CME Two Hundred Ninety-Four Consecutive Facial Fractures in an Urban Trauma Center: Lessons Learned Patrick Kelley, M.D., Marcus Crawford, M.D., Stephen Higuera, M.D., and Larry H. Hollier, M.D. Houston, Texas Learning Objectives: After studying this article, the participant should be able to: 1. Understand the different technical options available for repairing facial fractures. 2. Know which technical points facilitate performance of fixation of the facial skeleton by relatively inexperienced surgeons. 3. Have a basic understanding of the most common complications arising after facial fracture repair. 4. Have an understanding of how to avoid surgical complications following facial fracture repair. Background: The treatment of facial trauma is associated with a myriad of po- tential complications. This may be com- pounded by the relative lack of compliance seen in the patient population within an urban trauma center and by the requisite involvement of residents in this care. Methods: This study retrospectively evalu- ated 189 patients with a total of 294 separate fractures treated over a 3.5-year period. Results: The overall rate of complications was 7.8 percent. Conclusions: The experience at a high-vol- ume level I trauma center with residents as the primary physicians has confirmed that facial trauma surgery may be undertaken with an acceptably low complication rate. Numer- ous technical factors were thought to be re- sponsible for this, including the use of miniplates for treatment in the majority of mandibular fractures, overcorrection of or- bital volume in fractures involving the globe, and the use of a transconjunctival incision with a lateral canthotomy for access to the lower eyelid structures. (Plast. Reconstr. Surg. 116: 42e, 2005.) Among the myriad injuries seen in urban trauma centers, facial trauma is one of the most common. Given the broad variety of facial bone injuries seen, management can be com- plicated even for the most experienced clini- cian. This takes on added significance when one considers that residents in training are frequently involved in the care of these pa- tients. Although there are numerous ways to handle many facial skeletal injuries, the expe- rienced surgeon entrusted with the training of residents must always be cognizant of empha- sizing those methods that provide the desired outcome for the relative novice. Only as train- ees become more skilled with their technique should more complex methods be introduced. This study evaluated a large group of pa- tients at a level I urban trauma center under- going surgical management of facial skeletal injuries. In all cases, the same faculty plastic surgeon (and senior author, Dr. Hollier) was scrubbed with a sixth-year plastic surgery resi- dent acting in the capacity of surgeon. The results of these operations in terms of compli- cations were examined. Technical aspects of the operation, which were thought to improve the overall outcome while minimizing the com- plexity of the procedure itself, are examined. From the Michael E. DeBakey Department of Surgery, Division of Plastic and Reconstructive Surgery, Baylor College of Medicine. Received for publication August 6, 2004; revised December 14, 2004. DOI: 10.1097/01.prs.0000177687.83247.27 42e
Transcript
CME
Two Hundred Ninety-Four Consecutive FacialFractures in an Urban Trauma Center:Lessons LearnedPatrick Kelley, M.D., Marcus Crawford, M.D., Stephen Higuera, M.D., and Larry H. Hollier, M.D.Houston, Texas
Learning Objectives: After studying this article, the participant should be able to: 1. Understand the different technical optionsavailable for repairing facial fractures. 2. Know which technical points facilitate performance of fixation of the facial skeletonby relatively inexperienced surgeons. 3. Have a basic understanding of the most common complications arising after facialfracture repair. 4. Have an understanding of how to avoid surgical complications following facial fracture repair.
Background: The treatment of facialtrauma is associated with a myriad of po-tential complications. This may be com-pounded by the relative lack of complianceseen in the patient population within anurban trauma center and by the requisiteinvolvement of residents in this care.Methods: This study retrospectively evalu-ated 189 patients with a total of 294 separatefractures treated over a 3.5-year period.Results: The overall rate of complicationswas 7.8 percent.Conclusions: The experience at a high-vol-ume level I trauma center with residents asthe primary physicians has confirmed thatfacial trauma surgery may be undertaken withan acceptably low complication rate. Numer-ous technical factors were thought to be re-sponsible for this, including the use ofminiplates for treatment in the majority ofmandibular fractures, overcorrection of or-bital volume in fractures involving the globe,and the use of a transconjunctival incisionwith a lateral canthotomy for access to thelower eyelid structures. (Plast. Reconstr. Surg.116: 42e, 2005.)
