CMS in the 21 st Century 23rd Annual HFMA Southern California and San Diego/Imperial Chapter Fall Conference David Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco September 10, 2013
Transcript
CMS in the 21st CenturyCMS in the 21st Century
23rd Annual HFMA Southern California and San Diego/Imperial
Chapter Fall Conference
David Saÿen, MBARegional Administrator
Centers for Medicare & Medicaid ServicesSan Francisco
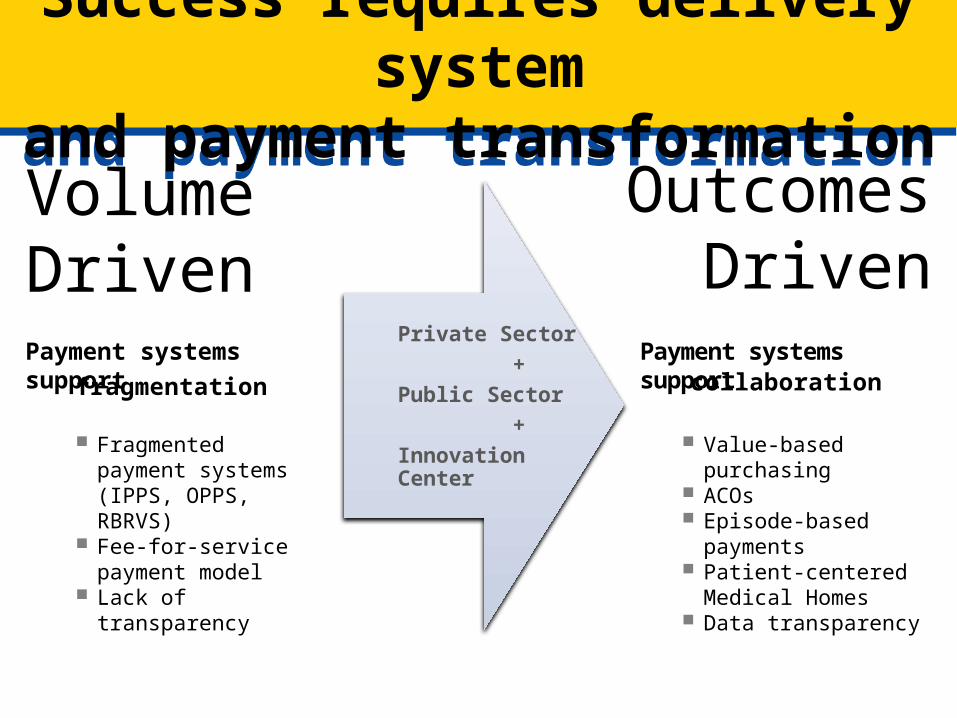
Value-based purchasing ACOs Episode-based payments Patient-centered Medical
Homes Data transparency
Volume Driven
Outcomes Driven
Payment systems supportcollaboration
Payment systems support
fragmentation
Fragmented payment systems (IPPS, OPPS, RBRVS)
Fee-for-service payment model
Lack of transparency
Private Sector +Public Sector +Innovation Center
Value-Based Purchasing Program Objectives over Time Towards Attainment of the Three-Part AimValue-Based Purchasing Program Objectives over Time Towards Attainment of the Three-Part Aim
Initial programs FY2012-2013
Proposed and near-term programsFY2014-2016
Longer-term FY2017+
•Limited to hospitals (HVBP) and dialysis facilities (QIP)•Existing measures providers recognize and understand•Focus on provider awareness, participation, and engagement
•Expand to include physicians•New measures to address HHS priorities•Increasing emphasis on patient experience, cost, and clinical outcomes•Increasing provider engagement to drive quality improvements, e.g., learning and action networks
•VBP measures and incentives aligned across multiple settings of care and at various levels of aggregation (individual physician, facility, health system)•Measures are patient-centered and outcome oriented•Measure set addresses all 6 national priorities well•Rapid cycle measure development and implementation•Continued support of QI and engagement of clinical community and patients•Greater share of payment linked to quality
Vision for VBP
FY2013 HVBP Program SummaryFY2013 HVBP Program Summary
