59
Clinical Review of Protopic Safety, Potential Risk, and Efficacy Martin M. Okun, M.D., Ph.D. Lisa Mathis, M.D. Division of Dermatologic and Dental Drug Products
| Date post: | 31-Dec-2015 |
| Category: |
Documents |
| Upload: | bernadette-shepherd |
| View: | 214 times |
| Download: | 1 times |

Clinical Review of Protopic Safety, Potential Risk, and
Efficacy
Martin M. Okun, M.D., Ph.D.
Lisa Mathis, M.D.
Division of Dermatologic and Dental Drug Products

Protopic Safety
• Safety Data Base– Adult and Pediatric Patients– 3 weeks, 12 weeks, 6 months, 12 months– 0.03%, 0.1%, 0.3% ointment

Protopic Safety Data Base
• Focus on:– Serious Adverse Events (AEs) and AEs
Discontinuation from Study (D/C)– AEs consistent with systemic
immunosuppression (e.g., lymphadenopathy, lymphoma, reactivation of VZV, HSV)

Adverse Events--Adults: 3 weeks treatment
No. ofAdults
TacrolimusOintmentStrength
SeriousAEs
AEs D/C
579 0.03% 2 (0.4%) 3 (0.5%)
571 0.1% 1 (0.2%) 5 (0.9%)
273 0.3% N/A 5 (2%)

Adverse Events--Adults: 3 weeks treatment
No. ofAdults
TacrolimusOintmentStrength
VZV HSV
579 0.03% 3 (0.5%)(zoster)
2 (1%)
571 0.1% 2 (0.4%)(zoster)
14 (2.4%)
273 0.3% N/A 1 (<1%)

Adverse Events--Adults: 12 weeks treatment
No. ofAdults
TacrolimusOintmentStrength
SeriousAEs
AEs D/C
210 0.03% 1 (<1%) 13 (6%)(mostlylocal AEs)
209 0.1% 6 (2 were post-treatment)
(3%)
11 (5%)(mostlylocal AEs)

Adverse Events--Adults: 12 weeks treatment
No. ofAdults
TacrolimusOintmentStrength
VZV HSV
210 0.03% 1 (<1%) 9 (3%)(includes2 KVE*)
209 0.1% 0 7 (2%)(includes1 KVE)
*Kaposi’s Varicelliform Eruption

Adverse Events--Adults: 6-12 months treatment
No. ofAdults
TacrolimusOintmentStrength
Duration SeriousAEs
AEs D/C
200 0.1% 6 months 10 (5%) 10 (5%)
1088 0.1% 12 months 22 (2%) 21 (2%)

Adverse Events--Adults: 6-12 months treatment
No. ofAdults
TacrolimusOintmentStrength
Duration VZV HSV
200 0.1% 6 months 2 13 (7%)(includes atleast 1 KVE)
1088 0.1% 12 months 2 (3%) 68 (6%)(19 reportedKVE cases)

Adverse Events--Pediatrics: 3 weeks treatment
No. ofChildren
TacrolimusOintmentStrength
SeriousAEs
AEs D/C
55 0.03% N/A 7 (13%)
62 0.1% N/A 1 (2%)

Adverse Events--Pediatrics: 3 weeks treatment
No. ofchildren
TacrolimusOintmentStrength
VZV HSV
55 0.03% 2 (1%)* 0
62 0.1% 0 1 (2%)
*both were chickenpox

Adverse Events--Pediatrics: 12 weeks treatment
No. ofchildren
TacrolimusOintmentStrength
SeriousAEs
AEs D/C
117 0.03% 1 (1%) 6 (5%)(mostly localAEs)
118 0.1% 5 (4%) 3 (3%)(mostly localAEs)

Adverse Events--Pediatrics: 12 weeks treatment
No. ofchildren
TacrolimusOintmentStrength
VZV HSV
117 0.03% 4* (3%) 2 (2%)(both wereKVE)
118 0.1% 1* (1%) 4 (3%)
*all were chickenpox

