4/28/2016 1 CMS UPDATES: CY 2016 OPPS and What it Means to Your Hospital John Zelem, MD, FACS, VP, Clinical & Regulatory Agenda • CY2016 Outpatient Prospective Payment System Final Rule • Short Inpatient Hospital Stays • QIO Review of Short Inpatient Hospital Stays • Recovery Audit Program Updates • Utilization Review, Best Practices, and Benchmarks
Transcript
4/28/2016
1
CMS UPDATES: CY 2016 OPPS and What it Means to Your Hospital
John Zelem, MD, FACS, VP, Clinical & Regulatory
Agenda
• CY2016 Outpatient Prospective Payment System Final Rule
• Short Inpatient Hospital Stays
• QIO Review of Short Inpatient Hospital Stays
• Recovery Audit Program Updates
• Utilization Review, Best Practices, and Benchmarks
• The 2016 Outpatient Prospective Payment System final rule was published on October 30, 2015 and became effective on January 1, 2016.
• The rule finalized two key provisions:
1. Short inpatient hospital stays (stays when the physician expects the beneficiary to require less than two midnights of hospital care) are payable on a case-by-case basis; and
2. A shift in medical review strategy to have Quality Improvement Organizations (QIOs), and not the Medicare Administrative Contractors (MACs), conduct these reviews of short inpatient stays.
4
4/28/2016
3
Short Inpatient Hospital Stays
Did CMS eliminate the 2-midnight rule when it finalized its policy to allow for Medicare Part A payment on a case-by-case basis for inpatient admissions that do not satisfy the 2-midnight benchmark?
No.
And, Maybe.
5
2-Midnight Rule Recap – The Benchmark and Presumption
The 2-Midnight Benchmark:
“Surgical procedures, diagnostic tests, and other treatments would be generally considered appropriate for inpatient hospital admission and payment under Medicare Part A when the physician expects the patient to require a stay that crosses at least 2 midnights and admits the patient to the hospital based upon that expectation.” – 80 FR 70539
“For purposes of determining whether the 2-midnight benchmark is met and, therefore, whether an inpatient admission is appropriate for Medicare Part A payment, we consider the physician’s expectation including the total time spent receiving hospital care—not only the expected duration of care after inpatient admission, but also any time the beneficiary has spent (before inpatient admission) receiving outpatient services, such as observation services, treatments in the emergency department, and procedures provided in the operating room or other treatment area.” – 80 FR 70539
6
4/28/2016
4
2-Midnight Rule Recap – The Benchmark and Presumption
The 2-Midnight Presumption:
“Under the 2-midnight presumption, inpatient hospital claims with lengths of stay greater than 2 midnights after the formal admission following the order are presumed to be appropriate for Medicare Part A payment and are not the focus of medical review efforts, absent evidence of systematic gaming, abuse, or delays in the provision of care in an attempt to qualify for the 2-midnight presumption.” – 80 FR 70539
7
“Rare and Unusual” Circumstances
• “In the FY 2014 IPPS final rule we stated the 2-midnight benchmark provides that hospital stays expected to last less than 2 midnights are generally inappropriate for hospital admission and Medicare Part A payment absent rare and unusual circumstances. In that rule, we stated that we would provide additional subregulatory guidance on those circumstances.”
– CMS Questions and Answers Relating to Patient Status Reviews (3/12/14)
• “Under the existing rare and unusual policy, only one exception –prolonged mechanical ventilation – has been identified to date.”
– 80 FR 70541
8
4/28/2016
5
“Rare and Unusual” Circumstances continued
“After consideration of the public comments we received, we are finalizing, without modification, our proposal to revise our previous “rare and unusual” exceptions policy to allow for Medicare Part A payment on a case-by-case basis for inpatient admissions that do not satisfy the 2-midnight benchmark, if the documentation in the medical record supports the admitting physician’s determination that the patient requires inpatient hospital care despite an expected length of stay that is less than 2 midnights.” – 80 FR 70545
9
Are Short Inpatient Hospital Stays Rare and Unusual?