• Two domains:
• Clinical Process of Care (12 measures)
• Patient Experience of Care (8 HCAHPS dimensions)
• Hospitals are given points for Achievement and Improvement for each measure or dimension, with the greater set of points used
• 70% of Total Performance Score based on Clinical Process of Care measures
• 30% of Total Performance Score based on Patient Experience of Care dimensions
• Payment adjustments in process
13 Clinical Process of Care Measures8 Patient Experience of
Care Dimensions 1. AMI-7a Fibrinolytic Therapy Received within 30 Minutes of Hospital Arrival
2. AMI-8 Primary PCI Received within 90 Minutes of Hospital Arrival
3. HF-1 Discharge Instructions4. PN-3b Blood Cultures Performed in the ED Prior to
Initial Antibiotic Received in Hospital5. PN-6 Initial Antibiotic Selection for CAP in
Immunocompetent Patient6. SCIP-Inf-1 Prophylactic Antibiotic Received within
One Hour Prior to Surgical Incision7. SCIP-Inf-2 Prophylactic Antibiotic Selection for
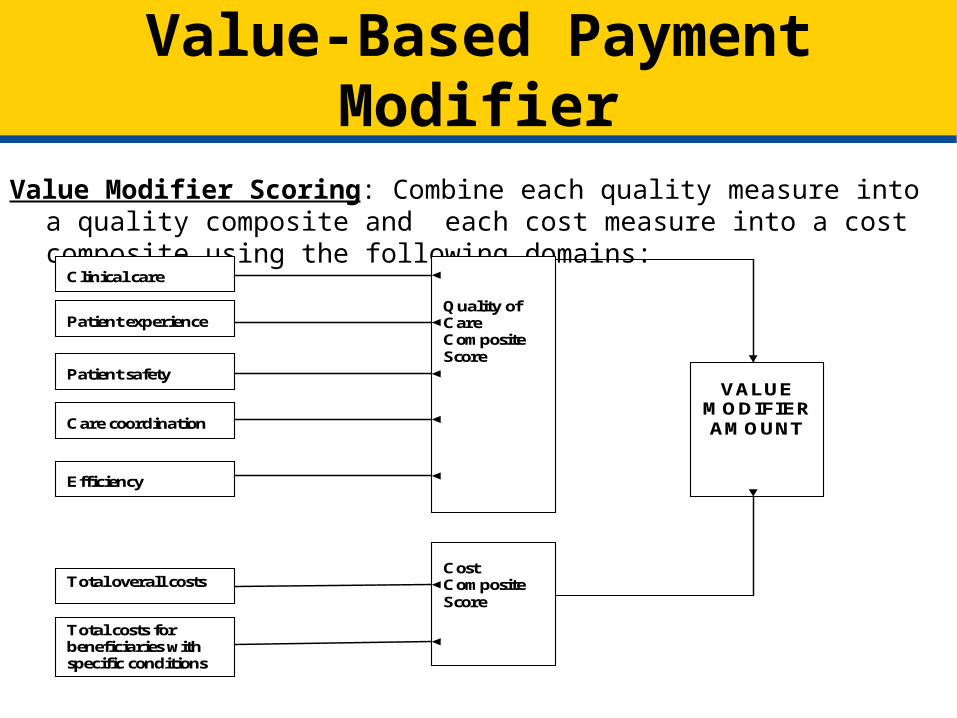
Value Modifier Scoring: Combine each quality measure into a quality composite and each cost measure into a cost composite using the following domains:
Clinical care
Patient experience
Patient safety
Care coordination
Efficiency
Total overall costs
Total costs for beneficiaries with specific conditions
Quality of Care Composite Score
Cost Composite Score
VALUE MODIFIER AMOUNT
• Readmissions penalties for applicable hospitals starting FY 13• The FY 2012 IPPS/LTCH PPS Final Rule sets forth:
• Conditions and readmissions to which program will apply for the first program year
• Readmission measures/methodology and calculation of readmission rates (e.g., CMS will use 30-day AMI, HF, and PN measures based on 3 years of data: July 1, ‘08 - June 30, ‘11)
• Public reporting of readmission data• Next year’s (FY13) proposed rule will include specific information
regarding payment adjustment• For more information, see:
