45
Clinical Updates in Solid Tumor Oncology Panama City, Panama Jonathan Riess, MD, MS Assistant Professor of Medicine UC Davis School of Medicine

Clinical Updates in Solid Tumor Oncology
Panama City, Panama
Jonathan Riess, MD, MSAssistant Professor of Medicine
UC Davis School of Medicine
17th Annual Advances in OncologySeptember 30-October 1, 2016
Sacramento, CA
Jonathan Riess, M.D.Clinical Updates in Solid Tumor Oncology.
Relevant financial relationships in the past twelve months by presenter or spouse/partner:
Grant/Research Support: Merck, Novartis, MilleniumConsultant: Celgene, Ariad, Clovis, MedTronic
The speaker will directly disclosure the use of products for which are not labeled (e.g., off label use) or if the product is still investigational.

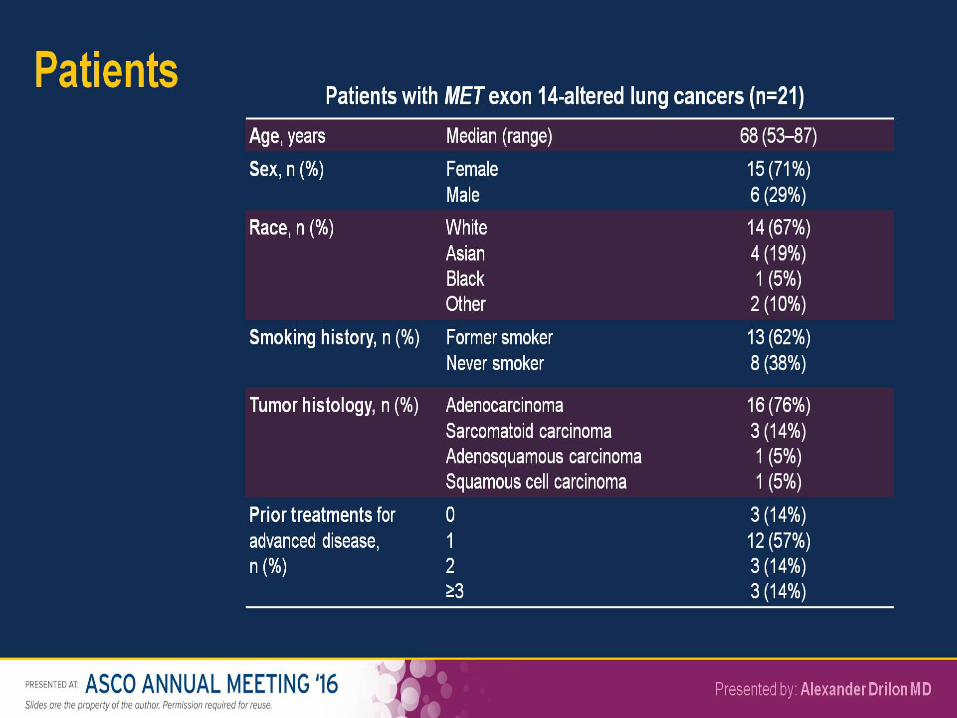
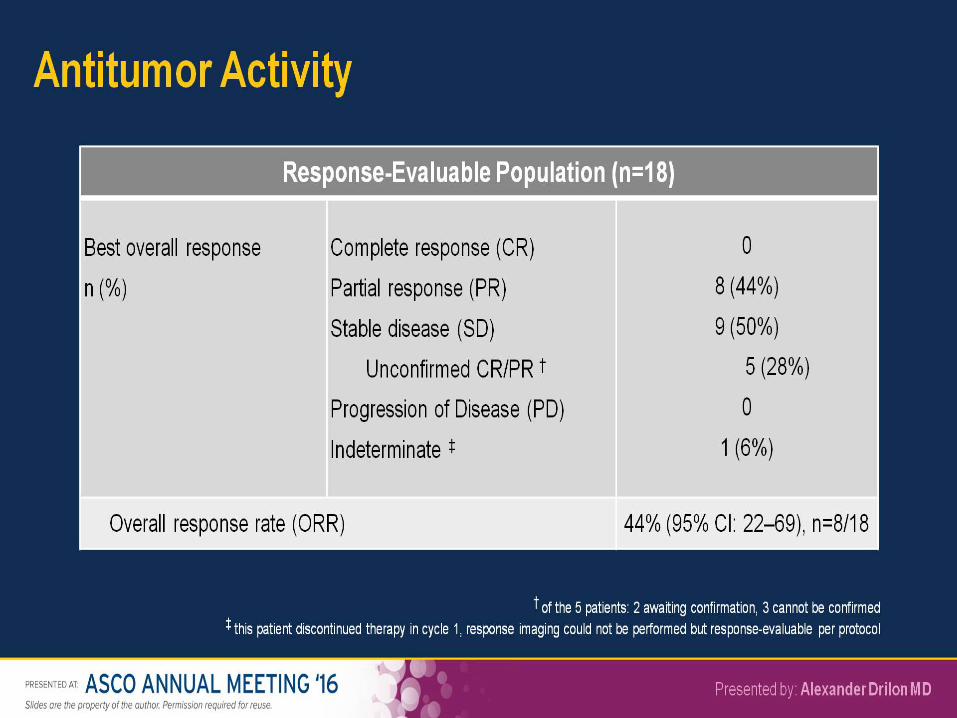
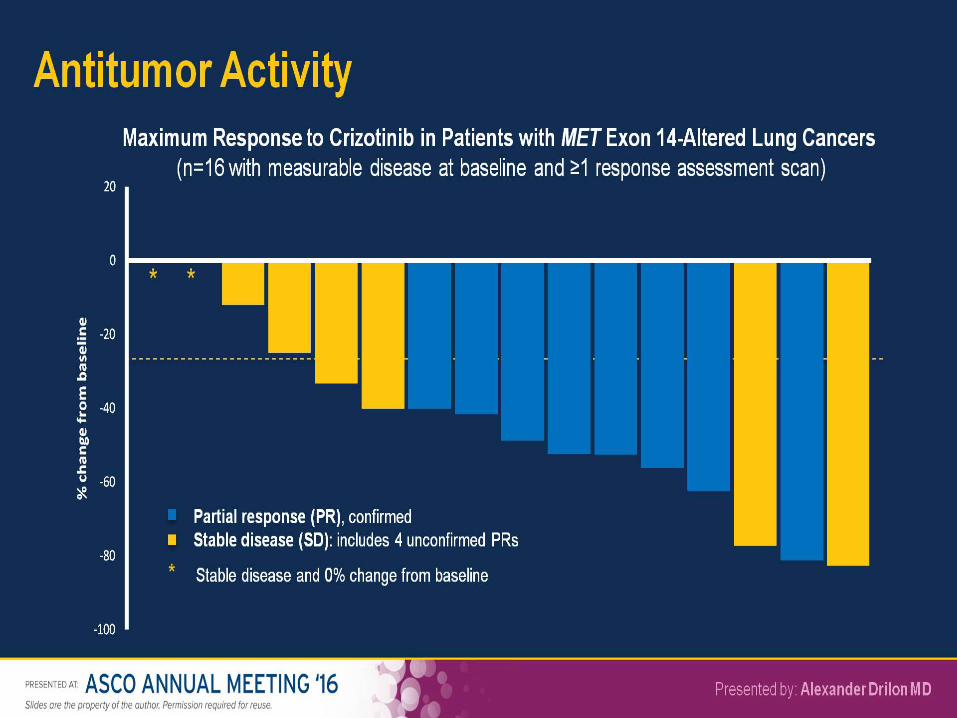
Abstracts: NSCLC/MetastaticAbstract 108: Efficacy and safety of crizotinib in patients (pts) with advanced MET exon 14-altered non-small cell lung cancer (NSCLC). (Alexander E. Drilon)
Abstract 9004: Local Consolidative Therapy (LCT) to improve progression-free survival (PFS) in patients with oligometastatic non-small cell lung cancer (NSCLC) who receive induction systemic therapy (IST): Results of a multi-institutional phase II randomized study. (Daniel Richard Gomez)
Abstract 9008: Primary analysis for alectinib versus crizotinib in ALK-inhibitor naïve ALK positive non-small cell lung cancer (ALK+ NSCLC) in randomized open-label phase III trial (J-ALEX study). (Hiroshi Nokihara)
Abstract 8500: Bayesian randomized trial comparing intensity modulated radiation therapy versus passively scattered proton therapy for locally advanced non-small cell lung cancer. (Zhongxing X. Liao)

