This activity is jointly provided by Clinical and Patient Educators Association and Integritas Communications. This activity is supported by an educational grant from AstraZeneca. To be held in conjunction with the American Diabetes Association’s 75th Scientific Sessions
Transcript
This activity is jointly provided by Clinical and Patient Educators Association and Integritas Communications.
This activity is supported by an educational grant from AstraZeneca.
To be held in conjunction with the American Diabetes Association’s 75th Scientific Sessions
Lawrence Blonde, MD, FACP, FACEDirector, Ochsner Diabetes Clinical Research Unit Department of Endocrinology, Diabetes and Metabolism Associate Internal Medicine Residency Program Director Ochsner Medical Center New Orleans, Louisiana
Jaime A. Davidson, MD, FACP, MACEClinical Professor of Medicine Touchstone Diabetes Center University of Texas, Southwestern Medical Center Dallas, Texas
Daniel Einhorn, MD, FACP, FACEClinical Professor of Medicine University of California, San Diego Diabetes and Endocrine Associates Medical Director, Scripps Whittier Diabetes Institute La Jolla, California
PREA
MB
LE
4
TARGET AUDIENCEThe educational design of this activity addresses the needs of endocrinologists and other health care providers involved in the treatment of patients with type 2 diabetes.
STATEMENT OF NEED/PROGRAM OVERVIEWOver the last decade, increased understanding of the pathophysiology of type 2 diabetes mellitus (T2DM) has aided the development of new and expanding classes of antihyperglycemic medications.1-3 Agonists of glucagon-like peptide-1 (GLP-1) receptors, for example, take advantage of incretin hormone signaling to induce glucose-independent insulin release from pancreatic β cells, reduce hepatic glucose production, slow gastric emptying, and increase satiety.1,3,4 The potential benefits and risks of GLP-1 receptor agonists for various patient types or complicating comorbidities are the subjects of much ongoing clinical research.5-10 Indeed, education on how to achieve individualized glycemic targets and appropriately use these medications is of great practical interest to endocrinologists and other health care providers. This Clinical Issues™ program will provide attendees at the 2015 Scientific Sessions of the American Diabetes Association with scientifically rigorous, clinically accurate, and highly applicable recommendations for the roles of GLP-1 receptor agonists in multimodal T2DM management.
REFERENCES1. American Diabetes Association. Standards of medical care in diabetes–2015. Diabetes Care.
2015;36(suppl 1):S1-S94.
2. Defronzo RA. Banting Lecture. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. Diabetes. 2009;58(4):773-795.
3. Freeman JS. Role of the incretin pathway in the pathogenesis of type 2 diabetes mellitus. Cleve Clin J Med. 2009;76(suppl 5):S12-S19.
4. Inzucchi SE, et al. Management of hyperglycemia in type 2 diabetes: a patient-centered approach: Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012;35(6):1364-1379.
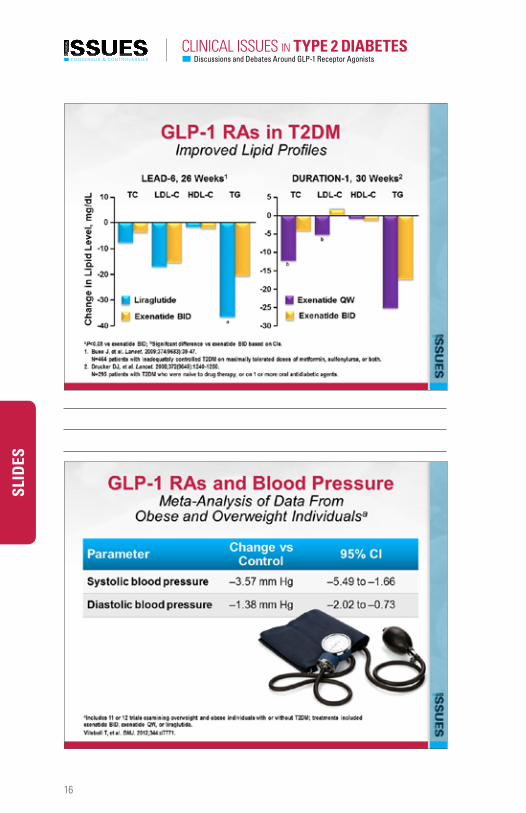
5. Wang B, et al. Blood pressure-lowering effects of GLP-1 receptor agonists exenatide and liraglutide: a meta-analysis of clinical trials. Diabetes Obes Metab. 2013;15(8):737-749.
