225 Clinical Investigation Development of Coronary Heart Disease in Familial Hypercholesterolemia Hiroshi Mabuchi, MD, Junji Koizumi, MD, Masami Shimizu, MD, Ryoyu Takeda, MD, and the Hokuriku FH-CHD Study Group We studied the development of coronary artery disease in 10 homozygous and 692 heterozygous patients with familial hypercholesterolemia. Seventy-five (22%) male heterozygotes and 35 (10%) female heterozygotes were affected by myocardial infarction, which was first noted in men in the 3rd decade of life and in women in the 4th decade of life. Thirty-eight (70%) out of the deceased 54 heterozygous patients died of coronary heart disease. The mean age at death was significantly less in male heterozygotes (54 years) than in female heterozygotes (69 years). Five homozygous and 105 male and 56 female heterozygous patients received coronary angiographic evaluation. The regression equations between age (X) and coronary stenosis index (Y1 obtained by assigning score (0 to 5) to each of 15 coronary artery segments were Y= 1.57X-20.43 (r=0.956, p <0.05) in the homozygotes, Y=0.52X-9.11 (r=0.438, p <0.001) in the male heterozygotes, and Y=0.47X- 12.54 (r=0.343, p <0.01) in the female heterozygotes. From these data, we can assume that coronary artery stenosis detectable by angiography will occur after 17 and 25 years of age in male and female heterozygotes, respectively, and the treatment of heterozygotes with lipid-lowering drugs can be delayed until late adolescence. (Circulation 1989;79:225-332) F amilial hypercholesterolemia (FH) is a com- mon autosomal dominant disorder caused by a mutation of the gene for the low-density lipoprotein (LDL) receptor.1 FH is frequently asso- ciated with premature coronary heart disease (CHD), and the rate of death from CHD among heterozy- gotes is several times higher than that among the general population.1-4 Homozygous patients do not usually survive to reach the age of 30,1,5 whereas the mean age at death for male and female heterozygotes is 54 and 65,4,6,7 respectively. There are no data, however, reporting when FH patients develop coro- nary heart disease documented by coronary angiog- raphy. The National Institutes of Health Consensus Development Conference on lowering cholesterol to prevent heart disease has recommended that strict dietary intervention is indicated for children with a blood cholesterol level above 200 mg/dl and that nonresponders should be considered for treatment with a lipid-lowering agent.8 Several authors, who From the Second Department of Internal Medicine, Kanazawa University School of Medicine, Kanazawa, Japan. Supported by the grant for Primary Hyperlipidemia Research Projects of the Welfare Ministry of Japan. Address for correspondence: Hiroshi Mabuchi, MD, The Second Department of Internal Medicine, Kanazawa University School of Medicine, Takara-machi 13-1, Kanazawa 920, Japan. Received April 20, 1988; revision accepted October 25, 1988. have suggested that the earliest possible treatment of hypercholesterolemia can lead to the best results for FH patients, have treated children with FH.9 There are, however, no reports that indicate when CHD develops in FH and how rapidly it progresses. In the present study, we examined coronary angiographic findings to estimate the onset and progression of CHD in FH patients and to deduce when treatment of hypercholesterolemia can be initiated. Methods Patient Selection Consecutive 10 homozygous (five men and five women) and 692 heterozygous (340 men and 352 women) patients with FH from 372 families had been enrolled in this study since 1974. FH was diagnosed according to the following two criteria: 1) primary hypercholesterolemic patients (arbitrarily above 230 mg/dl in any age group) with tendon xanthomas,10 and 2) primary hypercholesterolemic patients with and without tendon xanthomas in a first-degree relative of familial hypercholesterolemic patients. The diagnosis of homozygous FH was made on hypercholesterolemic patients with gener- alized xanthomas whose parents had been ascer- tained as heterozygous FH. All the data of these patients were obtained before the introduction of the treatment with the drugs such as bile acid- by guest on June 1, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript
225
Clinical Investigation
Development of CoronaryHeart Disease in Familial Hypercholesterolemia
Ryoyu Takeda, MD, and the Hokuriku FH-CHD Study Group