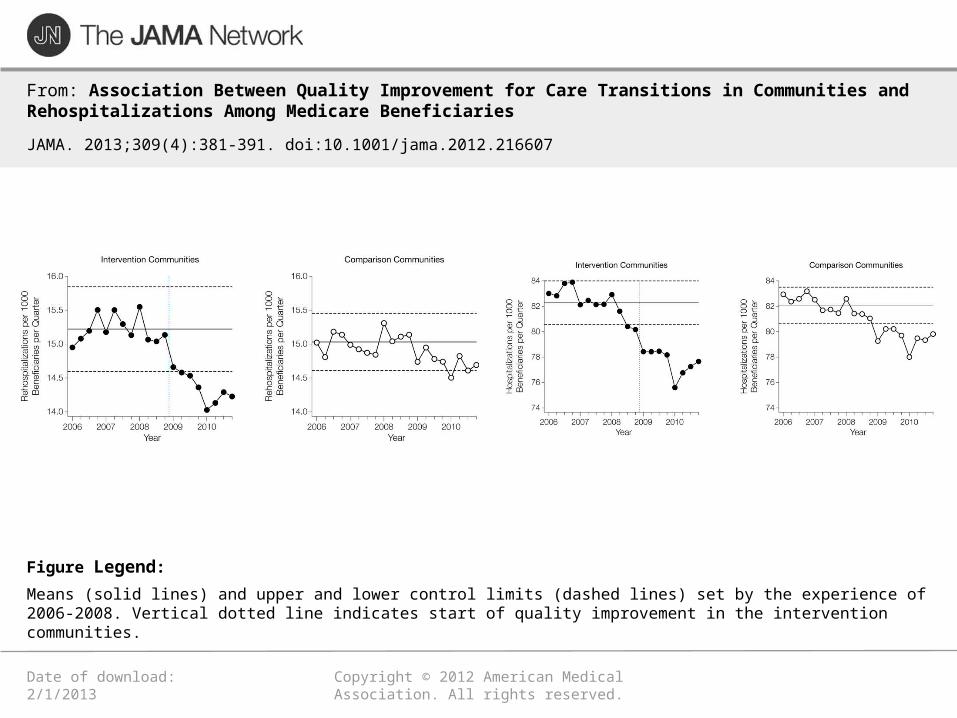
Means (solid lines) and upper and lower control limits (dashed lines) set by the experience of 2006-2008. Vertical dotted line indicates start of quality improvement in the intervention communities.
Figure Legend:
Fee for Service Medicare Recovery Audit Program Fee for Service Medicare Recovery Audit Program
• The Recovery Auditors are CMS contractors who are tasked with detecting and correcting improper payments
• Statute gives CMS the authority to pay the Recovery Auditors on a contingency fee basis.
• Primarily review claims after they are paid (post payment review)
• In September 2012, CMS implemented a 3-year demonstration to allow for prepayment review in 11 error-prone states (including California and Missouri for Region D)
Fee for Service Medicare Recovery Audit Program Fee for Service Medicare Recovery Audit Program
Fee for Service Medicare Recovery Audit ProgramFee for Service Medicare Recovery Audit Program
FY 2012 Results
• Overpayments Collected - $2.291 billion• Underpayments Restored - $109.4 million• Total Program Corrections - $2.4 billion
Fee for Service Medicare Recovery Audit Program Fee for Service Medicare Recovery Audit Program
FY 2012 Results – California
FY 2012 Results – Region D (includes California)
FY 2012 Results – Region D (includes California)
• Top Overpayment Issues– Minor Surgery and Other Treatment Billed as Inpatient– Medical Necessity Review of Surgical Cardiovascular
Procedures– Medical Necessity Review of Neurological Conditions
• Top Underpayment Issues– Incorrect Patient Status– MS-DRG Validation of Gastrointestinal Procedures– MS-DRG Validation of Nervous System Procedures
Pioneer ACOs Succeed in Improving Care, Lowering Costs
Pioneer ACOs Succeed in Improving Care, Lowering Costs
Key results for performance year 1:
• 40% Pioneer ACOs produced shared savings with CMS, generating a gross savings of $87.6 million in 2012 and a net savings of $33 million to Medicare.
