Clostridium Difficile: Clostridium Difficile: Epidemiology Epidemiology and Clinical Spectrum and Clinical Spectrum Cassandra D Salgado, MD, Cassandra D Salgado, MD, MS MS Associate Professor of Medicine Associate Professor of Medicine Hospital Epidemiologist, MUSC Hospital Epidemiologist, MUSC March 15, 2012 March 15, 2012
Cassandra D Salgado, MD, MSCassandra D Salgado, MD, MSAssociate Professor of MedicineAssociate Professor of MedicineHospital Epidemiologist, MUSCHospital Epidemiologist, MUSC
March 15, 2012March 15, 2012
I have no Disclosures to report I have no Disclosures to report relevant to the content of this relevant to the content of this
presentation.presentation.Cassandra D Salgado, MD, MSCassandra D Salgado, MD, MS
Associate Professor of MedicineAssociate Professor of MedicineHospital Epidemiologist, MUSCHospital Epidemiologist, MUSC
March 15, 2012March 15, 2012
Case Presentation
• 50 year old female was admitted for COPD exacerbation. She was treated with steroids, inhalers, and antibiotics.
• On hospital day 6 she develops fever of 102°F hypotension, diarrhea, and increased WBC count with profound bandemia (WBC= 48,000 with 30% bands).
• Septic workup was done…
Case PresentationCase Presentation
• Patient continued to decompensate Patient continued to decompensate with continued fevers and hypotension with continued fevers and hypotension requiring vasopressors and transfer to requiring vasopressors and transfer to MICUMICU
• Bowel movements ceased on hospital Bowel movements ceased on hospital day 8 and patient was evaluated for day 8 and patient was evaluated for toxic megacolon…toxic megacolon…
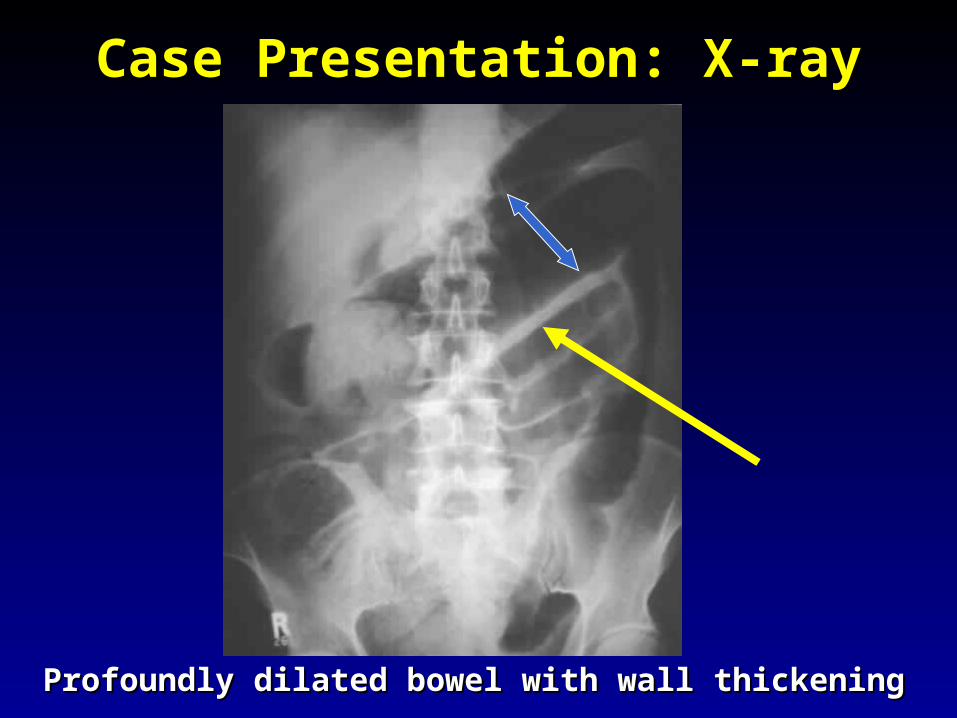
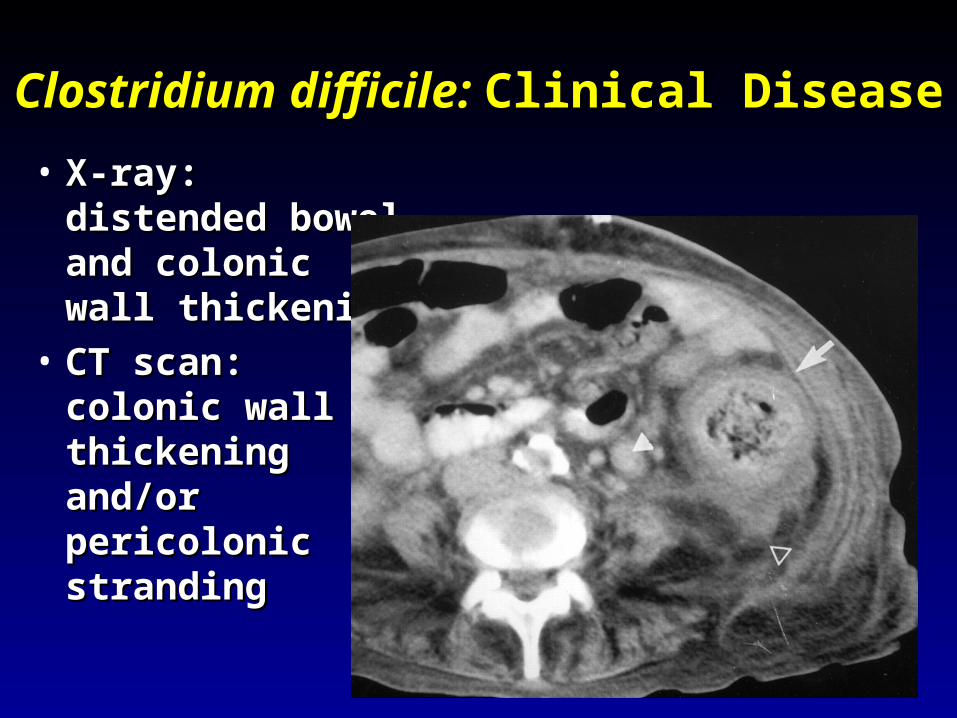
Case Presentation: X-rayCase Presentation: X-ray
Profoundly dilated bowel with wall thickeningProfoundly dilated bowel with wall thickening
Case PresentationCase Presentation• The patient was taken to surgery…The patient was taken to surgery…
Case PresentationCase Presentation
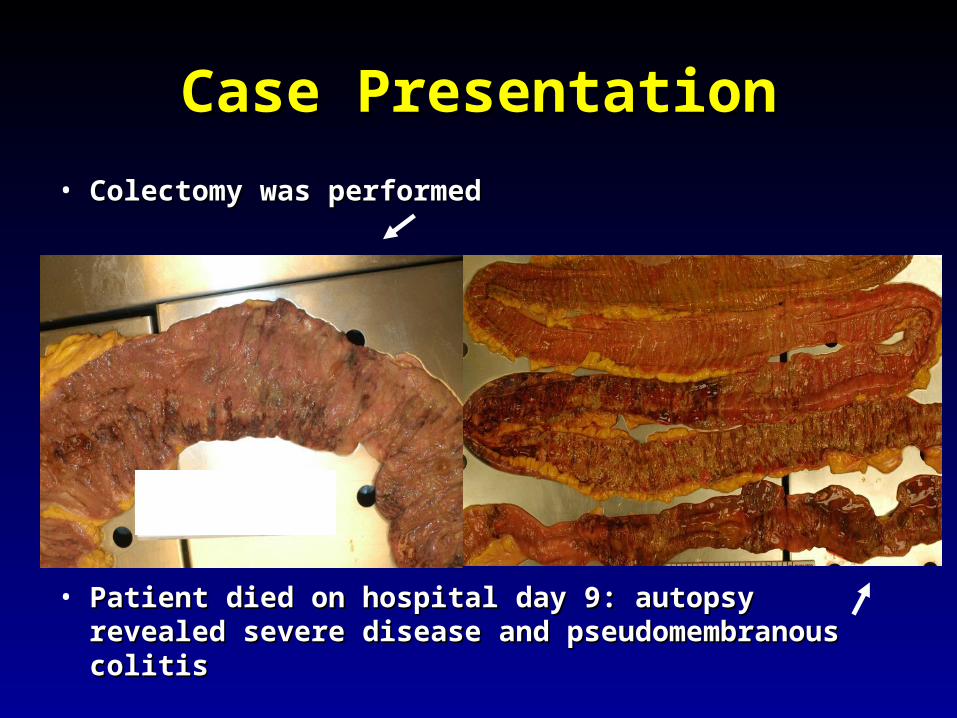
• Colectomy was performedColectomy was performed
• Patient died on hospital day 9: autopsy revealed Patient died on hospital day 9: autopsy revealed severe disease and pseudomembranous colitissevere disease and pseudomembranous colitis
•C. diffC. diff is a is a spore spore formingforming gram-positive gram-positive anaerobic bacillus that anaerobic bacillus that produces at least two produces at least two exotoxins (A and B) exotoxins (A and B) and a binary toxinand a binary toxin
•The ability to produce The ability to produce spores allows spores allows C. diffC. diff to to be acquired from be acquired from outside the host outside the host
C. difficileC. difficile: Epidemiology: Epidemiology• ““difficult” to isolate in laboratorydifficult” to isolate in laboratory• 1978: cause of pseudomembranous colitis1978: cause of pseudomembranous colitis• Most commonly recognized microbial cause of Most commonly recognized microbial cause of
hospital-acquired diarrheahospital-acquired diarrhea• 3-5% of healthy adults are colonized3-5% of healthy adults are colonized• 20-40% of hospitalized patients are colonized20-40% of hospitalized patients are colonized• Asymptomatic carriers outnumber patients with Asymptomatic carriers outnumber patients with
Clostridium DifficileClostridium Difficile: Risk Factors: Risk Factors• Exposure to antibiotics the preeminent risk Exposure to antibiotics the preeminent risk
factor for developing diseasefactor for developing disease• More than 90% of healthcare-associated CDI More than 90% of healthcare-associated CDI
occur while on antibioticsoccur while on antibiotics– Agents active against anaerobic organisms are Agents active against anaerobic organisms are
considered to present the greatest risk (clindamycin)considered to present the greatest risk (clindamycin)– Most cases are associated with Most cases are associated with ββ-lactam therapy -lactam therapy – Growing number of reports of associations with Growing number of reports of associations with
