February 23-26, 2015 Seattle, Washington HIV/AIDS Seattle Update CCO Independent Conference Coverage of the 2015 Conference on Retroviruses and Opportunistic Infections* *CCO is an independent medical education company that provides state-of-the-art medical information to healthcare professionals through conference coverage and other educational programs. This program is supported by an educational grant from This program is supported by educational grants from Gilead Sciences, Merck, and ViiV.
Transcript
February 23-26, 2015Seattle, Washington
HIV/AIDS Seattle UpdateCCO Independent Conference Coverageof the 2015 Conference on Retroviruses and Opportunistic Infections*
*CCO is an independent medical education company that provides state-of-the-art medical information to healthcare professionals through conference coverage and other educational programs.
This program is supported by an educational grant from
This program is supported by educational grants fromGilead Sciences, Merck, and ViiV.
clinicaloptions.com/hiv2015 Conference on Retroviruses and Opportunistic Infections
About These Slides
Users are encouraged to use these slides in their own noncommercial presentations, but we ask that content and attribution not be changed. Users are asked to honor this intent
These slides may not be published or posted online without permission from Clinical Care Options (email [email protected])
DisclaimerThe materials published on the Clinical Care Options Web site reflect the views of the authors of the CCO material, not those of Clinical Care Options, LLC, the CME providers, or the companies providing educational grants. The materials may discuss uses and dosages for therapeutic products that have not been approved by the United States Food and Drug Administration. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or using any therapies described in these materials.
clinicaloptions.com/hiv2015 Conference on Retroviruses and Opportunistic Infections
Faculty
Joseph J. Eron, Jr., MDProfessor of Medicine and EpidemiologyUniversity of North Carolina School of MedicineDirector, AIDS Clinical Trials UnitUniversity of North CarolinaChapel Hill, North Carolina
Joel E. Gallant, MD, MPHMedical Director of Specialty Services Southwest CARE CenterSanta Fe, New MexicoAdjunct Professor of MedicineDivision of Infectious DiseasesJohns Hopkins University School of MedicineBaltimore, Maryland
Kathleen E. Squires, MDW. Paul and Ida H. Havens Professor of Infectious DiseasesDirector, Division of Infectious DiseasesSidney Kimmel Medical College of Thomas Jefferson UniversityPhiladelphia, Pennsylvania
clinicaloptions.com/hiv2015 Conference on Retroviruses and Opportunistic Infections
Disclosures