We studied the development of coronary artery disease in 10 homozygous and 692 heterozygouspatients with familial hypercholesterolemia. Seventy-five (22%) male heterozygotes and 35(10%) female heterozygotes were affected by myocardial infarction, which was first noted inmen in the 3rd decade of life and in women in the 4th decade of life. Thirty-eight (70%) out ofthe deceased 54 heterozygous patients died of coronary heart disease. The mean age at deathwas significantly less in male heterozygotes (54 years) than in female heterozygotes (69 years).Five homozygous and 105 male and 56 female heterozygous patients received coronary
angiographic evaluation. The regression equations between age (X) and coronary stenosis index(Y1 obtained by assigning score (0 to 5) to each of 15 coronary artery segments were
Y= 1.57X-20.43 (r=0.956, p <0.05) in the homozygotes, Y=0.52X-9.11 (r=0.438, p <0.001) inthe male heterozygotes, and Y=0.47X- 12.54 (r=0.343, p <0.01) in the female heterozygotes.From these data, we can assume that coronary artery stenosis detectable by angiography willoccur after 17 and 25 years of age in male and female heterozygotes, respectively, and thetreatment of heterozygotes with lipid-lowering drugs can be delayed until late adolescence.(Circulation 1989;79:225-332)
F amilial hypercholesterolemia (FH) is a com-mon autosomal dominant disorder causedby a mutation of the gene for the low-density
lipoprotein (LDL) receptor.1 FH is frequently asso-ciated with premature coronary heart disease (CHD),and the rate of death from CHD among heterozy-gotes is several times higher than that among thegeneral population.1-4 Homozygous patients do notusually survive to reach the age of 30,1,5 whereas themean age at death for male and female heterozygotesis 54 and 65,4,6,7 respectively. There are no data,however, reporting when FH patients develop coro-nary heart disease documented by coronary angiog-raphy. The National Institutes of Health ConsensusDevelopment Conference on lowering cholesterol toprevent heart disease has recommended that strictdietary intervention is indicated for children with ablood cholesterol level above 200 mg/dl and thatnonresponders should be considered for treatmentwith a lipid-lowering agent.8 Several authors, who
From the Second Department of Internal Medicine, KanazawaUniversity School of Medicine, Kanazawa, Japan.
Supported by the grant for Primary Hyperlipidemia ResearchProjects of the Welfare Ministry of Japan.Address for correspondence: Hiroshi Mabuchi, MD, The
Second Department of Internal Medicine, Kanazawa UniversitySchool of Medicine, Takara-machi 13-1, Kanazawa 920, Japan.Received April 20, 1988; revision accepted October 25, 1988.
have suggested that the earliest possible treatment ofhypercholesterolemia can lead to the best results forFH patients, have treated children with FH.9 Thereare, however, no reports that indicate when CHDdevelops in FH and how rapidly it progresses. In thepresent study, we examined coronary angiographicfindings to estimate the onset and progression ofCHD in FH patients and to deduce when treatmentof hypercholesterolemia can be initiated.
MethodsPatient Selection
Consecutive 10 homozygous (five men and fivewomen) and 692 heterozygous (340 men and 352women) patients with FH from 372 families hadbeen enrolled in this study since 1974. FH wasdiagnosed according to the following two criteria: 1)primary hypercholesterolemic patients (arbitrarilyabove 230 mg/dl in any age group) with tendonxanthomas,10 and 2) primary hypercholesterolemicpatients with and without tendon xanthomas in afirst-degree relative of familial hypercholesterolemicpatients. The diagnosis of homozygous FH wasmade on hypercholesterolemic patients with gener-alized xanthomas whose parents had been ascer-tained as heterozygous FH. All the data of thesepatients were obtained before the introduction ofthe treatment with the drugs such as bile acid-
by guest on June 1, 2018http://circ.ahajournals.org/
binding resins, probucol, and inhibitors of 3-hydroxy-3-methylglutaryl coenzyme A (HMG CoA)reductase.1'The diagnosis of myocardial infarction was
accepted when the following three criteria werefulfilled: characteristic clinical history, serial changesin electrocardiogram suggesting or proving myocar-dial infarction (Q waves) or injury (ST elevations),and transient increase of serum glutamic-oxalo-acetic transaminase, serum creatine phosphoki-nase, or serum lactate dehydrogenase. Diagnosis ofangina pectoris was based on location and quality ofthe pain as well as its precipitation by exertion andrelief by rest or nitroglycerin. Patients with normalresting electrocardiograms were given a Master'stwo-step exercise test or a treadmill test. Submaxi-mal exercise tests were performed on the treadmill.Exercise was performed at a 10% grade starting at 1mph with subsequent increases in speed until anginaor extreme exhaustion occurred or until the submax-imal predicted heart rate was achieved. Myocardialischemia was defined as 1 mm of flat or downslopingST segment depression. Causes of death were basedon autopsy studies, hospital records, or interviewswith the attending physicians.4