fluoroquinolone therapy fluoroquinolone therapy – Duration of antecedent therapy may be brief (surgical Duration of antecedent therapy may be brief (surgical
prophylaxis) prophylaxis)
C. DiffC. Diff and Antibiotic Use and Antibiotic Use• Broad-spectrum agents with a greater effect on the normal intestinal flora have been associated Broad-spectrum agents with a greater effect on the normal intestinal flora have been associated
with CDADwith CDAD• Meta-analysis: 49 studiesMeta-analysis: 49 studies
Clostridium DifficileClostridium Difficile: Risk Factors: Risk Factors• Cancer with or without chemotherapyCancer with or without chemotherapy• GI surgery and other types of GI manipulationGI surgery and other types of GI manipulation• Older ageOlder age• Severity of illnessSeverity of illness• Immunocompromising conditions Immunocompromising conditions • Longer duration of stay in hospitalLonger duration of stay in hospital• ICU stayICU stay• Exposure to an infected roommateExposure to an infected roommate• Anti-ulcer medicationsAnti-ulcer medications
C. diffC. diff: Special Populations: Special Populations• Most cases of CDI occur in healthcareMost cases of CDI occur in healthcare• Among hospitalized patientsAmong hospitalized patients
– Medical patients are at increased risk compared to Medical patients are at increased risk compared to surgical patientssurgical patients
• C. diffC. diff is the most common cause of acute is the most common cause of acute diarrheal illness in LTCFdiarrheal illness in LTCF– Population is older, receive more medications known Population is older, receive more medications known
to increase risk of to increase risk of C. diffC. diff• Neonates may also be colonized withNeonates may also be colonized with C. diff C. diff
– Up to 70%Up to 70%– Neonates colonized with toxogenic strains less likely Neonates colonized with toxogenic strains less likely
than adults to develop symptomatic diseasethan adults to develop symptomatic disease• Neonates may lack receptors for toxin A in their immature Neonates may lack receptors for toxin A in their immature
enterocytesenterocytes
Sunenshine R. Clev Clinic J Med 2006;73:187.Sunenshine R. Clev Clinic J Med 2006;73:187.
ulcerations which release proteins, mucus, and inflammatory cells
• Type 1- mildest changes confined to superficial layers • Type 2- more severe with marked secretions• Type 3- intense necrosis and full intestinal thickness
involvement produces a confluent membrane
C. diffC. diff: Clinical Disease: Clinical Disease
• Fulminant colitis (rare)• Severe abdominal pain, abdominal
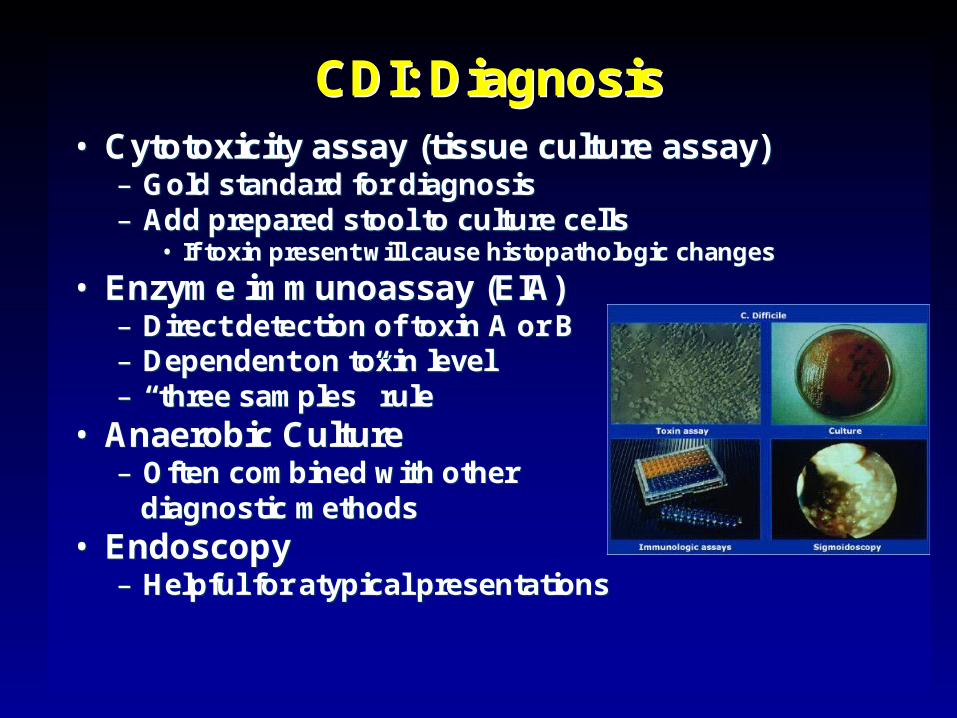
–– Gold standard for diagnosisGold standard for diagnosis–– Add prepared stool to culture cellsAdd prepared stool to culture cells
•• If toxin present will cause If toxin present will cause histopathologichistopathologic changeschanges
•• Enzyme immunoassay (EIA)Enzyme immunoassay (EIA)–– Direct detection of toxin A or BDirect detection of toxin A or B–– Dependent on toxin levelDependent on toxin level–– ““three samplesthree samples”” rulerule
•• Anaerobic CultureAnaerobic Culture–– Often combined with otherOften combined with other
diagnostic methodsdiagnostic methods
•• EndoscopyEndoscopy–– Helpful for atypical presentationsHelpful for atypical presentations
2 hrs2 hrs 8080--95%95% Easy to useEasy to use Decreased Decreased sensitivity for sensitivity for low level toxinlow level toxin
SunenshineSunenshine R. R. ClevClev Clinic J Med 2006;73:187.Clinic J Med 2006;73:187.PlanchePlanche T. Lancet ID 2008;8:777T. Lancet ID 2008;8:777--784784
Decreases PPV and limits clinical management
CDI: DiagnosisCDI: Diagnosis•• PCR Based TestingPCR Based Testing
–– Directed towards Directed towards toxin B or toxin A toxin B or toxin A and Band B
–– Sensitivity and Sensitivity and specificity 97specificity 97--100%100%
–– No No ““three samplesthree samples””
–– Compares well with Compares well with toxinogenictoxinogenic cultureculture
–– Considered by Considered by some to be the best some to be the best clinical diagnostic clinical diagnostic tooltool
Clostridium DifficileClostridium Difficile: At What Cost?: At What Cost?