Joseph J. Eron, Jr., MD, has disclosed that he has received consulting fees from AbbVie, Bristol-Myers Squibb, Gilead Sciences, GlaxoSmithKline/ViiV, Merck, Tibotec/Janssen, and Tobira; and has received funds for research support from GlaxoSmithKline/ViiV.
Joel E. Gallant, MD, has disclosed that he has received consulting fees from Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck, and ViiV and funds for research support from AbbVie, Bristol-Myers Squibb, Gilead Sciences, GlaxoSmithKline/ViiV, Janssen, Merck, and Sangamo Biosciences.
Kathleen E. Squires, MD, has disclosed that she has received funds for research support paid to Thomas Jefferson University from Gilead Sciences and has served on advisory boards for Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck, and ViiV.
Prevention
clinicaloptions.com/hiv2015 Conference on Retroviruses and Opportunistic Infections
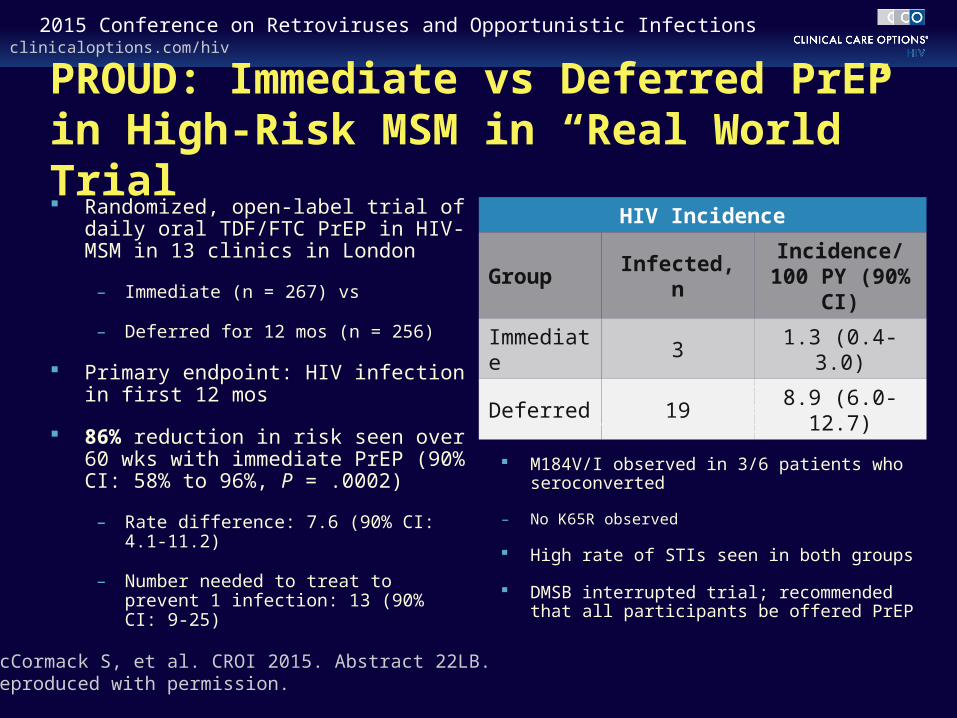
PROUD: Immediate vs Deferred PrEP in High-Risk MSM in “Real World” Trial Randomized, open-label trial of daily
oral TDF/FTC PrEP in HIV- MSM in 13 clinics in London
– Immediate (n = 267) vs
– Deferred for 12 mos (n = 256)
Primary endpoint: HIV infection in first 12 mos
86% reduction in risk seen over 60 wks with immediate PrEP (90% CI: 58% to 96%, P = .0002)
– Rate difference: 7.6 (90% CI: 4.1-11.2)
– Number needed to treat to prevent 1 infection: 13 (90% CI: 9-25)
2 of 3 infected persons in immediate group seroconverting at study entry or shortly after first dose of PrEP
M184V/I observed in 3/6 patients who seroconverted
– No K65R observed
High rate of STIs seen in both groups
DMSB interrupted trial; recommended that all participants be offered PrEP
HIV Incidence
Group Infected, nIncidence/100 PY (90% CI)
Immediate 3 1.3 (0.4-3.0)
Deferred 19 8.9 (6.0-12.7)
McCormack S, et al. CROI 2015. Abstract 22LB.Reproduced with permission.
clinicaloptions.com/hiv2015 Conference on Retroviruses and Opportunistic Infections
0.20
0.16
0.12
0.08
0.04
0.000 2 4 6 8 10 12 14 16 18 20 22 24 26
Mos
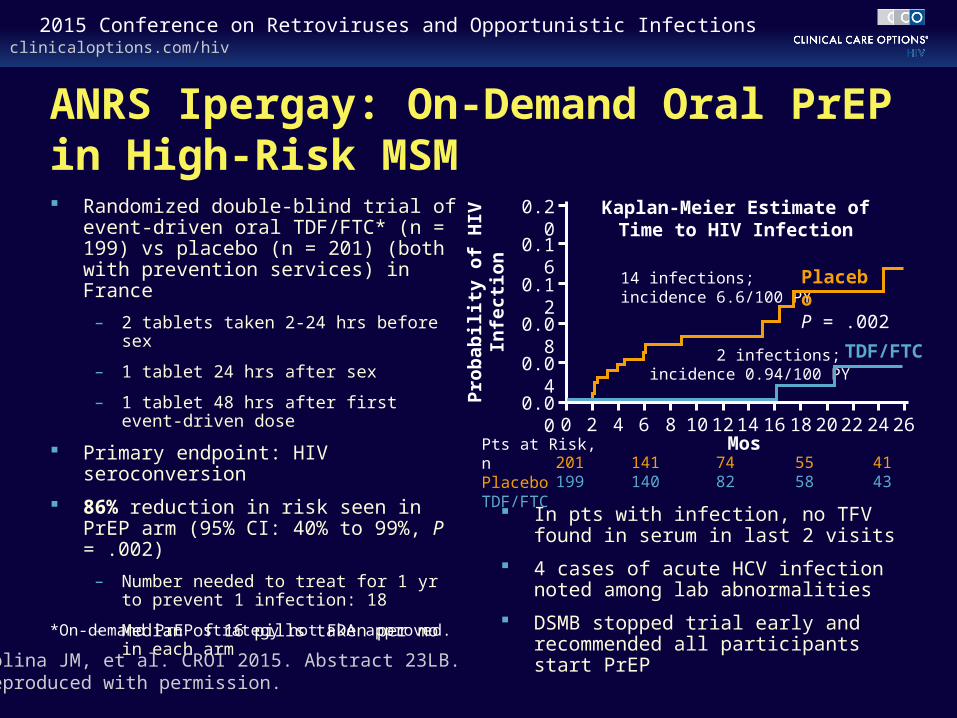
ANRS Ipergay: On-Demand Oral PrEP in High-Risk MSM Randomized double-blind trial of event-
driven oral TDF/FTC* (n = 199) vs placebo (n = 201) (both with prevention services) in France
– 2 tablets taken 2-24 hrs before sex
– 1 tablet 24 hrs after sex
– 1 tablet 48 hrs after first event-driven dose
Primary endpoint: HIV seroconversion
86% reduction in risk seen in PrEP arm (95% CI: 40% to 99%, P = .002)
– Number needed to treat for 1 yr to prevent 1 infection: 18
– Median of 16 pills taken per mo in each arm
In pts with infection, no TFV found in serum in last 2 visits
4 cases of acute HCV infection noted among lab abnormalities
DSMB stopped trial early and recommended all participants start PrEPMolina JM, et al. CROI 2015. Abstract 23LB.