Cardiac CatheterizationCoronary angiography was performed with the
Judkins technique before (first projection) and after(other projections) sublingual administration of 0.3mg nitroglycerin. A left coronary angiography wasperformed in the 50, 15°, 300, and 600 right anterioroblique projections and additional projections includ-ing angulated views. A right coronary angiographywas performed in the 300 right anterior oblique andthe 450 or 600 left anterior oblique projection. Therecordings were made on 35 mm cinefilm exposed at60 frames/sec with a cardioscope U system made bythe Siemens Erma Company. Coronary angiogramswere interpreted by two or, in case of doubt, threeinvestigators without knowledge of the patient'sclinical history and serum lipid values. The extentand severity of stenotic changes were assessed byassigning scores to each of the 15 segments, accord-ing to the classification of the American HeartAssociation Grading Committee. The coronary ste-nosis index (CSI) was defined as the sum of thesescores.12 A normal coronary angiogram was graded0, stenosis of less than 25% was graded 1, 25-50%stenosis was graded 2, 50-75% stenosis was graded3, and more than 75% stenosis was graded 4. Thus,the highest possible CSI was graded 60. Coronaryangiographic study was performed in 58 heterozy-gotes with myocardial infarction, 34 heterozygoteswith angina pectoris or myocardial ischemia, and 69asymptomatic heterozygotes. The asymptomatic het-erozygotes received the angiographic evaluationbecause of the high frequency of premature CHD intheir affected family members.
Hypertension was defined as present if eitherantihypertensive treatment had been instituted or
maile% aleil
40 -
30
20 -
10
0 -
Age (yr) 0 10 20 30 40 50 60 70 80
male (n) 9 20 45 64 83 77 31 11
female (n) 6 26 43 40 49 89 76 23
FIGURE 1. Bar chart of incidence of myocardial infarc-tion by age group in male and female heterozygotes withfamilial hypercholesterolemia.
blood pressure was above 160 mm Hg systolic or 95mm Hg diastolic or both. Manifest diabetes mellituswas defined as present with fasting hyperglycemiaof 140 mg/dl or greater. Oral glucose tolerance wasassessed in all patients after ingestion of 75 or 50 gglucose. The criteria for varying degrees of glucoseintolerance suggested by WHO Expert Committee13and Japan Diabetes Society14 were applied. Therelative body weight was calculated by wt/(ht-100)x0.9. Subjects who smoked at least 10cigarettes/day were classified as current smokers.
Laboratory DeterminationBlood samples, obtained in the morning after a
12-hour overnight fast, were allowed to clot atroom temperature. Methods of lipoprotein frac-tions and lipid determinations were discussed inour previous study.15
StatisticsFor statistical procedures, Student's t test and
regression analysis were performed according to stan-dard statistical methods with a computer system.
ResultsIncidence of Myocardial Infarction
Myocardial infarction was diagnosed in 75 of 340(22%) male patients and 35 of 352 (10%) femalepatients with heterozygous FH. The incidence ofmyocardial infarction by age is shown in Figure 1.Myocardial infarction was first noted in the men inthe 3rd decade of life and in the women in the 4thdecade of life, with incidences gradually increasingby age. About 30% of male FH patients more than50 years of age and 20% of female FH patients morethan 60 years were affected by myocardial infarc-tion (Figure 1). Six of 10 homozygotes and 54 of 692heterozygotes have died. Sudden death or heartfailure was the cause of death in all six deceasedhomozygotes (Table 1). Their average age at deathwas 26 years, with an average serum cholesterollevel of 772 mg/dl. Thirty-eight (70.4%) out of the
by guest on June 1, 2018http://circ.ahajournals.org/
All values are mean ± SD. To convert cholesterol and triglyc-eride values to millimoles per liter, multiply by 0.026 and0.01129, respectively.
deceased 54 heterozygotes died of CHD. The meanage at death was significantly less in male heterozy-gotes (54 years) than in female heterozygotes (69years) (p <0.001) (Table 1). The mean serum cho-lesterol levels of deceased male and female hetero-zygotes were 371 and 346 mg/dl, respectively.