• Costs for Pioneer ACO beneficiaries grew by only 0.3%. This is below historical Medicare growth rates and well below the 0.8% growth rate for similar beneficiaries.
• As a group, Pioneer ACOs generated gross savings of $87.6 million, or 1.2 percent savings on a total benchmark of $7.59 billion for over 669,000 beneficiaries.
• Pioneer ACOs successfully reported quality measures and performed better than the Medicare fee-for-service population on a variety of measures, such as blood pressure and cholesterol control measures
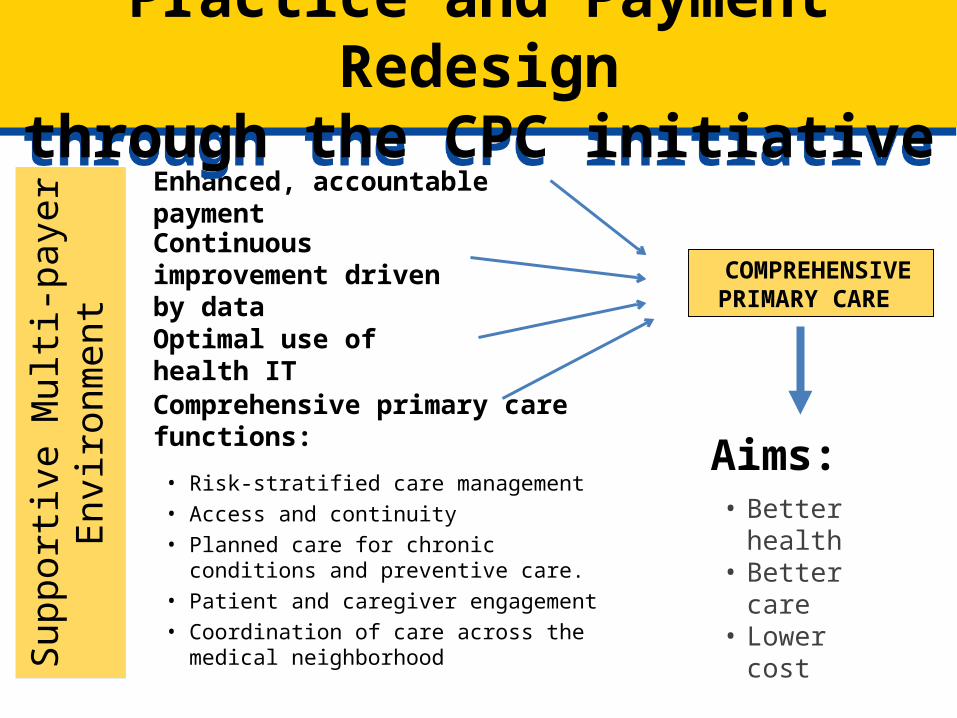
COMPREHENSIV
EPRIMARY CARE
Aims:• Better
health• Better
care • Lower
cost
Continuous improvement driven by data
Comprehensive primary care functions:
• Risk-stratified care management• Access and continuity• Planned care for chronic conditions
and preventive care.• Patient and caregiver engagement• Coordination of care across the
medical neighborhood
Enhanced, accountable payment
Optimal use of health IT
Sup
port
ive M
ult
i-payer
En
vir
onm
ent
Practice and Payment Redesignthrough the CPC initiative
Practice and Payment Redesignthrough the CPC initiative
1. Risk-stratified care management
2. Access and continuity
3. Planned care for chronic conditions and preventive care
4. Patient and caregiver engagement
5. Coordination of care across the medical neighborhood
• Many free preventive services and a free annual wellness visit.
