PLEASE SCROLL DOWN FOR ARTICLE 7KLV DUWLFOH ZDV GRZQORDGHG E\ >&XUWLQ 8QLYHUVLW\ /LEUDU\@ 2Q -XO\ $FFHVV GHWDLOV $FFHVV 'HWDLOV >VXEVFULSWLRQ QXPEHU @ 3XEOLVKHU 5RXWOHGJH ,QIRUPD /WG 5HJLVWHUHG LQ (QJODQG DQG :DOHV 5HJLVWHUHG 1XPEHU 5HJLVWHUHG RIILFH 0RUWLPHU +RXVH 0RUWLPHU 6WUHHW /RQGRQ :7 -+ 8. 3V\FKRWKHUDS\ 5HVHDUFK 3XEOLFDWLRQ GHWDLOV LQFOXGLQJ LQVWUXFWLRQV IRU DXWKRUV DQG VXEVFULSWLRQ LQIRUPDWLRQ KWWSZZZLQIRUPDZRUOGFRPVPSSWLWOHaFRQWHQWW &OLQLFDO VXSHUYLVLRQ ,WV LQIOXHQFH RQ FOLHQWUDWHG ZRUNLQJ DOOLDQFH DQG FOLHQW V\PSWRP UHGXFWLRQ LQ WKH EULHI WUHDWPHQW RI PDMRU GHSUHVVLRQ 0DWWKHZ %DPEOLQJ D 5REHUW .LQJ D 3DWULFN 5DXH E 5REHUW 6FKZHLW]HU F :DUUHQ /DPEHUW G D 8QLYHUVLW\ RI 4XHHQVODQG E &RUQHOO 8QLYHUVLW\ F 4XHHQVODQG 8QLYHUVLW\ RI 7HFKQRORJ\ G 9DQGHUELOW &HQWHU IRU (YDOXDWLRQ DQG 3URJUDP ,PSURYHPHQW 7R FLWH WKLV $UWLFOH %DPEOLQJ 0DWWKHZ .LQJ 5REHUW 5DXH 3DWULFN 6FKZHLW]HU 5REHUW DQG /DPEHUW :DUUHQ &OLQLFDO VXSHUYLVLRQ ,WV LQIOXHQFH RQ FOLHQWUDWHG ZRUNLQJ DOOLDQFH DQG FOLHQW V\PSWRP UHGXFWLRQ LQ WKH EULHI WUHDWPHQW RI PDMRU GHSUHVVLRQ 3V\FKRWKHUDS\ 5HVHDUFK ٢ 7R OLQN WR WKLV $UWLFOH '2, 85/ KWWSG[GRLRUJ Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.
SUMMARY: 127 clients; 127 Therapists; 40 supervisors.training provided for problem solving therapy (PST) supervision vs no supervision group (randomised): supervised group superior in 1. alliance ratings 2. lower BDI scores at post-test 3. client satisfaction 4. higher retention note: only 8 supervision sessions- possible allegiance to supervision group that might inflat results
Clinical supervision: Its influence on client-rated working alliance andclient symptom reduction in the brief treatment of major depression
MATTHEW BAMBLING1, ROBERT KING1, PATRICK RAUE2, ROBERT SCHWEITZER3,
& WARREN LAMBERT4
1University of Queensland, 2Cornell University, 3Queensland University of Technology, and 4Vanderbilt Center for Evaluation
and Program Improvement
(Received 29 January 2004; revised 28 February 2005; accepted 8 March 2005)
AbstractSupervision of psychotherapists and counselors, especially in the early years of practice, is widely accepted as beingimportant for professional development and to ensure optimal client outcomes. Although the process of clinical supervisionhas been extensively studied, less is known about the impact of supervision on psychotherapy practice and client symptomoutcome. This study evaluated the impact of clinical supervision on client working alliance and symptom reduction in thebrief treatment of major depression. The authors randomly assigned 127 clients with a diagnosis of major depression to 127supervised or unsupervised therapists to receive eight sessions of problems-solving treatment. Supervised therapists wererandomly assigned to either alliance skill!/ or alliance process!/focused supervision and received eight supervision sessions.Before beginning treatment, therapists received one supervision session for brief training in the working alliance supervisionapproach and in specific characteristics of each case. Standard measures of therapeutic alliance and symptom change wereused as dependent variables. The results showed a significant effect for both supervision conditions on working alliance fromthe first session of therapy, symptom reduction, and treatment retention and evaluation but no effect differences betweensupervision conditions. It was not possible to separate the effects of supervision from the single pretreatment session and ispossible that allegiance effects might have inflated results. The scientific and clinical relevance of these findings is discussed.
Clinical supervision has traditionally been consid-ered an important part of training and the profes-
sional development of therapists, being rated highly
in the experience of trainees as well as practitionersin the field (Orlinsky, Botermans, & Ronnestad,
2001; Steven, Goodyear, & Robertson, 1998).
Bernard and Goodyear (1992) found that therapistsassessed supervision as an indispensable training
activity that increased both self- and therapeutic
awareness. Further, therapists have rated supervisionhighly as an educational procedure that develops
treatment skills and professional competency (Ste-
ven et al., 1998).In Australia, supervision is considered an impor-
tant posttraining professional activity and is not
restricted to the graduate training setting. Duringsupervision, a supervisor and therapist may system-
atically examine case-specific treatment and process
issues as a method of enhancing both therapistawareness and skills necessary to manage the com-
plexities of client work. Within the practice of
psychotherapy and counseling, there is the expecta-tion that supervision might enhance the clinical
impact of therapeutic intervention. Therefore, a
supervised therapist might reasonably expect toachieve greater clinical outcomes in client work
than an unsupervised therapist (Steven et al., 1998).The proposition that supervision is a procedure
that can enhance client outcome appears to be anassumption based on its historical importance in the
training and practice of psychotherapy and has not
been subject to adequate empirical investigation.There have been 32 published reviews of empirical
studies of clinical supervision and counselor trainingsince 1988 (Bambling & King, 2000); most conclude
that, although we know a lot about the process and
characteristics of supervision, particularly in thegraduate training setting, little empirical evidence
exists regarding the effect of supervision on achiev-
ing measurable clinical outcomes for clients. Generalcriticism of the supervision literature includes pro-
blems of inadequate power, poor methodology, Type
Correspondence: Matthew Bambling, Department of Psychiatry, University of Queensland, Mental Health Centre, K Floor, RoyalBrisbane Hospital, Herston, Queensland 4029, Australia. E-mail: [email protected]
Psychotherapy Research, May 2006; 16(3): 317!/331
ISSN 1050-3307 print/ISSN 1468-4381 online # 2006 Society for Psychotherapy Research
DOI: 10.1080/10503300500268524
Downloaded By: [Curtin University Library] At: 10:05 19 July 2010
darylchow
darylchow
darylchow
I and II errors, and an absence of outcome research(Bambling & King, 2000; Ellis, Ladany, Krengel, &Schult, 1996; Holloway, 1996; Watkins, 1998).
However, the existing supervision research pro-vides four reasonably robust findings that suggestsupervision has the potential to enhance measurableclient symptom outcome: (a) A positive supervisoryrelationship increases supervisee tendency to modeland accommodate observed supervisor therapeuticskills and may enhance supervisee’s demonstrationof the same therapeutic skills in client work (Pierce &Schauble, 1971; Schacht, Howe, & Berman, 1989);(b) supervision reduces supervisee anxiety and roleambiguity and enhances confidence in counselingpractice (Friedlander, Keller, Peca-Baker, & Olk,1986; Kennard, Stewart, & Gluck, 1987); (c) super-vision contributes to the development of basiccounseling skills, although its impact on the devel-opment of more complex counseling skills is unclear(Lambert & Ogles, 1997); (d) supervision may assisttherapists to manage working alliance and resolvetherapeutic impasses (Alpher, 1991; Patton & Kiv-lighan, 1997).