Coronary Angiographic StudyFive homozygous and 105 male and 56 female
heterozygous patients received coronary angio-graphic evaluation. Their clinical data are shown inTable 2. Serum LDL cholesterol levels of thehomozygotes were almost twice those of the het-erozygotes. In the male heterozygotes, coronaryangiographic study was performed in 49 patients(46%) with myocardial infarction, in 19 patients(18%) with angina pectoris or myocardial ischemia,and in 37 patients (35%) without symptoms andsigns of coronary heart disease (Table 3). In thefemale heterozygotes, the study was performed innine patients (16%) with myocardial infarction, 15patients (27%) with angina pectoris or myocardialischemia, and 32 patients (57%) without symptomsand signs of coronary heart disease (Table 3). Thesepatients were divided into two age-matched young(less than 49 years) and old (more than 50 years)groups. In any patient groups, those with myocar-dial infarction showed significantly higher CSI thanthose without symptoms and signs of CHD (p < 0.01)(Table 3). In the young female patient groups, thosewith angina pectoris or myocardial ischemia showed
significantly higher CSI than those without symp-
toms and signs (p<0.05) (Table 3).CSI and age of each patient are plotted in Figures
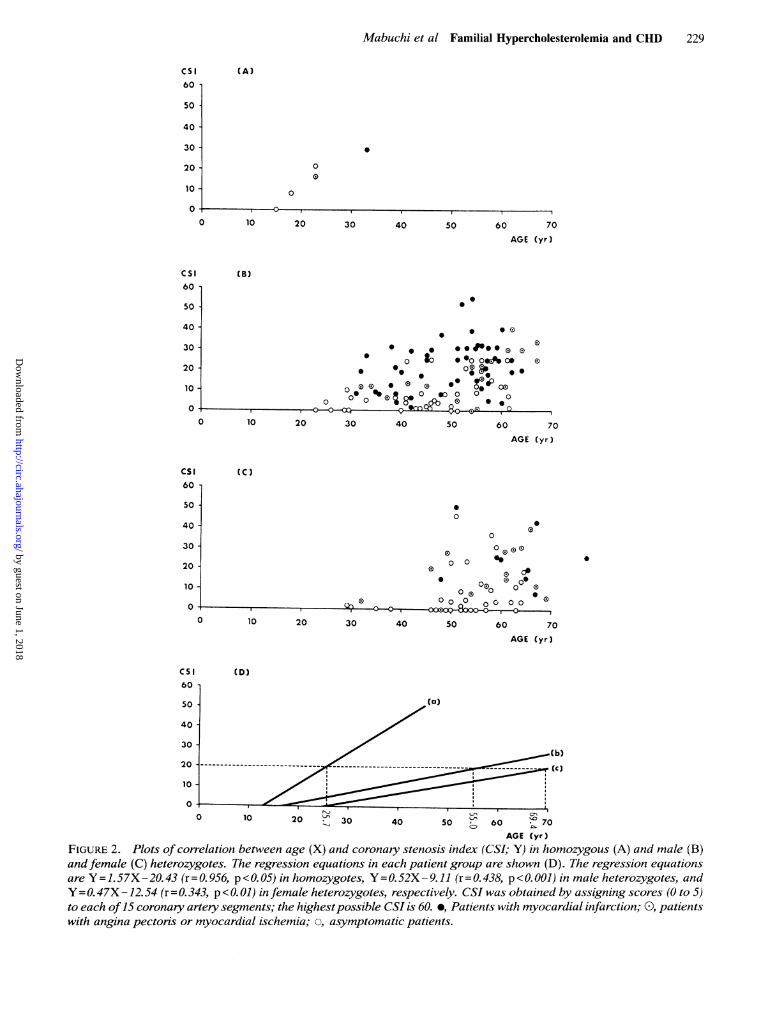
2A, 2B, and 2C. Their regression equations betweenage (X) and CSI (Y) are Y=1.57X-20.43 (r=0.956,p<0.05) in the homozygotes, y=0.52X-9.11(r=0.438,p<0.001) in the male heterozygotes, andY=0.47X-12.54 (r=0.343, p<0.01) in the femaleheterozygotes (Figure 2D). Midpoint and standarddeviation of CSI in five age groups (20-29, 30-39,40-49, 50-59, and 60-70 years) were shown inFigure 3. As might be predicted from the regressionequations in Figures 2D and 3, coronary stenosisshould begin, on the average, at 13 years of age inthe homozygotes and then at 17 and 25 years of age
in the male and the female heterozygotes, respec-
tively. The regression coefficient of the homozygoteswas about three times that of male and femaleheterozygotes. The age at which CSI reaches 20, forexample, could be predicted by this equation. Wecan estimate that CSI reaches 20 at the age of 25.7years in the homozygotes, 56.0 years in the maleheterozygotes, and 69.2 years in the female heterozy-gotes (Figure 2D). These ages exactly coincide withthose of the deceased FH patients (Table 1).