• A 52.5% discount on covered brand-name medications for those in the prescription drug donut hole. More than 6.6 million beneficiaries have saved over $7 billion since the law was signed. The donut hole will be closed in 2020.
• Cracks down on fraud to protect Medicare, including tougher penalties for criminals.
• Makes sure your doctors can spend more time with you and improve care coordination.
• Improvements that extend the lifeof the Medicare Trust Fund.
The Law Strengthens MedicareThe Law Strengthens Medicare
• Many preventive services like flu shots, diabetes screenings, mammograms, and other cancer screenings are free.
• Every year, you can get a free Wellness Visit – a chance to sit down and spend more time with your doctor to discuss your health.
• In the first six months of 2013, 16.5 million people with traditional Medicare received at least one of these free services.
• Before the law passed, a person with traditional Medicare could pay as much as $160 for some colorectal screenings – today , it is free.
The Law Keeps Seniors HealthyThe Law Keeps Seniors Healthy
• Seniors in Medicare now get 52.5% off their covered brand-name drugs and 21% off of the cost of generic drugs while in the donut hole.
• This discount has saved Californians $573,726,255 on prescription drugs.
• These savings occur at the pharmacy. You don’t have to file any forms or wait for a check.
• The donut hole will be closed by 2020.
The Law Saves Seniors MoneyThe Law Saves Seniors Money
The health care law provides unprecedented new tools and resources to fight and prevent fraud and abuse in Medicare.
The Law Cracks Down on Fraud and Abuse
The Law Cracks Down on Fraud and Abuse
“Metro Detroit Man Charged in $30 million Medicare Fraud Scheme”
-- Detroit Free Press
“Fraud Offenders Convicted in Massive Home Healthcare Case”
-- The Miami Herald
“Health Care Fraud Prosecutions on Pace To Rise 85%”
-- USA Today
• Some seniors with multiple chronic conditions see an average of 14 different doctors and fill 50 prescriptions a year.
• The health care law helps doctors and nurses coordinate care using electronic health records.
• The law helps your doctors and specialists stay on the same page, helping you spend more time with your doctor.
The Law Helps Improve CareThe Law Helps Improve Care
• Protection from the worst insurance company abuses
• Makes health care more affordable
• Better access to care
The Law Helps FamiliesThe Law Helps Families
The Law Helps FamiliesThe Law Helps Families
• Insurance companies can no longer deny coverage to children with pre-existing conditions.
• An additional 3.0 million young adults have health insurance (435,000 in California).
• Millions more Americans have access to free preventive services.
• Insurance companies are more accountable to consumers.
• Thousands of new doctors and nurses around the country.
• The law protects all your guaranteed Medicare benefits.
• You can continue to choose your own doctor.
• Seniors still have access to a strong Medicare Advantage program.
• The law adds 10 years to the life of the MedicareTrust Fund.
Did You Know…Did You Know…
• A new way to get health insurance• Enrollment starts October 1, 2013
• Coverage begins January 2014
• About 25 million Americans will have access to quality health insurance– Up to 20 million may qualify for
help to make it more affordable
– Working families can get help through the Marketplace
The Health Insurance MarketplaceThe Health Insurance Marketplace
• Help will be available in the Marketplace– Toll-free call center - 24/7
• 150 languages– Website chat 24/7 (English and Spanish)– Help in-person
• Navigators • Other trained enrollment assisters
– Local Community Health Centers, libraries, hospitals and other locations in local communities
• Agents and brokers
Assistance – It’s Available If You Need ItAssistance – It’s Available If You Need It
Learn MoreLearn More
https://www.healthcare.gov/
1-800-318-2596
http://www.coveredca.com/
1-888-975-1142
Contact InformationContact Information
David W. SaÿenRegional AdministratorSan Francisco Regional OfficeCenters for Medicare & Medicaid [email protected]