• Estimated 3,000,000 new cases of Estimated 3,000,000 new cases of C. diffC. diff diarrhea and colitis in US hospitals diarrhea and colitis in US hospitals annuallyannually– Affects as many as 10% of patients Affects as many as 10% of patients
hospitalized for more than 2 dayshospitalized for more than 2 days– Relapsing disease occurs in 20-25% of Relapsing disease occurs in 20-25% of
adequately treated patientsadequately treated patients• Further relapses occur in 65% of patients who Further relapses occur in 65% of patients who
have suffered more than one relapsehave suffered more than one relapse
Clostridium DifficileClostridium Difficile: At What Cost?: At What Cost?Study Mortality LOS (excess) Costs
Miller MA. 2002 1.5% 13.6 days $85,000 per yr
Kyne L. 2002 NR 10.2 (3.6) days $3,669 per pt
McFarland LV. 1999 0% NR $10,970 per pt
Wilcox MH. 1996 NR 46.5 (21.3) days £4,000 per pt
Riley TV. 1995 NR 24.5 (18) days *$1,250,000 per yr
responsible for most nosocomial diarrhea. responsible for most nosocomial diarrhea. Risks for CDI include antibiotic exposure, Risks for CDI include antibiotic exposure, other drugs, older age, and co-morbidities. other drugs, older age, and co-morbidities. CDI has been associated with notable CDI has been associated with notable morbidity, but traditionally low rates of morbidity, but traditionally low rates of severe disease and mortality.severe disease and mortality.
C. diffC. diff: New Epidemiologic Issues: New Epidemiologic Issues
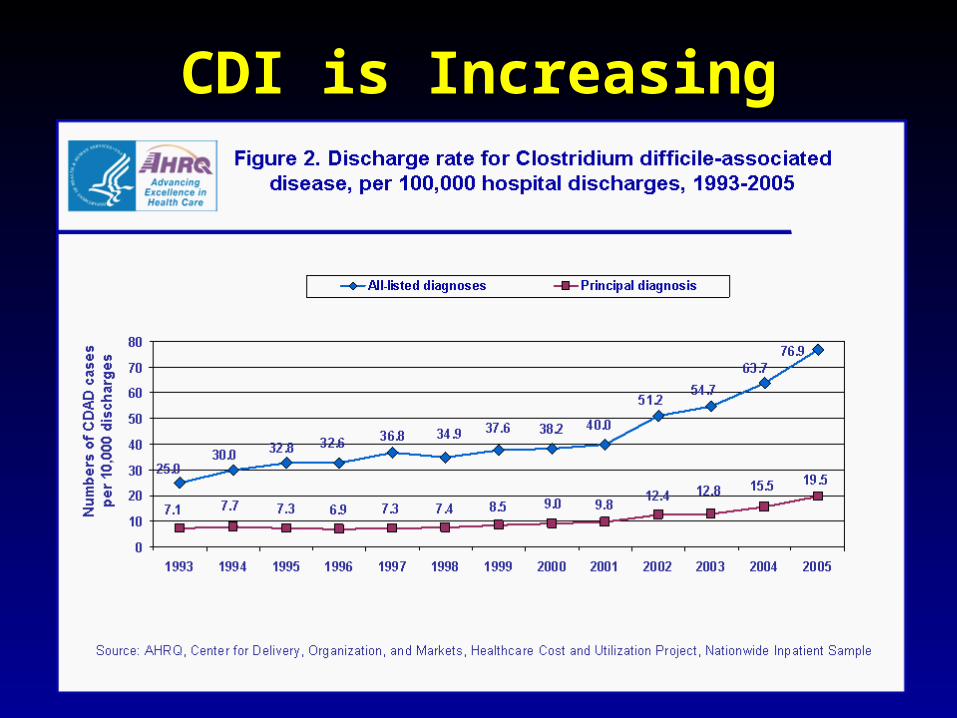
• C. diff ratesC. diff rates are increasing are increasing
• More severe disease with higher More severe disease with higher mortality and higher rates of colectomy mortality and higher rates of colectomy
• A common epidemic strain has been A common epidemic strain has been found in North America and Europefound in North America and Europe– Fluoroquinolone use may be driving its Fluoroquinolone use may be driving its
emergenceemergence
CDI is IncreasingCDI is Increasing• Average rate of CDI among NNIS Average rate of CDI among NNIS
hospitals from 1987-1998hospitals from 1987-1998– 12.2 cases per 10,000 pt-days12.2 cases per 10,000 pt-days
• Teaching hospitals: 13.0 per 10,000 pt daysTeaching hospitals: 13.0 per 10,000 pt days• Non-teaching hospitals: 11.4 per 10,000 pt daysNon-teaching hospitals: 11.4 per 10,000 pt days
• CDC reports that hospitalizations with a CDC reports that hospitalizations with a discharge diagnosis of CDI discharge diagnosis of CDI – Was 31 per 100,000 in 1996Was 31 per 100,000 in 1996– Was 61 per 100,000 in 2003Was 61 per 100,000 in 2003
C. diffC. diff-Associated Infection-Associated Infection
Incidence of CDI per 10,000 patient daysIncidence of CDI per 10,000 patient daysNNIS 1987-2001 Archibald et al JID 2004;189:1585NNIS 1987-2001 Archibald et al JID 2004;189:1585
Recent data: Incidence of healthcare-associated C. diff colonization and infection are 29.5 and 28.1 cases per 10,000 pt days, respectively.
