28,739); including 324 trisomy 21, 82trisomy 18, 41 trisomy 13, and 61monosomy X (Table 2). One sample wasnot assigned a risk score for chromo-some 21 due to a maternal chromosome21 partial duplication but was accuratelyidentified as fetal trisomy 21 by the
ogy NOVEMBER 2014
laboratory. Of 20,384 samples evaluatedfor additional sex chromosome aneu-ploidies, other than monosomy X, therewere 14 (0.07%) identified: 6 XXX, 6XXY, and 2 XYY. Fetal sex was reportedin 24,522 cases. There were no reports ofgender discordance from womenreceiving low-risk reports. For womenreceiving high-risk reports, confirma-tion of fetal sex was available for 109cases, of which 108 (99.1%) were cor-rect; the single discordant case was re-ported as high-risk for monosomy X(Supplementary Figure) but cytogenetictesting revealed a 46, XY fetus. Although
FIGURE 4Increasing maternal weight increases maternal cfDNA and decreasesfetal cfDNA
Box plots depicting absolute levels of A, maternal and B, fetal cell-free DNA in maternal circulation asa function of maternal weight. Boxes indicate 75th (upper) and 25th (lower) quartiles, solid line within
box indicates median, dashed line within box indicates mean, capped whiskers indicate 90th (upper)
and 10th (lower) percentiles, diamonds indicate 95th (upper) and 5th (lower) percentiles.
Dar. Clinical performance of SNP-based NIPT. Am J Obstet Gynecol 2014.
ajog.org Obstetrics Research
cases with known multiple gestationswere excluded, the NATUS algorithmidentified 127 (0.4%) samples as having>2 fetal haplotypes, indicative of eitherunreported twins, vanishing twin, ortriploidy.
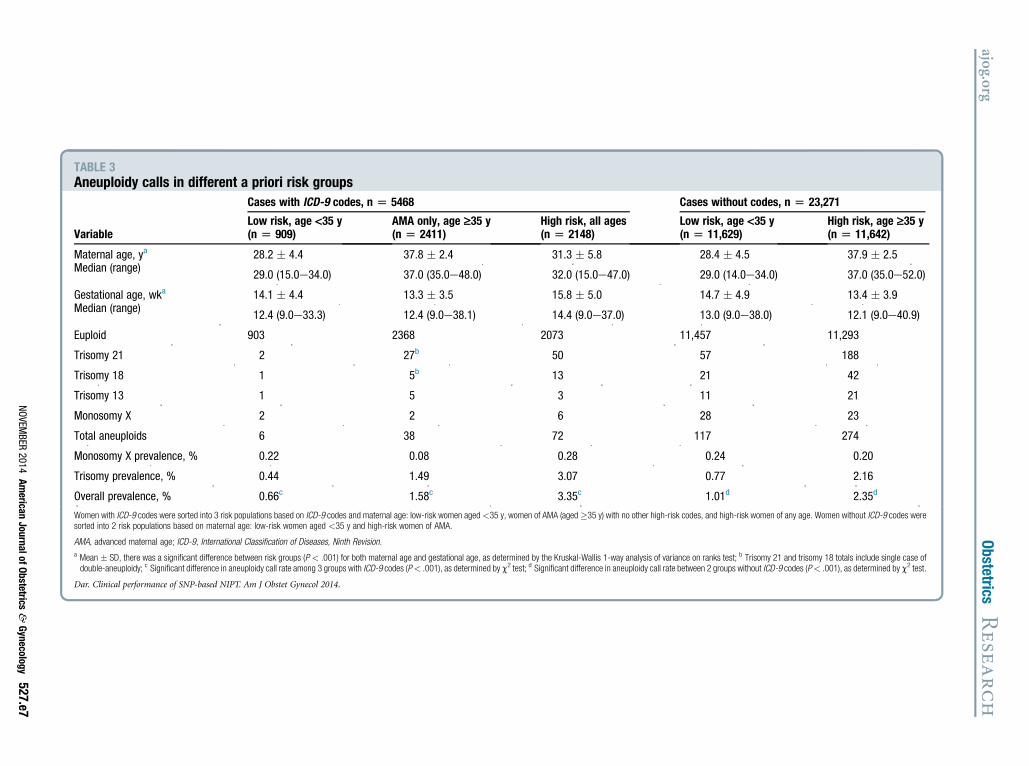
ICD-9 codes were associated with19.0% (5468/28,739) of women: 16.6%were low-risk, 44.1% were high-riskbased only on advanced maternal age(�35 years), and 39.3% had high-riskcodes. As expected, the incidence ofaneuploidy calls was smallest in the low-risk group (0.7%), followed by advancedmaternal age women (1.6%), and largestin the high-risk group (3.4%) (Table 3).Results for the 23,271 samples with-out ICD-9 codes showed a similar dif-ference in aneuploidy calls betweenwomen aged <35 years (1.0%, 117/11,629) and those aged�35 years (2.4%,274/11,642).
Follow-up of high-risk callsFrom 17,885 cases in the follow-upcohort, outcome information wassought for the 356 high-risk calls; 152high-risk calls from the whole cohortdescribed above were not containedwithin the follow-up cohort.