Antitumor Activity and Safety of Crizotinib <br />in Patients with Advanced MET Exon 14-Altered <br />Non-Small Cell Lung Cancer

Slide 3

Distribution of genotypes among 933 patients with nonsquamous non–small-cell lung cancer (NSCLC).
Mark M. Awad et al. JCO doi:10.1200/JCO.2015.63.4600
©2016 by American Society of Clinical Oncology

Slide 4

Slide 6
Slide 8
Slide 10
Slide 11

Slide 13

Slide 17

Conclusions
• MET exon 14 alterations should now be assessed routinely in advanced NSCLC – Next generation sequencing assays are adequate
• Presence of MET exon 14 alterations predicts for response to MET inhibitors
• Recommended algorithm for MET exon 14 altered NSCLC:– Refer for clinical trial consideration– In absence of clinical trial, crizotinib is appropriate
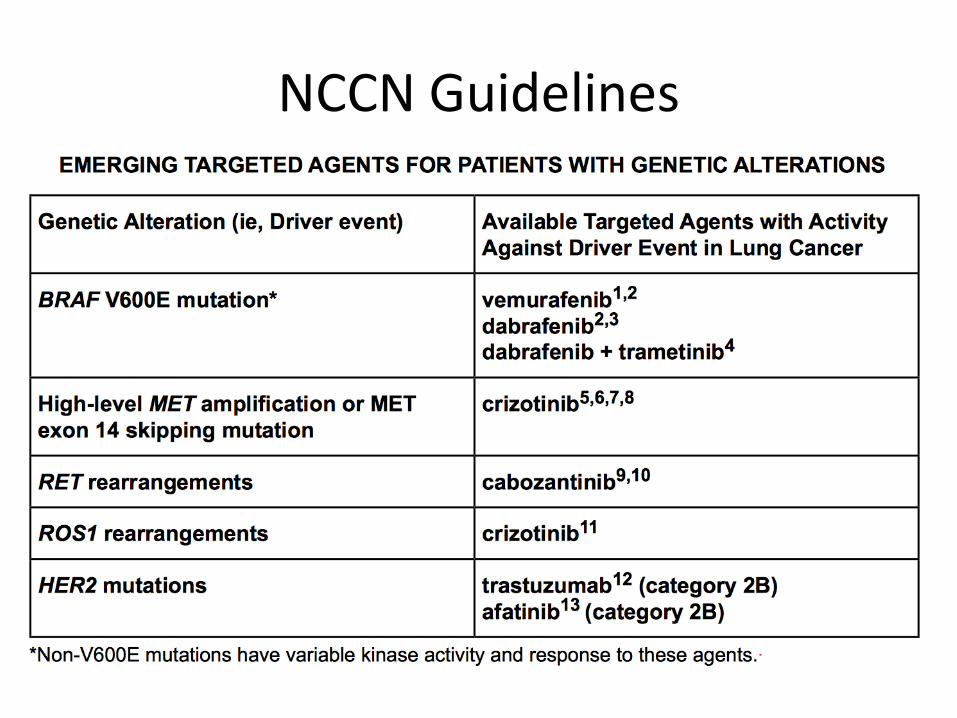
NCCN Guidelines
Local Consolidative Therapy (LCT) Improves Progression-Free Survival (PFS) in Patients with Oligometastatic Non-Small Cell Lung Cancer (NSCLC) who do not Progress after Front Line Systemic Therapy (FLST): Results of a Multi-Institutional Phase II Randomized Study
Daniel Gomez, George Blumenschein, Jack Lee, Mike Hernandez, Ross Camidge, Robert Doebele, Laurie Gaspar, Don Gibbons, Jose Karam, Brian Kavanagh, Ritsuko Komaki, Alexander Louie, David Palma, Anne Tsao, William William, Jianjun Zhang, Stephen Swisher*, John Heymach*, on behalf of the MD Anderson Cancer Center Lung Cancer Moon Shot Initiative
*Co-senior authors

Trial Design
Presented by: Daniel Gomez, M.D.
Surgery and RT Allowed
Crossover Allowed at
ProgressionStep 1:
Enrollment
Front Line Systemic Therapy
Step 2: EnrollmentNon-PD, Enroll,
Randomize
Physician choice for standard
maintenance or surveillance*
LCT(surgery ± radiation
to primary and metastases)
Physician choice for standard
maintenance or surveillance*
Consider LCT(surgery ± radiation
to primary and metastases)
Local Consolidative Therapy
No Local Consolidative Therapy
PD/Toxicity
PD
All patients had stage IV disease, three or fewer metastases, and no progression
after initial treatment with chemotherapy