C. diffC. diff: Increased Morbidity and Mortality: Increased Morbidity and Mortality
• A hospital in Pittsburgh reports 253 A hospital in Pittsburgh reports 253 nosocomial CDI cases in 2 years with an nosocomial CDI cases in 2 years with an increase from 2.7 to 6.8 cases per 1,000 increase from 2.7 to 6.8 cases per 1,000 discharges (p<0.001)discharges (p<0.001)11
• A Chicago hospital reports increased A Chicago hospital reports increased severity of CDI and increased mortality in severity of CDI and increased mortality in MICU and oncology patientsMICU and oncology patients22
– high rates of shockhigh rates of shock– 37% mortality37% mortality
11Muto et al. ICHE 2005;26:273., Muto et al. ICHE 2005;26:273., 22Patel et al. 2005 SHEA Annual Meeting #285.Patel et al. 2005 SHEA Annual Meeting #285.
C. diffC. diff: Increased Morbidity and Mortality: Increased Morbidity and Mortality
• Prospective study of 1719 CDI episodes Prospective study of 1719 CDI episodes in 12 Quebec hospitalsin 12 Quebec hospitals– Determine incidence of CDI and Determine incidence of CDI and
complicationscomplications• 22.5 per 1,000 admissions22.5 per 1,000 admissions
– Incidence increased with ageIncidence increased with age
• 30-day attributable mortality was 6.9%30-day attributable mortality was 6.9%– Attributable mortality increased with ageAttributable mortality increased with age
Loo VG et al. NEJM 2005;353(23):2442.Loo VG et al. NEJM 2005;353(23):2442.
C. diffC. diff: Pathogenicity: Pathogenicity
• In general, In general, C. diffC. diff strains either possess the strains either possess the entire genetic element (PaLoc) responsible entire genetic element (PaLoc) responsible for producing toxin (toxigenic strains) or lack for producing toxin (toxigenic strains) or lack this genetic element and thus, do not cause this genetic element and thus, do not cause disease (non-toxigenic strains)disease (non-toxigenic strains)
C. diffC. diff: Pathogenicity: Pathogenicity
• Mutation(s) in the Mutation(s) in the tcdtcd C gene can cause the C gene can cause the C. diffC. diff strain to strain to produce increased amounts of toxin causing more severe produce increased amounts of toxin causing more severe disease.disease.– 16 x more toxin A and 23 x more toxin B16 x more toxin A and 23 x more toxin B
• A binary toxin may also contribute, but clinical significance A binary toxin may also contribute, but clinical significance is not yet known.is not yet known.
• This “epidemic strain” is PCR ribotype 027, PFGE type This “epidemic strain” is PCR ribotype 027, PFGE type NAP1, and restriction endonuclease type B1.NAP1, and restriction endonuclease type B1.
States with BI/NAP1/027 strain of C. difficile
DC
PRAK
HI
Recent data: among patients colonized or infected with C. diff, 36% and 63% have the NAP1 strain, respectively
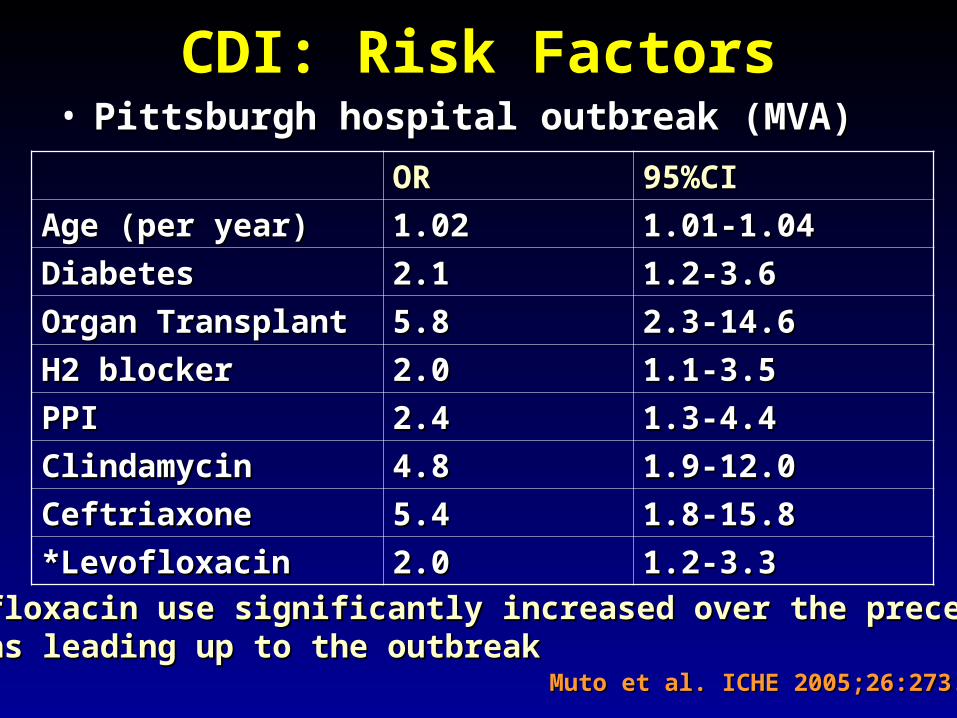
Age (per year)Age (per year) 1.021.02 1.01-1.041.01-1.04
DiabetesDiabetes 2.12.1 1.2-3.61.2-3.6
Organ TransplantOrgan Transplant 5.85.8 2.3-14.62.3-14.6
H2 blockerH2 blocker 2.02.0 1.1-3.51.1-3.5
PPIPPI 2.42.4 1.3-4.41.3-4.4
ClindamycinClindamycin 4.84.8 1.9-12.01.9-12.0
CeftriaxoneCeftriaxone 5.45.4 1.8-15.81.8-15.8
*Levofloxacin*Levofloxacin 2.02.0 1.2-3.31.2-3.3
Muto et al. ICHE 2005;26:273.Muto et al. ICHE 2005;26:273.
*Levofloxacin use significantly increased over the preceding *Levofloxacin use significantly increased over the preceding months leading up to the outbreakmonths leading up to the outbreak
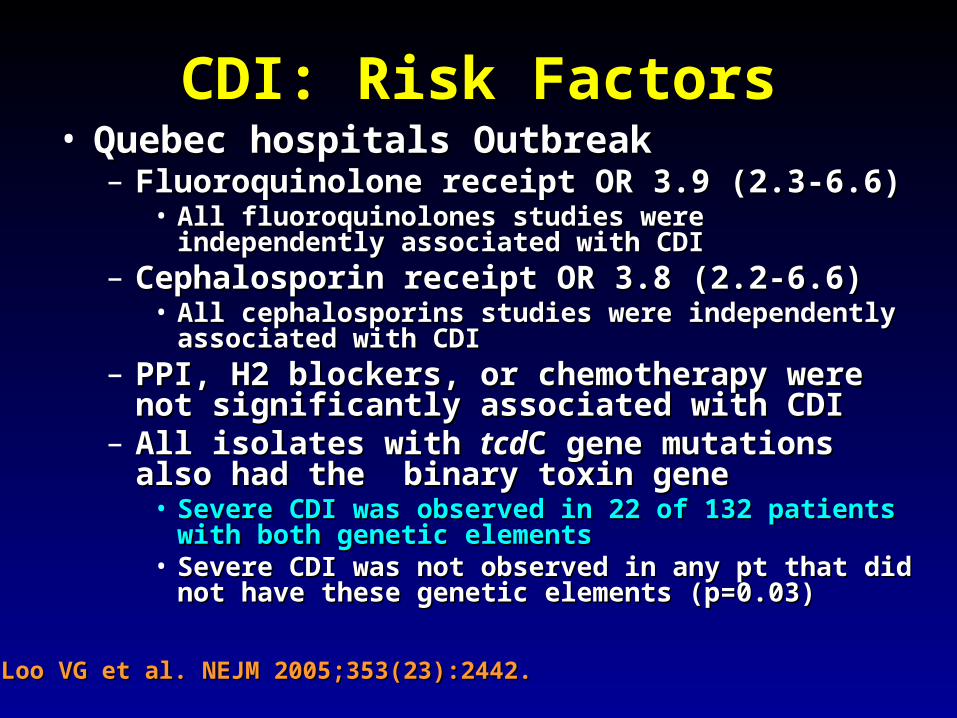
– Fluoroquinolone receipt OR 3.9 (2.3-6.6)Fluoroquinolone receipt OR 3.9 (2.3-6.6)• All fluoroquinolones studies were independently All fluoroquinolones studies were independently
associated with CDIassociated with CDI– Cephalosporin receipt OR 3.8 (2.2-6.6)Cephalosporin receipt OR 3.8 (2.2-6.6)
• All cephalosporins studies were independently associated All cephalosporins studies were independently associated with CDIwith CDI
– PPI, H2 blockers, or chemotherapy were not PPI, H2 blockers, or chemotherapy were not significantly associated with CDIsignificantly associated with CDI
– All isolates with All isolates with tcdtcdC gene mutations also had the C gene mutations also had the binary toxin genebinary toxin gene
• Severe CDI was observed in 22 of 132 patients with both Severe CDI was observed in 22 of 132 patients with both genetic elementsgenetic elements
• Severe CDI was not observed in any pt that did not have Severe CDI was not observed in any pt that did not have these genetic elements (p=0.03)these genetic elements (p=0.03)
Loo VG et al. NEJM 2005;353(23):2442.Loo VG et al. NEJM 2005;353(23):2442.
