22
Clinical Skills Task Group #5 Report Chairs: K. Klym and R. Brown
Clinical Skills Task Group #5 Report
Chairs: K. Klym and R. Brown

TG#5 Clinical Skills
Co-Chairs: Rob Brown, Karen Klym
Assignment: The nature and complexity of the skills required of the
physician is wide-ranging. The skill set includes and is built upon
foundational skills such as communication, organization, and leadership. It
progresses to specific functions, such as history taking, physical
examination, emergency management and procedures. This TG will focus
on defining the scope of clinical skills, identifying the pedagogical
approaches to be used, identifying key principles for integration with
cognitive curriculum, connecting goals and objectives and evaluation and
outlining overall timing/structure of clinical skills instruction.
Keywords: clinical skills, communication skills, History taking, physical examination, conflict resolution, procedural skills, crisis resource management.

Task Group #5

Definition of Clinical Skill
Anything that a physician DOES
Simple complex
Blood glucose monitoring
Clinical Reasoning
Broad scope
Mapping to CanMeds or another framework not udnertaken

Our Process Summer 2011
Literature search for curriculum development
Collation of AFMC, AAMC, GMC, CUSEC lists into one
master list
Committee Meetings Sept-Oct 2011
Review Master list
Deleted clearly inappropriate skills
Combined similar individual skills into single skills
Combined single skills into larger skills as appropriate
AFMC document considered to me a minimum standard throughout

Process Part 2
Reorganized list to categories with similar properties
Interviewing and Record-keeping
Physical Exam
Procedural
Clinical Reasoning
Diagnostic Testing
Separation of Essential Clinical Presentations
Many “skills” from the master list were felt to represent ECP’s
Removed but recorded

Process Part 3
Describing incremental learning
Several taxonomies considered
Miller
Bloom
Dreyfus
AFMC
Modified AFMC taxonomy used
Maps directly to AFMC for procedural skills
4-point scale modified for non-procedural skills for consistency
Supplemented with RIME for interviewing and record-keeping

Performance Level
Expectation
Level 1: Describe the elements of the interview
Level 2: Perform with guidance
Level 3: Perform successfully independently in a
straightforward situation
Level 4: Perform successfully independently in a complex
environment/situation
Skill End of Med 2
Oral Case Presentation R- 4 I- 3
M- 2 E- 1
Interviewing and Record-keeping
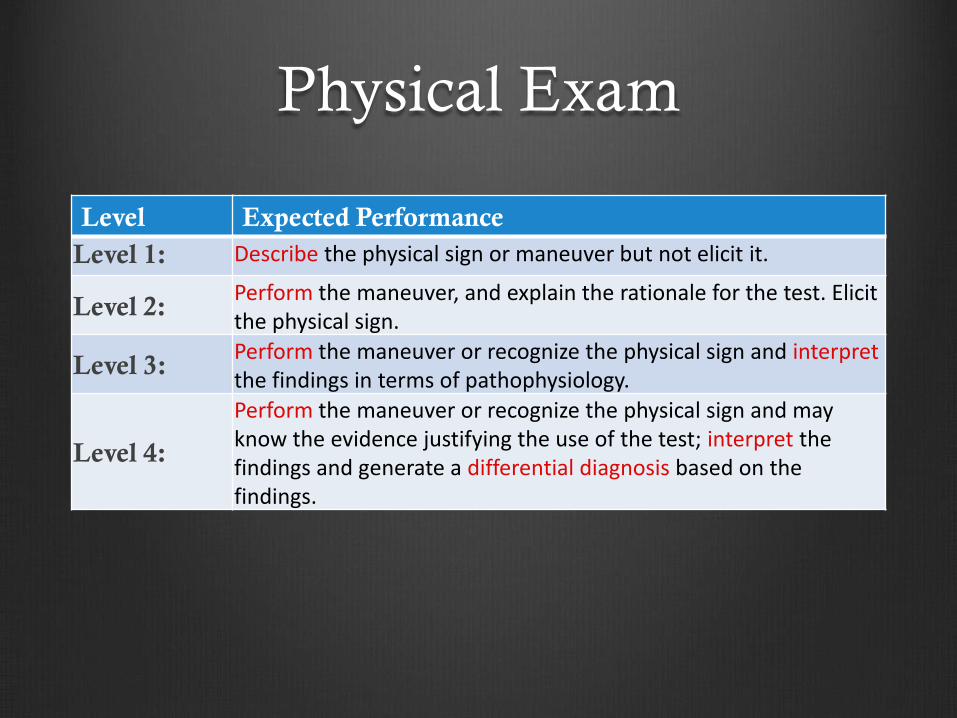
Physical Exam
Level Expected Performance
Level 1: Describe the physical sign or maneuver but not elicit it.
Level 2: Perform the maneuver, and explain the rationale for the test. Elicit the physical sign.
Level 3: Perform the maneuver or recognize the physical sign and interpret the findings in terms of pathophysiology.
Level 4:
Perform the maneuver or recognize the physical sign and may know the evidence justifying the use of the test; interpret the findings and generate a differential diagnosis based on the findings.