Although this evidence suggests that supervisionmight have the potential to enhance client symptomoutcome in therapy, the research focus to date hasbeen on the impact of supervision on supervisoryalliance, therapist approach, confidence, and coreskills rather than on clearly defined client outcomessuch as symptom reduction (Bambling & King,2000; Ellis et al., 1996, Ladany, Ellis, & Fridlander,1999). However, the general focus of the existingresearch allows some speculation regarding twopossible pathways of action for supervision on clientoutcome. Two pathways are of particular interest;supervision may enhance clinical outcomes forclients by influencing the working alliance betweentherapist and client (Patton & Kivlighan, 1997) andmay provide a method of training therapists how tomanage interpersonal processes in therapy (Lambert& Ogles, 1997).
The working alliance represents a usable super-vision construct because it is measurable and has arobust relationship with symptom improvement andquality of therapeutic work (Horvath & Bedi, 2002;Martin, Garske, & Davis, 2000). Utilizing super-vision to enhance therapists’ use of alliance manage-ment techniques is consistent with evidence thattherapist training can have a positive effect on client-rated working alliance (Hilsenroth, Ackerman,Clemence, Strassie, & Handler, 2002).
In the treatment of depression, client-rated work-ing alliance appears to have an independent effect onclient outcome and predicts client outcome betterthan form of therapy in the psychological treatmentof depression. Specifically, early client working
alliance scores appear particularly predictive of lateralliance scores, client retention in therapy, and clientsymptom reduction scores in the treatment ofdepression (Horvath & Bedi, 2002; Krupnick,Stotsky, Simmens, & Moyer, 1996). Likewise, poorclient-rated working alliance in therapy relates topoorer outcomes and greater rates of client non-completion in therapy (Bambling & King, 2001;Kivlighan & Schmitz, 1992; Patton & Kivlighan,1997). Clients with depression are a suitable targetgroup to test an alliance-focused supervision ap-proach because of the sensitivity of depression toalliance effects.
A popular pantheoretical concept of workingalliance was developed by Bordin in the late 1970s(Bordin, 1994) and operationalized as a researchinstrument by Horvath and Greenberg (1989). Thisview of working alliance provides discrete subcate-gories of alliance behavior: bond, task, and goal.Bordin (1983) believed that this pantheoreticaldefinition of working alliance was ideally suited asa generic supervision approach that might enhancealliance in therapy.
It might reasonably be expected that an alliance-focused supervision approach could be used tostrategically enhance client perception of workingalliance. In a disorder such as depression, in whichclient-rated working alliance and symptom outcomeappear strongly related, increased client-rated work-ing alliance might provide the mechanism by whichsupervision may enhance client symptom outcome.
In view of an absence of empirical data concerningthe kind of supervision most likely to promotetherapist behavior that advances alliance, we decidedto test two different supervision approaches. Thesewere derived from two dominant traditions inpsychotherapy and psychotherapy supervision. Inone approach, the supervisor focused on the devel-opment of therapist skills thought to enhancealliance (alliance skill focus). In the other, thesupervisor focused on therapist awareness of andsensitivity to the therapeutic relationship (allianceprocess focus).
We hypothesized the following:
Hypothesis 1: Clients who receive supervisedtherapy for major depression will demonstratehigher working alliance scores compared with acontrol group of clients who receive the same typeof therapy but from unsupervised therapists.
Hypothesis 2: Clients receiving supervised therapyfor depression will demonstrate a greater reduc-tion of Beck Depression Inventory (BDI) scores,assessed at treatment end, compared with a
318 M. Bambling et al.
Downloaded By: [Curtin University Library] At: 10:05 19 July 2010
control group of clients who receive the same typeof therapy but from unsupervised therapists.
Hypothesis 3: Clients receiving supervised therapywill evaluate their treatment more positively com-pared with a control group of clients who receivethe same type of therapy but from unsupervisedtherapists.
Hypothesis 4: Clients receiving supervised therapywill be more likely to complete treatment com-pared with a control group of clients who receivethe same type of therapy but from unsupervisedtherapists.
Hypothesis 5: The supervision process approachthat focuses on creating awareness of interpersonalprocesses to manage working alliance in therapywill demonstrate different client working alliancescores and reduction of BDI scores at treatmentendpoint than skill-focused supervision proce-dures that focus on behavioral strategies to man-age the working alliance.
Method
Design
This study used a nested design with multipleintervals of measurement. The experimental variablewas supervision; levels were process-focus condition(n"/34), skill-focus condition (n"/31), and no-supervision condition (n"/38). Dependent variableswere client-rated working alliance in therapy (mea-surement points at Sessions 1, 3, and 8), clientsymptom scores (measurement at intake assessmentand Sessions 1 and 8), dropout before completion ofa full course of treatment, and satisfaction withtherapy. The clinical intervention was a standardizedtherapy approach (eight sessions of problem-solvingtreatment; PST) that did not vary across conditions.This study received full review and approval fromthe Behavioural and Social Sciences Ethical ReviewCommittee University of Queensland, Australia.
Participant nesting in the experimental design was1:1 therapist (n"/38) treating clients (n"/38) in theunsupervised condition and 1:1:1 proposed super-visors (n"/65) supervising therapists (n"/65) andtreating clients (n"/65) in both skill- and process-focused conditions. This requirement for eachparticipant to be involved in only one treatmentcondition was to ensure independence of cases andavoid a clustering effect. However, because ofresource implications, target supervisor numberscould not be achieved. To address the short fall insupervisor number the first author supervised anequal number of the therapist cohort in each
13); process focus supervision (n"/13). The remain-ing supervisors supervised (n"/19) skills focus con-dition and (n"/20) in the process focus condition.To evaluate researcher-provided supervision fordifferential effects on Working Alliance Inventory(WAI) scores, an analysis of variance (ANOVA) wasconducted with the supervision provided by theresearcher and all other supervision cases as twogrouping variables. Researcher-provided supervisionhad no effect on either WAI (p"/.498) or BDI (p"/
.428) scores. As a result, the assumption of noclustering effect was maintained for purposes of thedata analysis (see Table I for results). Becausesupervision may affect variances as well as means,we performed Levene tests to determine whether thehomogeneity of variance assumptions for ANOVAwas met (see Results section).
PST is an evidence-based brief counseling ap-proach with treatment effectiveness equivalent toantidepressant medication (Mynors-Wallis & Gath,1996; Mynors-Wallis, Gath, Day, & Baker, 2000).PST is a simplified form of traditional problem-solving therapy (Nezu, Nezu, & Perri, 1989), whichprobably derives its effectiveness through activationof common factors, because there is no evidence thatsolutions or problem mastery are specific mediatingvariables (Mynors-Wallis, 2002). PST was chosenfor this study because it can be taught to therapists ina short period of time, and it is likely that treatmenteffects are more sensitive to alliance that treatmenttechnique. Like traditional problem-solving therapy,there are three main steps in delivering PST: (a)Client symptoms are linked with problems; (b), theproblems are defined, clarified, and prioritized, and(c) systematic structured procedures are used to findand test solutions to problems (Mynors-Wallis &Gath, 1997).
Supervision condition: skill and process foci
Working alliance process-focus and working allianceskill-focus supervision manuals were developed forthis study.
Process focus. In the process supervision condition,case discussion focused on assisting therapists todevelop an understanding of the interpersonal dy-namics occurring during the therapy. Supervisioncase discussions focused on monitoring implicitclient feedback, changes in client anxiety level, flowof exchanges, resistance, and perceived dynamics inthe relationship with the therapist. It was expectedthat increased therapist awareness of the interperso-nal processes within the therapy as impacting onalliance would assist therapists to make adjustments
Effect of clinical supervision in treatment of major depression 319
Downloaded By: [Curtin University Library] At: 10:05 19 July 2010
Daryl Chow
in their approach toward clients that would enhancethe alliance. Therapists in this condition were not,however, given specific recommendations for alli-ance-promoting behavior.