CDI: An Antibiotic-Resistance Issue?CDI: An Antibiotic-Resistance Issue?• Pittsburgh hospital outbreakPittsburgh hospital outbreak
– No isolates R to metronidazole or vancomycinNo isolates R to metronidazole or vancomycin– 85.7% R to clindamycin85.7% R to clindamycin
• Clindamycin was a significant riskClindamycin was a significant risk– 94.5% R to levofloxacin 94.5% R to levofloxacin
• Levofloxacin was a significant riskLevofloxacin was a significant risk
• Quebec hospitals OutbreakQuebec hospitals Outbreak– No isolates R to metronidazole, vancomycin or No isolates R to metronidazole, vancomycin or
clindamycinclindamycin• Clindamycin was not a significant riskClindamycin was not a significant risk
– 100% of predominate type isolates R to 100% of predominate type isolates R to ciprofloxacin, moxifloxacin, gatifloxacin, and ciprofloxacin, moxifloxacin, gatifloxacin, and levofloxacinlevofloxacin
• All FQ were associated with increased riskAll FQ were associated with increased risk
Muto et al. ICHE 2005;26:273., Loo VG et al. NEJM 2005;353(23):2442.Muto et al. ICHE 2005;26:273., Loo VG et al. NEJM 2005;353(23):2442.
CDI and FluoroquinolonesCDI and Fluoroquinolones• Characterization of 187 Characterization of 187 C. diffC. diff isolates from 8 isolates from 8
healthcare facilities from 2001-2003 and healthcare facilities from 2001-2003 and comparison to historic isolatescomparison to historic isolates– An epidemic strain was identified and was An epidemic strain was identified and was
responsible for 50% or more of the isolates from responsible for 50% or more of the isolates from most facilities (binary toxin and most facilities (binary toxin and tcdtcdC deletions in all)C deletions in all)
– This epidemic strain was in existence since 1984This epidemic strain was in existence since 1984– Compared to similar historic strains where no R to Compared to similar historic strains where no R to
FQ was detected, all recent strains were R to FQ was detected, all recent strains were R to gatifloxacin and moxifloxacingatifloxacin and moxifloxacin
– Conclusion: A previously uncommon strain of Conclusion: A previously uncommon strain of C. diff C. diff with variation in toxin genes has become more R to with variation in toxin genes has become more R to fluoroquinolones and has emerged as a cause of fluoroquinolones and has emerged as a cause of geographically dispersed outbreaks of CDIgeographically dispersed outbreaks of CDI
McDonald LC et al. NEJM 2005;353(23):2433.McDonald LC et al. NEJM 2005;353(23):2433.
C. diffC. diff: Community Setting: Community Setting
• 31 yo woman 14 weeks pregnant with twins developed 3 weeks 31 yo woman 14 weeks pregnant with twins developed 3 weeks of intermittent diarrhea- stool specimens positive for of intermittent diarrhea- stool specimens positive for C. diffC. diff– Only ABX exposure was TMP-SXT 3 mo priorOnly ABX exposure was TMP-SXT 3 mo prior– Treated but ultimately developed severe disease hospitalized for Treated but ultimately developed severe disease hospitalized for
18 days18 days– Had recurrent disease 4 days after discharge, spontaneously Had recurrent disease 4 days after discharge, spontaneously
aborted her fetuses, developed sepsis and diedaborted her fetuses, developed sepsis and died• CDC and Philadelphia Department of Public Health launched CDC and Philadelphia Department of Public Health launched
investigationinvestigation
C. diffC. diff: Community Setting: Community Setting• 33 cases of CA-CDI were reported from NH, PA, 33 cases of CA-CDI were reported from NH, PA,
NJ, OH, all but 1 occurring in 2004-2005 NJ, OH, all but 1 occurring in 2004-2005 – 15 (46%) required hospitalization or an ED visit15 (46%) required hospitalization or an ED visit– 13 (39%) had a relapse requiring treatment13 (39%) had a relapse requiring treatment– 8 (24%) reported no ABX exposure in prior 3 months8 (24%) reported no ABX exposure in prior 3 months
• 3 of these cases had exposure to patient with “diarrheal 3 of these cases had exposure to patient with “diarrheal illness” (2 confirmed C. diff)illness” (2 confirmed C. diff)
– Of those who had received ABX (25 patients)Of those who had received ABX (25 patients)• 3 had received 3 had received <<3 doses, 2 had received only 1 dose3 doses, 2 had received only 1 dose• 10 reported exposure to clindamycin10 reported exposure to clindamycin
– 10 among peripartum women10 among peripartum women• Transmission to close contacts evident for 4 patientsTransmission to close contacts evident for 4 patients
– 23 among non-peripartum individuals23 among non-peripartum individuals• Ages 6 mo to 72 years (mean 26 years)Ages 6 mo to 72 years (mean 26 years)
C. diffC. diff: Community Setting: Community Setting
• The estimated minimum annual The estimated minimum annual incidence of CA-CDI in Philadelphia incidence of CA-CDI in Philadelphia and its surrounding four counties and its surrounding four counties – 7.6 per 100,000 population7.6 per 100,000 population– One case for every 5,549 outpatient ABX One case for every 5,549 outpatient ABX
prescriptionsprescriptions• Twice as high as the <1 case per 10,000 cited in Twice as high as the <1 case per 10,000 cited in
earlier studiesearlier studies
C. diffC. diff: Community Setting: Community Setting
• ConclusionsConclusions– These cases of severe CDI among individuals These cases of severe CDI among individuals
previously thought to be at low risk might reflect previously thought to be at low risk might reflect changing epidemiologychanging epidemiology
– Certain features of CDI that have been uncommon Certain features of CDI that have been uncommon in the past might be changingin the past might be changing
• Close-contact transmissionClose-contact transmission• High recurrence rateHigh recurrence rate• Younger age patientsYounger age patients• Lack of ABX exposureLack of ABX exposure
– Because reporting was voluntary, the true Because reporting was voluntary, the true incidence of CDI is likely higherincidence of CDI is likely higher
• Clostridium DifficileClostridium Difficile– Emerging issues related to CDI include an Emerging issues related to CDI include an
increase in overall disease incidence associated increase in overall disease incidence associated with an epidemic strain that contains a mutation with an epidemic strain that contains a mutation for increased toxin production and thus more for increased toxin production and thus more severe disease with higher risk of death. This severe disease with higher risk of death. This strain has an increased rate of resistance to strain has an increased rate of resistance to certain antimicrobials, particularly certain antimicrobials, particularly fluoroquinolones, which may be driving the rates. fluoroquinolones, which may be driving the rates. Additionally, the epidemiology of CDI in the Additionally, the epidemiology of CDI in the community, previously thought to be low risk, community, previously thought to be low risk, may be changing.may be changing.