CONSORT Diagram
Presented by: Daniel Gomez, M.D.
N=12 progression N=5 refused randomization
N=4 lost to follow-upN=3 further studies deemed
ineligibleN=1 study closed prior to
randomization
74 PatientsEnrolled into Step 1(Induction Phase)
49 PatientsEnrolled into Step 2
andRandomization
25 Patients NotEnrolled into Step 2
andRandomization
25 PatientsReceiving LCT
24 PatientsReceiving No LCT
At DSMC review in 1/2016, study closed due to observed efficacy in experimental arm after randomization of 49 patients
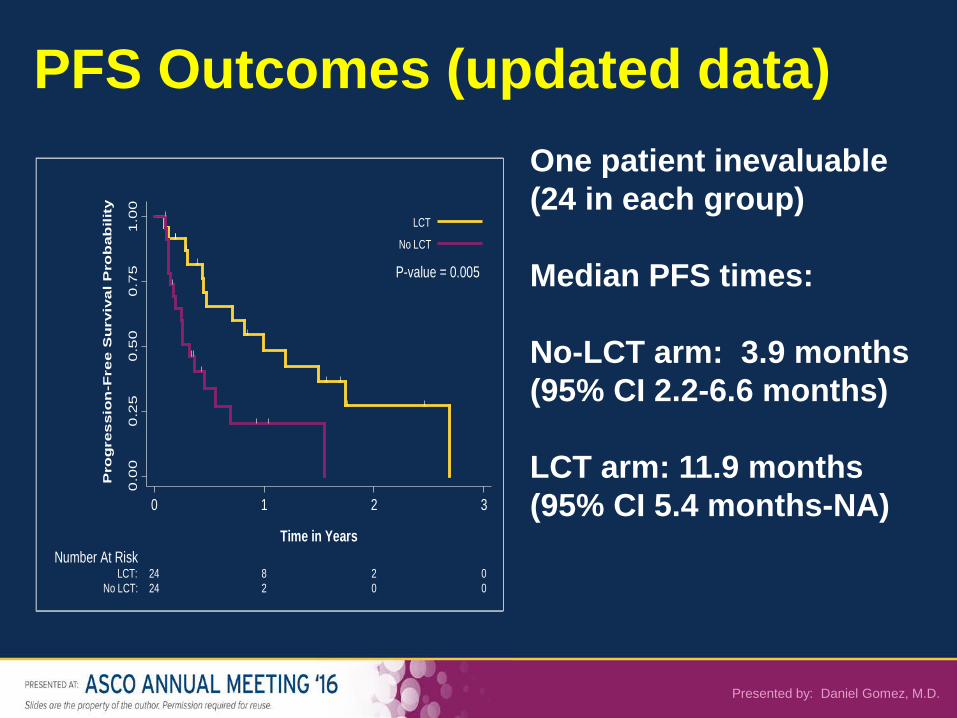
PFS Outcomes (updated data)One patient inevaluable (24 in each group)
Median PFS times:
No-LCT arm: 3.9 months (95% CI 2.2-6.6 months)
LCT arm: 11.9 months (95% CI 5.4 months-NA)
P-value = 0.005
0.0
00
.25
0.5
00
.75
1.0
0
Pro
gre
ssio
n-F
ree S
urv
iva
l P
rob
ab
ilit
y
24 2 0 0No LCT:24 8 2 0LCT:
Number At Risk
0 1 2 3
Time in Years
LCT
No LCT
Presented by: Daniel Gomez, M.D.

Patterns of Failure
• Difference in patterns of failure trended towards significance (p=0.09)– Higher proportion of locoregional only failures in no-LCT
arm (17% in no-LCT vs. 4% in LCT arm)– Higher proportion of metastatic only failures in LCT arm
(40% in LCT vs. 25% in no-LCT arm)– Higher proportion of both locoregional and metastatic
failures in no-LCT arm (29% in no-LCT vs. 8% in LCT arm)
Presented by: Daniel Gomez, M.D.

Time to New Site Failure (TNSF)
Median TNSF time 11.9 months in LCT arm vs. 5.7 months in no-LCT arm (p=0.0497)
P-value = 0.0497
0.0
00
.25
0.5
00
.75
1.0
0
Su
rviv
al F
ree
of
Ne
w L
esio
n P
rob
ab
ilit
y
24 2 1 0No LCT:24 8 2 0LCT:
Number At Risk
0 1 2 3
Time in Years
LCT
No LCT
Presented by: Daniel Gomez, M.D.
Conclusions
• In oligometastatic (1-3 mets) NSCLC, local consolidative therapy after systemic therapy appears to improve PFS– Exploratory analysis: LCT increased time to development of new
lesions• Results of trial are intriguing but not yet practice
changing– Population: highly heterogeneous (clinically and
biologically)– Sample size: limited– Quality of life: unknown– Crossover design confounds overall survival endpoint
Alectinib versus Crizotinib in ALK Inhibitor Naïve ALK-Positive Non-Small Cell Lung Cancer:
Primary Results from the J-ALEX Study
Hiroshi Nokihara, Toyoaki Hida, Masashi Kondo, Young Hak Kim, Koichi Azuma, Takashi Seto, Yuichi Takiguchi, Makoto Nishio, Hiroshige Yoshioka, Fumio Imamura, Katsuyuki Hotta,
Satoshi Watanabe, Koichi Goto, Kazuhiko Nakagawa, Tetsuya Mitsudomi, Nobuyuki Yamamoto, Hiroshi Kuriki, Ryoichi Asabe, Tomohiro Tanaka, Tomohide Tamura
Presented by: Hiroshi Nokihara