Reproduced with permission.
*On-demand PrEP strategy not FDA approved.
2 infections; incidence 0.94/100 PY
14 infections; incidence 6.6/100 PY
201199
141140
7482
5558
4143
Pts at Risk, nPlaceboTDF/FTC
Placebo
TDF/FTC
P = .002
Pro
bab
ilit
y o
f H
IV
Infe
ctio
n
Kaplan-Meier Estimate of Time to HIV Infection
clinicaloptions.com/hiv2015 Conference on Retroviruses and Opportunistic Infections
Oral PrEP + ART as Prevention in High-Risk Serodiscordant Couples Partners Demonstration Project in Africa
– Oral daily TDF/FTC PrEP for HIV-uninfected partner in serodiscordant couple continued 6 mos beyond initiation of ART for infected partner
– High-risk couples defined as younger age, fewer children, uncircumcised HIV-negative male, cohabitating, unprotected sex in past mo, high HIV-1 RNA in HIV-positive partner
Interim analysis
– > 95% of HIV-negative partners using PrEP
– 80% of HIV-positive partners have initiated ART; of these, > 90% with suppression
96% reduction in expected infections
‒ IRR, expected vs observed: 0.04 (95% CI: 0.01-0.19; P < .0001)
In pts with seroconversion, no TFV detectable in plasma at time of seroconversion
– HIV-positive partner in 1 couple not on ART (high CD4+ count)
– Other couple dissolved and HIV-negative partner in new relationship
Baeten J, et al. CROI 2015. Abstract 24. Reproduced with permission.
HIV Incidence, Actual vs Expected
Group Infected, nIncidence/100 PY
(95% CI)
Expected 39.7 5.2 (3.7-6.9)
Actual 2 0.2 (0-0.9)
clinicaloptions.com/hiv2015 Conference on Retroviruses and Opportunistic Infections
Medical Cost Savings Associated With HIV Prevention in the United States Cost modeling analysis of the Medical Expenditure Panel
Survey
Investigators used Cost-Effectiveness of Preventing AIDS Complications Model to project discounted lifetime medical costs, assuming HIV infection at 35 yrs of age
The medical cost savings of averting 1 HIV infection was found to be $229,800
Cost savings are higher if taking secondary infections into account and lower if infection is delayed vs totally averted
Schackmann R, et al. CROI 2015. Abstract 1104.
clinicaloptions.com/hiv2015 Conference on Retroviruses and Opportunistic Infections
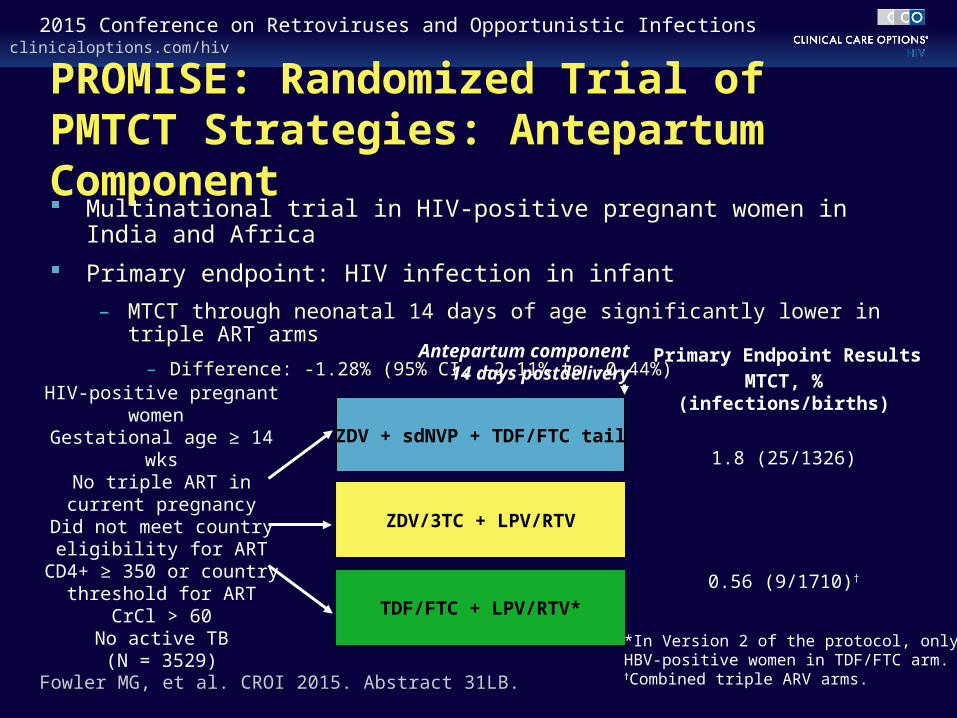
PROMISE: Randomized Trial of PMTCT Strategies: Antepartum Component Multinational trial in HIV-positive pregnant women in India and Africa
Primary endpoint: HIV infection in infant
– MTCT through neonatal 14 days of age significantly lower in triple ART arms
– Difference: -1.28% (95% CI, -2.11% to -0.44%)
Fowler MG, et al. CROI 2015. Abstract 31LB.