Adverse Events--Pediatrics: 1 year treatment
No. ofchildren
Tacrolimusointmentstrength
SeriousAEs
AEs D/C
92 ages 2-6;
96 ages 7-17
0.03% 0 0
393ages 2-6
0.1% 20 (5%) 10 (3%)
429ages 7-17
0.1% 22 (5%) 10 (2%)
44ages 7-17
0.3% 0 4 (9%)

Adverse Events--Pediatrics: 1 year treatment
No. ofchildren
Tacrolimusointmentstrength
VZV HSV
92ages 2-6;96ages 7-17
0.03% 0 0
393ages 2-6;429ages 7-17
0.1% 17 (2%)( 1 definiteherpes zoster, 7definitechickenpox)
25 (3%) (1 KVE)
44ages 7-17
0.3% 0 0

Lymphadenopathy in Clinical Studies
• Total cases: 33 No. of PatientsStrength
• Adults on 3 weeks therapy: 7 (0.1%)
• Adults on 1 year therapy: 3 (0.03%)
9 (0.1%)
• Children on 3 weeks therapy: 1 (0.1%)
• Children on 1 year therapy: 3 (0.03%)
10 (0.1%)
Lymphadenopathy Etiology• 68 year old male developed a parotid lymphoma. Uncertain if
lymphoma was a pre-existing condition
• 59 year old male developed CTCL.
• 6 cases with no clear etiology:– 4 resolved spontaneously– 2 discontinued therapy and were lost to follow up.
• 11 cases were related to skin infections:– 9 resolved on antibiotics– 3 discontinued therapy but had resolution of the lymphadenopathy.
• 12 cases related to URIs, resolved on antibiotics.• 2 cases related to tooth infections.

Common Adverse Events: 3 Twelve Week Studies
• Comparing AE rates across vehicle and active treatment arms complicated by the >50% discontinuation of patients in the vehicle arm
• Application site AEs (e.g., burning, pruritus, erythema, treatment-site infection):
– vehicle: 59% .03%: 75% .1%: 72%
• No obvious increase in local AEs as concentration increases

Common Adverse Events: 2 One Year Studies with 0.1% ointment
• Application Site AEs:– Pediatric Study 54% (16% of these coded
severe)– Adult Study 78% (28% of these coded severe), – Prevalence of Skin Burning declined to <10%
by week 4 of long-term studies

Safety Conclusions
• Most patients tolerated the 0.03% or 0.1% ointment concentrations.– Ointment use associated with application site
reactions in ~75% of patients– Most such reactions were mild and transient
• Tacrolimus 0.03% and 0.1% ointments had similar adverse event profiles
Safety Conclusions (cont’d)
• Possibility of an increased incidence of herpes zoster, herpes simplex, and Kaposi’s varicelliform eruption may exist
• Two patients developed lymphoma
• 6 patients developed lymphadenopathy with no obvious etiology

Efficacy Database
• 3 efficacy studies, identically designed:– multi-center, double-blinded, randomized– 12 weeks in duration– 3 arms:
• vehicle ointment, tacrolimus .03% ointment, tacrolimus .1% ointment
• Two studies in adult patients (-035, -036)
• One study in pediatric patients (-037)

Study Subjects
• Moderate to severe atopic dermatitis
• extent of involvement: 2%-100% BSA, with most having greater than 1/3 BSA
• Adult studies– -035: 15-77 years; -036: 16-79 years
• Pediatric studies– 037: 2-15 years

