21
PULMONARY EMBOLISM CLINICAL features & Diagnosis
| Date post: | 15-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | bala-murugan |
| View: | 52 times |
| Download: | 0 times |
PULMONARY EMBOLISM
CLINICAL features & Diagnosis
.
• Life threatening causes of chest pain and shortness of breath “DYSPNOEA
• Pain sharp worse fro deep breathe “often called pleuritic pain”.
• They may present with HEMOPTYSIS
• The patient may have stable vital signs (blood pressure, heart rate, respiratory rate, and
oxygen saturation) but frequently presents with an elevated heart rate.
• A severe pulmonary embolus can present with shock or cardiac arrest, particularly when a
large clot blocks the outflow of blood from the right side of the heart to the lungs (saddle
embolus).
• Depending on the amount of blood clot (clot burden or clot load),
• oxygen saturation can be variably compromised as can the blood pressure and heart
rate. In a classic presentation,
•The heart rate and respiratory rate are elevated as the body tries to compensate.
INVESTIGATIONATERIAL BLOOD
• PaCO2 – Partial pressure of CO2 in the blood ,critical in regulating levels and maintaining body ph
• PaCO2 is maintained at 5.3 kPa (40 mmHg)
• D- dimer and other circulating markers.
• D-dimers is a specific degradation product released into the circulation when cross-linked fibrin undergoes endogenosis.
• An elevated D-dimer is limited value, as it occurs in a number of conditions including P.E
.
• Take note of the chest pain and breathlessness
• Physical examination will concentrate Heart and lungsSince the chest pain may
be presenting complains of heart attackPneumonia,
pneumothorax ( collapsed lung)And dissection of an
aortic aneurysm
• The physical exam will also include looking for signs of a D.V.T in an extremely
warmth swelling
redness , andtenderness.
• NB note that the signs associated with deep vein thrombosis may be completely absent even in the PRESENTS of a clot.
‘
• Full blood count • Electrolytes• BUN (blood urea nitrogen)• Creatinine blood test• Chest x-ray, and • Electrocardiogram• The chest x-ray is often normal in P.E• The EKG/ECG may be normal, but usually
demonstration a rapid heart rate• So called sinus tachycardia (heart > 100 bpm).• If there is significant blockage in a pulmonary
artery.• It acts like a dam and it harder for the heart to
push blood pas t the obstruction clot or clots.• This can result in the change in the electrical
signal passing through the heart by stretching the heart muscle, revealed on a EKG a so called right heart strain.
• Since the cost of missing the diagnosis of P.E can be death, the approach to diagnosis is to prove that no P.E exists.
PULMONARY Hypertension
Fatigue Hoarseness Difficulty breathing (dyspnoea) Dizziness Palpitations Fainting spells ( syncope ) Swelling of legs and ankles ( edema) Bluish Lips, skin ( cyanosis ) Chest pain
. A complete history and physical exam is done.
An electrocardiogram (ECG) may show a strain on the right side of your
heart.
Blood tests are done to indicate how much oxygen is in your blood, or to test
if you have a collagen vascular disease.
A chest x-ray may show a large pulmonary artery and right-sided heart. This
test may also show diseases of the lung such as
emphysema.
A lung scan is done to show the blood supply
in your lungs
A CT or CAT scan is a computerized x-ray
that can get a better view of the lungs and your
heart.
Echocardiogram uses sonar (sound waves) to
show the pumping function of your heart and how the valves work.
A pulmonary function test is done to measure the volume of air in your
lungs. Results are obtained by breathing into a mouth piece while exercising
on a treadmill or bicycle.
An exercise tolerance test will require you to walk on a treadmill as fast as
you can for 6 minutes to evaluate how much exercise you can do before you
have symptoms.
A right heart catheterization is the most accurate way to diagnose
pulmonary hypertension. A small tube or catheter is put into a vein in your
neck and then guided into the right side of your heart and pulmonary artery to
measure pressures.