J-ALEX Phase III Study Design
Stratification factors:
R1:1
Key Entry Criteria• Stage IIIB/IV or recurrent
ALK-positive NSCLC• ALK centralized testing
(IHC and FISH or RT-PCR)• ECOG PS 0-2• ≥1 measurable lesion
assessed by investigator• Treated/asymptomatic brain
metastases allowed• ≤1 prior chemotherapy
Alectinib 300 mg BID PO, 28-day cycle
(N=100)
Crizotinib 250 mg BID PO, 28-day cycle
(N=100)
Endpoints• Primary
- PFS assessed by IRF*
• Secondary- OS- ORR- PK- QOL- CNS PFS- Safety
25
Clinical stage (IIIB/IV vs. Recurrent)Prior chemotherapy (0 vs. 1)ECOG PS (0/1 vs. 2)
JapicCTI-132316
*IRF Independent Review Facility
Presented by: Hiroshi Nokihara

Safety Overview
Alectinib(N=103)
Crizotinib(N=104)
Any AEs 100 (97.1%) 104 (100.0%)
Grade 3/4 AEs 27 (26.2%) 54 (51.9%)
Treatment-related deaths 0 0
Serious AEs 15 (14.6%) 27 (26.0%)
Discontinuation of study drug due to AEs 9 (8.7%) 21 (20.2%)
Dose interruptions due to AEs 30 (29.1%) 77 (74.0%)
26Presented by: Hiroshi Nokihara

Alectinib (n=83)
Crizotinib (n=90)
ORR [95%CI]
91.6% [85.6 -97.5]
78.9% [70.5 -87.3]
ORR* assessed by IRF
Objective Tumor Response
Presented by: Hiroshi Nokihara 27
ORR assessed by investigator in ITT population
Alectinib(n=83)
Water fall plot* assessed by IRF
CR or PR SD, PD or NE
Crizotinib(n=90)
Alectinib (N=103)
Crizotinib (N=104)
ORR [95%CI]
85.4% [78.6 -92.3]
70.2% [61.4 -79.0]

Primary Endpoint: PFS by IRF (ITT Population)
0 6 12 18 27
100
80
60
40
20
0
Prog
ress
ion-
free
surv
ival
rate
(%)
24213 9 151
7665
3621
94
19386
4940
2714
103102
No. of patients at riskAlectinib
Crizotinib103104
Presented by: Hiroshi Nokihara 28
Time (months)
10.2 months
NR
HR = 0.34, p<0.001

Presented by: Hiroshi Nokihara 29
Conclusions
• Alectinib is superior to crizotinib as frontline therapy of ALK-positive NSCLC– RR: 85% vs 70%– PFS HR = 0.34 (p<0.001)
• mPFS: Not reached vs. 10 months– Time to progression for those with brain metastases: PFS was 92%
better for alectinib– Toxicity profile favored alectinib
• Caveats: Japanese-only trial, cost (third party reimbursement) • Bottom line:
– Alectinib can be considered as frontline ALK-targeted therapy (particularly pts with brain mets)
– We await definitive results of global ALEX trial

A Bayesian Randomization Trial of Intensity Modulated Radiation Therapy (IMRT) vs.
3-Dimensional Passively Scattered Proton Therapy (3DPT) for Locally Advanced Non-Small Cell
Lung Carcinoma
(clinicaltrials.gov identifier NCT00915005)
Zhongxing Liao, J. Jack Lee, Ritsuko Komaki, Daniel R. Gomez, Michael O’Reilly, Pamela K. Allen, Frank Fossella, John V. Haymach, George R. Blumenschein,Noah Chan Choi, Thomas F. Delaney, Stephen M. Hahn, Charles Lu, James D.
Cox, and Radhe Mohan
Supported in part by NCI grants P01 CA021230 and U19 CA021239.

Hypothesis
Proton therapy will – Reduce irradiated lung volume, hence
reduce radiation pneumonitis (RP)– Achieve same local control (LC) with
same biological effective radiation dose (Proton relative biological equivalence=1.1)

Primary Objective
Protocol Failure (Dual endpoints):• Radiation Pneumonitis grade > 3
(CTCAE 3.0)– IMRT = 15%– 3DPT = 5%
• Local failure (PET, CT, biopsy):– IMRT = 3DPT– 15% at 6mo & 25% at 12mo.