Study Protocol
• Wash out of non-medicated and medicated topical products
• Subjects applied ointment twice daily to essentially all areas of active disease
• Patients who cleared continued treatment for an additional week
• Prespecified treatment success at week 12: complete clearance or 90% improvement
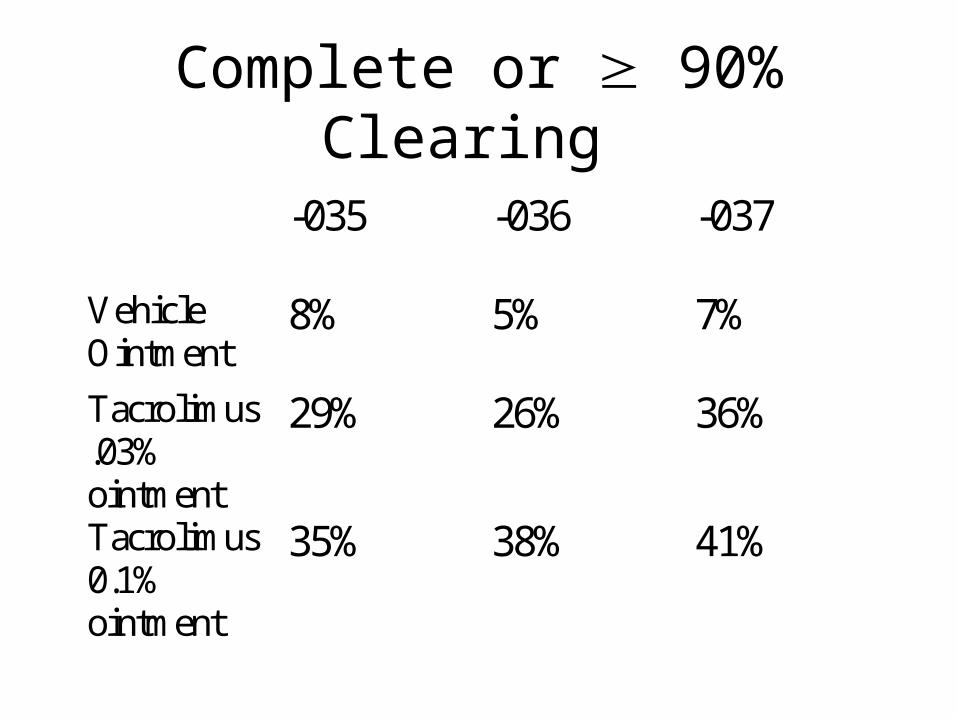
Complete or 90% Clearing
-035 -036 -037
VehicleOintment
8% 5% 7%
Tacrolimus.03%ointment
29% 26% 36%
Tacrolimus0.1%ointment
35% 38% 41%

Efficacy Outcomes
• In all three studies:– 0.1%, 0.03% ointments statistically significantly
superior to vehicle
– 0.1% ointment numerically, but not statistically, superior to 0.03% ointment:
• in -035,-036: treatment differences of 6, 12 percentage points
• in -037: treatment difference of 5 percentage points
• Is lack of statistical superiority due to equal efficacy or to Type II error?

Power Analysis
• Clinical studies may not have been adequately powered to detect statistically significant, clinically relevant differences in treatment effect between 0.03% and 0.1% ointments:– power of 0.18 to detect 10 percentage point
difference– power of 0.8 to detect 18 percentage point
difference

-035 and -036 Population Subsets: 0.03% vs. 0.1%
• 0.1% numerically superior to 0.03% ointment:– in males (32%-28%) and in females (40%-27%)– caucasians (40%-33%), african-americans (29%-16%),
asian-americans (42%-22%)– in patients who had baseline moderate disease (40%-
38%) and had baseline severe disease (35%-20%)– in patients who are older than 65 years (25%-22%) and
who are younger than 65 years (38%-27%)

-037 Population Subsets: 0.03% vs. 0.1%
• 0.1% numerically superior to 0.03% ointment:– caucasians (45%-40%), african-americans (27%-
25%), asian-americans (83%-43%)– patients with moderate baseline disease (47%-44%)
and with severe baseline disease (37%-30%)– ages 2-6 years (48%-38%)– males (44%-33%)
037 Population Subsets: 0.03% vs. 0.1%
• 0.03% numerically superior to 0.1 % ointment:– ages 7-15 years (32% vs. 30%)– females (39% vs. 38%)

Secondary Endpoint Outcomes: 0.03% vs. 0.1%
• In all 3 pivotal studies, 0.1% ointment was numerically superior to 0.03% ointment:– % patients with complete clearing at EOT, – reduction in % BSA involvement at EOT,– % patients with 50% improvement at week 1,
• Patient’s assessment of pruritus:– 0.1% ointment numerically superior in -035,
numerically inferior in -036, equal in -037

Efficacy Conclusions:
• Both tacrolimus ointment concentrations were statistically significantly efficacious over vehicle.
• Tacrolimus 0.1% ointment was numerically efficacious over 0.03%:– overall primary efficacy variable– most clinically relevant population subsets– most clinically relevant secondary efficacy variables

Efficacy Conclusions (2):
• Clinical studies may have been underpowered to detect clinically relevant, statistically significant differences in treatment outcomes between tacrolimus 0.1% and 0.03% ointments.