• “We would like to clarify that our proposed modification to the current exceptions process does not define inpatient hospital admissions with expected lengths of stay less than 2 midnights as rare and unusual. Rather, it modifies our current “rare and unusual” exceptions policy to allow Medicare Part A payment on a case-by-case basis for inpatient admissions that do not satisfy the 2-midnight benchmark.” – 80 FR 70545
10
4/28/2016
6
2016 OPPS Final Rule – Short Inpatient Hospital Stays
“When a beneficiary enters a hospital for a surgical procedure not specified as inpatient only under § 419.22(n), a diagnostic test, or any other treatment, and the physician expects to keep the beneficiary in the hospital for only a limited period of time that does not cross 2 midnights, the services would be generally inappropriate for payment under Medicare Part A.” – 80 FR 39349
Prior Guidance
“Under the proposed policy change, for stays for which the physician expects the patient to need less than 2 midnights of hospital care and the procedure is not on the inpatient only list or on the national exception list, an inpatient admission would be payable on a case-by-case basisunder Medicare Part A in those circumstances under which the physician determines that an inpatient stay is warranted and the documentation in the medical record supports that an inpatient admission is necessary.” – 80 FR 70541
Post 1/1/2016 Guidance
11
CY 2016 OPPS Final Rule Summary
• Staying the same:
“We did not propose any changes for hospital stays that are expected to be greater than 2 midnights; that is, if the physician expects the patient to require hospital care that spans at least 2 midnights and admits the patient based on that expectation, the services are generally appropriate for Medicare Part A payment.” – 80 FR 70541
“We also did not propose to change the 2-midnight presumption.” – 80 FR 70541
12
4/28/2016
7
Custodial, Convenience, and Delay
• Staying the same:
“Notwithstanding any other provision of this title, no payment may be made under part A or part B for any expenses incurred for items or services where such expenses are for custodial care.” – Social Security Act, §1862(a)(9)
“CMS' longstanding instruction has been and continues to be that hospital care that is custodial, rendered for social purposes or reasons of convenience, and is not required for the diagnosis or treatment of illness or injury, should be excluded from Part A payment.” – CMS Questions and Answers Relating to Patient Status Reviews (3/12/14)
“Any evidence of systematic gaming, abuse or delays in the provision of care in an attempt to receive the 2-midnight presumption could warrant medical review.” – CMS Questions and Answers Relating to Patient Status Reviews (3/12/14)
Inpatient Admission Orders
• “For purposes of payment under Medicare Part A, an individual is considered an inpatient of a hospital, including a critical access hospital, if formally admitted as an inpatient pursuant to an order for inpatient admission by a physician or other qualified practitioner.” – 42 CFR §412.3
• Key considerations:
– The inpatient admission order is a Condition of Payment
– The inpatient admission order must be signed/authenticated by a physician or other practitioner
– The inpatient admission order must be signed/authenticated prior to discharge
• For payment purposes, the following factors, among others, would be relevant to determining whether an inpatient admission where the patient stay is expected to be less than 2 midnights is nonetheless appropriate for Part A payment:
– The severity of the signs and symptoms exhibited by the patient;
– The medical predictability of something adverse happening to the patient; and
– The need for diagnostic studies that appropriately are outpatient services (that is, their performance does not ordinarily require the patient to remain at the hospital for 24 hours or more).
– 80 FR 70541
16
4/28/2016
9
Short Inpatient Hospital Stays – Then and Now
• What is the difference between what constituted an appropriate short inpatient hospital stay prior to the 2-Midnight rule’s implementation on October 1, 2013 and what will be considered appropriate as a result of the 2016 OPPS policy modification being implemented on January 1, 2016?
– From a clinical perspective?
• Nothing. “Consistent with our longstanding policy, all inpatient admissions must be medically reasonable and necessary and be supported by documentation in the patient’s medical record.” – 80 FR 70545
• Chapter 1, § 10 of the Medicare Benefit Policy Manual remains unchanged.
17
Short Inpatient Hospital Stays – Then and Now
• What is the difference between what constituted an appropriate short inpatient hospital stay prior to the 2-Midnight rule’s implementation on October 1, 2013 and what will be considered appropriate as a result of the 2016 OPPS policy modification being implemented on January 1, 2016?
– “Consistent with longstanding Medicare policy, the decision to formally admit a patient to the hospital is subject to medical review.” – 80 FR 70541
– “For cases not meeting the 2-midnight benchmark,… payment of the claim under Medicare Part A will be subject to the clinical judgment of the medical reviewer.” – 80 FR 70541
– “Cases for which the physician determines that an inpatient admission is necessary, but that do not span at least 1 midnight, would be prioritized for medical review.” – 80 FR 70541
18
4/28/2016
10
[Section Break Slide – Insert Section Title]QIO Review of Short Inpatient Hospital Stays
QIO Review of Short Inpatient Hospital Stays
• “We are changing our medical review strategy for short hospital stays and will have QIO [Quality Improvement Organization] contractors conduct reviews of short inpatient stays.” – 80 FR 70546
– The MACs will no longer be responsible for conducting these types of reviews (as they had been under Probe & Educate).
– This change in medical review strategy was effective as of October 1, 2015.
20
4/28/2016
11
QIO Review of Short Inpatient Hospital Stays
• Short stay reviews will be performed by the two Beneficiary and Family Centered Care QIOs (BFCC-QIOs): Livanta and KePRO.