Skill focus. In the alliance skill-focus condition,therapists were assisted to apply counseling behaviorsto enhance client experience of bond, task, and goals.Supervision case discussion was used to identifyclient behaviors or characteristics likely to hinder oradvance therapy by examining explicit client feed-back from session to session, satisfaction with ther-apy, level of comfort with the therapist, and clarity oftherapy goals and client tasks. Unlike the allianceprocess condition, therapists were given explicitadvice and guidance concerning the kinds of beha-viors and interventions likely to enhance alliance.
Eight sessions of supervision were provided tomatch the number of therapy sessions. The firstsession was provided pretreatment, and the remain-ing sessions occurred after each of the first sevenclient therapy sessions.
Supervision pretreatment meeting
Therapists allocated to supervised conditions wererequired to attend a pretreatment supervision meet-ing with their supervisor during which they wereoriented to the supervision model. The training
component of the pretreatment session consisted ofsupervisors instructing therapists in early alliancemanagement principles described in the supervisionmanual. In the supervision component of the pre-treatment session, supervisors and therapists dis-cussed characteristics of the case with an emphasison applying alliance management principles. Super-visors and therapists had access to client assessmentinformation and histories.
Participants
Supervisors. Supervisors were volunteers recruitedthrough private practices, mental health services,and journal advertisement. Supervisors were notpaid for participation but were given free trainingaccredited by the University of Queensland, Depart-ment of Psychiatry, in the supervision approach inreturn for participating in the study. Participantscould use the accredited training for continuingeducation (CE) points or for other professionalpurposes. Written informed consent was obtainedfrom supervisors after the purpose and procedures ofthis study were explained both verbally and throughthe provision of a written information sheet.
The minimum supervisor requirements were grad-uate qualifications in a recognized mental healthdiscipline and 2 years of experience providing super-vision. Forty supervisors (31 women and nine men)
Table I. Analysis of pretreatment group differences.
Downloaded By: [Curtin University Library] At: 10:05 19 July 2010
Daryl Chow
Daryl Chow
were recruited and provided supervision to thera-pists in this study. The average age of supervisorswas 49.9 years (SD"/9.4, range"/34!/67 years).Seven (17.5%) supervisors had a doctorate degree;16 (40%) a master’s degree in psychology; 10 (25%)a master’s degree in psychotherapy; and three(7.5%) a master’s degree in social work; two (5%)were registration-level psychologists; one (2.5%) hada social work degree; and one (2.5%) was a mentalhealth graduate in other disciplines. Supervisors hada mean experience level of 11.2 years (SD"/4.2,range"/2!/20 years).
Supervisors were trained in two separate groupsaccording to expressed preference for the skill orprocess supervision approach. Most training wasconducted at the Department of Psychiatry, Uni-versity of Queensland, situated at a large publichospital. Training took the form of a 1-day work-shop. At the completion of training, supervisors wereassessed in the use of skill or process supervisionmanuals against competency criteria based on super-vision role-plays. A rating of competency was part ofthe selection criteria for participation as a supervisorin this study.
Therapists. Volunteer therapists were recruitedthrough media and journal advertisement. Thera-pists were not paid but were given free accreditedtraining in PST in return for participating in thestudy. Participants could use the accredited trainingfor CE points or for other professional purposes.Written informed consent was obtained from thera-pists after the purpose and procedures of this studywere explained both verbally and through the provi-sion of a written information sheet.
Minimum therapist requirements were graduatequalifications in mental health and 1 year of graduateexperience providing counseling services to clients.Australia does not have a requirement for doctoral-level qualifications in mental health practice. Onehundred twenty-seven therapists (96 women and 31men) were recruited and trained and gave consent toparticipate in this study. Therapist mean age was44.1 years (SD"/10.1, range"/23!/67 years). Six(4.7%) therapists had a doctorate degree, 32 (25%)a registration-level qualification in psychology; 27(21.3%) a master’s degree in psychology, 27 (21.3%)a master’s degree in psychotherapy, nine (7.1%) amaster’s degree in social work, and six (4.7%) asocial work degree; 20 (15.7%) were graduates inother mental health disciplines. Mean therapistexperience was 8.8 years (SD"/5.8, range"/2!/25)providing counseling services.
Seven recruitments and seven 16-hr PST work-shops were conducted over the study period. Allparticipant therapists were required to attend train-
ing and were assessed for competence in using thePST treatment manual. Four volunteer therapistsaccredited in PST assisted the first and secondauthors as cotrainers at workshops. Trainers andcotrainers rated each therapist participant for de-monstrated competency using each stage of PST inworkshop training sessions. A rating of competencyin PSTwas required as part of the therapist selectioncriteria for this study. All potential therapists wereaware that after training they would be allocated toeither an unsupervised or a supervision condition.Participants were not made aware of the skill!/
process focus of supervision.
Clients. Client participants were recruited throughlocal mental health networks and media advertising.Treatment was provided free of charge to participat-ing clients, and they would typically attend therapysessions at rooms provided by the Department ofPsychiatry. Written informed consent was obtainedfrom clients after the purpose and procedures of thisstudy were explained both verbally and through theprovision of a written information sheet. Appropriatealternate referrals were made for those not meetingthe inclusion criterion.
The inclusion criterion for clients was a primarydiagnosis of major depression made by the firstauthor using a clinical interview conducted inaccordance with the Mini International NeurologicalInventory (MINI; Sheehan & Lecrubier, 1998) andthe BDI (Beck, Steer, & Garbin, 1987) as an initialscreen. Comorbidity along Axis I and Axis II of theDiagnostic and Statistical Manual of Mental Disorders(4th ed.; DSM!/IV; American Psychiatric Associa-tion, 1994) was tolerated as long as major depressionwas the primary diagnosis.
Existing medication users were accepted into thisstudy because preexisting antidepressant use has notbeen shown to either enhance or detract from positivetreatment outcome in cognitive!/behavioral therapy(Oei & Yeoh, 1999). Antidepressant use was basis forexclusion if started at the time of intake because itmight confound the interpretation of gains made intreatment. Clients starting medication at intake werereferred or rescheduled for another intake assessmentlater in the study period depending on their needsand interests. Potential clients were excluded fromparticipation if depression was not the primarydiagnosis and on the basis of antisocial personalitydisorder, active suicidality, psychosis, or incapacity tounderstand or conform to assessment or treatmentrequirements. A management protocol, includingspecialized mental health referral, was developed todeal with potential participants not meeting theinclusion criteria and participant clients who mightdeteriorate during treatment.
Effect of clinical supervision in treatment of major depression 321
Downloaded By: [Curtin University Library] At: 10:05 19 July 2010
Daryl Chow
Daryl Chow
Daryl Chow
Daryl Chow
After recruitment and assessment, 127 clients (87women and 40 men) participated in the study. Themean client age was 39.1 years (SD"/12.0, range"/
18!/67 years). Forty-two (33.1%) clients had a highschool or equivalent education, 24 (18.9%) post-high school or trade/technical qualifications, and 61(48%) university qualifications. Twenty-four(18.9%) clients were current users of antidepressantmedication (typically selective serotonin reuptakeinhibitors), whereas 103 (81.1%) were not usingmedication for depression.