Information regarding invasive testinguptake was available for 251/356(70.5%) cases that received a high-riskresult: 39.0% (139) elected invasivetesting and 31.5% (112) declined inva-sive tests, and of the remaining 105(29.5%), 39 had a spontaneous demiseor elective termination. Within the356 high-risk calls, there were in total58 reported spontaneous abortions,including 16 cases categorized as TP, 2FP, 4 with ultrasound findings suggestiveof aneuploidy, and 36 with unconfirmedoutcomes. There were 57 reported elec-tive terminations, including 30 casescategorized as TP, 5 with ultrasoundfindings suggestive of aneuploidy, and22 elective terminations with uncon-firmed outcomes.
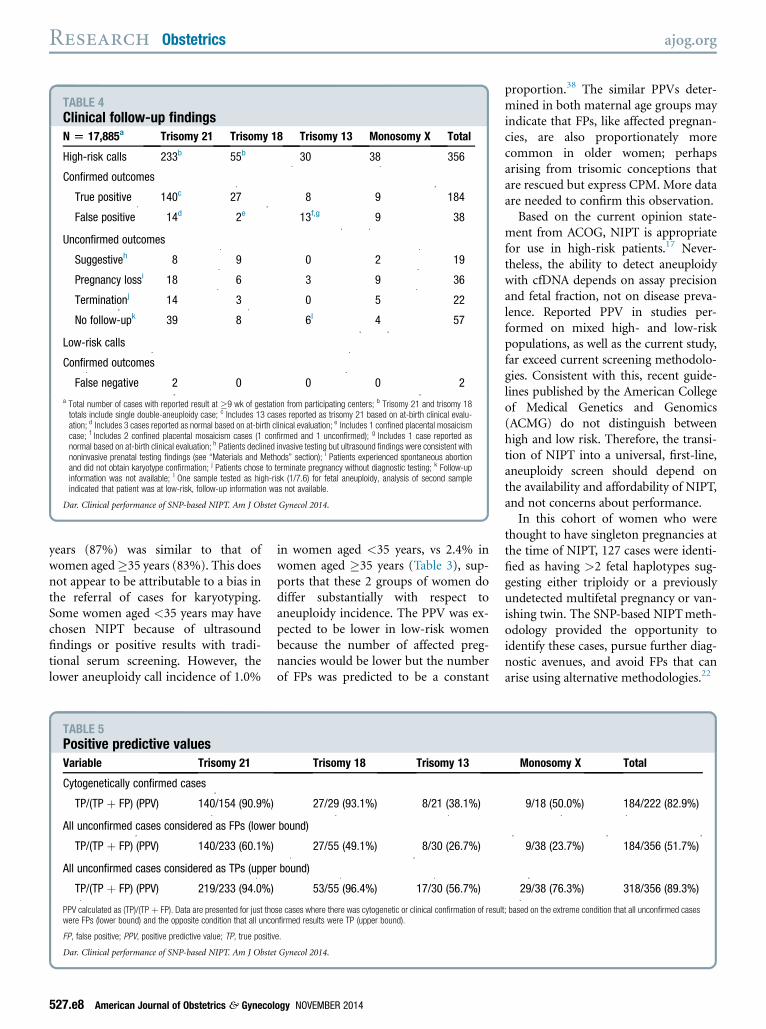
At the conclusion of clinical follow-up, 62.4% (222/356) of high-risk callshad karyotype information or at-birthconfirmation: 184 confirmed affectedpregnancies (TP) and 38 unaffectedpregnancies (FP) (Table 4). Eight casesshowed placental or fetal mosaicism:
5 fetal mosaics (TP) were confirmed byamniocentesis (2 trisomy 21, 2 trisomy18, 1 monosomy X), and 3 cases wereconsidered FP because of confinedplacental mosaicism (CPM). Two CPMcases were high risk for trisomy 13 andwere identified as mosaics by chorionicvillus sampling (CVS), one was deter-mined to be euploid by amniocentesis,and the other did not have a follow-up
NOVEMBER 2014 Ameri
amniocentesis but ultrasound at 20weeks was read as normal. In the thirdCPM case, at-birth testing revealed a100% trisomy 18 placenta and a euploidchild. Two FN results (both trisomy 21)were reported to the laboratoryfollowing amniocentesis due to otherindications.
For the sex chromosome aneu-ploidies XXX, XXY, and XYY, 7 of the
TABLE 2Number of fetal aneuploidy high-risk calls in reported commercial casesAll cases, N [ 28,739a Trisomy 21 Trisomy 18 Trisomy 13 Monosomy X
Risk �99/100 298b 78b 26 53
1/100 � Risk <99/100 25 4 15 8
Total 324b,c 82b 41 61
Prevalence, 1 in: 88 349 697 467a Total number of cases with reported result at�9 wk of gestation; b Trisomy 21 and trisomy 18 totals include a single case ofdouble-aneuploidy; c Includes 1 case with a detected partial maternal chromosome 21 duplication, the fetus was determinedto be high risk for trisomy 21 but the algorithm did not calculate a risk score.
Dar. Clinical performance of SNP-based NIPT. Am J Obstet Gynecol 2014.
Research Obstetrics ajog.org
14 high-risk calls were within thefollow-up cohort. Clinical follow-uprevealed 4 cases with known out-comes: 2 TP (1 XXX, 1 XXY) and 2 FP(both XXX).
Based on the cases with cytoge-netic confirmation, women with anintermediate-risk score were morelikely to have a FP result (19/24, 79.2%)than women with a maximum-riskscore (19/198, 9.6%, P < .001). Forthe 36 cases that experienced sponta-neous abortion and did not obtainkaryotype confirmation, 33 (91.7%)had a maximum-risk score. All 22patients who elected to terminate thepregnancy without confirmation had amaximal-risk score.