Clinical features Pulmonary edema
Cardiogenic pulmonary edema◦ ischemia with or without myocardial infarction
◦ exacerbation of chronic systolic or diastolic heart failure, and dysfunction of the mitral or aortic valve
◦ paroxysmal nocturnal dyspnea or orthopnea
Noncardiogenic pulmonary edema ◦ pneumonia
◦ sepsis
◦ aspiration of gastric contents
◦ major trauma associated with the administration of multiple blood-product transfusions
Laboratory Testing
Electrocardiography Elevated troponinlevels
Measurement of electrolytes, the serum osmolarity, and a toxicology screen
Serum amylase and lipase
Laboratory Testing
BNP level below 100 pg per milliliter indicates that heart failure is unlikely (negative predictive value, >90 percent)
BNP level greater than 500 pg per milliliter indicates that heart failure is likely (positive predictive value, >90 percent)
BNP is secreted predominantly by the cardiac ventricles in response to wall stretch or increased intracardiac pressures
Laboratory Testing
BNP levels between 100 and 500 pg per milliliter provide inadequate diagnostic discrimination
BNP can also be secreted by the right ventricle, and moderate elevations have been reported in patients with acute pulmonary embolism, cor pulmonale, and pulmonary hypertension
Echocardiography
The first approach to assessing left ventricular and valvular function in patients in whom the history, physical and laboratory examinations, and the chest radiograph do not establish the cause of pulmonary edema
Less sensitive in identifying diastolic dysfunction
Does not rule out cardiogenic pulmonary edema
Pulmonary-Artery Catheterization
Assess the pulmonary-artery occlusion pressure
Is considered the gold standard for determining the cause of acute pulmonary edema
Monitoring of cardiac filling pressures, cardiac output, and systemic vascular resistance