Sixty-six clients (52%) had a diagnosis of majordepression only. For the remaining client popula-tion, primary comorbidity included agoraphobia(n"/4; 3.1%), social phobia (n"/5; 3.9%), ob-sessive!/compulsive disorder (n"/5; 3.9%), general-ized anxiety disorder (n"/33; 26%), and panicdisorder (n"/14; 11%). Primary Axis II diagnosisrevealed avoidant personality disorder (n"/5; 3.9%),dependent personality disorder (n"/3; 2.3%), ob-sessive!/compulsive personality disorder (n"/1;0.8%), passive!/aggressive personality disorder(n"/3; 2.3%), self-defeating personality disorder(n"/3; 2.3%), narcissistic personality disorder (n"/
2; 1.5%), and borderline personality disorder (n"/3;2.3%). Whereas most clients had a satisfactory levelof health, seven reported poor health: ill health (n"/
All therapists were provided with a therapist packthat included the treatment manual, study measures,and blank audiotapes individually packaged andmarked with instructions for use. A booklet wasincluded that provided detailed instruction for theuse of all measures in accordance with the studyschedule and all study protocols.
All supervisors were provided with a supervisionpack that included the supervision manual andindividually packaged measures and detailed instruc-tions for session usage. A booklet was included in thesupervisor pack that provided an overview of thesupervision assessment, detailed instruction in theiruse, and a detailed description of the therapist studyschedule and all study protocols.
In addition, both supervisors and therapistswere instructed in the use of these packs and theadministration of all supervision- and therapy-relatedassessment as part of respective training workshops.
Allocation of study participants
Recruitment of clients and therapists was continualthroughout this study. Participants were assigned
random numbers on induction. Clients were ran-domly allocated to unsupervised or supervised skillor process conditions, with the secondary randomallocation of therapists to unsupervised or super-vised process and skill supervision conditions on acontinual bases until cell sizes were achieved (Sher-idan, 1979).
Supervisors were matched to either skill or processsupervision conditions. A matched approach tosupervisor allocation maximized consistency ofsupervision approach by the removal of variabilityresulting from differences in experience or signifi-cant preexisting variations in style by supervisors.
Data analysis
This study used repeated measures of client workingalliance scores and self-rated depression in a nesteddesign. Repeated measures ANOVA was conductedto evaluate the effect of supervision on ratings ofclient working alliance (WAI) and outcome (BDI)across treatment measurement intervals. Within-subject variables were Assessment Intervals 1, 3,and 8, and the between-subject variables were super-vision condition. Dependent variables were WAI andBDI and treatment evaluation scores.
Measures
Intake assessment: pretherapy. The MINI!/5 wasused as the principal instrument guiding the clinicalinterview to diagnose depression and comorbidityalong Axis I. The MINI was designed as a briefstructured interview for the major Axis I psychiatricdisorders in DSM!/IV and International Classifica-tion of Diseases (10th ed.). Validation and reliabilitystudies have demonstrated that the MINI is com-parative to the Structured Clinical Interview forDSM (SCID-P) and the CIDI (Composite Interna-tional Diagnostic Interview) and can be adminis-tered in a much briefer period of time (Sheehan &Lecrubier, 1998).
The BDI is a 21-item inventory that is widely usedto assess depression severity. It has high internalconsistency and correlates highly with other self-report measures of depression and with clinicians’ratings of depression (range"/.60!/.90; Beck et al.,1987).
Axis II diagnosis was assessed using the SCIDscreen and formal diagnostic interview. The SCIDhas demonstrated fair to good median interraterkappa (.40!/.75) based on test and retest reliabilitystudies (Zanarini et al., 2000).
The Social Skills Inventory (SSI) was included tocontrol for therapists’ preexisting capacity to form aworking alliance with clients (Crowley, 2000). The
322 M. Bambling et al.
Downloaded By: [Curtin University Library] At: 10:05 19 July 2010
darylchow
SSI is a 90-item instrument designed as a self-reportmeasure to assess basic verbal and nonverbal socialcommunication skills in adults and has high subscalereliability. Total scale reliability is a"/.94 (Riggio,1986). SSI results are reported in Table I.
Assessment during therapy. In this study the BDIwas administered at intake, immediately beforeTreatment Session 1, and immediately at the com-pletion of Session 8 (endpoint).
The WAI is a 36-item inventory rated on a 7-pointLikert scale made up of three alliance subscalesassessing bond, task, and goal. Internal consistencyof the whole scale is high (range"/.87!/.93) as it isfor the subscales (.92 for bond, .92 for task, and .89for goal; Horvath & Greenberg, 1989). In this studyonly client-rated WAI scores for Sessions 1, 3, and 8are reported.
The Treatment Evaluation Scale is designed toprovide a simple subjective client evaluation ofsatisfaction with treatment and is not intended tobe a measure of treatment impact. The scale ratessatisfaction with therapy along five items on a 5-point scale administered at the end of therapy. Itemsinclude degree that counseling met needs, (b) degreethat counseling assisted with problems, (c) satisfac-tion with time allotted, (d) satisfaction with treat-ment, and (e) desire for same treatment again. Noreliability properties have been reported by Scott andFreeman (1992).
Therapists completed a PST adherence scale thatmeasured the degree of conformity to the therapyapproach. Two external raters unaware of super-vision conditions rated and rerated therapist PSTadherence using audiotapes of the therapy sessions.The PST adherence scale used in this study wasdeveloped directly from the clinical steps of PSTandsuccessfully used in PST training workshops toassess all therapists for accreditation. It consistedof six items on a 7-point Likert-type scale.
Supervisors used a Supervision Focus AdherenceScale (SFAS) developed for this study to self-rateskill- and process-focus adherence in this study attreatment-supervision endpoint. The SFAS contains20 items providing separate subscale scores for skilland process focus in supervision. The SFAS demon-strated moderate total scale reliability (a"/.70) andhigh subscale reliability for skill (a"/.97) and process(a"/.92) focus of supervision.
Results
Twenty-four clients (18.9%) who did not completethe full course of therapy were excluded from themain analysis to minimize the effect of missing dataon sample size, leaving 103 completed cases. Nine
clients left therapy after Session 1, eight after Session2, four after Session 3, two after Session 6, and oneafter Session 7.
Preintervention group differences
Chi-square analysis and ANOVA were used toinvestigate group differences (process supervisionvs. skill supervision vs. no supervision) in respectto client demographic or pretreatment clinical scoresor therapist variables. No differences were found.Table I reports pretreatment variables betweensupervised and unsupervised conditions.
Homogeneity of variance in WAI and BDIscores
Variance of end-of- treatment client-ratedWAI scoreswas greater for the unsupervised clients (SD"/25.1)than for the process supervision clients (SD"/19.7)or the skill supervision clients (SD"/18.3). Accordingto Levene’s test of equity of error variance, thisdifference was significant, F(2, 100)"/4.2, pB/ .05.Variance of end-of-treatment BDI scores was greaterfor the unsupervised clients (SD"/9.2) than for theprocess supervision clients (SD"/7.2) or the skillsupervision clients (SD"/6.7). According to Levene’stest of equity of error variance, this difference wassignificant, F(2, 121)"/4.3, pB/.05. Because AN-OVA is robust with respect to heteroscedasticity,these differences were not considered to be ofsufficient magnitude to result in spurious results.
Client-rated working alliance scores
Repeated measures ANOVA revealed that client-rated WAI scores increased over the duration of thetreatment, F(2, 99)"/22.37, pB/.01 (Table II).Pairwise comparisons with Bonferroni correctionsrevealed a significant increase in mean WAI score(6.9-point change, pB/.01) between Sessions 1 and3 and a further significant increase (6.1-pointchange, pB/.01) between Sessions 3 and 8. Therewas a significant main effect for supervision on thetransformed WAI average across measures, F(2,100)"/54.9, pB/.01. The interaction between super-
Table II. Mean client-rated WAI scores across treatment.