Among the myriad injuries seen in urbantrauma centers, facial trauma is one of themost common. Given the broad variety of facialbone injuries seen, management can be com-plicated even for the most experienced clini-cian. This takes on added significance whenone considers that residents in training arefrequently involved in the care of these pa-tients. Although there are numerous ways tohandle many facial skeletal injuries, the expe-rienced surgeon entrusted with the training ofresidents must always be cognizant of empha-sizing those methods that provide the desiredoutcome for the relative novice. Only as train-ees become more skilled with their techniqueshould more complex methods be introduced.
This study evaluated a large group of pa-tients at a level I urban trauma center under-going surgical management of facial skeletalinjuries. In all cases, the same faculty plasticsurgeon (and senior author, Dr. Hollier) wasscrubbed with a sixth-year plastic surgery resi-dent acting in the capacity of surgeon. Theresults of these operations in terms of compli-cations were examined. Technical aspects ofthe operation, which were thought to improvethe overall outcome while minimizing the com-plexity of the procedure itself, are examined.
From the Michael E. DeBakey Department of Surgery, Division of Plastic and Reconstructive Surgery, Baylor College of Medicine. Receivedfor publication August 6, 2004; revised December 14, 2004.
DOI: 10.1097/01.prs.0000177687.83247.27
42e
PATIENTS AND METHODS
We performed a retrospective analysis of 189patients with facial fractures treated at BenTaub General Hospital in Houston, Texas,from September of 1998 to February of 2002.All of the patients were treated by residents onthe plastic surgery service under the supervi-sion of one faculty surgeon at this level Itrauma center. Data were analyzed accordingto demographics, mechanism of injury, frac-ture location, and surgical complications. Thefollow-up ranged from 3 days to 5 years, with anaverage follow-up of 74 days.
Among the study group, 158 patients (84percent) were men and 31 (16 percent) werewomen. Most of the patients were between theages of 21 and 30 years (Fig. 1). As in otherretrospective reviews of facial trauma in theurban setting, interpersonal violence was theprimary mechanism of injury.1 Ninety-one pa-tients (48.1 percent) sustained injuries in thismanner. The remaining injuries were causedby automobile crashes, falls, automobile-pedestrian accidents, and contact sports (Fig.2). A history of drug and/or alcohol abuse wasreported by many patients. The most commonfractures treated were of the mandible (TableI). These 140 fractures constituted 47.6 per-cent of the group, followed by (in decreasingfrequency) fractures of the zygoma and frac-tures of the orbit (Fig. 3).
During the period of review, techniques ofexposure and fixation were uniform, as a singlefaculty surgeon supervised all procedures.Noncomminuted parasymphyseal and bodyfractures of the mandible were all treated in-traorally using miniplate fixation along theideal lines of osteosynthesis. Mandibular anglefractures were treated intraorally by placing asingle matrix or strut miniplate. Comminutedfractures and fractures involving substantialbone loss were treated with locking reconstruc-tion plates. All subcondylar fractures weretreated using maxillomandibular fixation. Or-bitozygomatic fractures were exposed using in-cisions in the gingivobuccal sulcus, transcon-junctivally in the lower eyelid and through alateral extension of the supratarsal fold in theFIG. 1. Facial trauma age distribution in years.
FIG. 2. Mechanisms of injury.
TABLE IFracture Location
Location No. (%)
Mandible 140(47.62)Zygoma 51(17.35)Orbit 33(11.22)Nose 19(6.46)Frontal sinus 15(5.1)Nasoethmoidal-orbital 14(4.76)Palate 9(3.06)Le Fort I 4(1.36)Le Fort II 4(1.36)Le Fort III 4(1.36)Panfacial 1(0.34)Total 294(100)
Vol. 116, No. 3 / FACIAL FRACTURES IN A TRAUMA CENTER 43e
upper eyelid. A coronal incision was only usedif the infraorbital rim and zygomatic buttresseswere so comminuted that adequate alignmentrequired arch visualization. A Carol-Gerardscrew was used for disimpaction and alignmentof the fracture in all cases. All orbital floor andmedial wall fractures were treated with syn-thetic implants, including titanium meshes,resorbable implants, and high-density porouspolyethylene. Exposure was exclusively bymeans of a transconjunctival approach.