Common complications included hematoma at the insertion site, arterial puncture, bleeding, arrhythmias, and bloodstream infection
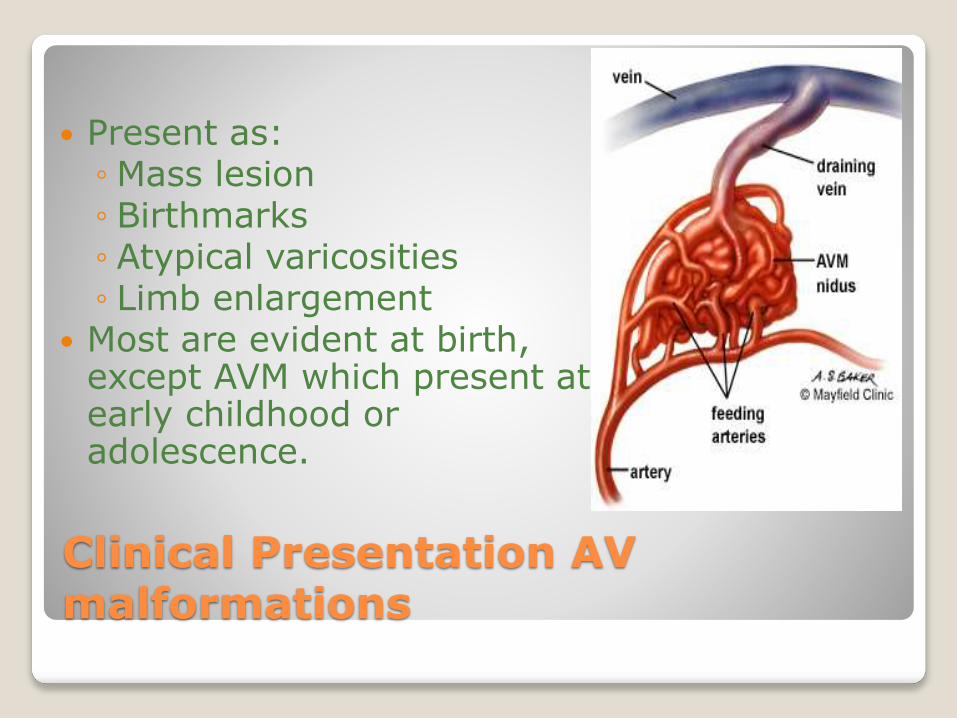
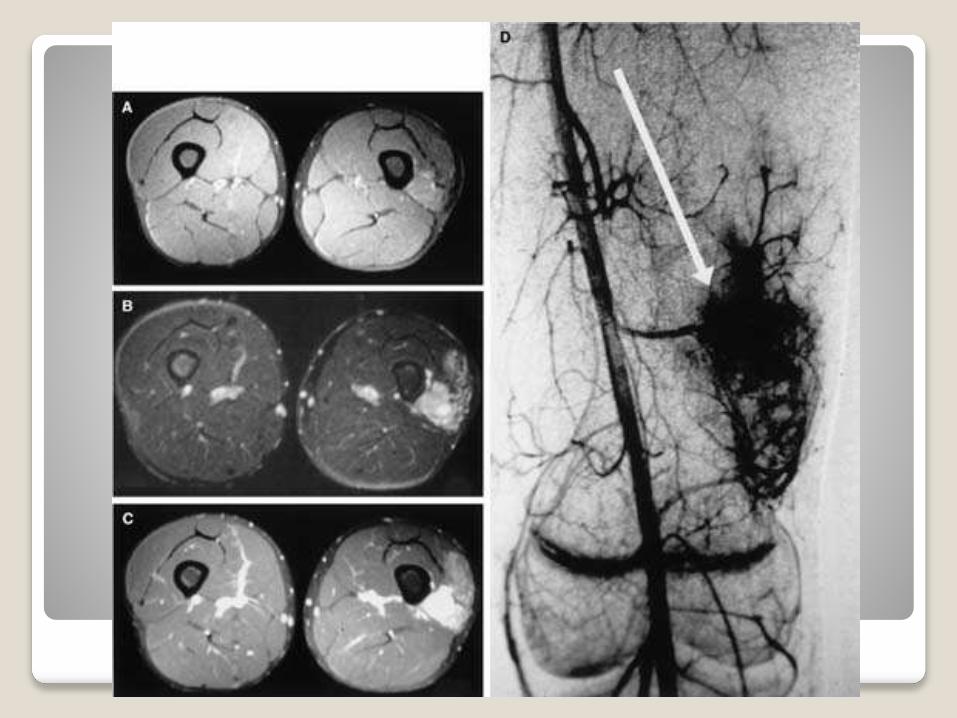
Clinical Presentation AV malformations
Present as:◦ Mass lesion◦ Birthmarks◦ Atypical varicosities◦ Limb enlargement
Most are evident at birth, except AVM which present at early childhood or adolescence.
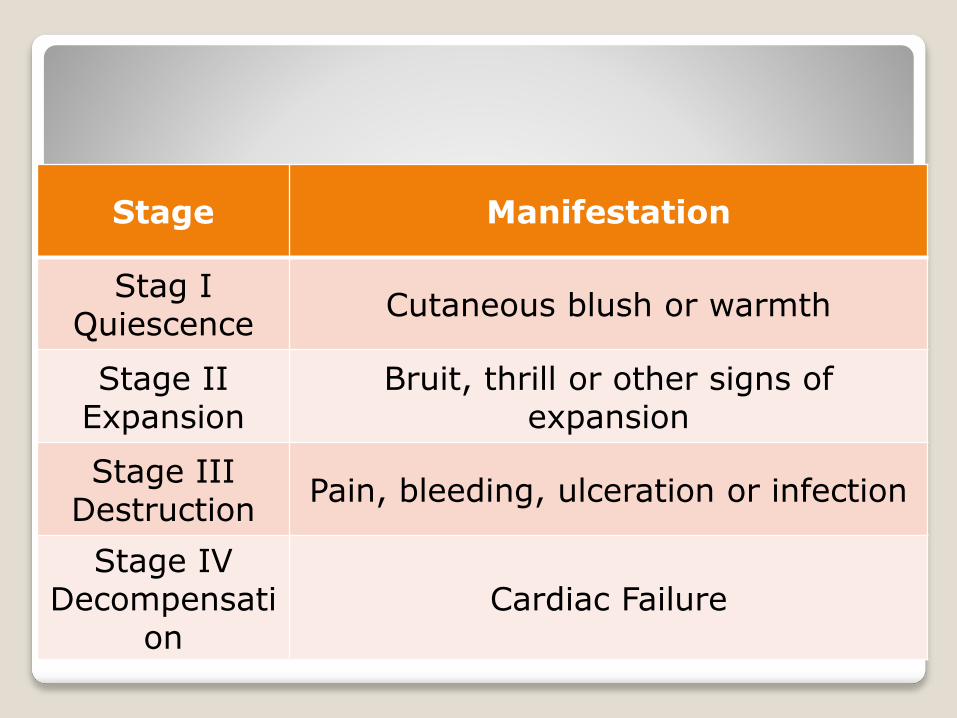
Staging of AVMs
Stage Manifestation
Stag IQuiescence
Cutaneous blush or warmth
Stage IIExpansion
Bruit, thrill or other signs of expansion
Stage IIIDestruction
Pain, bleeding, ulceration or infection
Stage IVDecompensati
onCardiac Failure
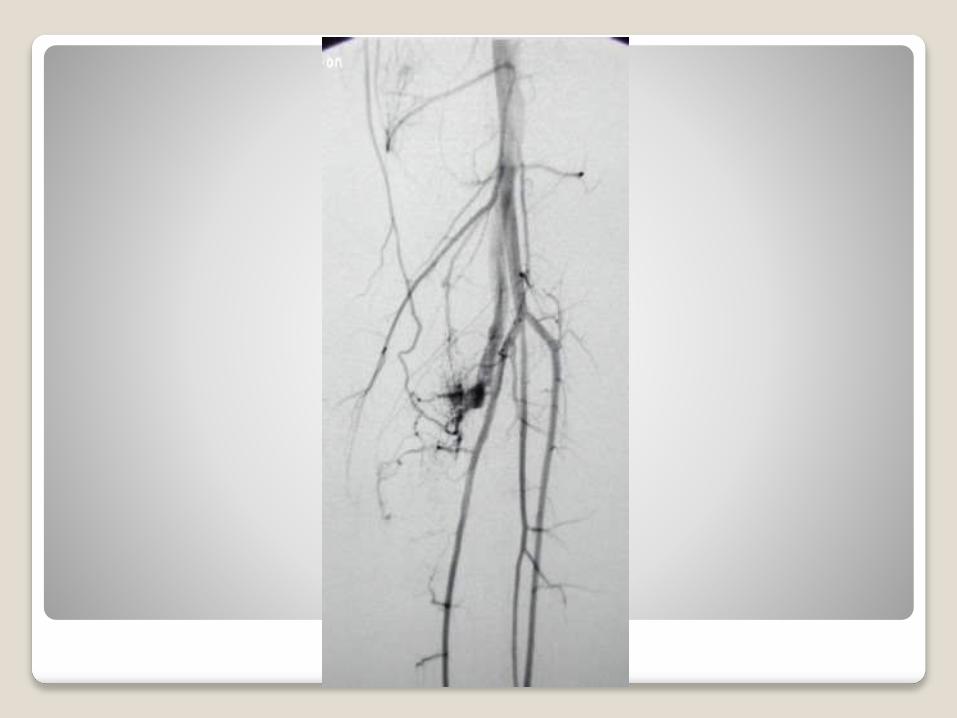
Diagnosis
Essentially by Imaging studies:
US (initial evaluation)
CT scan, CT Angiography
MRI, MRA (leading imaging modality)
Conventional Angiography
1. Diagnosis
2. Determine the extent of the lesion
3. Search for associated abnormalities