Effect of clinical supervision in treatment of major depression 323
Downloaded By: [Curtin University Library] At: 10:05 19 July 2010
vision condition and WAI measurement session wasnonsignificant, F(4, 198)"/0.882, p"/.476.
Differences among the process supervision group,skill supervision group, and no-supervision groupwith respect to average WAI scores across the threerepeated measures were investigated with pairwisecomparisons, using Bonferroni corrections, of theestimated marginal means. This analysis revealedthat estimated marginal WAI means of both super-vision groups (process supervision"/233.9; skillsupervision"/225.5) were higher than that of theno-supervision group (191.6; pB/.01 in each case).The marginal means of the two supervision groupsdid not differ significantly (p"/.221), suggesting nodifference between groups.
Symptoms of depression
Repeated measures ANOVA revealed BDI scores forthe full sample reduced across the repeated mea-sures, F(1, 120)"/330.4, pB/ .01. Pairwise compar-isons with Bonferroni corrections revealed asignificant reduction in mean BDI scores (1.9-pointchange, pB/.01) between intake and pretest and asignificant but much greater reduction (22.3-pointchange, pB/.01) between intake and posttreatment.There was a significant main effect for supervisionon the average BDI score across measures, F(2,100)"/6.8, pB/ .01. There was significant interactionbetween supervision group and change in BDI score,F(4, 242)"/3.9, pB/.01. These scores are repre-sented in Table III, which illustrates lower BDIscores for supervised therapy compared with un-supervised therapy at treatment endpoint.
Differences among the process supervision group,skill supervision group, and no-supervision groupwith respect to changes in mean BDI scores wereinvestigated with pairwise comparisons, using Bon-ferroni corrections, of the estimated marginal meansof posttreatment BDI scores when intake and pre-treatment BDI scores were entered as covariates.This analysis revealed that estimated marginal BDImeans of both supervision groups (process super-vision"/6.3; skill supervision"/8.6) were lower thanthat of the no-supervision group (12.2; pB/.01 in
each case). The marginal means of the two super-vision groups did not differ significantly, suggestingno differences between groups (p"/ .503).
Client treatment evaluation
Univariate ANOVA revealed that client-rated treat-ment evaluation scores differed between groups,F(2, 100)"/13.73, pB/.01. Post hoc group compar-isons using Bonferroni corrections showed that bothsupervision groups had higher treatment evaluationscores (pB/.01) but that there was no significantdifference in effect between skill and process super-vision focus on client evaluation scores (p"/ .617).
Client noncompletion rate
Supervision demonstrated a strong effect on clientattrition rates in this study. Client noncompletionwas defined as failure to complete Session 8 oftherapy. The unsupervised group had higher rate ofclient treatment noncompletion than both super-vised groups, x2(2, N"/127)"/23.83, pB/.01. In theunsupervised group, the proportion of clients notcompleting Session 8 was 21 of 60 (35%); in the skillfocus group, 2 of 33 (6.1%); and in the process focusgroup 1 of 34 (3.0%).
Supervisor skill and process focus adherencescores (SFAS)
Skill-focus and process-focus therapists’ SFAS sub-scale scores were compared using t tests to evaluateself-rated adherence to supervision focus. The pro-cess condition revealed a significant difference be-tween process subscale scores (M"/62.26, SD"/
7.70) and skill subscale scores (M"/42.76, SD"/
12.20), demonstrating the expected effect towardprocess supervision, t(64)"/33.85, pB/.01. The skillcondition revealed a significant difference betweenskill subscale scores (M"/60.54, SD"/8.70) andprocess subscale scores (M"/45.21, SD"/11.67),demonstrating the expected effect toward skill super-vision, t(64)"/30.48, pB/.01. Each supervision ap-proach was equivalent in the degree of adherence totheir respective skill and process conditions, t(64)"/
0.174, p"/.678.
PST adherence
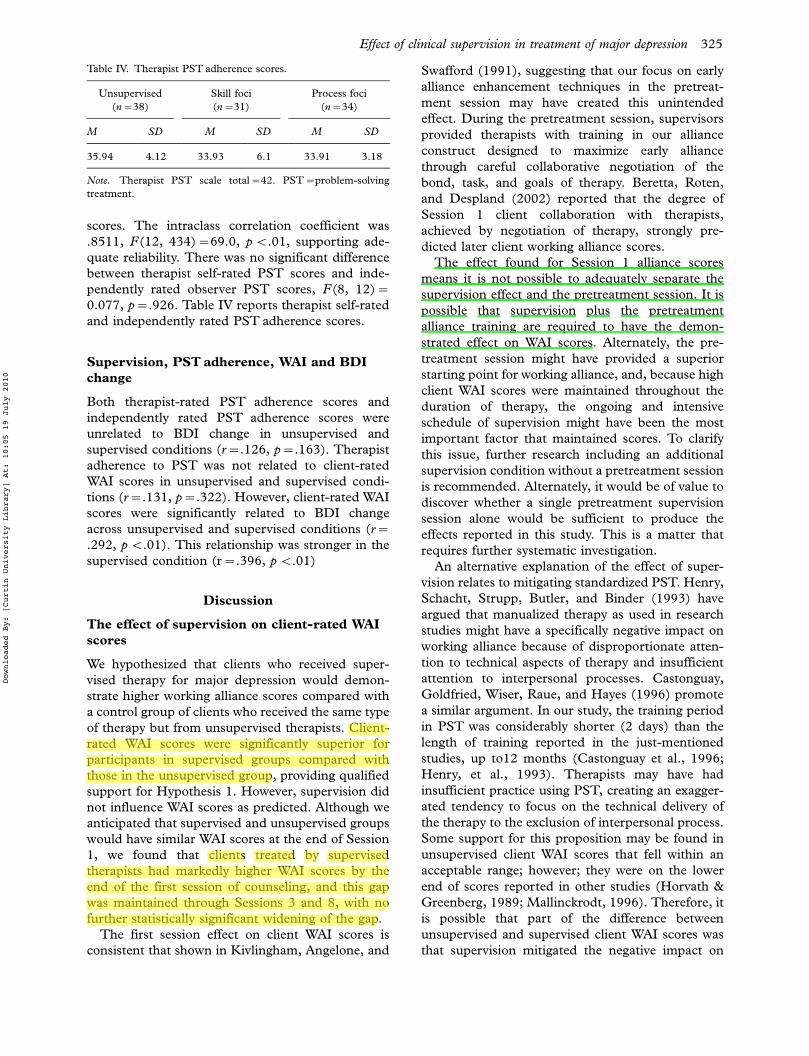
Therapist self-rated and independently rated PSTadherence was satisfactory in all three groups. Therewere no differences in adherence between condi-tions, and supervision did not influence PST adher-ence, F(2, 100)"/1.76, p"/.177.
PST adherence interrater reliability was under-taken on dual independently rated observer PST
Table III. Mean BDI scores pre- and posttreatment.
Both therapist-rated PST adherence scores andindependently rated PST adherence scores wereunrelated to BDI change in unsupervised andsupervised conditions (r"/.126, p"/.163). Therapistadherence to PST was not related to client-ratedWAI scores in unsupervised and supervised condi-tions (r"/.131, p"/.322). However, client-rated WAIscores were significantly related to BDI changeacross unsupervised and supervised conditions (r"/
.292, pB/.01). This relationship was stronger in thesupervised condition (r"/.396, pB/.01)
Discussion
The effect of supervision on client-rated WAIscores
We hypothesized that clients who received super-vised therapy for major depression would demon-strate higher working alliance scores compared witha control group of clients who received the same typeof therapy but from unsupervised therapists. Client-rated WAI scores were significantly superior forparticipants in supervised groups compared withthose in the unsupervised group, providing qualifiedsupport for Hypothesis 1. However, supervision didnot influence WAI scores as predicted. Although weanticipated that supervised and unsupervised groupswould have similar WAI scores at the end of Session1, we found that clients treated by supervisedtherapists had markedly higher WAI scores by theend of the first session of counseling, and this gapwas maintained through Sessions 3 and 8, with nofurther statistically significant widening of the gap.