6. Monami M, et al. Effects of glucagon-like peptide-1 receptor agonists on cardiovascular risk: a meta-analysis of randomized clinical trials. Diabetes Obes Metab. 2014;16(1)38-47.
7. Shao N, et al. Benefits of exenatide on obesity and non-alcoholic fatty liver disease with elevated liver enzymes in patients with type 2 diabetes. Diabetes Metab Res Rev. 2014;30(6):521-529.
8. Schwartz S, DeFronzo RA. Is incretin-based therapy ready for the care of hospitalized patients with type 2 diabetes?: The time has come for GLP-1 receptor agonists! Diabetes Care. 2013;36(7):2107-2111.
9. Elkind-Hirsch K, et al. Comparison of single and combined treatment with exenatide and metformin on menstrual cyclicity in overweight women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2008;93(7):2670-2678.
10. Seufert J, Gallwitz B. The extra-pancreatic effects of GLP-1 receptor agonists: a focus on the cardiovascular, gastrointestinal, and central nervous systems. Diabetes Obes Metab. 2014;16(8):673-688.
PREA
MB
LE
5For additional CME activities log on to
EDUCATIONAL OBJECTIVESAfter completing this activity, the participant should be better able to:
• Describe the relative benefits and risks of GLP-1 receptor agonists versus other oral and injectable antidiabetes medications
• Select among available short- and long-acting GLP-1 receptor agonists when intensifying T2DM therapy for various patient types
• Tailor combination regimens that include GLP-1 receptor agonists and other antihyperglycemic agents based on disease severity, comorbidities, and risks of hypoglycemia
• Engage in open dialogues with patients about the clinical profiles of GLP-1 receptor agonists and treatment adherence
PROGRAM AGENDA6:00 am – 6:10 am Faculty Introductions
6:10 am – 6:30 am Positioning GLP-1 Receptor Agonists in T2DM Algorithms for Treatment Intensification
6:30 am – 6:50 am GLP-1 Receptor Agonists in Multimodal Combination Regimens
6:50 am – 7:10 am Managing Heterogeneous Patient Populations: Addressing Clinical Comorbidities and Other Complications
7:10 am – 7:30 am Emerging Evidence for Potential Benefits and Risks of GLP-1 Receptor Agonists
7:30 am – 7:45 am Ask the Experts: Questions and Answers
INSTRUCTIONS TO RECEIVE CREDITIn order to receive credit for this activity, the participant must complete the program evaluation form at the conclusion of the symposium.
FEE INFORMATION & REFUND/CANCELLATION POLICYThere is no fee for this educational activity.
PREA
MB
LE
6
PHYSICIAN ACCREDITATION STATEMENTThis activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of Clinical and Patient Educators Association (CPEA) and Integritas Communications. CPEA is accredited by the ACCME to provide continuing medical education for physicians.
Physician Credit DesignationClinical and Patient Educators Association designates this live activity for a maximum of 1.75 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
CPEA Contact InformationFor information about the accreditation of this program, please contact CPEA at 303-953-4580 or [email protected].
DISCLOSURE OF CONFLICTS OF INTERESTClinical and Patient Educators Association (CPEA) requires instructors, planners, managers and other individuals and their spouses/life partners who are in a position to control the content of this activity to disclose any real or apparent conflict of interest they may have as related to the content of this activity. All identified conflicts of interest are thoroughly vetted by CPEA for fair balance, scientific objectivity of studies mentioned in the materials or used as the basis for content, and appropriateness of patient care recommendations.