Potential Risk
• What is the potential risk of systemic immunosuppression induced by percutaneous absorption of tacrolimus?– What is the lowest amount of tacrolimus
percutaneous penetration at which clinically relevant systemic immunosuppression occurs?

Systemic Immunosuppression in Organ Transplant Recipients
• May manifest as lymphoproliferative disease, often associated with aggressive immunosuppression
• Frequently associated with acute or past infection with Epstein-Barr virus
• May progress to lymphoma or death

Lymphoproliferative Disorder in Adults
• Prevalence estimated at 0.8% in transplant patients.• Spectrum of disease ranges from polymorphic, polyclonal
B cell proliferation to frank lymphoma.• Most often associated with aggressive
immunosuppression and EBV infection.• Treatment includes reduction in immunosuppression,
antiviral therapy, debulking, chemotherapy and radiotherapy.
• Spontaneous regression can occur.• Mortality is over 50%.

Lymphoproliferative Disorder in Children
• Incidence estimated to be from 4-8% in transplant patients.
• 3 major risk factors: allograft type, EBV infection or reactivation, and immunosuppression.
• Can affect any organ system, and can be diffuse or focal. Abdominal disease is most frequent.
• Treatment involves reduction in immunosuppression, antivirals, and conventional antineoplastic therapy.
• Regression after withdrawing immunosuppression ranges from 23% to 65%.
• Mortality is lower than in adults, approximately 20-50%.

Time from Initiation of Immunosuppression to Development of
Lymphoproliferative Disease
• Tacrolimus: 12.6±5.1 months
• Cyclosporin A: 49.7±20.7 months
• Tacrolimus Rescue*: 9.8±3 months* Patients initially treated with CsA, but rescued
with high-dose tacrolimus secondary to graft rejection
Target Trough Whole Blood Levels of Tacrolimus for Immunosuppression in
Transplant Patients
• Trough blood levels correlates with systemic immunosuppression
• First month post-transplant: 12-15 ng/ml• Post-transplant months 1-3: 10-12 ng/ml• Post-transplant months 3-6: 5-10 ng/ml• After post-transplant month 6: In selected
patients, levels <5 ng/ml may be adequate if graft function is stable, but immunosuppression is highly variable.

Tacrolimus Blood Levels in Pivotal Controlled Studies
• Blood samples collected at weeks 1, 3, and EOT to measure tacrolimus levels.
• Blood samples collected at random with respect to time of last tacrolimus application (i.e., NOT trough levels)

Maximum Tacrolimus Blood Concentrations: -037
Patient Age:2-6 years
Tacrolimus 0.03%(n=16)
Tacrolimus 0.1%(n=17)
<blq 89% 80%
blq<1ng/ml 8% 13%
1-<2 ng/ml 4% 3%
2-<5 ng/ml 3%
Patient Age:7-15 years (n=10) (n=13)<blq 100% 100%

Maximum Tacrolimus Blood Concentrations: -035,-036
Adult Patients Tacrolimus0.03% (n=194)
Tacrolimus0.1% (n=193)
<blq 70% 59%
blq<1 ng/ml 21% 22%
1-<2 ng/ml 6% 12%
2-<5 ng/ml 3% 6%
5 ng/ml 1% (5.82 ng/ml,8.13 ng/ml)
1% (5.30 ng/ml)
What accounts for the isolated elevated tacrolimus blood levels?
• Why are the two highest levels detected in the 0.03% arm, even though the trend is for more patients in the 0.1% arm to have levels above blq? Possible explanations:– Isolated patients in 0.03% arm absorb more tacrolimus
systemically because of less efficacy– Covariate unrelated to treatment arm– Variability in the tacrolimus assay– Chance