The first session effect on client WAI scores isconsistent that shown in Kivlingham, Angelone, and
Swafford (1991), suggesting that our focus on earlyalliance enhancement techniques in the pretreat-ment session may have created this unintendedeffect. During the pretreatment session, supervisorsprovided therapists with training in our allianceconstruct designed to maximize early alliancethrough careful collaborative negotiation of thebond, task, and goals of therapy. Beretta, Roten,and Despland (2002) reported that the degree ofSession 1 client collaboration with therapists,achieved by negotiation of therapy, strongly pre-dicted later client working alliance scores.
The effect found for Session 1 alliance scoresmeans it is not possible to adequately separate thesupervision effect and the pretreatment session. It ispossible that supervision plus the pretreatmentalliance training are required to have the demon-strated effect on WAI scores. Alternately, the pre-treatment session might have provided a superiorstarting point for working alliance, and, because highclient WAI scores were maintained throughout theduration of therapy, the ongoing and intensiveschedule of supervision might have been the mostimportant factor that maintained scores. To clarifythis issue, further research including an additionalsupervision condition without a pretreatment sessionis recommended. Alternately, it would be of value todiscover whether a single pretreatment supervisionsession alone would be sufficient to produce theeffects reported in this study. This is a matter thatrequires further systematic investigation.
An alternative explanation of the effect of super-vision relates to mitigating standardized PST. Henry,Schacht, Strupp, Butler, and Binder (1993) haveargued that manualized therapy as used in researchstudies might have a specifically negative impact onworking alliance because of disproportionate atten-tion to technical aspects of therapy and insufficientattention to interpersonal processes. Castonguay,Goldfried, Wiser, Raue, and Hayes (1996) promotea similar argument. In our study, the training periodin PST was considerably shorter (2 days) than thelength of training reported in the just-mentionedstudies, up to12 months (Castonguay et al., 1996;Henry, et al., 1993). Therapists may have hadinsufficient practice using PST, creating an exagger-ated tendency to focus on the technical delivery ofthe therapy to the exclusion of interpersonal process.Some support for this proposition may be found inunsupervised client WAI scores that fell within anacceptable range; however; they were on the lowerend of scores reported in other studies (Horvath &Greenberg, 1989; Mallinckrodt, 1996). Therefore, itis possible that part of the difference betweenunsupervised and supervised client WAI scores wasthat supervision mitigated the negative impact on
Effect of clinical supervision in treatment of major depression 325
Downloaded By: [Curtin University Library] At: 10:05 19 July 2010
darylchow
darylchow
darylchow
alliance of the application of a standardized andrelatively unfamiliar and newly acquired therapeutictechnique.
The primary competing explanation of effect inthis study is participant allegiance to the supervisioncondition. There is evidence that positive therapistallegiance is a predictor of successful therapy out-come (Hollon, 1999; Luborsky et al., 1999) andmight enhance not only the technical characteristicsof therapy but also the working alliance.
Therapists knew that they were randomly assignedto supervised or unsupervised conditions. The resultmight have been to create differences in motivationbetween conditions that may have influenced out-come. Future studies may control for allegiance byaccounting for the level of allegiance as a mediatingvariable.
The high client working alliance scores may alsohave been an indication of commitment to theresearch condition. We do not believe this is highlylikely because therapists were instructed not to telltheir clients if they were in supervised or controlconditions. However, it is possible that, in discussionwith their therapists, enough clients might havebecome aware of their supervised status to creategreater credibility regarding the therapist or thetherapy, resulting in expectancy-like effect. Positiveexpectancy is associated with greater client commit-ment, motivation, and engagement in therapy (Fen-ton, Cecero, Nich, Frankforter, & Carroll, 2001;Lambert & Ogles, 2004).
Supervision and client BDI scores
We hypothesized that clients receiving supervisedtherapy for depression would demonstrate a greaterreduction of BDI scores assessed at treatment endcompared with a control group of clients who receivethe same type of therapy but from unsupervisedtherapists. Hypothesis 2 was supported becauseclients receiving supervised therapy achieved a sig-nificantly greater reduction in BDI scores than thosereceiving unsupervised therapy.
Mean BDI change in the unsupervised conditionwas equivalent to results reported for PST byMynors-Wallis et al. (2000). The mean BDI scoresfor both supervised groups at treatment endpointcorresponded to remitted depression, whereas un-supervised mean scores approached mild depression.Greater numbers of clients in the supervised condi-tion achieved BDI scores that indicated clinicalremission of depression (44 of 65) compared withthe unsupervised therapy condition (18 of 38).
The extent of symptom reduction in supervisedtherapy groups was greater than is usually reportedfor PST. This might suggest that alliance-oriented
supervision can enhance usual treatment effects inPST. If this is the case, then replication is importantto determine whether the supervision effect istransferable across other brief therapies for depres-sion.
Using an objective treatment outcome measure ata posttreatment follow-up point by an independentclinician unaware of condition assignment mightassist in clarifying the relationship between symptomoutcome and supervision (Fenton et al., 2001).
A competing argument to explain the effect ofsupervision on BDI scores might be that supervisionhad the unintended effect of assisting therapists toeffectively apply PST. To counter this argument, it isnecessary to demonstrate that increased workingalliance, and not PST, provided the mechanism ofchange in supervised conditions. Therapist PSTadherence should be independent and unrelated toclient WAI scores and BDI change. Further, higherworking alliance scores should be associated withgreater BDI change in the supervised condition. Theresults of this study provide partial support for thiscontention. PST adherence was unrelated to BDIchange in supervised conditions. WAI scores weresignificantly related to BDI change in both super-vised and unsupervised conditions. The enhancedclient WAI scores in the supervised conditionachieved a substantial increase in the correlation ofthe relationship with BDI change compared with theunsupervised condition. Although this evidence isnot definitive, the current findings provide supportthe idea that higher client WAI scores in thesupervised conditions were the likely mechanism ofenhanced client symptom change.
Client treatment evaluation
Our third hypothesis was that clients receivingsupervised therapy would evaluate their treatmentmore positively compared with a control group ofclients who receive the same type of therapy but fromunsupervised therapists. Hypothesis 3 was sup-ported because supervision had a significant effecton client treatment satisfaction. Clients treated bysupervised therapists were more satisfied than thosetreated by unsupervised therapists. Client satisfac-tion might be regarded not only as an indication oftreatment success but also as an independent mea-sure of treatment effect (Kokotovic & Tracey, 1990;Martin et al., 2000; Piper et al., 1999; Stiles, Agnew-Davies, Hardy, Barkham, & Shapiro, 1998).
In this study, unsupervised therapy treatmentevaluation scores were equivalent to those reportedby Scott and Freeman (1992), indicating an accep-table level of satisfaction with treatment. The strongsupervision effect on treatment satisfaction reported
326 M. Bambling et al.
Downloaded By: [Curtin University Library] At: 10:05 19 July 2010
darylchow
darylchow
darylchow
Daryl Chow
in this study is not surprising given the higherworking alliance scores reported in the groupstreated by supervised therapists. A considerablebody of literature indicates a connection betweenthe strength of working alliance in therapy and clienttreatment satisfaction (Horvath, Gaston, & Lu-borsky, 1995; Horvath & Symonds, 1991; Kokotovic& Tracey, 1990; Martin et al., 2000; Piper et al.,1999; Stiles et al., 1998). However, it is possible thathigh treatment satisfaction scores did not relate tohigh working alliance but were an artifact of theallegiance or expectancy effects discussed previously.