Nonlipid coronary risk factors, such as diabetesmellitus, obesity, hypertension, and smoking, were
studied in more than 86% of the male and 91% ofthe female heterozygotes, and they showed no
effects on CSI (Tables 4 and 5).
DiscussionA high level of plasma cholesterol is a major risk
factor for CHD. The Lipid Research Clinics Coro-nary Primary Prevention Trial produced convincingevidence that lowering plasma cholesterol levels inhypercholesterolemic men reduces the likelihood oftheir having a myocardial infarction.16'17 FH hasbeen known to be highly associated with CHD. Inthe present study, coronary artery stenosis was
demonstrated in four of five homozygotes, and one
male homozygote aged 15 years, who had beenonce treated with clofibrate ineffectively for 2 years,showed no coronary artery stenosis. Several casesin which homozygotes less than 17 years of agehave developed severe coronary artery stenosis or
supravalvular aortic stenosis have been reported.18" 9
TABLE 2. Clinical Data in Homozygous and Heterozygous Familial Hypercholesterolemic Patients Studied by Coronary Angiography
Cholesterol Achilles CoronaryFamilial Age tendon stenosishypercholesterolemia n (yr) Serum VLDL IDL LDL HDL Triglyceride Phospholipid thickness* index
All values are milligrams per deciliter and given as mean+SD. To convert cholesterol, triglyceride, and phospholipid values tomillimoles per liter, multiply by 0.026, 0.01129, and 0.324, respectively.VLDL, very low-density lipoprotein; IDL, intermediate-density lipoprotein; LDL, low-density lipoprotein; HDL, high-density
lipoprotein.*Normal values in Japanese subjects, 6.3+0.2 mm (mean+SEM).
by guest on June 1, 2018http://circ.ahajournals.org/
TABLE 3. Angiographically Defined Coronary Artery Disease in Familial HypercholesterolemicPatients With Myocardial Infarction, Angina Pectoris and/or Myocardial Ischemia, or No Symptoms and Signs ofCoronary Artery Disease
Sex Angina pectoris No symptoms or signsAge group Myocardial or of coronary heart(yr) infarction myocardial ischemia disease
All values are mean ± SD.CSI, coronary stenosis index.*p<0.05, tp<0.01 compared with patients having no symptoms or signs of coronary heart disease.
Goldstein et al,' who studied the prevalence ofCHD in a group of 54 homozygotes, found that theprevalence of CHD in the age group 0-10 years was60% in the receptor-negative homozygotes and 0%in the receptor-defective homozygotes. In the agegroup 10-20 years, the prevalence ofCHD was 47%in the receptor-negative homozygotes and 36% inthe receptor-defective homozygotes. Thus, homozy-gous patients should be treated as soon as thediagnosis is established, and plasma exchange, LDLapheresis,20 or other drastic therapies such as livertransplantation21 or portacaval shunt22 rather thandrug therapy have been applied. Four of our homozy-gous patients are now under the treatment withLDL apheresis.About 70% of heterozygous patients died of cor-
onary heart disease.4 Heiberg6 and Beaumont et a17reported that the incidence of coronary heart dis-ease in FH was much higher in men than in women,and the mean age of onset was 9 years sooner inmales. Kwiterowich et a123 found that none of the 70children with FH in his study had CHD in the 1stand 2nd decades, whereas half of their parents(mean age, 37.4 years) had CHD. The mean ages atwhich the affected men and women developed CHDwere 39.7 and 41.3 years, respectively. Among theheterozygotes less than 30 years of age, the inci-dence was extremely low (about 5% for men and 0%for women). However, there are few papers report-ing on CHD that have been documented by thecoronary angiography of FH patients. Hirobe et a124has reported that high-density lipoprotein (HDL)
cholesterol levels were higher and Achilles tendonthickness was less in 52 FH patients without CHDwhen compared with those with CHD. In our pre-vious study, severe coronary angiographic findingswere observed in FH patients compared with non-FH patients.25 Moreover, a high incidence of coro-nary ectasia was observed in male patients withFH.25 These reports, however, did not show whenCHD begins and how it progresses in FH patients.The present study consists of mixed FH patients
with myocardial infarction, angina pectoris, or nosymptoms, who agreed to receive coronary angio-graphic study. More patients with previous myocar-dial infarction (46% in the men and 16% in thewomen) or anginal pain have been included in thisstudy than patients without symptoms. If the studyhad included more asymptomatic patients, the fre-quency of coronary artery stenosis might have beensmaller and its onset later than in the present study.Despite these limiting characteristics, our studyprovides information about the course of CHD inthis subset of FH patients.Coronary atherosclerosis will be accelerated by