Clinical Outcome and Blood Levels
Week 1 Week 3 EOT
Study No. 035 Blood level(ng/ml)
5.82 0.5 2
0.03%ointment
Clinical Eval. slightlyimproved
markedlyimproved
markedlyimproved
Study No. 036 Blood level 8.13 blq blq
0.03%ointment
Clinical Eval. slightlyimproved
moderatelyimproved
notappreciablyimproved
Study No. 036 Blood level blq 5.3 .85
0.1% ointment Clinical Eval. markedlyimproved
markedlyimproved
cleared

Percentage of Patients with Moderate Improvement or Better
by Week 1
Clinical Study 0.03% ointment 0.1% ointment
97-035 27% 45%
97-036 43% 46%
97-037 51% 59%
By improving patients more quickly, 0.1% ointment may reduce the percentage of patients who are susceptible to absorbing high levels of tacrolimus

Blood Levels in a Long-term Study
Blood levels tend to decline over time.Marked variability is noted throughout the study.

Persistent Blood Tacrolimus Levels in the One Year Study
• 60% of subjects had persistently elevated tacrolimus blood concentrations – This percentage refers to subjects who did not
have a specimen measuring blq within any of the following time periods: week 1, week 2, months 1, 3, 6, and 12,
– Not all subjects had measurements within each of these periods

Persistent Blood Tacrolimus Levels in the One Year Study
• Of the 48 subjects who did have 6 specimens collected, 54% had detectible tacrolimus concentrations in all specimens
Potential Risk: Topical Vs. Systemic Exposure
Topical:
• Intermittent exposure
• Levels only sporadically above blq in most patients
• Are tacrolimus levels at or near the application site higher than systemic levels?
Systemic:
• Lifetime exposure
• At least 6 months of >5 ng/ml serum trough levels

Potential Risk: Unresolved Issues
• The minimum systemic exposure at which there is clinically relevant Tacrolimus ointment-induced immunosuppression is unknown.
• The possibility of regional immunosuppression induced by topical application of Tacrolimus cannot be excluded.

Tacrolimus 0.03% vs. 0.1% ointment: 0.03%
Pros:•May have fewer patients with detectible blood levels•Most patients with detectible blood levels seem to have lower levels
Cons:•May have inferior efficacy•May be more associated with transient elevations above 5 ng/ml early in treatment.

Tacrolimus 0.03% vs. 0.1% ointment: 0.1%
Pros:•May have superior efficacy•No evidence of an adverse event signal suggesting greatertoxicity
Cons:•Most of those patients with detectible blood levels seem to have higher levels

Advisory Committee Question #1
• Is there sufficient evidence for effectiveness of Protopic, 0.03%, in the treatment of atopic dermatitis?

Advisory Committee Question #2
• Is there sufficient evidence for superior effectiveness of Protopic 0.1% compared to 0.03%…
a)…in adults?
b)…in children?

Advisory Committee Question #3
• Has the safety profile of Protopic been adequately determined for long term, intermittent therapy in the treatment of moderate to severe atopic dermatitis not adequately responsive to or intolerant of conventional treatment…a)…in adults for both 0.03% and 0.1%?
b)…in children for 0.03%?

Advisory Committee Question #4
• The proposed indication for Protopic, which would allow – for both 0.03% and 0.1%, – for unrestricted chronic therapy,– as a first-line treatment of atopic dermatitis, – in adults and children 2 years and older
may be decomposed into the following elements which may be reconstructed into indications:

Advisory Committee Question #4
Adults Children (2years and up)
Unrestrictedchronic therapyvs. time-limitedacute therapy?
? ?
First-line vs.second-linetreatment?
? ?
0.03%, 0.1%,both, or neither?
? ?

Advisory Committee Question #4
• Is approval of Protopic recommended and, if so, under what conditions [concentration(s), first- vs. second-line, chronic vs. (time-limited) acute therapy] in which age groups?

Advisory Committee Question #5
• Are there additional studies needed to provide information important for the labeling of Protopic? If so, what studies are recommended? (Consider the issues of lymphoma, local suppression of immunity, photocarcinogenesis, etc.)

