CDI: TreatmentCDI: Treatment• Stop the inciting antibioticStop the inciting antibiotic
– Up to 25% will recover without further therapyUp to 25% will recover without further therapy
• Metronidazole vs. Vancomycin– Several older retrospective studies comparing oral
metronidazole to oral vancomycin • Metronidazole just as effective
– Response rates >95%
• Less expensive ($2 day vs. $70 day)• Less risk for VRE emergence and spread
– A recent prospective observational study• Response rate to metronidazole was only 78%
– Due to recent emergence of newer strain?
CDI: TreatmentCDI: Treatment• Metronidazole vs. Vancomycin
– Both drugs have good in vitro activity• Median MICs <1.0
– Both drugs promote VRE overgrowth in the stool during treatment
– Relapse rates after treatment are about the same for both drugs
– Controversy regarding gut levels of metronidazole
• Only present with active disease?
Wafa N. AAC 2008;52(7):2403-2406.
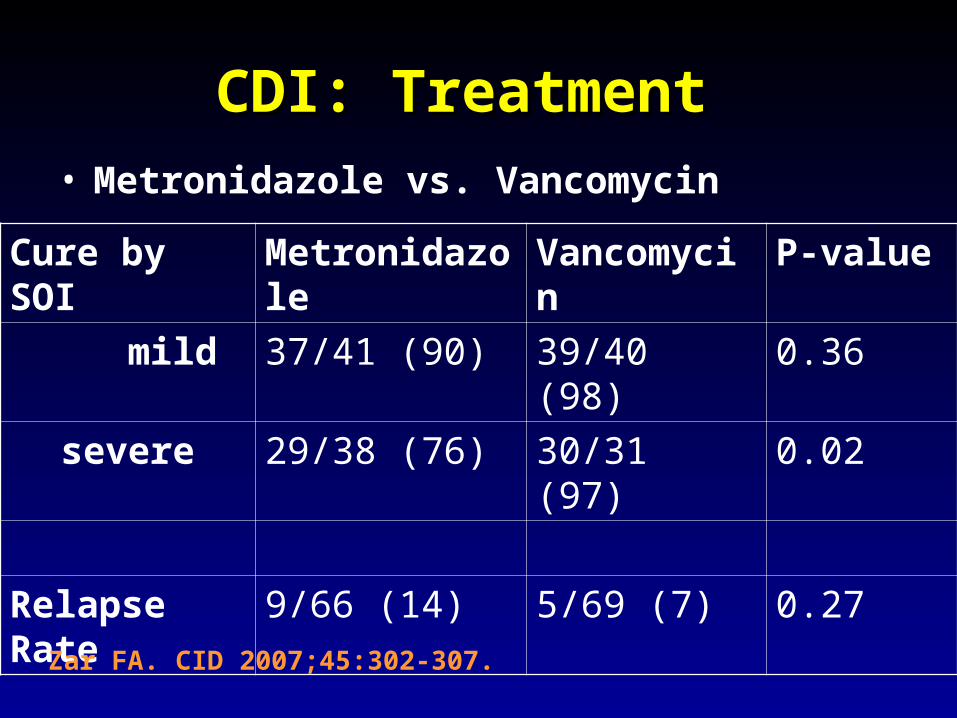
CDI: TreatmentCDI: Treatment • Metronidazole vs. Vancomycin
Cure by SOI Metronidazole Vancomycin P-value
mild 37/41 (90) 39/40 (98) 0.36
severe 29/38 (76) 30/31 (97) 0.02
Relapse Rate 9/66 (14) 5/69 (7) 0.27
Zar FA. CID 2007;45:302-307.
CDI: TreatmentCDI: Treatment • Metronidazole vs. Vancomycin
Cure by SOI Metronidazole Vancomycin P-value
mild 26/33 (79) 23/27 (85) NS
moderate 40/53 (75) 58/73 (80) NS
severe 37/58 (65) 28/33 (85) <0.05
Relapse Rate 29/100 (29) 27/103 (23) NS
Louie T. ICAAC 2007. Abstract K-4259.
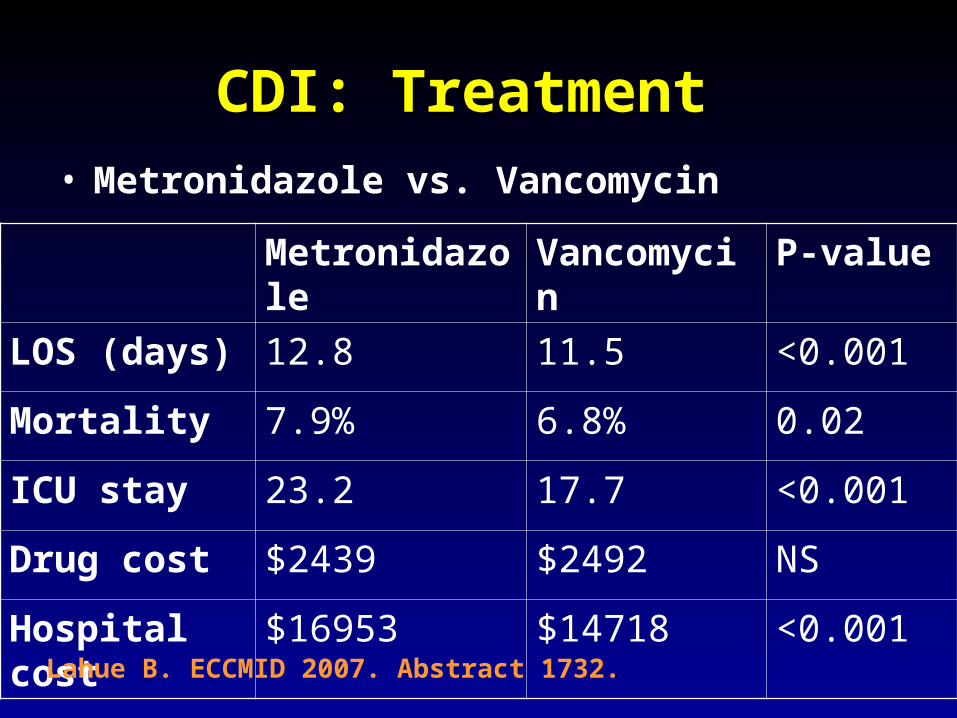
CDI: TreatmentCDI: Treatment • Metronidazole vs. Vancomycin
Metronidazole Vancomycin P-value
LOS (days) 12.8 11.5 <0.001
Mortality 7.9% 6.8% 0.02
ICU stay 23.2 17.7 <0.001
Drug cost $2439 $2492 NS
Hospital cost $16953 $14718 <0.001
Lahue B. ECCMID 2007. Abstract 1732.