Positive predictive valueBased only on cases with cytogeneticdiagnosis (Table 4), the PPV was90.9% for trisomy 21 and 82.9% for all 4cytogenetic abnormalities combined(Table 5). A theoretical PPV was alsocalculated under the 2 boundary condi-tions that all unconfirmed high-riskcases were either FP or TP (Table 5).This provided a range for the PPV of60-94% for trisomy 21 and 52-89% forall abnormalities combined.
Among women without ICD-9-codedindications, 63 women aged <35 yearsreceived high-risk calls, of which 39(60.9%) had diagnostic testing and34 were TP, a PPV of 87.2% (95% CI,72.6e95.7%). Of 176 women �35 yearswith high-risk calls, 105 (59.7%) hadconfirmatory karyotyping and 87wereTP,a PPVof 82.9% (95% CI, 74.3e89.5%).
COMMENT
This report of initial clinical experiencewith this SNP-based NIPT in >31,000pregnancies demonstrates that perfor-mance in clinical settings is consistentwith validation studies.2-5 Using onlycases confirmed through chromosomeanalysis or clinical evaluation at birth,the PPV in this mixed low- and high-riskpopulation is 90.9% for trisomy 21 and82.9% for all 4 aneuploidies, which is farbetter than current screening methods.Even under the highly conservativeassumption that all unconfirmed high-risk cases are incorrect, this test still
527.e6 American Journal of Obstetrics & Gynecol
offers improved clinical performanceover traditional screening.The main advantage of this study is
the robust information it provides onclinical application of NIPT, which cancontribute to, and improve, both testperformance and counseling of patients.Fetal fraction, the main variable that af-fects redraw rates, is positively correlatedwith gestational age and negativelycorrelated with maternal weight,agreeing with previous studies.30-33
There are 2 main clinical implicationsfrom these findings. First, adequatedating will lower the need for redraw,particularly at early gestational ages.Second, inclusion of a paternal bloodsample significantly lowers redraw ratesand should be offered to patients,particularly those >200 lb. Importantly,cases with extremely low fetal fraction,which typically do not resolve withredraw, may have an increased risk forfetal aneuploidy.2 This is likely particu-larly important for maternal triploidy,which is associated with smaller pla-centas and lower fetal fractions,2,5 andtrisomy 13 and trisomy 18 pregnancies.In addition to determining the most
likely ploidy state of a fetus, the NATUSalgorithm also generates a chromosome-specific risk score, which is a measure ofthe probability of nonmosaic fetalaneuploidy. As expected, data showedthat maximum-risk results are morelikely to be TP than intermediate-riskresults. Although a high-risk score ap-pears to bemore indicative of a TP result,individual numerical values should beinterpreted cautiously. Regardless of therisk score, confirmatory studies must beoffered to all womenwith positive results
ogy NOVEMBER 2014
without exception. This is particularlyimportant in light of the finding herethat 6.2% of women with high-risk re-sults chose to terminate the pregnancywithout invasive test confirmation.
Although referred to as fetal cfDNA,the primary source of cfDNA is placentaltrophoblast cells.34 CPM, estimated to bepresent in 1-2% of 10- to 12-week ges-tations,35,36 impacts all NIPTs. Valida-tion studies have typically excludedsamples with fetal mosaicism or CPM.Yet, it is clear that when NIPT is per-formed in a clinical setting, the effect ofmosaicism cannot be ignored, and itsimpact on FP and FN results should beaddressed. In this cohort, 8/222 (3.6%)high-risk calls showed evidence ofmosaicism. Two cases with CVS resultsthat supported NIPT findings were latercategorized as FPs because of CPM.Further, since most FPs in this cohortwere determined by amniocentesis or at-birth testing without placental geneticanalysis, there may be additional, unde-tected CPM cases within the FPs. From aretrospective analysis of CVS, Gratiet al37 estimated that the FP rate wouldbe 0.08% for the 4 common aneu-ploidies. Our findings, combined withthe known incidence of CPM-relatedFPs and FNs, further reinforce the needfor adequate pretest counseling, as rec-ommended by American Congress ofObstetrics and Gynecology (ACOG).17
Patients undergoing CVS followinghigh-risk results with NIPT should becounseled that mosaic conditions canoccur and later amniocentesis may berequired.
An unexpected finding in this studywas that the PPV for women aged <35
Women with ICD-9 codes were sorted into 3 risk populations based on ICD-9 codes and maternal age: low-risk women aged<35 y, women of AMA (aged�35 y) with no other high-risk codes, and high-risk women of any age. Women without ICD-9 codes weresorted into 2 risk populations based on maternal age: low-risk women aged <35 y and high-risk women of AMA.
AMA, advanced maternal age; ICD-9, International Classification of Diseases, Ninth Revision.
a Mean � SD, there was a significant difference between risk groups (P < .001) for both maternal age and gestational age, as determined by the Kruskal-Wallis 1-way analysis of variance on ranks test; b Trisomy 21 and trisomy 18 totals include single case ofdouble-aneuploidy; c Significant difference in aneuploidy call rate among 3 groups with ICD-9 codes (P< .001), as determined by c2 test; d Significant difference in aneuploidy call rate between 2 groups without ICD-9 codes (P< .001), as determined by c2 test.