RESULTS
During the follow-up period, 23 complica-tions were noted among the 294 fractures,yielding a 7.8 percent overall complicationrate. Twenty-one of the complications requiredoperative repair, whereas two were managedwith nonoperative therapy. Problems aftermandibular fracture repair contributed to only13 percent of the 23 complications. Among the13 patients with complications related to repairof a mandible fracture, six experienced a post-operative infection. The cause was most fre-quently hardware failure, treatment of whichconsisted of removal of hardware and replace-
ment by more rigid fixation. The remainingcomplications consisted of malocclusion, in-traoral plate exposure, orofacial fistula, tris-mus, and a failed free fibula flap. Numbness ofthe lower lip was not evaluated. There were nocomplications requiring operative repairwithin the subset of patients who receivedtreatment for subcondylar fractures, includingno cases of malocclusion.
Complications from orbital fracture repaircontributed to five of the 23 complications.Enophthalmos (acute or delayed) was seen inthree of the 33 orbital fracture repairs, result-ing in a 9 percent incidence of enophthalmosfollowing orbital fracture repair. The tech-nique for correction of postoperative enoph-thalmos involved repeated reconstruction witheither titanium or porous polyethylene im-plants. No patient demonstrated diplopia atthe time of last follow-up.
After repair of frontal sinus fractures, onepatient experienced an infection of the cal-cium phosphate bone cement used that re-quired removal, and another patient devel-oped postoperative sinusitis that was effectivelytreated with oral antibiotics. Of the 14 patientswho experienced nasoethmoidal-orbitalfractures, one patient experienced persistenttelecanthus. This was repaired with repeatedtransnasal wiring.
Table II lists all the complications that wereencountered and their subsequent manage-ment. Table III lists the complication rates byfracture location.
DISCUSSION
Since the initial descriptions by Michelet andothers of internal fixation with small plates andscrews for facial fractures, surgeons have devel-oped a myriad of techniques to accompany theongoing development of commercially avail-able materials.2 These methods are often vari-ations on traditional surgical approaches thathave been adjusted to appropriately fit specificclinical situations.
An examination of the data demonstratesthat the most common fracture treated was ofthe mandible (47.62 percent, n � 140). Ourtechniques vary depending on the type (simpleversus comminuted) and location of the frac-ture. In accordance with the principles de-scribed by Champy et al., miniplate fixationalong the ideal lines of osteosynthesis was thepreferred form of stabilization for simplefractures.3 When used in the appropriate situ-
FIG. 3. Facial fracture locations.
44e PLASTIC AND RECONSTRUCTIVE SURGERY, September 1, 2005
ations, there can be no question that miniplatefixation results in a lower incidence of maloc-clusion than does fixation with larger recon-struction plates. These smaller plates, typicallyaccommodating screws 2 mm in diameter, donot have to be precisely adapted to the man-dibular contour, as do larger plates. Of course,they are not applicable to all mandibular frac-tures. The greater the instability present in themandible, the more prone one should be touse larger plates. Comminuted fractures, frac-tures involving substantial bone loss, and mul-tiple mandibular fractures should cause one toconsider using larger reconstruction plates(Fig. 4). When such plates are chosen, how-ever, the surgeon should typically use lockingplates.4,5 Locking reconstruction plates func-tion in that the screw is threaded into the plate
at the end of its insertion, preventing the bonefrom being pulled up to a maladapted plate. Inessence, the plate acts as a form of “internal”external fixator. Consequently, just as withminiplates, one need not contour the plateexactly to the shape of the underlying mandi-ble. These are less likely to result in a maloc-clusion. In addition, loose screws should theo-retically never be seen, as the screw isdependent on the plate itself for stability andnot its contact with the bone.