other risk factors, such as hypertension, diabetes,smoking, and obesity. However, in the presentstudy, there were no associations between CSI andnonlipid coronary risk factors. These nonlipid cor-onary risk factors appear to be overshadowed bythe prominent risk factors of inborn hypercholester-olemia and age in FH patients.6FH is an autosomal dominant disease, which is
completely expressed at birth and early in child-
by guest on June 1, 2018http://circ.ahajournals.org/
AGE (yr)FIGURE 2. Plots of correlation between age (X) and coronary stenosis index (CSI; Y) in homozygous (A) and male (B)and female (C) heterozygotes. The regression equations in each patient group are shown (D). The regression equationsare Y = 1.57X -20.43 (r = 0.956, p <0.05) in homozygotes, Y=0. 52X -9.11 (r = 0.438, p< 0.001) in male heterozygotes, andY = 0. 47X -12.54 (r = 0. 343, p < 0. 01) in female heterozygotes, respectively. CSI was obtained by assigning scores (0 to 5)to each of15 coronary artery segments; the highestpossible CSI is 60. *, Patients with myocardial infarction; 0), patientswith angina pectoris or myocardial ischemia; o, asymptomatic patients.
cs'60
so
40
30
20
10
(A)
0E)
0
01- - 1
cs'
Cs'60
(C)
5o A40
by guest on June 1, 2018http://circ.ahajournals.org/
Cs' fibrous plaques is uncertain and the extent of fatty40 streaks in youth does not predict the extent of30 male raised lesions in later life, these data suggest that a
20 rational approach to the prevention of CHD should10 a begin early in life.27 The National Institutes of
efrrarlllllwU> ; S e + S -Health Consensus Conference has recommended40 special guidelines for management of children.830- Strict dietary intervention is indicated, but treat-20
ment with a lipid-lowering agent in most children
should be deferred until evidence is available aboutthe safety and efficacy of drug therapy in children.
0 10 20 30 40 50 60 70 The coronary arteriogram has generally beenAGE (yr) found to reveal less-extensive disease than does
FIGURE 3. Plot of midpoint and standard deviation postmortem examination.28 However, clinically sig-(shadow area) ofcoronaty stenosis index (CSI) in five age nificant involvement is defined as 50% reduction ofgroups. the diameter of the main left coronary artery or 75%
or greater reduction of the diameter of the lumen inhood.1 The earlier the treatment of hypercholester- the right coronary, left anterior descending, or
olemia is started, the better the outcome of CHD in circumflex artery or their major branches. PatientsFH. However, the view that treatment of hyper- with normal coronary arteries have an excellentcholesterolemia in childhood will reduce adult mor- chance of remaining free of the disease for manybidity and mortality from CHD is necessarily based years.29'30 Discrepancies exist between arterial his-on extrapolation from controlled clinical trials in topathology and arteriography, but a properly per-middle-aged, high-risk, hypercholesterolemic formed coronary angiogram provides a true picturemen,16,17 since such studies have not been done on of the arterial lumen in living humans. Although thechildren. Newman et a126 reported that in young quality of the coronary atherosclerotic plaques waspatients aortic fatty streaks were strongly related to similar among FH patients and normolipidemicantemortem levels of both total and LDL choles- patients,31 the progression of CHD in the heterozy-terol and were inversely correlated with the ratio of gotes may be greater than in the general population,HDL cholesterol to LDL plus very-low-density as the progression of CHD in the homozygotes waslipoprotein (VLDL) cholesterol, and coronary artery three times that in the heterozygotes (Figure 2D).fatty streaks were correlated with VLDL choles- Although no heterozygotes less than 20 years of age
terol. Although the progression of fatty streaks to underwent coronary angiography in the present
TABLE 4. Angiographically Defined Coronary Artery Disease in Familial Hypercholesterolemic Patients WithDiabetes Mellitus, Impaired Glucose Tolerance, or Normal Glucose Tolerance
Sex Impaired NormalAge group Diabetes glucose glucose(yr) mellitus tolerance tolerance
Mabuchi et al Familial Hypercholesterolemia and CHD 231
TABLE 5. Angiographically Defined Coronary Artery Disease in Familial Hypercholesterolemic Patients With or WithoutObesity, Hypertension, or Smoking Habits
All values are mean SD.Obesity: + +, more than + 20%; +, + 10-19%; -, less than + 10% of ideal body weight. Hypertension: Known hypertension and blood
pressure readings of 160/95 mm Hg or higher. Smoking: currently smoking more than 10 cigarettes/day.