The faculty reported the following financial relationships or relationships to products or devices they or their spouses/life partners have with commercial interests related to the content of this CME activity:
Lawrence Blonde, MD, FACP, FACE
Grant Research Support to Dr. Blonde’s institution from Eli Lilly and Company, Novo Nordisk, and sanofi-aventis U.S. LLC. Speakers Bureau for AstraZeneca, Janssen Pharmaceuticals, Inc., Merck & Co., Inc. Novo Nordisk, and sanofi-aventis U.S. LLC. Consultant to AstraZeneca, GlaxoSmithKline, Intarcia Therapeutics, Inc., Janssen Pharmaceuticals, Inc., Merck & Co., Inc., Novo Nordisk, Quest Diagnostics Inc., and sanofi-aventis U.S. LLC.
PREA
MB
LE
7For additional CME activities log on to
Jaime A. Davidson, MD, FACP, MACE
Consultant to and Advisory Board Member for Amgen Inc., Aspire Bariatrics, AstraZeneca, Boehringer Ingelheim GmbH, Bristol-Myers Squibb Company, Eli Lilly and Company, Janssen Pharmaceuticals, Inc., Johnson & Johnson, Lifescan, Inc., Merck & Co., Inc., Novo Nordisk, Roche Diagnostics, and sanofi-aventis U.S. LLC. Speakers Bureau for Janssen Pharmaceuticals, Inc., Novo Nordisk, and Takeda Pharmaceuticals Limited.
Daniel Einhorn, MD, FACP, FACE
Consultant to and Grant Research Support from AstraZeneca, Eli Lilly and Company, Janssen Pharmaceuticals, Inc., Novo Nordisk, sanofi-aventis U.S. LLC, and Takeda Pharmaceuticals Limited. Speakers Bureau for Janssen Pharmaceuticals, Inc.
The planners and managers reported the following financial relationships or relationships to products or devices they or their spouses/life partners have with commercial interests related to the content of this CME activity:
Andrea Funk Nothing to discloseAmanda Glazar, PhD Nothing to discloseJim Kappler, PhD Nothing to disclose
DISCLOSURE OF UNLABELED USEThis educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the FDA. Clinical and Patient Educators Association (CPEA) and Integritas Communications do not recommend the use of any agent outside of the labeled indications.
The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of any organization associated with this activity. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings.
DISCLAIMERParticipants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagnosis or treatment discussed in this activity should not be used by clinicians without evaluation of patient conditions and possible contraindications on dangers in use, review of any applicable manufacturer’s product information, and comparison with recommendations of other authorities.
8
SLID
ES
9For additional CME activities log on to
SLID
ES
10
SLID
ES
11For additional CME activities log on to
SLID
ES
12
SLID
ES
13For additional CME activities log on to
SLID
ES
14
SLID
ES
15For additional CME activities log on to
SLID
ES
16
SLID
ES
17For additional CME activities log on to
SLID
ES
18
SLID
ES
19For additional CME activities log on to
SLID
ES
20
SLID
ES
21For additional CME activities log on to
SLID
ES
22
SLID
ES
23For additional CME activities log on to
SLID
ES
24
SLID
ES
25For additional CME activities log on to
SLID
ES
26
SLID
ES
27For additional CME activities log on to
SLID
ES
28
SLID
ES
29For additional CME activities log on to
SLID
ES
30
SLID
ES
31For additional CME activities log on to
SLID
ES
32
SLID
ES
33For additional CME activities log on to
SLID
ES
34
SLID
ES
35For additional CME activities log on to
SLID
ES
36
SLID
ES
37For additional CME activities log on to
SLID
ES
38
SLID
ES
39For additional CME activities log on to
SLID
ES
40
SLID
ES
41For additional CME activities log on to
SLID
ES
42
SLID
ES
43For additional CME activities log on to
SLID
ES
44
SLID
ES
45For additional CME activities log on to
SLID
ES
46
SLID
ES
47For additional CME activities log on to
SLID
ES
48
SLID
ES
RESO
URC
E CE
NTE
R
49For additional CME activities log on to
GUIDELINES » Standards of medical care in diabetes—2015.
American Diabetes Association. Diabetes Care. 2015;38(suppl 1):S1-S94.
REFERENCES » Initial combination therapy with metformin, pioglitazone and exenatide is
more effective than sequential add-on therapy in subjects with new-onset diabetes. Results from the Efficacy and Durability of Initial Combination Therapy for Type 2 Diabetes (EDICT): a randomized trial. Abdul-Ghani MA, Puckett C, Triplitt C, et al. Diabetes Obes Metab. 2015;17(3):268-275.