Client treatment retention
We hypothesized that clients receiving supervisedtherapy will be more likely to complete treatmentcompared with a control group of clients who receivethe same type of therapy but from unsupervisedtherapists. The hypothesis was supported becausesupervision had a significant effect on client treat-ment retention. The total client noncompletion ratefor the study cohort was 18.8%, which comparesfavorably to rates found for comparably sized treat-ment cohorts in the cognitive therapy literature fordepression, ranging from 21% to 45% (Organista,Munoz, & Richardo, 1994; Scott & Freeman, 1992).The unsupervised group had a noncompletion rateof 30.6%. Mynors-Wallis et al. (2000) reported aclient noncompletion rate in two PST treatmentgroups of 38.8% and 21.9%. The noncompletionrate for the supervised therapy (6.2%) was lowerthan for the unsupervised therapy and lower than therate reported in previous studies using PST.
Positive client-rated working alliance has beenshown to significantly increase treatment retention.Safran, Muran, Samstag, and Winston (2002) de-monstrated that an alliance-enhanced form of treat-ment called brief relational therapy (BRT) achievedsignificantly greater treatment retention for clientswho had difficulty forming alliances compared withother brief approaches (cognitive!/behavioral ther-apy, short term dynamic therapy). The specific focusof supervision on alliance in the current study mayhave augmented the retention effect by assistingtherapists to better accommodate clients who mayhave had difficulty forming alliances. Regardless ofthe mechanisms of supervision on retention, theseremain important results because the clinical effec-tiveness of treatment is a function of treatmentcompletion as well as treatment efficacy.
Supervision focus, WAI and BDI scores
We hypothesised that, as a result of their differentfocus, supervision process procedures would achieve
different client working alliance scores in therapyand different client BDI scores at treatment end-point than the skill-focused procedures. Despitesatisfactory differentiation of skill and process super-vision approaches, there was no evidence to suggestthat alliance process focus had a greater impact onworking alliance and symptom reduction. The find-ing of equivalency of effect between the skill andprocess foci on both WAI scores and BDI scoresmeans that relational and insight techniques ofalliance management are not superior to cognitiveand behavioral techniques; therefore, the mechan-isms by which supervision enhances alliance andtreatment outcome are not clear. The equivalence ofeffect may indicate that the effectiveness of thissupervision rests on a general focus on alliance orinfluence of common factors.
Limitations of the study
As noted in the Discussion section, the majorlimitation of this study is that it is not possible toseparate the supervision effect from any pretreat-ment session and therapist allegiance effects. Twofurther limitations of this study should be noted.
An a priori power analysis for each plannedstatistical analysis to determine appropriate samplesize before beginning data collection was undertaken(n"/187). The total number of client participantswho completed therapy was 103 divided into threeprovisional cells (M"/34 each). Although providinga moderate sample size, total power was insufficientto ensure that Type II errors could not occur.Second, the study was not designed to detect subtledifferences over time in working alliance, symptomchange, and supervision across the duration oftherapy. The study was designed to detect totaldifferences between groups over time. Therefore,any tensions that were resolved in therapy as a resultof supervision could also have influenced workingalliance and not be reflected in the data. Third, theprincipal researcher in this study undertook asignificant amount of the supervision across bothconditions. Although there was no detectable differ-ence in WAI and BDI scores compared with othersupervisors, it remains possible that researcher-provided supervision might have influenced resultsin some unknown way, reducing detectable effectbetween approaches.
Matters for future research
The strength of effect found in this study providesinitial evidence that supervision can play a role indeveloping the working alliance and enhancingtreatment outcome. The finding of an effect for the
Effect of clinical supervision in treatment of major depression 327
Downloaded By: [Curtin University Library] At: 10:05 19 July 2010
darylchow
darylchow
pretreatment session on early alliance scores suggests
a possible effect for alliance training as an indepen-dent intervention or in conjunction with supervision.
The equivalency of effect for both supervisionapproaches means that results of this study do not
permit conclusions regarding the degree to which the
focus, frequency, and content of supervision areimportant or whether nonspecific factors are respon-
sible for the supervision effect. Nonspecific factors
play a major role in psychotherapy outcome, espe-cially in treatment of depression (King, 1998), and it
is possible that they are equally important in the
effect of supervision.Replication is important to confirm both the
nature and extent of supervision effects. This could
best be done by testing alliance-focused supervision
against a form of supervision that is similar in itsnonspecific attributes, duration and frequency of
contacts, and form of contacts with and without
pretreatment sessions but differs in the content ofcontacts (alliance focus vs. focus on technique of
therapy). Examining these factors will determine the
effect if any, of the technical components of super-vision when provided independent of a working
alliance!/focused approach.
Implications for practice
This is the first time that the relationship betweensupervision and client outcome has been investigated
using a randomized controlled treatment trial meth-
odology. Implications must be viewed with somecaution. However, the results of this study provide
qualified support that supervision that focuses on
working alliance can influence client perception ofalliance and enhance treatment outcome in the brief
psychotherapeutic treatment of depression. At thisstage, there is evidence that both the skill and
process supervision used in this study were able to
effectively achieve these ends. However, it would bepremature to conclude that any form of supervision
or brief training in alliance management would
reliably reproduce the effects reported here.The main effect for this form of supervision
appears to be in its focus on working alliance. To
apply these findings to the practice of clinical
supervision, the implications are that it may beimportant to train supervisors in alliance manage-
ment principles independent of supervisory theory.
The standardized supervision approaches used inthis study may provide a suitable procedure for
training supervisors in the use of alliance manage-
ment techniques.
References
Alpher, V. (1991). Interdependence and parallel processes: A case
study of structural analysis of social behavior in supervision and
and cost after 16 weeks. BMJ , 304 , 883!/887.Sheehan, D., & Lecrubier, Y. (1998). Mini International Neu-
ropsychiatric Interview: English version 5.0.0. Journal ofClinical Psychiatry, 59 , 34!/57.
Sheridan, C. (1979). Methods in experimental psychology. Holt,
Rinehart & Winston.
Steven, D., Goodyear, R., & Robertson, P. (1998). Supervisor
development: An exploratory study in changes in stance and
emphasis. Clinical supervisor , 16 , 73!/88.Stiles, W., Agnew-Davies, R., Hardy, G., Barkham, M., &
Shapiro, D. (1998). Relations of the alliance with psychother-
apy outcome: Findings in the Second Sheffield Psychotherapy
Project. Journal of Consulting and Clinical Psychology, 66 , 791!/802.
Watkins, E. (1998). Psychotherapy supervision in the 21st
century: Some pressing needs and impressing possibilities.
Journal of Psychotherapy Practice and Research , 7 , 2.Zanarini, M., Skodol, A., Bender, D., Dolan, R., Sanislow, C., &
Schaefer, E. (2000). The Collaborative Longitudinal Person-
ality Disorders Study: Reliability of Axis I and II diagnoses.
Journal of Personality Disorders , 14 , 291!/299.