CDI: TreatmentCDI: Treatment
• Appropriate antibiotics directed towards Appropriate antibiotics directed towards C. diff C. diff should should be given for 10 days for mild to moderate diseasebe given for 10 days for mild to moderate disease– Metronidazole (PO or IV), Vancomycin (PO)Metronidazole (PO or IV), Vancomycin (PO)
• Most experts recommend starting with Most experts recommend starting with metronidazolemetronidazole
• Clinicians should be vigilant about monitoring Clinicians should be vigilant about monitoring responseresponse
– If disease does not progress, should not consider If disease does not progress, should not consider treatment failure before 6-7 daystreatment failure before 6-7 days
– Vancomycin may be more appropriate for severe Vancomycin may be more appropriate for severe diseasedisease
• Intraluminal or oralIntraluminal or oral
– Consider surgery if CDI progresses or if severeConsider surgery if CDI progresses or if severe
CDI: Treatment
• Nitazoxanide vs. Vancomycin (severe disease)
Nitazoxanide Vancomycin P-value
EOT response
8/10 (80) 7/10 (70) NS
Relapse 1/10 (10) 1/10 (10) NS
Sustained response
7/10 (70) 6/10 (60) NS
Musher D. CID 2009;48:e41-e46.
CDI: Treatment• Fidaxomicin vs. Vancomycin
Package Insert DIFICID 2011.
Clinical Response EOT Sustained Response
Dificid Vanco Difference
(95% CI)
Dificid Vanco Difference
(95% CI)
Trial 1 88% 86% 2.6%
(-2.9-8.0)
70% 57% 12.7%
(4.4-20.9)
Trail 2 88% 87% 1.0%
(-4.8-6.8%)
72% 57% 14.8%
(5.9-23.3%)
Some evidence to suggest that Dificid may be better for non-B1 isolates of C Diff when compared to vancomycin (redcued recurrence). Equivalent for B1 isolates.
• Rifaximin (antibiotic): effective when Rifaximin (antibiotic): effective when used with vancomycin for recurrent used with vancomycin for recurrent diseasedisease
• Meta-analysis of 12 studies to identify Meta-analysis of 12 studies to identify risks for recurrent diseaserisks for recurrent disease– Continued use of non-CDI antibioticsContinued use of non-CDI antibiotics
• OR 4.23 95%CI 2.10-8.55, p<0.001OR 4.23 95%CI 2.10-8.55, p<0.001
– Concomitant receipt of antacid medicationsConcomitant receipt of antacid medications• OR 2.15 95%CI 1.13-4.08, p=0.02OR 2.15 95%CI 1.13-4.08, p=0.02
• No consensus on recurrent diseaseNo consensus on recurrent disease– Alternative agents, pulsed or tapering Alternative agents, pulsed or tapering
vancomycin coursesvancomycin courses– Ion-exchange resins and polymersIon-exchange resins and polymers– IVIG: some positive results in case reportsIVIG: some positive results in case reports
• Do not treat asymptomatic colonizationDo not treat asymptomatic colonization– Current therapies not effective for this purposeCurrent therapies not effective for this purpose
• Vancomycin effects not sustained and may place pts at Vancomycin effects not sustained and may place pts at risk for prolonged carriage after treatmentrisk for prolonged carriage after treatment
• Can only obtain significant intraluminal levels of Can only obtain significant intraluminal levels of metronidazole in presence of diarrheametronidazole in presence of diarrhea
CDI: Alternative RegimensCDI: Alternative Regimens• Meta-analysis of RR by Type of Probiotic for Meta-analysis of RR by Type of Probiotic for
Prevention of Antibiotic Associated DiarrheaPrevention of Antibiotic Associated Diarrhea
McFarland LV. Am J Gastro 2006;101:812.McFarland LV. Am J Gastro 2006;101:812.
• Meta-analysis of 6 RCT for Prevention of CDIMeta-analysis of 6 RCT for Prevention of CDI– RR 0.59, 95%CI 0.41- 0.85, p=0.005RR 0.59, 95%CI 0.41- 0.85, p=0.005– Only Saccharomyces showed significant reduction Only Saccharomyces showed significant reduction
for recurrent CDIfor recurrent CDI
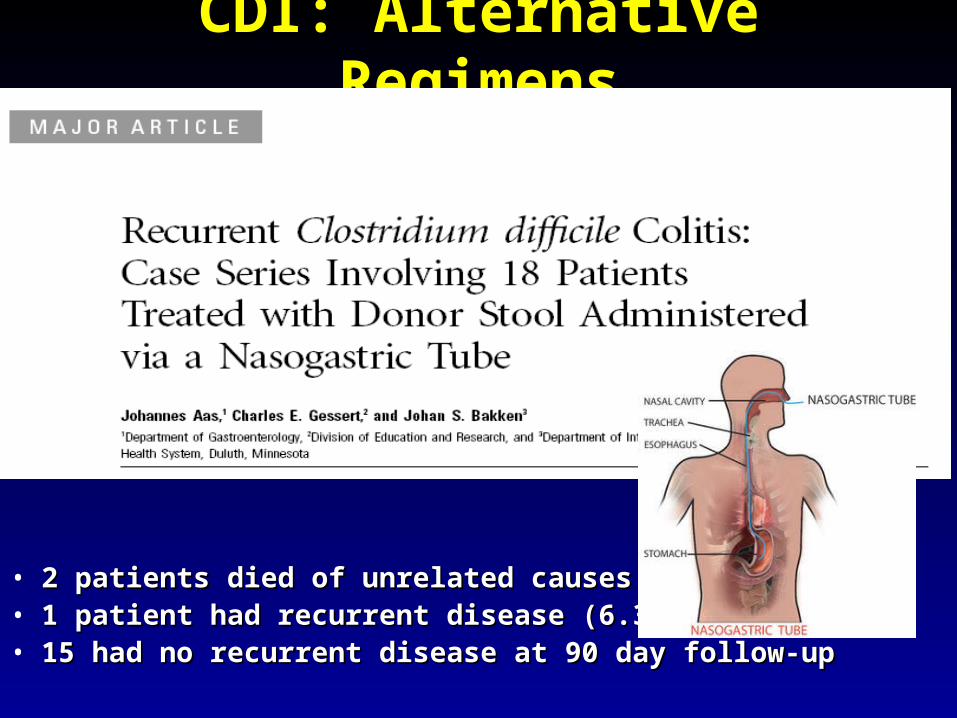
CDI: Alternative RegimensCDI: Alternative Regimens
• 2 patients died of unrelated causes2 patients died of unrelated causes• 1 patient had recurrent disease (6.3%)1 patient had recurrent disease (6.3%)• 15 had no recurrent disease at 90 day follow-up15 had no recurrent disease at 90 day follow-up
C. DiffC. Diff: Transmission: Transmission• Two major potential reservoirs of Two major potential reservoirs of C. diffC. diff in in
hospitals are patients and inanimate objectshospitals are patients and inanimate objects• ContinuedContinued pressure from indiscriminate pressure from indiscriminate
antibiotic useantibiotic use– Failure to stop antibiotics when they are no longer Failure to stop antibiotics when they are no longer
indicatedindicated
• Patients with symptomatic intestinal infection Patients with symptomatic intestinal infection probably contribute mostprobably contribute most– Contamination of the environment due to persistence Contamination of the environment due to persistence
of highly resistant sporesof highly resistant spores• Can persist for many weeks or months after the patient has Can persist for many weeks or months after the patient has
left the environmentleft the environment
– Personnel hand carriage probably accounts for the Personnel hand carriage probably accounts for the majority of hospital transmissionmajority of hospital transmission
Original (Incorrect) Hypothesis Original (Incorrect) Hypothesis for for C. diffC. diff Hospital Infection Hospital Infection
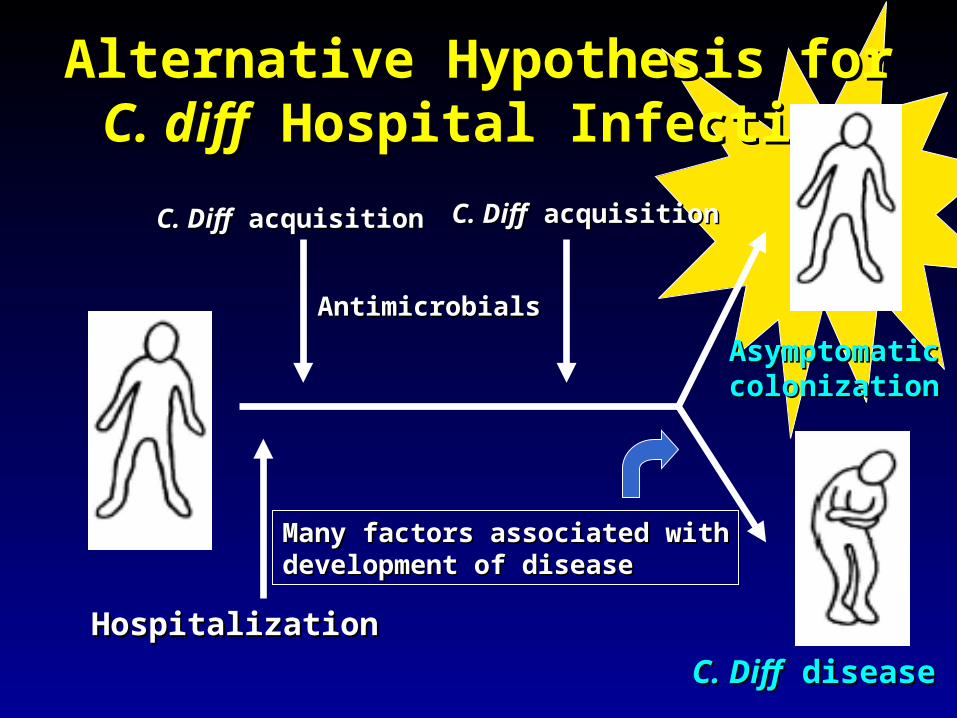
HospitalizationHospitalization
C. DiffC. Diff acquisition acquisition AntimicrobialsAntimicrobials