» Is insulin the most effective injectable antihyperglycaemic therapy? Buse JB, Peters A, Russell-Jones D, et al. Diabetes Obes Metab. 2015;17(2):145-151.
» Risk of cardiac arrhythmias during hypoglycemia in patients with type 2 diabetes and cardiovascular risk. Chow E, Bernjak A, Williams S, et al. Diabetes. 2014;63(5):1738-1747.
RESO
URC
E CE
NTE
R
50
» Glucagon-like peptide 1 receptor agonist or bolus insulin with optimized basal insulin in type 2 diabetes. Diamant M, Nauck MA, Shaginian R, et al. Diabetes Care. 2014;37(10):2763-2773.
» Glucagon-like peptide-1 receptor agonist and basal insulin combination treatment for the management of type 2 diabetes: a systematic review and meta-analysis. Eng C, Kramer CK, Zinman B, Retnakaran R. Lancet. 2014;384(9961):2228-2234.
» Efficacy and safety of a fixed-ratio combination of insulin degludec and liraglutide (IDegLira) compared with its components given alone: results of a phase 3, open-label, randomised, 26-week, treat-to-target trial in insulin-naive patients with type 2 diabetes. Gough SC, Bode B, Woo V, et al. Lancet Diabetes Endocrinol. 2014;2(11):885-893.
» Central effects of GLP-1: new opportunities for treatments of neurodegenerative diseases. Hölscher C. J Endocrinol. 2014;221(1):T31-T41.
» Incretins and the intensivist: what are they and what does an intensivist need to know about them? Plummer MP, Chapman MJ, Horowitz M, Deane AM. Crit Care. 2014;18(1):205.
» Benefits of exenatide on obesity and non-alcoholic fatty liver disease with elevated liver enzymes in patients with type 2 diabetes. Shao N, Kuang HY, Hao M, Gao XY, Lin WJ, Zou W. Diabetes Metab Res Rev. 2014;30(6):521-529.
» Using real-world data to evaluate the association of incretin-based therapies with risk of acute pancreatitis: a meta-analysis of 1,324,515 patients from observational studies. Wang T, Wang F, Gou Z, et al. Diabetes Obes Metab. 2015;17(1):32-41.
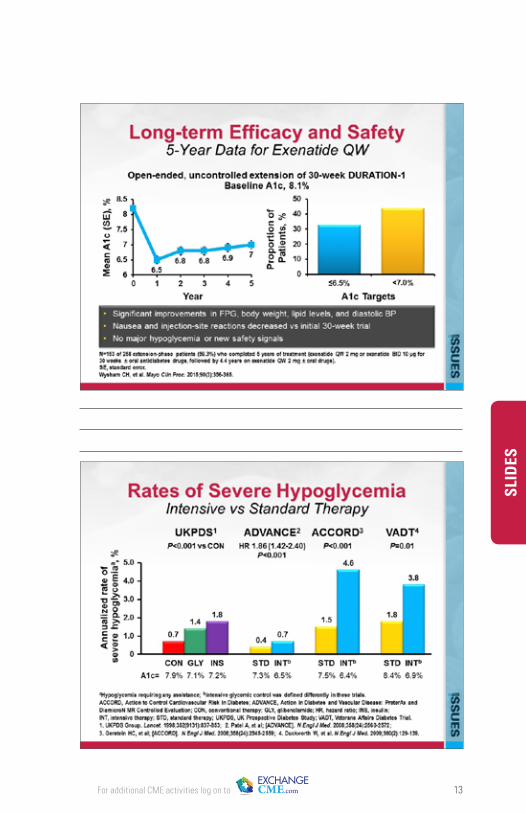
» Five-year efficacy and safety data of exenatide once weekly: long-term results from the DURATION-1 randomized clinical trial. Wysham CH, MacConell LA, Maggs DG, Zhou M, Griffin PS, Trautmann ME. Mayo Clin Proc. 2015;90(3):356-365.
All rights reserved. No part of this syllabus may be used or reproduced in any manner whatsoever without written permission except in the case of brief quotations embedded in articles or reviews.
Please visit the CLINICAL RESOURCE CENTER for additional information and resources