Another important point is the appropriatetreatment of subcondylar fractures. There aremany advocates of open reduction. Most pointout that the results of the open approach arebetter with respect to range of opening, dimin-ished deviation on opening, and restoration ofthe mandibular contour at rest.6–8,11 Althoughthis may be the case, the real question is
TABLE IIIFracture Location, Complications, and Complication Rate
TABLE IIFracture Repair, Complications, and Correction
Fracture Repair Complications Correction
Mandible Intraoral plate exposure Pectoralis flap coverageMandible body Infected ORIF Removal of infected tension bandMandible body Infected ORIF Extraction of retained tooth rootsMandible body Infected ORIF I & D, removal of loose screwMandible angle Malocclusion Removal of strut plates, MMFMandible angle Orofacial fistula Closure of fistulaMandible parasymphysis Infected ORIF Removal of 2.0 plate, replaced with 2.4 LRMandible angle Infected ORIF Third molar extractionMandible angle Infected ORIF Third molar extraction and LR plate replacementMandible angle Screws in fracture line Repeat ORIFMandible body Failed free fibula to reconstruct lateral defect Repeat free fibulaMandible Soft-tissue infection Debridement and antibiotic therapyMandible angle/subcondylar Trismus Oral exercisesOrbital floor Delayed enophthalmos Medpor wedgeOrbital floor Entropion Palatal graft for entropionOrbital floor Extrusion of hardware Removal of hardwareOrbital floor Lower lid retraction MassageOrbital floor Enophthalmos Repeat ORIF with titanium meshFrontal sinus fracture Infected Mimex RemovalFrontal sinus Sinusitis Antibiotic therapyOrbitozygoma fracture Enophthalmos Medpor wedgeZygomatic arch fracture Malunion Osteotomy and replatingNOE Telecanthus Repeat ORIF and transnasal wiring
ORIF, open reduction and internal fixation; NOE, nasoethmoidal-orbital.
FIG. 4. Locking plate.
Vol. 116, No. 3 / FACIAL FRACTURES IN A TRAUMA CENTER 45e
whether or not the additional morbidity of theopen approach is worth it. That is, even thougha patient treated in a closed fashion for a sub-condylar fracture often deviates with maximalopening and has some loss of definition of thejawline at rest, we have yet to have a patientcomplain of this. This must be contrasted witha potential facial nerve injury secondary toopening a subcondylar injury. With most openapproaches to reduce and plate the condylarregion, facial nerve injury is the primary con-cern. Even though this is typically temporary,the surgeon cannot know this immediatelypostoperatively. Many of these patients must befollowed for months before recovery is appar-ent. In addition, recovery of the nerve is notalways complete, with ongoing facial asymme-try being problematic. Although there hasbeen a great deal of interest in the endoscopicapproach, this has a very steep learningcurve.9,10 As such, for all but the most experi-enced surgeons, it is entirely appropriate totreat the majority of these patients in maxillo-mandibular traction of some sort. The type ofintermaxillary fixation and its duration are en-tirely dependent on the patient’s occlusion. Inthose cases in which, once all other mandibu-lar fractures are fixated, the occlusion is at itspreinjury level despite the subcondylar injury,no further treatment or intermaxillary elasticsare quite acceptable. However, when the occlu-sion is still quite disordered following fixationof the other mandibular fractures, strong con-sideration should be given to maxillomandibu-lar wires. Given the relative unreliability ofmany patients with these injuries, elasticsshould generally not be trusted. The durationof intermaxillary fixation depends entirely onthe level of the subcondylar fracture and theseverity of the malocclusion being treated.Rarely, however, should it exceed 3 to 4 weeks.It is important to note that intermaxillary fixa-tion never truly reduces the fracture. Rather, itforces the patient to functionally adapt the biteto the existing subcondylar displacement, re-storing the preinjury occlusion.
This is not to say, however, that no subcon-dylar fracture should be treated in an openfashion.11 In any patient in whom intermaxil-lary fixation is contraindicated, such as thosewith a severe poorly controlled seizure disor-der, open reduction should be strongly consid-ered. In addition, in patients with massive pan-facial injuries with bilateral subcondylarfractures, open reduction of one side should
be considered to establish the posterior facialheight. We must emphasize that no subcondy-lar injuries in this series were treated in anopen fashion.