Procedural
Level Expected Performance
Level 1: Describe the indications, contraindications, risks, common
complications and the process of the procedure
Level 2: Perform the procedure under supervision in a non-clinical
setting (e.g. simulated set-up)
Level 3: Perform the procedure in a stable patient under supervision in
a controlled clinical setting
Level 4: Perform the procedure in a stable patient without supervision
in a controlled clinical setting

Clinical Reasoning Level Expectation
Level 1: Describe the elements of the interview
Level 2: Perform with guidance
Level 3: Perform successfully independently in a
straightforward situation
Level 4: Perform successfully independently in a complex
environment/situation

Diagnostic Testing Level Expectation
Level 1: Describe the approach to interpretation
Level 2: Demonstrate an orgaized approach to interpretation of the test
Level 3: Identify and interpret the physiologic significance of abnormal findings
Level 4: Identify the key diagnostic findings for the test in all of the Essential Clinical presentations

General Principles for Reform
Spiral Curriculum
Deliberate Practice and Reflection
Utilize multiple learning experiences
Design good goals and objectives
Provide teacher development
Student engagement
Orientation
Ongoing curriculum development

Timing and Structure
Synchrony with knowledge curriculum
Ideal but not completely possible
Clinical Reasoning
Core of the organization for clinical skills
Reflection on fully developed cases through Med 1
Through second year introduce
Increasing complexity and information seeking in virtual cases
actual Hx Px into cases using structured and unstructured Pts
Progress through RIME levels in structured + unstructured CPA’s
Add in other skills as appropriate to support reasoning
Recommendation 1 Timing and structure
Attempt to coordinate skills sessions with the related
knowledge curriculum
Build an incremental clinical reasoning curriculum with the
other clinical skills interposed at appropriate points
Introduce complex skills in a spiral and developmental
course structure
Recommendation 2 Foster deliberate practice and reflection
Provide structured sessions in skills lab with guided reflection
Create print and web-based modules for procedural skills
and/or physical exam skills for self-study
Provide self-directed access to skills training models and
modules for reinforcing self-study
Utilize a log of ECP’s and clinical skills that incorporates
some degree of preceptor feedback and learner reflection

Recommendation 3 Multiple methodologies
Most skills should be taught in multiple ways over multiple
exposures, with gradual integration into more comprehensive
real or simulated patient care events

Recommendation 4 Introduce clinical exposures
Introduce actual patient exposures into training at multiple
levels with goals and objectives aimed at the level of the
trainee.

Recommendation 5 Teacher development
Create formal teacher development programs for
Deliberate practice and reflection
Provision of feedback
Goals and Objectives of sessions
Create and disseminate appropriate goals and objectives for
all sessions
Create a structure/approach for recognition and
development of teachers

Recommendation 6 Clerkship Sessions
Create specific sessions with structured patient encounters or
focused real patient sessions to reinforce communication, basic
interview and exam skills as well as advanced clinical reasoning

Recommendation 7 Student Orientation
Create web-based orientation material for
overall course structure
goals and objectives
general milestones for progress
principles guiding curriculum
Provide a specific session to inform students of orientation
material, emphasize principles of deliberate practice and
promote active participation

Recommendation 8 Continuous Improvement
Include a prospective plan for reassessment and improvement with
specific timelines using student and faculty feedback

