Randomized and Treated According to Randomization Analysis
Comparative IMRT and 3DPSPT plans evaluated
N = 225
Treated with IMRTN=92
Preferred protons
N = 6
IMRT N = 105
Signed informed consent N= 274
Excluded from analysis N=49:1. Chemotherapy only : 12. Consented twice3. Closed to patient accrual: 34. Disease progression: 85. GTV movement > 2 cm: 16. Ineligible body weight: 17. Insurance denied: 88. No Chemo: 29. No good for proton: 110. Poor PFT : 411. Patient wants proton only: 212. Screening Failure: 4 (Stage I:
1 & Stage IV:2)13. Surgery: 114. tumor too large: 115. TX at local facility: 116. Violation of the study: 417. Withdraw IC: 5
Plans randomizable
N = 181
3DPT N = 76
Treated with 3DPTN = 57
Insurance denied protons so treated
with IMRTN=15
3DPT betterN = 13
Off study due to Unacceptable plan
N =3
IMRT plan betterN = 28
Plans not randomizable
N=44
Off protocolN = 4
Off protocolN = 7
(3 insurance denial protocol)

Baseline Characteristics
• Demographics (age, gender, ECOG, smoking status, histology, stage) no difference.
• Target Volumes:
Target Volumes (cc) IMRT 3DPT Total P valuesGTV Median 66.10 77.7 70.3 0.141
Min-Max (5.75-686.59) (1.9-673.7) (1.9-686.59)ITV
Median 257.655 320.7 292.7 0.055Min-Max (42.01-1316.24) (30-1384) (30-1384)
PTVMedian 429.35 524.9 480.31 0.071Min-Max (103.92-1776.06) (76-1906) (76-1906)
• RT dose 74 Gy: IMRT vs. 3DPT = 63% vs. 75.4% (p<0.001)

0.00
0.25
0.50
0.75
1.00
Pro
port
ion
57 38(12) 21(7) 12(1) 9(0) 3(0) 1(1)Proton92 62(16) 36(10) 20(1) 13(0) 6(0) 0(1)IMRT
Number at risk
0 12 24 36 48 60 72Months
Protocol Failure
0.00
0.25
0.50
0.75
1.00
Pro
port
ion
57 56(0) 48(5) 44(1) 41(0)Proton92 86(1) 78(3) 74(2) 72(0)IMRT
Number at risk
0 3 6 9 12Months
Grade >3 TRP
0.00
0.25
0.50
0.75
1.00
Pro
port
ion
57 40(6) 21(8) 12(1) 9(0) 3(0) 1(1)Proton92 66(10) 38(11) 21(1) 14(0) 6(1) 0(1)IMRT
Number at risk
0 12 24 36 48 60 72Months
Local Failure
P=0.55
Protocol Failure - Randomized and Treated According to Protocol
Protocol Failure (Dual endpoints):RP grade > 3 (CTCAE 3.0)IMRT = 15% vs. 6.5% 3DPT = 5% vs. 10.5%
Local Failure at 12 month (PET, CT, biopsy):IMRT = 3DPT = 25% vs. 10.7%
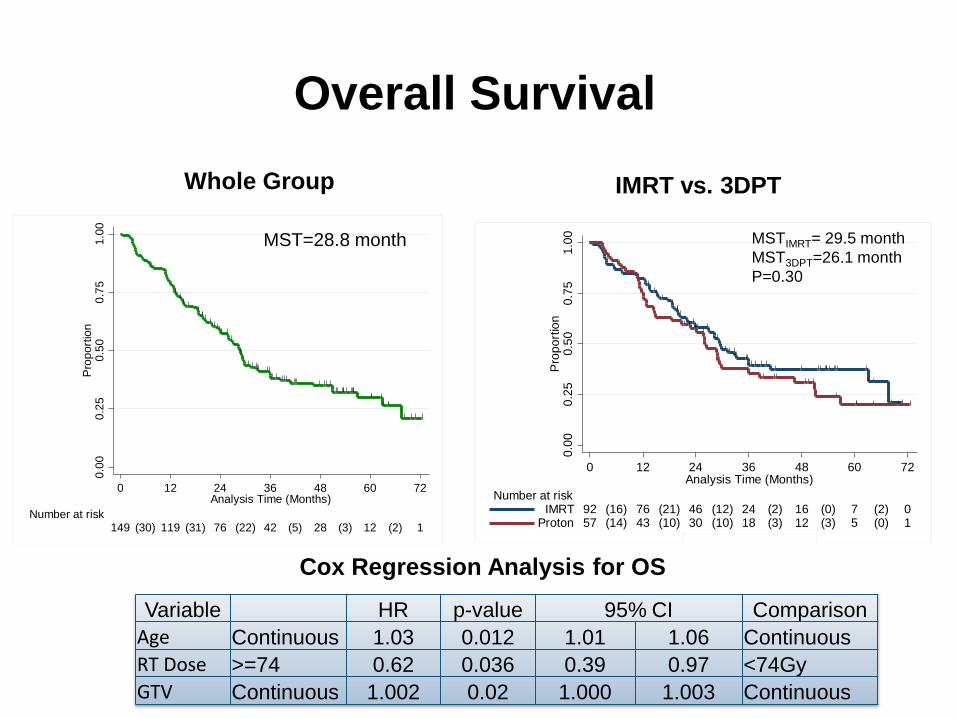
Overall SurvivalWhole Group IMRT vs. 3DPT
Cox Regression Analysis for OS Variable HR p-value 95% CI Comparison
Age Continuous 1.03 0.012 1.01 1.06 ContinuousRT Dose >=74 0.62 0.036 0.39 0.97 <74GyGTV Continuous 1.002 0.02 1.000 1.003 Continuous
0.00
0.25
0.50
0.75
1.00
Prop
ortio
n
149 119(30) 76(31) 42(22) 28(5) 12(3) 1(2) Number at risk
0 12 24 36 48 60 72Analysis Time (Months)
0.00
0.25
0.50
0.75
1.00
Prop
ortio
n
57 43(14) 30(10) 18(10) 12(3) 5(3) 1(0)Proton92 76(16) 46(21) 24(12) 16(2) 7(0) 0(2)IMRT
Number at risk
0 12 24 36 48 60 72Analysis Time (Months)
MST=28.8 month MSTIMRT= 29.5 monthMST3DPT=26.1 monthP=0.30