Dar. Clinical performance of SNP-based NIPT. Am J Obstet Gynecol 2014.
TABLE 4Clinical follow-up findingsN [ 17,885a Trisomy 21 Trisomy 18 Trisomy 13 Monosomy X Total
High-risk calls 233b 55b 30 38 356
Confirmed outcomes
True positive 140c 27 8 9 184
False positive 14d 2e 13f,g 9 38
Unconfirmed outcomes
Suggestiveh 8 9 0 2 19
Pregnancy lossi 18 6 3 9 36
Terminationj 14 3 0 5 22
No follow-upk 39 8 6l 4 57
Low-risk calls
Confirmed outcomes
False negative 2 0 0 0 2
a Total number of cases with reported result at �9 wk of gestation from participating centers; b Trisomy 21 and trisomy 18totals include single double-aneuploidy case; c Includes 13 cases reported as trisomy 21 based on at-birth clinical evalu-ation; d Includes 3 cases reported as normal based on at-birth clinical evaluation; e Includes 1 confined placental mosaicismcase; f Includes 2 confined placental mosaicism cases (1 confirmed and 1 unconfirmed); g Includes 1 case reported asnormal based on at-birth clinical evaluation; h Patients declined invasive testing but ultrasound findings were consistent withnoninvasive prenatal testing findings (see “Materials and Methods” section); i Patients experienced spontaneous abortionand did not obtain karyotype confirmation; j Patients chose to terminate pregnancy without diagnostic testing; k Follow-upinformation was not available; l One sample tested as high-risk (1/7.6) for fetal aneuploidy, analysis of second sampleindicated that patient was at low-risk, follow-up information was not available.
Dar. Clinical performance of SNP-based NIPT. Am J Obstet Gynecol 2014.
Research Obstetrics ajog.org
years (87%) was similar to that ofwomen aged�35 years (83%). This doesnot appear to be attributable to a bias inthe referral of cases for karyotyping.Some women aged <35 years may havechosen NIPT because of ultrasoundfindings or positive results with tradi-tional serum screening. However, thelower aneuploidy call incidence of 1.0%
Dar. Clinical performance of SNP-based NIPT. Am J Obste
527.e8 American Journal of Obstetrics & Gynecol
in women aged <35 years, vs 2.4% inwomen aged �35 years (Table 3), sup-ports that these 2 groups of women dodiffer substantially with respect toaneuploidy incidence. The PPV was ex-pected to be lower in low-risk womenbecause the number of affected preg-nancies would be lower but the numberof FPs was predicted to be a constant
Trisomy 18 Trisomy 13
27/29 (93.1%) 8/21 (38.1%)
bound)
27/55 (49.1%) 8/30 (26.7%)
r bound)
53/55 (96.4%) 17/30 (56.7%)
se cases where there was cytogenetic or clinical confirmation of resulnfirmed results were TP (upper bound).
e.
t Gynecol 2014.
ogy NOVEMBER 2014
proportion.38 The similar PPVs deter-mined in both maternal age groups mayindicate that FPs, like affected pregnan-cies, are also proportionately morecommon in older women; perhapsarising from trisomic conceptions thatare rescued but express CPM. More dataare needed to confirm this observation.
Based on the current opinion state-ment from ACOG, NIPT is appropriatefor use in high-risk patients.17 Never-theless, the ability to detect aneuploidywith cfDNA depends on assay precisionand fetal fraction, not on disease preva-lence. Reported PPV in studies per-formed on mixed high- and low-riskpopulations, as well as the current study,far exceed current screening methodolo-gies. Consistent with this, recent guide-lines published by the American Collegeof Medical Genetics and Genomics(ACMG) do not distinguish betweenhigh and low risk. Therefore, the transi-tion of NIPT into a universal, first-line,aneuploidy screen should depend onthe availability and affordability of NIPT,and not concerns about performance.
In this cohort of women who werethought to have singleton pregnancies atthe time of NIPT, 127 cases were identi-fied as having >2 fetal haplotypes sug-gesting either triploidy or a previouslyundetected multifetal pregnancy or van-ishing twin. The SNP-based NIPTmeth-odology provided the opportunity toidentify these cases, pursue further diag-nostic avenues, and avoid FPs that canarise using alternative methodologies.22
Monosomy X Total
9/18 (50.0%) 184/222 (82.9%)
9/38 (23.7%) 184/356 (51.7%)
29/38 (76.3%) 318/356 (89.3%)
t; based on the extreme condition that all unconfirmed cases
The main limitation of this study isthe incomplete follow-up data, partic-ularly on low-risk patients, precludingprecise calculation of sensitivity andspecificity. While follow-up was notconducted on low-risk patients, giventhe clinical significance of a FN report,and based on our laboratory experi-ence, it is likely that FNs would bevoluntarily reported; there were 2voluntarily reported FNs. However, thelack of comprehensive follow-up on alllow-risk patients precluded determi-nation of the negative predictive value.Nevertheless, it is important to notethat strong performance characteristicswere in keeping with prior validationstudies,2,3,24 even with the inclusion ofmosaic samples. Follow-up of normalresults remains an issue for all labora-tories that wish to track results forquality assurance, and we support theACMG recommendation for a nationalregistry.16
In conclusion, this is a large-scalereport of clinical utilization of NIPT.Analysis of >31,000 samples from bothlow- and high-risk women supportedthat test performance of this NIPTmethod in a clinical setting mirrors therobust performance reported in valida-tion studies.