Mandibular angle fractures must be givenspecial attention. These are some of the mostdifficult fractures to treat successfully. Thereare several issues to consider, including diffi-culty with intraoral visualization and the prob-lem of third molar management. Although themajority of uncomplicated angle fractures maybe managed using intraoral incisions andtransbuccal drill and screw placement, consentshould be given by all patients for an externalincision should the intraoral approach provetoo problematic. When placing fixation usingthe intraoral approach, we have found the ma-trix or strut plate to be very useful (Fig. 5).Generally the plate is placed in the midportionof the angle and secured using 6-mm-longscrews that are 2 mm in diameter. The plateitself needs no contouring and provides excel-lent stabilization.
With respect to the management of thirdmolars, the literature is replete with differentviewpoints.12–15 The only real benefit to reten-tion of this tooth is in its contribution to thestability of the angle. When large plates (2.4mm) are used for fracture fixation, there isrelatively little benefit to retaining the molar.However, when the intraoral approach is usedand small plates are applied, serious consider-ation should be given to maintaining the toothif possible because it adds stability. In general,the novice surgeon should err on the side ofremoving the molar when there is any questionregarding the condition of the periodontal tis-sues or possible damage to the molar itself.
FIG. 5. Mandibular strut/matrix plate rigidly fixating amandibular angle fracture (note that the mandibular thirdmolar has been removed).
46e PLASTIC AND RECONSTRUCTIVE SURGERY, September 1, 2005
Two infections in this series occurred in anglefractures with third molars left in position.
With respect to malar injuries, the most com-mon severe complication seen wasenophthalmos.16,17 Even in the best of hands,this is not an uncommon complication. Whenteaching residents the technique for correctingthe fracture, there are several important pointsto emphasize. First, the vast majority of theseinjuries can be corrected without a coronalincision. The only instance in which the coro-nal incision is needed is when there is so muchcomminution at the level of the infraorbitalrim and the zygomaticomaxillary buttress thatthese two cannot be used for accurate position-ing of the fragment. In these situations, visual-ization and alignment of the zygomatic archare helpful. Perhaps the most important pointto emphasize in teaching reduction and fixa-tion of malar fractures is the need to overcor-rect the position of the globe (Fig. 6). At theend of procedure, the globe on the affectedside should project more anteriorly than theunaffected globe. Given the swelling inducedby the injury and the operation, the eye on theoperative side must project more. If at the endof the procedure the globes are symmetric, oneshould expect postoperative enophthalmos. Ifthe overcorrection is not seen at the end of theprocedure, the surgeon has several options.One option is to remove the fixation and re-position the malar fragment. However, if thesurgeon is confident in the positioning of thezygoma, the second option is to overcorrect theorbital floor and intraorbital volume. As thevast majority of these injuries do require repairof the orbital floor, this may be the source ofthe error. One should not hesitate to add extravolume to the orbital cone should the globenot be in an appropriate position at the end ofthe procedure. In this series, only one of 51
malar fractures developed clinically significantenophthalmos using this philosophy.
Another important technical aspect facilitat-ing correction of the malar position is the useof a Carol-Gerard screw (Fig. 7). This instru-ment is available as a self-drilling screw thatmay be placed through the lower eyelid inci-sion into the zygoma, allowing it to be usedessentially as a handle. One may use this toboth disimpact the zygoma and to position itmuch like a joystick for fixation. This greatlyfacilitates ease of handling of the zygoma dur-ing these procedures.
In isolated orbital injuries, the same issuesapply with respect to enophthalmos.17,18 At theend of the procedure to reconstruct the frac-tured walls, the orbital volume should be over-corrected. The globe should project more an-teriorly. If it does not, adding additionalvolume to the orbital cone is mandatory toensure appropriate position postoperatively.Only one of the 33 patients with orbital floorinjuries developed clinically significant enoph-thalmos in this series. On repeated scanning,the enophthalmos in this case was thought tobe related solely to inaccurate reconstructionresulting in an increase in orbital volume.