C. DiffC. Diff disease disease
Alternative Hypothesis for Alternative Hypothesis for C. diffC. diff Hospital InfectionHospital Infection
Many factors associated withMany factors associated withdevelopment of diseasedevelopment of disease
Asymptomatic Asymptomatic C. diffC. diff Colonization Colonization
• Data from four prospective studies in Data from four prospective studies in which rectal swabs were obtained which rectal swabs were obtained weekly from hospitalized patients:weekly from hospitalized patients:– Rates of CDI in non-colonized patients was Rates of CDI in non-colonized patients was
3.6% compared to 1.3% in colonized 3.6% compared to 1.3% in colonized patients (p=0.02)patients (p=0.02)
– Rate also significantly decreased when Rate also significantly decreased when only patients who received antibiotics only patients who received antibiotics were analyzed (p=0.02)were analyzed (p=0.02)
Lancet 1998;351:633-636Lancet 1998;351:633-636
Clostridium difficileClostridium difficile: Control: Control
• Consider two distinct but related Consider two distinct but related approachesapproaches– Efforts directed at interrupting horizontal Efforts directed at interrupting horizontal
spread (keep patient from acquiring spread (keep patient from acquiring organism)organism)
– Efforts to minimize the possibility that Efforts to minimize the possibility that exposure will result in infection (reduce exposure will result in infection (reduce individual risk of disease)individual risk of disease)
Control Measures: Prevention of CDIControl Measures: Prevention of CDI• Follow antimicrobial usage restrictions Follow antimicrobial usage restrictions • Avoid electronic thermometersAvoid electronic thermometers• Dedicate patient care itemsDedicate patient care items• Use full barrier precautions for CDI ptsUse full barrier precautions for CDI pts• Place CDI pts in private roomPlace CDI pts in private room• Perform appropriate hand hygienePerform appropriate hand hygiene• Perform adequate environmental Perform adequate environmental
SHEA/IDSA Practice Recommendations. SHEA/IDSA Practice Recommendations. ICHE ICHE 2008;29:Suppl 1.2008;29:Suppl 1.
Hand Hygiene and Hand Hygiene and C. diffC. diff Risk Risk
• Hand washing with soap or chlorhexidine is Hand washing with soap or chlorhexidine is equally effective in removing spores of equally effective in removing spores of C. diff C. diff from the seeded hands of volunteersfrom the seeded hands of volunteers
• Alcohol hand hygiene products are not Alcohol hand hygiene products are not sporicidal and not likely to reduce the burden sporicidal and not likely to reduce the burden of spores on hands when used without hand of spores on hands when used without hand washingwashing
• CDI outbreaks have NOT been directly CDI outbreaks have NOT been directly related to use of alcohol hand hygiene related to use of alcohol hand hygiene productsproducts
Control Measures: Prevention of CDIControl Measures: Prevention of CDI
• Approaches that should not be considered for routine prevention – Testing of asymptomatic patients
– Repeat testing of CDI pts after successful therapy
• Unresolved issues– Use of contact precautions by family members
– Standing nursing orders for testing
– Restricting gastric acid lowering medications
SHEA/IDSA Practice Recommendations. SHEA/IDSA Practice Recommendations. ICHE ICHE 2008;29:Suppl 1.2008;29:Suppl 1.
Prevention of Prevention of C. diffC. diff Hospital Hospital InfectionInfection
Give non-toxigenic Give non-toxigenic C. diffC. diff
• CDI: Treatment and ControlCDI: Treatment and Control– Effective treatment regimens have been Effective treatment regimens have been
developed for mild to moderate disease which developed for mild to moderate disease which include metronidazole, vancomycin, and include metronidazole, vancomycin, and fidaxomicin. Severe disease may require fidaxomicin. Severe disease may require alternative uses of traditional drug regimens and alternative uses of traditional drug regimens and possibly adjunctive agents. The transmissibility possibly adjunctive agents. The transmissibility of of C. diffC. diff has been well described in healthcare has been well described in healthcare facilities and control measures have been facilities and control measures have been recommended. Novel prevention methods are recommended. Novel prevention methods are being considered.being considered.
SummarySummary• Clostridium difficileClostridium difficile remains an important remains an important
nosocomial pathogennosocomial pathogen• The epidemiology of The epidemiology of Clostridium difficileClostridium difficile is is
changingchanging– Increased rates in acute care and long term care facilitiesIncreased rates in acute care and long term care facilities– Increased morbidity and mortalityIncreased morbidity and mortality– Possibly due to a genetically altered strain with increased Possibly due to a genetically altered strain with increased
virulencevirulence
• Effective treatment regimens existEffective treatment regimens exist– Study of new treatment regimens should continueStudy of new treatment regimens should continue
• Effective control measures have been Effective control measures have been describeddescribed– Study of new or enhanced control measures should continueStudy of new or enhanced control measures should continue