Clinical performance of SNP-basedNIPT in a mixed high- and low-riskpopulation is consistent with perfor-mance in validation studies. SimilarPPVs were found in women aged <35years and aged �35 years. The strengthof the study is the robust information itprovides on clinical application of NIPT.The primary limitation is the incompletefollow-up data, particularly on low-riskpatients, precluding precise calculationof sensitivity and specificity.
This study supports the use of NIPTas a first-line screening test for aneu-ploidy in all patients. Furthermore, ithighlights the importance of, as well asprovides data that can improve, coun-seling of patients. Finally, the results ofthis study raise the questions of howmany FP results may be explained byCPM and how best to manage clinicalcare and diagnostic confirmation ofhigh-risk NIPT results in light of po-tential CPM. The extent to which CPM
may underlie NIPT FP results requiresfurther investigation. -
ACKNOWLEDGMENTS
We would like to thank Steven Aldridge and NiaSengupta for assistance with collecting andtracking follow-up information. We would alsolike to thank Dr AsimSiddiqui for critical review ofthe manuscript. N.S. and A.S. are employees ofNatera Inc. S.A. was employed by Natera Incduring the study and initial follow-up period.
REFERENCES
1. Chitty LS, Bianchi DW. Noninvasive prenataltesting: the paradigm is shifting rapidly. PrenatDiagn 2013;33:511-3.2. Pergament E, Cuckle H, Zimmermann B,et al. Single-nucleotide polymorphism-basednoninvasive prenatal testing in a high-risk andlow-risk cohort. Obstet Gynecol 2014;124:210-8.3. Nicolaides KH, Syngelaki A, Gil M,Atanasova V, Markova D. Validation of targetedsequencing of single-nucleotide polymorphismsfor non-invasive prenatal detection of aneuploidyof chromosomes 13, 18, 21, X, and Y. PrenatDiagn 2013;33:575-9.4. Samango-Sprouse C, Banjevic M, Ryan A,et al. SNP-based non-invasive prenatal testingdetects sex chromosome aneuploidies with highaccuracy. Prenat Diagn 2013;33:643-9.5. Nicolaides KH, Syngelaki A, Gil MD,Quezada MS, Zinevich Y. Prenatal detection offetal triploidy from cell-free DNA testing inmaternal blood. Fetal Diagn Ther 2014;35:212-7.6. Bianchi DW, Platt LD, Goldberg JD,Abuhamad AZ, Sehnert AJ, Rava RP. Genome-wide fetal aneuploidy detection by maternalplasma DNA sequencing. Obstet Gynecol2012;119:890-901.7. Palomaki GE, Deciu C, Kloza EM, et al. DNAsequencing of maternal plasma reliably identifiestrisomy 18 and trisomy 13 as well as Downsyndrome: an international collaborative study.Genet Med 2012;14:296-305.8. Palomaki GE, Kloza EM, Lambert-Messerlian GM, et al. DNA sequencing ofmaternal plasma to detect Down syndrome: aninternational clinical validation study. Genet Med2011;13:913-20.9. Ashoor G, Syngelaki A, Wagner M, Birdir C,Nicolaides KH. Chromosome-selectivesequencing of maternal plasma cell-free DNAfor first-trimester detection of trisomy 21 andtrisomy 18. Am J Obstet Gynecol 2012;206:322.e1-5.10. Ashoor G, Syngelaki A, Wang E, et al.Trisomy 13 detection in the first trimester ofpregnancy using a chromosome-selective cell-free DNA analysis method. Ultrasound ObstetGynecol 2013;41:21-5.11. Norton ME, Brar H, Weiss J, et al. Non-invasive chromosomal evaluation (NICE) study:
NOVEMBER 2014 Ameri
results of a multicenter prospective cohort studyfor detection of fetal trisomy 21 and trisomy 18.Am J Obstet Gynecol 2012;207:137.e1-8.12. Sparks AB, Struble CA, Wang ET, Song K,Oliphant A. Noninvasive prenatal detection andselective analysis of cell-free DNA obtained frommaternal blood: evaluation for trisomy 21 andtrisomy 18. Am J Obstet Gynecol 2012;206:319.e1-9.13. Sparks AB, Wang ET, Struble CA, et al.Selective analysis of cell-free DNA in maternalblood for evaluation of fetal trisomy. PrenatDiagn 2012;32:3-9.14. Bianchi DW, Parker RL, Wentworth J, et al.DNA sequencing versus standard prenatalaneuploidy screening. N Engl J Med 2014;370:799-808.15. Benn P, Borell A, Chiu R, et al. Positionstatement from the aneuploidy screening com-mittee on behalf of the Board of the InternationalSociety for Prenatal Diagnosis. Prenat Diagn2013;33:622-9.16. Gregg AR, Gross SJ, Best RG, et al. ACMGstatement on noninvasive prenatal screening forfetal aneuploidy. Genet Med 2013;15:395-8.17. American College of Obstetricians