ZDV + sdNVP + TDF/FTC tail
TDF/FTC + LPV/RTV*
ZDV/3TC + LPV/RTV
HIV-positive pregnant women Gestational age ≥ 14 wksNo triple ART in current
pregnancyDid not meet country
eligibility for ARTCD4+ ≥ 350 or country
threshold for ARTCrCl > 60
No active TB(N = 3529)
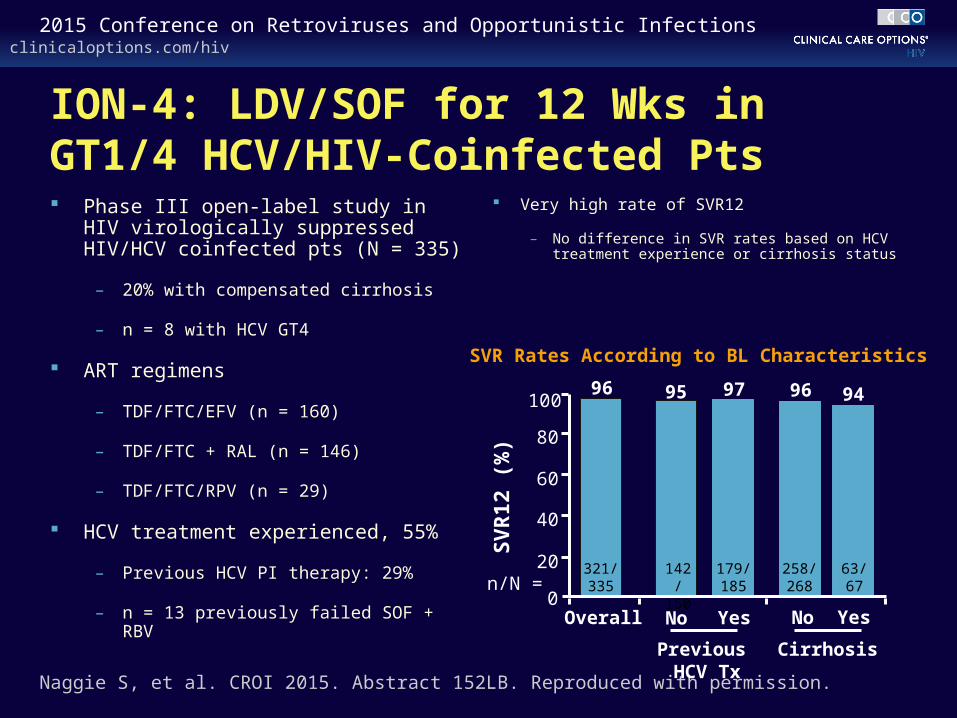
MTCT, % (infections/births)
1.8 (25/1326)
0.56 (9/1710)†
*In Version 2 of the protocol, only HBV-positive women in TDF/FTC arm. †Combined triple ARV arms.
Primary Endpoint ResultsAntepartum component14 days postdelivery
clinicaloptions.com/hiv2015 Conference on Retroviruses and Opportunistic Infections
PROMISE: Less MTCT but Adverse Events Greater in Triple ART Arms Higher moderate, but not severe, adverse pregnancy outcome with triple ARV
– Severe outcomes less in ZDV/3TC arm vs TDF/FTC arm
– Lower risk of infant death with ZDV/3TC vs TDF/FTC: 0.6% (2/346) vs 4.4% (15/341), P = .001
– Primarily among deaths in infants < 34 wks of gestational age
Fowler MG, et al. CROI 2015. Abstract 31LB. Reproduced with permission.





























![TB Clinical Intensive – Seattle “Treatment of Tuberculosis”nid]/5... · 1 TB Clinical Intensive – Seattle “Treatment of Tuberculosis” June 3, 2015 Masa Narita, MD Public](https://static.documents.pub/doc/80x56/5e11de62f66132191272686f/tb-clinical-intensive-a-seattle-aoetreatment-of-tuberculosisa-nid5-1.jpg)