study and the regression lines intercept at 17 and 25years of age in male and female heterozygotes,respectively, there may in fact be a threshold atabout age 20 in men and 30 in women beforeangiographic abnormalities are seen. As dietarymodification will lower the plasma cholesterol lev-els in children and nutritional habits and otherlifestyles develop early in life, dietary managementshould be started in childhood.8'23'27 However, thepossible adverse effects of a modified diet mustalways be carefully considered. Moreover, lipid-lowering drugs have been proved to be safe ingeneral for adult patients, but no drugs have everbeen proved safe for the long-term treatment ofchildren. Because CHD does not usually developuntil 30 years of age in male heterozygotes or until40 years of age in female heterozygotes, treatmentwith lipid-lowering drugs or other drastic methodsshould not be required for the child heterozygotesand can instead be deferred until late adolescence.
The Hokuriku Familial Hypercholesterolemia(FH)-Coronary Heart Disease (CHD) Study Group
(*Principal investigator)Kanazawa University School of Medicine-
Fukui Shinzo-Ketsuatsu Center-Senshu Hifumi,MD and Junichiro Mifune, MD.
Katsuyama Hospital-Yasuyuki Sakai, MD. *
Takaoka Municipal Hospital-Masayuki Oota,MD* and Tetsuji Sumitani, MD.
Koseiren Takaoka Hospital-Tomio Kametani,MD.*Toyama Red Cross Hospital-Tadashi Monji,
MD, Norio Kusunoki, MD, and Toshio Shinagawa,MD.
References1. Goldstein JL, Brown MS: Familial hypercholesterolemia, in
Stanbury JB, Wyngaarden JB, Fredrickson DS, GoldsteinJL, Brown MS (eds): The Metabolic Basis of InheritedDisease, ed 5. New York, McGraw-Hill Book Co, 1983, p 672
3. Stone NJ, Levy RI, Fredrickson DS, Verter J: Coronaryartery disease in 116 kindred with familial type II hyperli-poproteinemia. Circulation 1974;49:476
4. Mabuchi H, Miyamoto S, Ueda K, Oota M, Takegoshi T,Wakasugi T, Takeda R: Causes of death in patients withfamilial hypercholesterolemia. Atherosclerosis 1986;61:1
6. Heiberg A: The risk of atherosclerotic vascular disease insubjects with xanthomatosis. Acta Med Scand 1975;198:249
7. Beaumont V, Jacotot B, Beaumont JL: Ischemic disease inmen and women with familial hypercholesterolemia andxanthomatosis: A comparative study of genetic and environ-mental factors in 274 heterozygous cases. Atherosclerosis1976;24:441
9. Kwiterowich PO Jr, Bachorik PS, Franklin FA Jr, MargolisS, Georgopoulos L, Teng B, Sniderman AD: Effect ofdietary treatment and the plasma levels of lipids, lipoproteincholesterol and LDL B protein in children with type IIhyperlipoproteinemia: Detection and treatment of lipid andlipoprotein disorders in childhood. Prog Clin Biol Res 1985;188:123
10. Mabuchi H, Ito S, Haba T, Ueda K, Ueda R, Tatami R,Kametani T, Koizumi J, Ohta M, Miyamoto S, Takeda R,Takegoshi T: Discrimination of familial hypercholesterol-emia and secondary hypercholesterolemia by Achilles' ten-don thickness. Atherosclerosis 1977;28:61
11. Kane JP, Havel RJ: Treatment of hypercholesterolemia.Ann Rev Med 1986;37:427
by guest on June 1, 2018http://circ.ahajournals.org/
12. Tatami R, Mabuchi H, Ueda K, Haba T, Kametani T, Ito S,Koizumi J, Ohta M, Miyamoto S, Nakayama A, Kanaya H,Oiwake H, Genda A, Takeda R: Intermediate-density lipo-protein and cholesterol-rich very low density lipoproteinangiographically determined coronary artery disease. Circu-lation 1981;64:1174
13. World Health Organization (WHO) Expert Committee on
Diabetes Mellitus: Second Report. Technical Report Series646. WHO, Geneva, 1980
14. Japan Diabetes Society Committee on Diagnosis of Diabe-tes: Committee report. J Japan Diabetes Soc 1982;25:859