and Gy-necologists. Noninvasive prenatal testing forfetal aneuploidy. Committee opinion no. 545.Obstet Gynecol 2012;120:1532-4.18. Verweij EJ, Jacobsson B, vanScheltema PA, et al. European non-invasive tri-somy evaluation (EU-NITE) study: a multicenterprospective cohort study for non-invasive fetaltrisomy 21 testing. Prenat Diagn 2013;33:996-1001.19. Mazloom AR, Dzakula Z, Oeth P, et al.Noninvasive prenatal detection of sex chromo-somal aneuploidies by sequencing circulatingcell-free DNA from maternal plasma. PrenatDiagn 2013;33:591-7.20. Ehrich M, Deciu C, Zwiefelhofer T, et al.Noninvasive detection of fetal trisomy 21 bysequencing of DNA in maternal blood: a study ina clinical setting. Am J Obstet Gynecol2011;204:205.e1-11.21. Sehnert AJ, Rhees B, Comstock D, et al.Optimal detection of fetal chromosomal abnor-malities bymassively parallel DNA sequencing ofcell-free fetal DNA from maternal blood. ClinChem 2011;57:1042-9.22. Futch T, Spinosa J, Bhatt S, de Feo E,Rava RP, Sehnert AJ. Initial clinical laboratoryexperience in noninvasive prenatal testing forfetal aneuploidy from maternal plasma DNAsamples. Prenat Diagn 2013;33:569-74.23. Liao GJ, Chan KC, Jiang P, et al. Noninva-sive prenatal diagnosis of fetal trisomy 21 byallelic ratio analysis using targeted massivelyparallel sequencing of maternal plasma DNA.PLoS One 2012;7:e38154.24. Zimmermann B, Hill M, Gemelos G, et al.Noninvasive prenatal aneuploidy testing ofchromosomes 13, 18, 21, X, and Y, using tar-geted sequencing of polymorphic loci. PrenatDiagn 2012;32:1233-41.25. Dan S, Wang W, Ren J, et al. Clinical appli-cation of massively parallel sequencing-based
prenatal noninvasive fetal trisomy test for tri-somies 21 and 18 in 11,105 pregnancies withmixed risk factors. Prenat Diagn 2012;32:1225-32.26. Lau TK, ChanMK, Lo PS, et al. Clinical utilityof noninvasive fetal trisomy (NIFTY) testeearlyexperience. J Matern Fetal Neonatal Med2012;25:1856-9.27. Gil MM, QuezadaMS, Bregant B, FerraroM,Nicolaides KH. Implementation of maternalblood cell-free DNA testing in early screening foraneuploidies. Ultrasound Obstet Gynecol2013;42:34-40.28. Fairbrother G, Johnson S, Musci TJ,Song K. Clinical experience of noninvasive pre-natal testing with cell-free DNA for fetal trisomies21, 18, and 13, in a general screening popula-tion. Prenat Diagn 2013;33:580-3.29. Beamon CJ, Hardisty EE, Harris SC,Vora NL. A single center’s experiencewith noninvasive prenatal testing. Genet Med2014;16:681-7.
527.e10 American Journal of Obstetrics & Gynec
30. Wang E, Batey A, Struble C, Musci T,Song K, Oliphant A. Gestational age andmaternal weight effects on fetal cell-free DNA inmaternal plasma. Prenat Diagn 2013;33:662-6.31. Poon LC, Musci T, Song K, Syngelaki A,Nicolaides KH. Maternal plasma cell-free fetaland maternal DNA at 11-13 weeks’ gestation:relation to fetal and maternal characteristics andpregnancy outcomes. Fetal Diagn Ther2013;33:215-23.32. Canick JA, Palomaki GE, Kloza EM,Lambert-Messerlian GM, Haddow JE. Theimpact of maternal plasma DNA fetal fraction onnext generation sequencing tests for commonfetal aneuploidies. Prenat Diagn 2013;33:667-74.33. Ashoor G, Syngelaki A, Poon LC,Rezende JC, Nicolaides KH. Fetal fraction inmaternal plasma cell-free DNA at 11-13 weeks’gestation: relation to maternal and fetal charac-teristics. Ultrasound Obstet Gynecol 2013;41:26-32.
ology NOVEMBER 2014
34. Taglauer ES, Wilkins-Haug L, Bianchi DW.Review: cell-free fetal DNA in the maternal cir-culation as an indication of placental health anddisease. Placenta 2014;35(Suppl):S64-8.35. Choi H, Lau TK, Jiang FM, et al. Fetalaneuploidy screening by maternal plasma DNAsequencing: “false positive” due to confinedplacental mosaicism. Prenat Diagn 2013;33:198-200.36. Harrison KJ, Barrett IJ, Lomax BL,Kuchinka BD, Kalousek DK. Detection ofconfined placental mosaicism in trisomy 18conceptions using interphase cytogenetic anal-ysis. Hum Genet 1993;92:353-8.37. Grati FR, Malvestiti F, Ferreira JC, et al. Therole of feto-placental mosaicism in false positiveand falsenegative non-invasiveprenatal screening(NIPS) results. Genet Med 2014;16:620-4.38. Benn P, Cuckle H, Pergament E. Non-invasive prenatal diagnosis for Down syndrome:the paradigm will shift, but slowly. UltrasoundObstet Gynecol 2012;39:127-30.