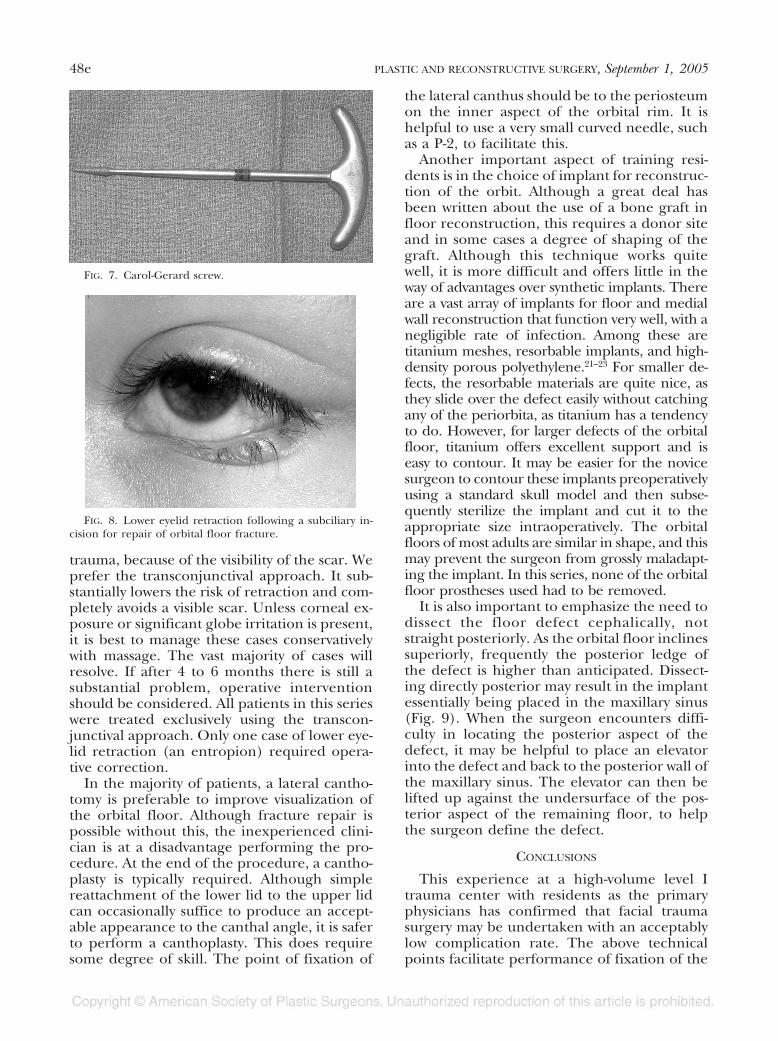
Another major issue in teaching techniquesof orbital surgery is to studiously avoid thetranscutaneous approaches to the orbital floor.There can be no question when the literatureand personal experience are reviewed thatlower eyelid retraction is much more commonwhen transcutaneous lower eyelid approachesare used for facial trauma (Fig. 8).19 The oneexception may be a subtarsal approach to thelower eyelid in which the skin incision is placedlow on the eyelid in a preexisting crease.20
Although this may be applicable to older pa-tients, it should generally be avoided for themore common younger patient with facial
FIG. 6. Overcorrection of the right globe consistent with anatomical reconstruc-tion of an orbital floor fracture.
Vol. 116, No. 3 / FACIAL FRACTURES IN A TRAUMA CENTER 47e
trauma, because of the visibility of the scar. Weprefer the transconjunctival approach. It sub-stantially lowers the risk of retraction and com-pletely avoids a visible scar. Unless corneal ex-posure or significant globe irritation is present,it is best to manage these cases conservativelywith massage. The vast majority of cases willresolve. If after 4 to 6 months there is still asubstantial problem, operative interventionshould be considered. All patients in this serieswere treated exclusively using the transcon-junctival approach. Only one case of lower eye-lid retraction (an entropion) required opera-tive correction.