• “BFCC-QIOs have begun to conduct post-payment reviews of claims and refer findings to the MACs for payment adjustments.” – 80 FR 70546
• “BFCC-QIOs will educate hospitals about claims denied under the 2-midnight policy and collaborate with these hospitals in their development of a quality improvement framework to improve organizational processes and/or systems” – 80 FR 70546
21
QIO Referral to Recovery Auditors
• Under the QIO short-stay inpatient review process, hospitals that are found to exhibit the following pattern of practices will be referred to the Recovery Auditor:
– Having high denial rates;
– Consistently failing to adhere to the 2-midnight rule;
– Having frequent inpatient hospital admissions for stays that do not span one midnight; or
– Failing to improve their performance after QIO educational intervention
Source: 80 FR 70546
22
4/28/2016
12
QIO Referral to Recovery Auditors
• In the CY 2016 OPPS final rule, commenters stated the need for transparency in the medical review process and requested additional information regarding the process for identifying providers deemed to be appropriate for Recovery Auditor referral.
• CMS Response: We will address technical medical review questions posed by the commenters in subregulatory guidance.
Source: 80 FR 70548
23
One more thing about BFCC-QIOs
• In the final rule, CMS said, “BFCC-QIOs will educate hospitals about claims denied under the 2-midnight policy and collaborate with these hospitals in their development of a quality improvement framework to improve organizational processes and/or systems.”
– Based on the post-payment review results, your hospital’s processes may come under scrutiny.
• But don’t wait for the QIO to ask! Now is the time to ask yourself:
– What is our process?
– What is the process we engage with to make appropriate inpatient admission decisions?
– Is this process consistent with recommended best practices and does it comply with all applicable Conditions of Participation?
24
4/28/2016
13
[Section Break Slide – Insert Section Title]Recovery Audit Program Updates
The Recovery Audit Program – Patient Status Reviews
• CMS announced in August 2015 that it will not approve Recovery Auditors to conduct patient status reviews until January 1, 2016.
• At that time, the Recovery Auditors will conduct patient status reviews focused on those providers that are referred from the QIOs based on their high denial rates.
• The number of claims a Recovery Auditor will be allowed to review for patient status will be based on the claim volume of the hospital and the denial rate identified by the QIO.
Source: 80 FR 70546
26
4/28/2016
14
The Recovery Audit Program – Current Status
• November 6, 2015 – CMS announced that the Requests for Proposals (RFPs) for the next round of Recovery Audit contracts were released.
• CMS seeks to close out current contracts by July 31, 2016.
• CMS has obtained modifications to the current Recovery Audit contracts that would permit each of the existing Recovery Auditors to continue recovery activities through July 31, 2016.
– Performant Recovery, CGI Federal, HealthDataInsights, and Cotiviti(formerly Connolly) have signed contract modifications allowing them to continue sending Additional Documentation Requests (ADRs).
• Enhancements in place as of November 6, 2015 status update:
– RAs must maintain an overturn rate of less than 10% at the first level of appeal.
– RAs must maintain an accuracy rate of at least 95%.
– Limited the RA look-back period to 6 months from the date of service for patient status reviews, in cases where the hospital submits the claim within 3 months of the date of service.
– RAs to incrementally apply the ADR limits to new providers under review.
– RAs must provide consistent and more detailed review information concerning new issues to their websites.
Source: Recovery Audit Program Enhancements (status as of November 6, 2015)
28
4/28/2016
15
Recovery Audit Program - Enhancements
• Enhancements which became effective January 1, 2016:
– CMS has the ADR limits for facility claims across all claim types of a facility.
– CMS is establishing ADR limits based on a provider’s compliance with Medicare rules.
Source: Recovery Audit Program Enhancements (status as of November 6, 2015)
29
Recovery Audit Program - Enhancements
• Enhancements that require modifications to the current contracts:
– RAs will have 30 days, instead of the current 60, to complete complex reviews and notify providers of their findings.
– RAs must wait 30 days to allow for a discussion request before sending the claim to the MAC for adjustment.
– RAs must confirm receipt of a provider’s discussion request within 3 business days.
– CMS will require the RAs to broaden their review topics to include all claim/provider types.
• Enhancements to be incorporated into new contracts:
– RAs will not receive a contingency fee until after the second level of appeal is exhausted.