SUPPLEMENTARY FIGURE45,X/46,XY mosaicism may explain the single discordant fetal sex result
Single-nucleotide polymorphism (SNP) data for single discordant fetal sex case are consistent with monosomy X fetus. Representative A, X-chromosome
and B, Y-chromosome SNP plots from female (XX), male (XY), and monosomy X (45,X) fetuses are shown using samples with fetal fractions of around
10% (I) and 20% (II). X-axis of each SNP plot represents the position along the chromosome, and y-axis indicates allele ratio. A, Fetal SNP data are
colored based on maternal genotype, with alleles arbitrarily labeled as A or B: where AA is blue, AB is green, and BB is red. When the maternal genotype is
homozygous at a specific SNP location (red or blue dots), the presence of single X-chromosome (45,X fetus or XY fetus) can easily be distinguished from 2
X-chromosomes (XX fetus); 45,X fetus with single paternal X-chromosome has a different SNP profile to that shown, but is easily distinguished by the
absence of maternal X-chromosome-derived SNPs in the fetus. B, Males are determined by the presence of Y-chromosome SNPs; as fetal fraction
increases, Y-chromosome SNPs migrate further away from X-axis, but Y-chromosome SNPs remain detectable down to at least 4% fetal fraction. C, For
the single discordant fetal sex case that had a fetal fraction of 10%, SNP data clearly indicate the presence of a single maternal X-chromosome, with no
paternal X-chromosome or Y-chromosome detected, leading to the monosomy X result. Mosaicism, which is frequently seen in association with a 45,X
cell line, is a possible explanation for this discordant result.
NIPT, noninvasive prenatal testing.
Dar. Clinical performance of SNP-based NIPT. Am J Obstet Gynecol 2014.
NOVEMBER 2014 American Journal of Obstetrics & Gynecology 527.e11
SUPPLEMENTARY TABLE 1Prevalence of International Classification of Diseases, Ninth Revision codes in low-risk, high-risk, and advancedmaternal age womenICD-9 code Description LR, n AMA, n HR, n Code type
228.1 Lymphangioma, any site 1 0 2 LR
278 Obesity, unspecified 0 1 1 LR
293.84 Anxiety disorder in conditions classified elsewhere 1 0 0 LR
300 Anxiety, dissociative and somatoform disorderseanxiety state unspecified
0 0 11 LR
305.03 Alcohol abuse, in remission 0 0 1 LR
305.1 Tobacco use disorder (tobacco dependence) 0 0 1 LR
306 Physiological malfunction arising from mental factorsemusculoskeletal
0 0 1 LR
313.1 Disturbance of emotions specific to childhood andadolescenceemisery and unhappiness disorder
1 0 0 LR
345 Epilepsy and recurrent seizures 0 0 1 LR
622.1 Dysplasia of cervix 6 0 0 LR
648.13 Thyroid dysfunctioneantepartum condition orcomplicationenot delivered during current episode ofcare
0 0 1 LR
649.13 Obesity complicating pregnancy, childbirth, orpuerperiumeantepartum condition or complicationenot delivered during current episode of care
0 1 0 LR
649.43 Epilepsy complicating pregnancy, childbirth, orpuerperium (antepartum obstetric condition, notdelivered during current episode of care)
0 1 0 LR
655.53 Suspected damage to fetus from drugs (antepartumcondition or complication)
1 2 1 LR
655.63 Suspected damage to fetus from radiation 0 1 0 LR
656.13 Other known or suspected fetal and placental problemsaffecting management of mothereRhesusisoimmunization
1 0 0 LR
695.3 Rosaceaeacne 0 0 1 LR
767.5 Facial nerve injuryefacial palsy 0 0 2 LR
780.39 Other convulsions 0 1 0 LR
790.92 Abnormal coagulation profile 0 0 1 LR
795.79 Other and unspecified nonspecific immunologicalfindings (raised antibody titer, raised level ofimmunoglobulins)
0 0 1 LR
V13.29 Personal history of diseaseeother genital system andobstetric disorders
0 0 1 LR
V13.63 Personal history of congenital malformations ofnervous system
1 0 0 LR
V19.5 Family history of skin condition 1 1 1 LR
V22.0 Supervision of normal first pregnancy 21 7 12 LR
V22.1 Supervision of other normal pregnancy 905 2421 2133 LR
V22.2 Pregnant state, incidental 28 8 6 LR
V23.41 Pregnancy with history of preterm labor 1 0 0 LR
Dar. Clinical performance of SNP-based NIPT. Am J Obstet Gynecol 2014. (continued)
Research Obstetrics ajog.org
527.e12 American Journal of Obstetrics & Gynecology NOVEMBER 2014
SUPPLEMENTARY TABLE 1Prevalence of International Classification of Diseases, Ninth Revision codes in low-risk, high-risk, and advancedmaternal age women (continued)
ICD-9 code Description LR, n AMA, n HR, n Code type
V23.85 Pregnancy resulting from assisted reproductivetechnology
0 1 0 LR
V26.31 Testing of female genetic disease carrier status 469 1476 1305 LR
V28.0 Encounter for antenatal screening of motherescreening for chromosomal anomalies byamniocentesis
0 2 1 LR
V28.1 Screening for raised alpha-fetoprotein levels inamniotic fluid
0 0 2 LR
V28.3 Encounter for routine screening for malformation usingultrasonics
2 0 1 LR
V28.6 Encounter for antenatal screening of motherescreening for streptococcus B
1 0 0 LR
V72.40 Pregnancy examination or testepregnancyunconfirmed
0 1 0 LR
V72.42 Pregnancy examination or testepositive result 0 0 1 LR