Conclusions
• Proton beam RT is no better than standard IMRT– Primary endpoint not met
• Pneumonitis numerically worse with protons• No significant differences in treatment failure rates• Trend for worse survival with proton beam
– IMRT 29.5 months vs. Proton 26.1 months
• Results dispel prevailing notion that proton beam RT is superior to standard RT
• Lack of clear benefits of proton beam RT do not justify its higher cost in this patient context

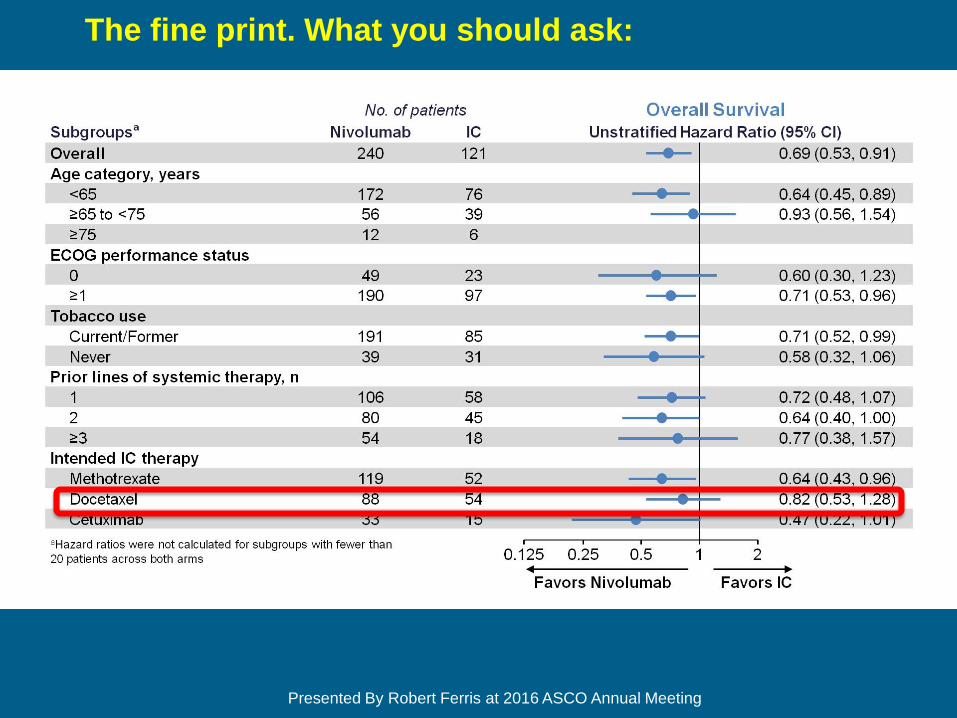
Nivolumab versus Investigator’s Choice Chemotherapy for R/ M SCCHN,
from ASCO 2016
Robert L. Ferris, George Blumenschein, Jr, Jerome Fayette, Joel Guigay, A. Dimitrios Colevas, Lisa Licitra, Kevin Harrington, Stefan Kasper, Everett E. Vokes, Caroline Even,
Francis Worden, Robert Haddad, Makoto Tahara, Naomi Kiyota, Manish Monga, Mark Lynch, William J. Geese, Justin Kopit, James W. Shaw, Maura L. Gillison

Nivolumab versus Investigator’s Choice Chemotherapy for R/ M SCCHN, second line and beyond
from ASCO 2016
Slide 8
Presented By Robert Ferris at 2016 ASCO Annual Meeting
The fine print. What you should ask:

Pembrolizumab, “ KEYNOTE-012” ASCO 2016
With permission, Ranee Mehra et al.
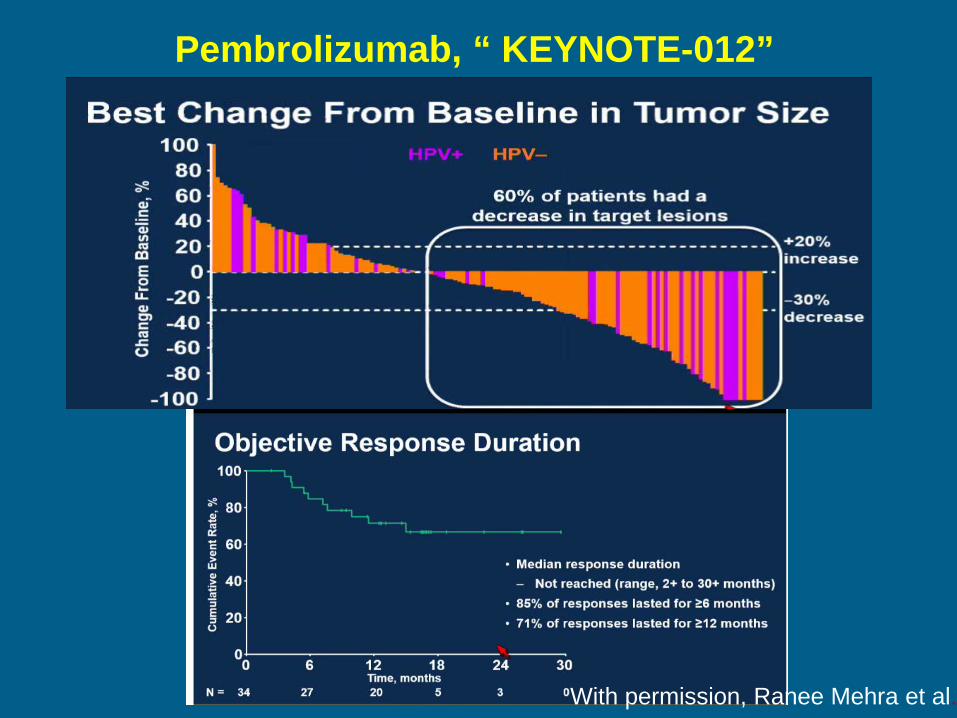
Pembrolizumab, “ KEYNOTE-012”
With permission, Ranee Mehra et al.

Prediction of response to pembrolizumab
With permission, Laura Chow et al. ASCO 2016.

Prediction of OS to pembrolizumab
With permission, Laura Chow et al. ASCO 2016.
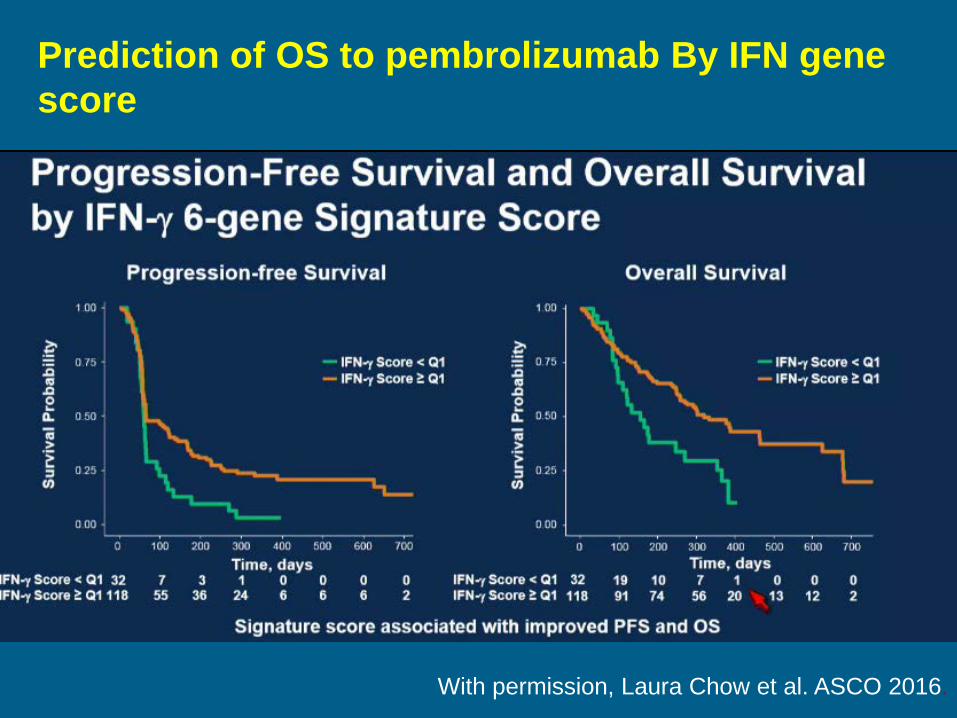
Prediction of OS to pembrolizumab By IFN gene score
With permission, Laura Chow et al. ASCO 2016.

