Source: Recovery Audit Program Enhancements (status as of November 6, 2015)
30
4/28/2016
16
[Section Break Slide – Insert Section Title]Utilization Review, Best Practices, and Benchmarks
Recommended Utilization Review Plan & Components
• The hospital must have in effect a utilization review (UR) plan that provides for review of services furnished by the institution and by members of the medical staff to patients entitled to benefits under the Medicare and Medicaid programs
PLAN
INTERPRET
REVIEW
• The UR Plan is the documented process by which the organization will adhere to the standards identified in the Conditions of Participation as well as the defined operational standard for the Utilization Review Committee
• The committee must review professional services provided in order to determine medical necessity and to promote the most efficient use of available health facilities and services
32
4/28/2016
17
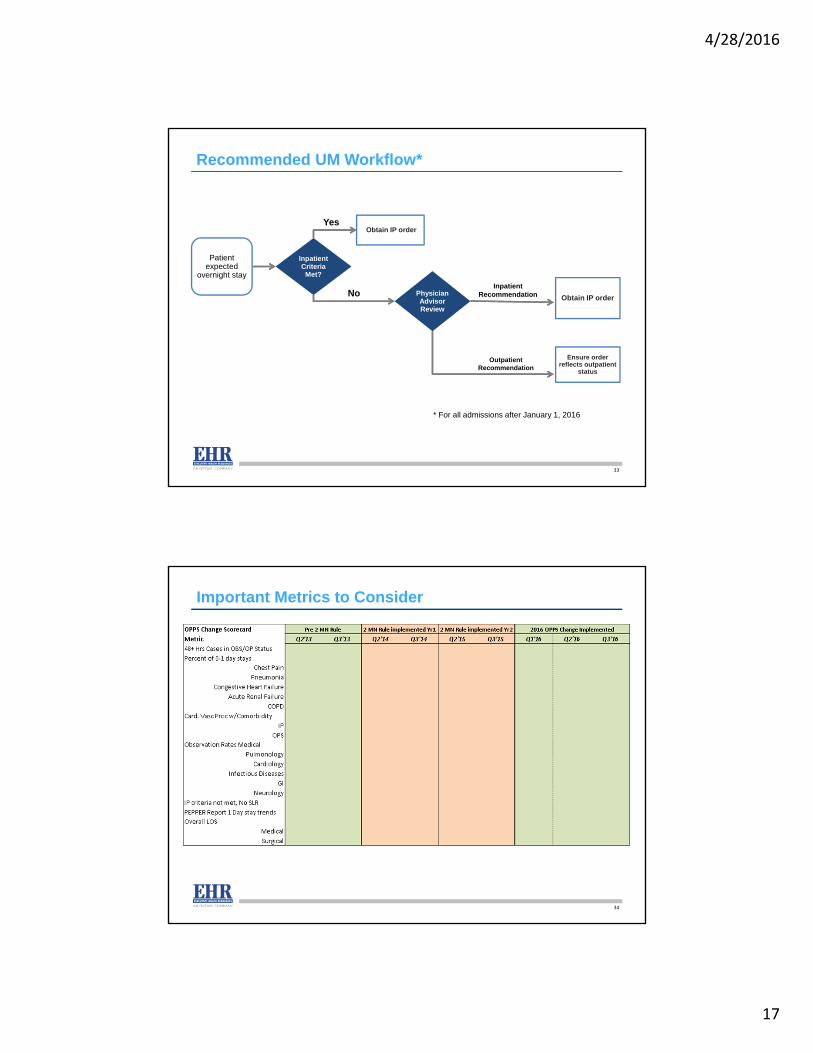
Recommended UM Workflow*
Inpatient Criteria
Met?
Obtain IP order
Obtain IP order
Ensure order reflects outpatient
status
Physician Advisor Review
InpatientRecommendation
OutpatientRecommendation
Patient expected
overnight stay
No
Yes
* For all admissions after January 1, 2016
33
Important Metrics to Consider
34
4/28/2016
18
Summary
• OPPS final rule is very similar to proposed rule
• Does not change 2 midnight rule but allows for more exceptions if medical necessity and documentation are clear
• Expect increased audits in 2016
• Clinical and Utilization Review documentation never more important
No part of this presentation may be reproduced or distributed.Permission to reproduce or transmit in any form or by any meanselectronic or mechanical, including presenting, photocopying,recording and broadcasting, or by any information storage andretrieval system must be obtained in writing from Executive Health Resources. Requests for permission should be directed to [email protected].
























![Medicare Program; CY 2018 Updates to the Quality …...Medicare Program; CY 2018 Updates to the Quality Payment Program [CMS-5522-P] Summary of Proposed Rule Subject Page I. Introduction](https://static.documents.pub/doc/80x56/5f086c667e708231d421f073/medicare-program-cy-2018-updates-to-the-quality-medicare-program-cy-2018-updates.jpg)

![ASPEN 11.2 Updates - surveyor-training …surveyor-training-content2.s3.amazonaws.com/data/172/LTCSP_Webin… · LTCSP ASPEN 11.2 Updates LTCSP 1. This is [Synora Jones] from CMS](https://static.documents.pub/doc/80x56/5ba16f5609d3f2b66a8c4903/aspen-112-updates-surveyor-training-surveyor-training-content2s3-ltcsp.jpg)