V77.2 Special screening for endocrine, nutritional, metabolic,and immunity disordersemalnutrition
0 0 1 LR
V77.6 Special screen for cystic fibrosis 19 19 19 LR
V77.7 Special screen for other inborn errors of metabolism 13 14 14 LR
V78.2 Special screen for sickle-cell disease 13 14 14 LR
V78.3 Special screen for other hemoglobinopathies 13 14 14 LR
V82.9 Unspecified condition 1 0 0 LR
659.53 AMAefirst pregnancy 29a 556 116 AMA
659.6 Elderly multigravida (unspecified as to episode of careor not applicable)
0 1 1 AMA
659.63 AMAenot first pregnancy 33a 1489 343 AMA
V23.82 Supervision of other HR pregnancy, elderlyprimigravida
SUPPLEMENTARY TABLE 1Prevalence of International Classification of Diseases, Ninth Revision codes in low-risk, high-risk, and advancedmaternal age women (continued)
ICD-9 code Description LR, n AMA, n HR, n Code type
646.31 Habitual aborter (for 646.3) 0 0 1 HR
646.33 Recurrent pregnancy loss (antepartum condition orcomplication not delivered during current episode ofcare)
0 0 4 HR
655.03 Central nervous system malformation in fetuseantepartum condition or complication
0 0 12 HR
655.13 Chromosomal abnormality in fetus (antepartumcondition or complication)
0 0 408 HR
655.23 Hereditary disease in family possibly affecting fetus(antepartum condition or complication)
0 0 70 HR
655.8 Other known or suspected fetal and placental problemsaffecting management of mother
0 0 4 HR
655.83 Other known or suspected fetal abnormality, notelsewhere classifiedeantepartum condition orcomplication
0 0 185 HR
655.9 Known or suspected fetal abnormality affectingmanagement of mothereunspecified (unspecified asto episode of care or not applicable)
0 0 1 HR
655.93 Known or suspected fetal abnormality affectingmanagement of mothereunspecified (antepartumcondition or complication)
0 0 8 HR
656.43 Intrauterine death (antepartum condition orcomplication)
SUPPLEMENTARY TABLE 1Prevalence of International Classification of Diseases, Ninth Revision codes in low-risk, high-risk, and advancedmaternal age women (continued)
ICD-9 code Description LR, n AMA, n HR, n Code type
747.5 Absence or hypoplasia of umbilical arteryesingleumbilical artery
0 0 3 HR
747.89 Other specified anomalies of circulatory systemeother(aneurysm, congenital, specified site not elsewhereclassified)
0 0 1 HR
748.1 Other anomalies of nose 0 0 1 HR
753.29 Obstructive defects of renal pelvis and uretereother 0 0 6 HR
754.7 Other deformities of feetetalipes, unspecified 0 0 1 HR
755.34 Reduction deformities of lower limbelongitudinaldeficiency, femoral, complete or partial (congenitalabsence of femur)
0 0 1 HR
756.17 Anomalies of spineespina bifida occulta 0 0 1 HR
758.5 Other condition due to autosomal anomalies (fetalaneuploidy)
0 0 6 HR
758.9 Condition due to anomaly of unspecified chromosome 0 0 1 HR
759.7 Multiple congenital anomalies, so described 0 0 2 HR
759.9 Congenital anomaly, unspecified 0 0 1 HR
764 “Light for dates” without mention of fetal malnutrition 0 0 1 HR
793.20 Nonspecific (abnormal) findings on radiological andother examination of body structureeotherintrathoracic organ
0 0 10 HR
793.60 Nonspecific (abnormal) findings on radiological andother examination of body structureeabdominal area,including retroperitoneum
0 0 1 HR
793.99 Nonspecific (abnormal) findings on radiological andother examination of body structureeother (placentalfinding by x-ray or ultrasound method, radiologicalfindings in skin and subcutaneous tissue)
SUPPLEMENTARY TABLE 1Prevalence of International Classification of Diseases, Ninth Revision codes in low-risk, high-risk, and advancedmaternal age women (continued)
ICD-9 code Description LR, n AMA, n HR, n Code type
V23.9 Unspecified HR pregnancy 0 0 6 HR
V26.89 Other specified procreative management 0 0 2 HR
V28.8 Other specified antenatal screening 0 0 17 HR
V28.81 Encounter for fetal anatomic survey 0 0 1 HR
a Unclear whether the uninformative single-nucleotide polymorphism pattern is maternal or fetal in origin.
Dar. Clinical performance of SNP-based NIPT. Am J Obstet Gynecol 2014.
SUPPLEMENTARY TABLE 2Exclusion categories for out-of-specification samplesExclusion category Count
Redraws accepted
Insufficient serum/plasma 127
<9 wk of gestationa 70
Test cancelled 45
Sample collection date too old 28
Missing information 11
Sample damaged 4
Wrong tube 4
Otherb 26
Redraws not requested
Multiple gestation 8
Egg donor 1
Surrogate 1
a Redraws are accepted once patient reaches 9 wks of gestation; b Includes uncommon exclusion reasons, such as hemolyzedblood samples and missing state-required waivers.
Dar. Clinical performance of SNP-based NIPT. Am J Obstet Gynecol 2014.
ajog.org Obstetrics Research
NOVEMBER 2014 American Journal of Obstetrics & Gynecology 527.e17















![Carotidynia-A Case Report with Clinical and Imaging Follow ... · with clinical response and relief of the symptoms [7]. The resolution of the imaging findings seems to follow the](https://static.documents.pub/doc/80x56/5e790a05eec353588552808d/carotidynia-a-case-report-with-clinical-and-imaging-follow-with-clinical-response.jpg)