In the majority of patients, a lateral cantho-tomy is preferable to improve visualization ofthe orbital floor. Although fracture repair ispossible without this, the inexperienced clini-cian is at a disadvantage performing the pro-cedure. At the end of the procedure, a cantho-plasty is typically required. Although simplereattachment of the lower lid to the upper lidcan occasionally suffice to produce an accept-able appearance to the canthal angle, it is saferto perform a canthoplasty. This does requiresome degree of skill. The point of fixation of
the lateral canthus should be to the periosteumon the inner aspect of the orbital rim. It ishelpful to use a very small curved needle, suchas a P-2, to facilitate this.
Another important aspect of training resi-dents is in the choice of implant for reconstruc-tion of the orbit. Although a great deal hasbeen written about the use of a bone graft infloor reconstruction, this requires a donor siteand in some cases a degree of shaping of thegraft. Although this technique works quitewell, it is more difficult and offers little in theway of advantages over synthetic implants. Thereare a vast array of implants for floor and medialwall reconstruction that function very well, with anegligible rate of infection. Among these aretitanium meshes, resorbable implants, and high-density porous polyethylene.21–23 For smaller de-fects, the resorbable materials are quite nice, asthey slide over the defect easily without catchingany of the periorbita, as titanium has a tendencyto do. However, for larger defects of the orbitalfloor, titanium offers excellent support and iseasy to contour. It may be easier for the novicesurgeon to contour these implants preoperativelyusing a standard skull model and then subse-quently sterilize the implant and cut it to theappropriate size intraoperatively. The orbitalfloors of most adults are similar in shape, and thismay prevent the surgeon from grossly maladapt-ing the implant. In this series, none of the orbitalfloor prostheses used had to be removed.
It is also important to emphasize the need todissect the floor defect cephalically, notstraight posteriorly. As the orbital floor inclinessuperiorly, frequently the posterior ledge ofthe defect is higher than anticipated. Dissect-ing directly posterior may result in the implantessentially being placed in the maxillary sinus(Fig. 9). When the surgeon encounters diffi-culty in locating the posterior aspect of thedefect, it may be helpful to place an elevatorinto the defect and back to the posterior wall ofthe maxillary sinus. The elevator can then belifted up against the undersurface of the pos-terior aspect of the remaining floor, to helpthe surgeon define the defect.
CONCLUSIONS
This experience at a high-volume level Itrauma center with residents as the primaryphysicians has confirmed that facial traumasurgery may be undertaken with an acceptablylow complication rate. The above technicalpoints facilitate performance of fixation of the
FIG. 7. Carol-Gerard screw.
FIG. 8. Lower eyelid retraction following a subciliary in-cision for repair of orbital floor fracture.
48e PLASTIC AND RECONSTRUCTIVE SURGERY, September 1, 2005
facial skeleton by relatively inexperienced sur-geons. Although there are many ways for theexperienced physician to approach facial frac-tures, some of the techniques do require agreater degree of skill. As with any reconstruc-tive procedure, the specifics of the patient’sfracture pattern are the ultimate guide to theappropriate technique.
Larry H. Hollier, M.D.Clinical Care Center, Suite 6206621 Fannin Street, MC CC 620.10Houston, Texas [email protected]
ACKNOWLEDGMENTS
Financial support for this study was provided by WalterLorenz Surgical, Inc. Dr. Larry H. Hollier, Jr., also receivesadditional financial support from Walter Lorenz Surgical,Inc., for his research team.
REFERENCES
1. Scherer, M., Sullivan, W. G., Smith, D. J., Jr.,Phillips, L.G., and Robson, M. C. An analysis of 1423 facialfractures in 788 patients at an urban trauma center. J.Trauma 29: 388, 1989.
2. Michelet, F. X., Deymes, J., and Dessus, B. Osteosyn-thesis with miniaturized screwed plates in maxillofa-cial surgery. J. Maxillofac. Surg. 1: 79, 1973.
3. Champy, M., Lodde, J. P., Schmitt, R., et al. Mandibularosteosynthesis by miniature screwed plates via buccalapproach. J. Maxillofac. Surg. 6: 14, 1978.
4. Ellis, E., and Graham, J. Use of a 2.0mm locking plate/screw system for mandibular fracture surgery. J. OralMaxillofac. Surg. 60: 642, 2002.