15. Mabuchi H, Kamon N, Fujita H, Michishita T, Takeda M,Kajinami K, Itoh H, Wakasugi T, Takeda R: Effects ofCS-514 on serum lipoprotein lipid and apolipoprotein levelsin patients with familial hypercholesterolemia. Metabolism1987;36:475
16. Lipid Research Clinics Program: The Lipid Research ClinicsCoronary Primary Prevention Trial results: I. Reduction inincidence of coronary heart disease. JAM 1984;251:351
17. Lipid Research Clinics Program: The Lipid Research ClinicsCoronary Primary Prevention Trial results: II. The relation-ship of reduction in incidence of coronary heart disease tocholesterol lowering. JAMA 1984;251:365
18. Sprecher DL, Schaefer EJ, Kent KM, Gregg RE, Zech LA,Hoeg JM, McManus B, Roberts WC, Brewer HB Jr: Car-diovascular features of homozygous familial hypercholester-olemia: Analysis of 16 patients. Am J Cardiol 1984;54:20
19. Allen JM, Thompson GR, Myant NB, Steiner R, OakleyCM: Cardiovascular complications of homozygous familialhypercholesterolemia. Br Heart J 1980;44:361
20. Thompson GR, Lowenthal R, Myant NB: Plasma exchangein the management of homozygous familial hypercholester-olemia. Lancet 1975;1:1208
21. Bilheimer DW, Goldstein JL, Grundy SM, Starzl TE, BrownMS: Liver transplantation to provide low-density lipoproteinreceptors and lower plasma cholesterol in a child withhomozygous familial hypercholesterolemia. N Engl J Med1984;311: 1658
22. Starzl TE, Chase HP, Ahrens EH Jr, McNamara DJ, Bil-heimer DW. Schaefer EJ, Rey J, Porter KA, Stein E,
Francavilla A, Benson LN: Portacaval shunt in patients withfamilial hypercholesterolemia. Ann Surg 1983;198:273
23. Kwiterowich PO Jr, Fredrickson DS, Levy RI: Familialhypercholesterolemia (one form of familial type II hyperli-poproteinemia): A study of its biochemical, genetic, andclinical presentation in childhood.JClin Invest 1974;53:1237
24. Hirobe K, Matsuzawa Y, Ishikawa M, Tarui S, YamamotoA, Nambu S, Fujimoto K: Coronary artery disease inheterozygous familial hypercholesterolemia.Atherosclerosis1982;44:201
25. Genda A, Nakayama A, Shimizu M, Nunoda S, Sugihara N,Suematsu T, Kita Y, Yoshimura A, Koizumi J, Mabuchi H,Takeda R: Coronary angiographic characteristics in Japa-nese patients with heterozygous familial hypercholesterol-emia. Atherosclerosis 1987;66:29
26. Newman WP III, Freedman DS, Voors AW, Gard PD,Srinivasan SR, Cresanta JL, Williamson GD, Webber LS,Berenson GS: Relation of serum lipoprotein levels andsystolic blood pressure to early atherosclerosis: The Boga-lusa Heart Study. N Engl JMed 1986;314:138
27. Kwiterovich PO Jr: Biochemical, clinical, epidemiologic,genetic, and pathologic data in the pediatric age grouprelevant to the cholesterol hypothesis: Commentary. Pedi-atrics 1986;78:349
28. Vlodaver Z, Frech R, Van Tassel RA, Edwards JE: Corre-lation of the antemortem coronary arteriogram and thepostmortem specimen. Circulation 1973;47:162
29. Marchandise B, Bourassa MG, Chaitman BR, Lesperance J:Angiographic evaluation of the natural history of normalcoronary arteries and mild coronary atherosclerosis. Am JCardiol 1978;41:216
30. Gensini GG, Kelly AE: Incidence and progression of coro-
nary artery disease: An angiographic correlation in 1,263patients. Arch Intern Med 1972;129:814
31. Roberts WC, Ferrans VJ, Levy RI, Fredrickson DS: Car-diovascular pathology in hyperlipoproteinemia: Anatomicobservations in 42 necropsy patients with normal or abnor-mal serum lipoprotein patterns. Am J Cardiol 1973;31:557
KEY WORDS * familial hypercholesterolemia * coronaryheart disease by guest on June 1, 2018
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.79.2.225
1989;79:225-232Circulation.
http://circ.ahajournals.org/content/79/2/225the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 1, 2018http://circ.ahajournals.org/