Zusammenfassung
Klinische Supervision: Ihr Einfluss auf Klienten-Einschatzungen der Arbeitsbeziehung und dieSymptomreduktion in Kurzzeittherapie vonschwerer Depression
Supervision von Psychotherapeuten und Beratern, beson-ders in fruhen Jahren ihres Praktizierens, wird weithin alswichtig fur die professionelle Entwicklung und das Errei-chen optimaler Therapieergebnisse angesehen. Obwohlder Prozess der klinischen Supervision ausfuhrlich unter-
Effect of clinical supervision in treatment of major depression 329
Downloaded By: [Curtin University Library] At: 10:05 19 July 2010
sucht wurde, ist weniger uber ihren Einfluss auf diepsychotherapeutisch Praxis und die Reduktion von Symp-tomen bekannt. Diese Untersuchung bewertete den Ein-fluss von klinischer Supervision auf die Arbeitsbeziehungder Klienten und die Symptomreduktion bei Kurzzeitther-apie von schwerer Depression. Die Autoren haben 127Klienten mit schwerer Depression dem Zufall nach 127supervisierten oder nicht supervisierten Therapeuten zu-gewiesen fur eine Problemlosungsbehandlung mit achtSitzungen. Supervisierte Therapeuten wurden dem Zufallnach einer Allianzfahigkeits-Supervision oder einer Alli-anzprozess-Supervision zugewiesen und erhielten achtSupervisionstrainings. Vor Beginn der Behandlung beka-men die Therapeuten eine Supervisions-Sitzung mit einemkurzen Training des Arbeitsbeziehungs-Supervisions-Zu-gangs und den spezifischen Charakteristika aller Klienten.Standardmasse der therapeutischen Allianz und der Symp-tomveranderungen wurden als abhangige Variablen ver-wendet. Die Ergebnisse zeigten einen signifikanten Effektfur beide Supervisionsbedingungen auf die Arbeitsbezie-hung von der ersten Therapiesitzung an, auf die Symp-tomreduktion, den Verbleib in der Therapie und dieBewertung, aber keinen Unterschied zwischen den Super-visionsbedingungen. Die Effekte der Supervision und derkurzen Einfuhrung zum Vorgehen der Behandlung warennicht zu trennen und es ist moglich, dass Loyalitatseffektedie Ergebnisse verstarkt haben. Die wissenschaftliche undklinische Relevanz der Ergebnisse wird diskutiert.
Resume
La supervision clinique : son influence sur l’alliancede travail evaluee par les clients et la reduction dessymptomes dans le traitement bref de la depressionmajeure
La supervision des psychotherapeutes et conseillers, surt-out dans les premieres annees de leur pratique, estlargement acceptee dans son importance pour le devel-oppement professionnel et pour assurer un effet cliniqueoptimal pour les clients. Bien que le processus de lasupervision clinique ait ete largement etudie, on a moinsde connaissance sur l’impact de la supervision sur lapratique psychotherapeutique et les resultats cliniquesdes clients. Cette etude a evalue l’impact de la supervisionclinique sur l’alliance de travail des clients et la reductiondes symptomes dans le traitement bref de la depressionmajeure. Les auteurs ont attribue au hasard 127 clientsavec un diagnostic de depression majeure a 127 thera-peutes supervises ou non supervises pour un traitement de8 seances d’un traitement de solution de problemes. Lestherapeutes supervises etaient assignes au hasard a unesupervision focalisee soit sur l’habilete soit sur le processusau sujet de l’alliance et ils recevaient 8 seances de super-vision. Avant de commencer le traitement, les therapeutesrecevaient une seance de supervision pour une formationbreve dans l’approche de la supervision de l’alliance detravail et pour des caracteristiques specifiques de chaquecas. Des mesures standard de l’alliance therapeutique etdu changement de symptomes etaient appliques en tantque variables dependantes. Les resultats montraient uneffet significatif pour les deux conditions de supervisionsur l’alliance de travail de la premiere seance therapeu-tique, la reduction des symptomes ainsi que l’adhesion auet l’evaluation du traitement, mais pas de difference dans
l’effet des deux conditions de supervision. Il n’etait paspossible de separer les effets de la supervision des la seanceunique de pre-traitement et il est possible que des effetsd’allegeance aient dilate les resultats. L’importance scien-tifique et clinique de ces resultats est discutee.
Resumen
Supervision clınica: su influencia sobre la alianzade trabajo evaluada por el cliente y la reduccionsintomatica en la terapia breve de la depresionmayor
La supervision de psicoterapeutas y consejeros, especial-mente en los primeros anos de practica, esta ampliamenteaceptada como importante para el desarrollo profesional ypara asegurar resultados optimos para el cliente. Si bien elproceso de supervision clınica ha sido extensamenteestudiado, menos se conoce acerca del impacto de lasupervision sobre la practica psicoterapeutica y el resultadode los sıntomas del cliente. Este studio evaluo el impactode la supervision clınica sobre la alianza de trabajo delcliente y la reduccion del sıntoma en la terapia breve de ladepresion mayor. Los autores asignaron al azar cientoveintisiente clientes con diagnostico de depresion mayor aciento veintisiete terapeutas supervisados o no, que reci-birıan ocho sesiones de terapia para resolver problemas.Los terapeutas supervisados fueron asignados al azar parauna supervision focalizada en el desarrollo de la habilidadpara hacer alianza (alliance skill) o en el proceso de laalianza (alliance process) y recibieron ocho sesiones desupervision. Antes de comenzar el tratamiento, los ter-apeutas recibieron una sesion de supervision para entre-namiento breve en la supervision para la alianza de trabajoy para caracterısticas especıficas de cada caso. Comovariables dependientes se utilizaron medidas estandar dealianza terapeutica y de cambio sintomatico. Los resulta-dos mostraron un efecto significativo para ambos tipos desupervision de la alianza de trabajo desde las primerassesiones de terapia, reduccion sintomatica, retencion en eltratamiento y evaluacion pero sin diferencia entre el efectode las condiciones de supervision. No fue possible separarlos efectos de la supervision de los de la sesion previa altratamiento y es posible que los efectos de la adhesion hayaiinflado los resultados. Se debate sobre la relevanciacientıfica y clınica de estos hallazgos.
Resumo
Supervisao clınica: a sua influencia nas avaliacoes daalianca terapeutica pelos clientes e na reducaosintomatica em tratamento breve da depressaomajor
A supervisao de psicoterapeutas e conselheiros, em espe-cial durante os primeiros anos de pratica, tem sidoconsensualmente aceite como sendo importante para odesenvolvimento profissional e para assegurar a optimiza-cao resultados terapeuticos. Embora os processos desupervisao clınica tenham sido amplamente estudados,pouco se conhece sobre o impacto da supervisao na praticapsicoterapeutica e nas melhorias sintomaticas do cliente.Este estudo avaliou o impacto da supervisao clınica na
330 M. Bambling et al.
Downloaded By: [Curtin University Library] At: 10:05 19 July 2010
alianca terapeutica e na reducao sintomatica em terapiabreve da depressao major. Os autores distribuıram aleator-iamente 127 clientes, diagnosticados com depressao ma-jor, a 127 terapeutas com e sem supervisao, parareceberem oito sessoes de tratamento de resolucao deproblemas. Os terapeutas supervisionados foram aleator-iamente distribuıdos por duas condicoes de supervisao,focadas nas competencias de alianca terapeutica oufocadas no processo da alianca, recebendo oito sessoesde supervisao. Antes do inıcio do tratamento, os terapeutasreceberam uma sessao de supervisao como treino breve naabordagem de supervisao da alianca terapeutica e infor-macao sobre as caracterısticas especıficas de cada caso.Foram usadas medidas estandardizadas da alianca tera-peutica e da mudanca sintomatica como variaveis depen-dentes. Os resultados demonstraram um efeitosignificativo, em ambas as condicoes de supervisao, naalianca terapeutica, na reducao sintomatica, manutencaodos ganhos terapeuticos e avaliacao do tratamento, masnao se verificaram diferencas entre as condicoes de super-visao. Nao foi possıvel separar os efeitos da supervisao dasessao unica de treino no pre-tratamento e e possıvel que
os efeitos do comprometimento tenham inflacionado osresultados. Sao discutidos os resultados em relacao a suarelevancia cientıfica e clınica.
Effect of clinical supervision in treatment of major depression 331
Downloaded By: [Curtin University Library] At: 10:05 19 July 2010