5. Herford, A. S., and Ellis, E. Use of a locking recon-struction bone plate/screw system for mandibular sur-gery. J. Oral Maxillofac. Surg. 56: 1261, 1998.
6. Yang, W. G., Chen, C. T., Tsay, P. K., and Chen, Y.R. Functional results of unilateral mandibular con-dylar process fractures after open and closed treat-ment. J. Trauma 52: 498, 2002.
7. Worsaae, N., and Thorn, J. J. Surgical versus nonsurgi-cal treatment of unilateral dislocated low subcondylarfractures: A clinical study of 52 cases. J. Oral Maxillofac.Surg. 52: 353, 1994.
8. Ellis, E., McFadden, D., Simon, P., and Throckmorton,G. Surgical complications with open treatment ofmandibular condylar process fractures. J. Oral Maxil-lofac. Surg. 58: 950, 2000.
9. Chen, C. T., Lai, J. P., Tung, T. C., and Chen, Y. R. En-doscopically assisted mandibular subcondylar fracturerepair. Plast. Reconstr. Surg. 103: 60, 1999.
10. Lee, C., Mueller, R., Lee, K., and Mathes, S. Endoscopicsubcondylar fracture repair: Functional, aesthetic,and radiographic outcomes. Plast. Reconstr. Surg. 102:1434, 1998.
11. Zide, M. F., and Kent, J. N. Indications for open reduc-tion of mandibular condyle fractures. J. Oral Maxillo-fac. Surg. 41: 89, 1983.
12. Fuselier, J. C., Ellis, E. E., and Dodson, B. Do mandib-ular third molars alter the risk of angle fracture? J. OralMaxillofac. Surg. 60: 515, 2002.
13. Halmos, D. R., Ellis, E. E., and Dodson, T. B. Mandibu-lar third molars and angle fractures. J. Oral Maxillofac.Surg. 62: 1076, 2004.
14. Meisami, T., Sojat, A., Sandor, G. K., Lawrence, H. P., andClokie, C. M. Impacted third molars and risk of an-gle fractures. Int. J. Oral Maxillofac. Surg. 21: 140, 2002.
15. Chan, D. M., Demuth, R. J., Miller, S. H., and Jastak,J. T. Management of mandibular fractures in unre-liable patient populations. Ann. Plast. Surg. 13: 298,1984.
16. Souyris, F., Klersy, F., Jammet, P., and Payrot, C. Malarbone fractures and their sequelae: A statistical study of1393 cases covering a period of 20 years. J. Craniomax-illofac. Surg. 17: 64, 1989.
17. Hosal, B. M., and Beatty, R. L. Diplopia and enoph-thalmos after surgical repair of blowout fractures. Or-bit 21: 27, 2002.
18. Kawamoto, H. K. Late posttraumatic enophthalmos: A cor-rectable deformity? Plast. Reconstr. Surg. 69: 423, 1982.
19. Patel, P. C., Sobota, B. T., Patel, N. M., Greene, J. S., andMillman, B. Comparison of transconjunctival versussubciliary approaches for orbital fractures: A review of60 cases. J. Craniomaxillofac. Surg. 4: 17, 1998.
20. Rohrich, R. J., Janis, J. E., and Adams, W. P., Jr. Sub-ciliary versus subtarsal approaches to orbitozygomaticfractures. Plast. Reconstr. Surg. 111: 1708, 2003.
21. Hollier, L. H., Rogers, N., Berzin, E., and Stal,S. Resorbable mesh in the treatment of orbital floorfractures. J. Craniofac. Surg. 12: 242, 2001.
22. Jacono, A. A., and Moskoowitz, B. Alloplastic implants fororbital wall reconstruction. Facial Plast. Surg. 16: 63.
23. Ellis, E., and Tan, Y. Assessment of internal orbital recon-struction for pure blowout fractures: Cranial bone graftsversus titanium mesh. J. Oral Maxillofac. Surg. 61: 442, 2003.
FIG. 9. Orbital floor implant in the maxillary sinus.
Vol. 116, No. 3 / FACIAL FRACTURES IN A TRAUMA CENTER 49e