October 12, 2017 CMS's Quality Payment Program: Maximizing Your Performance under the Merit-based Incentive Payment System Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health
Transcript
October 12, 2017
CMS's Quality Payment Program: Maximizing Your Performance under the
Merit-based Incentive Payment System
Elizabeth Arend, MPH
Quality Improvement AdvisorNational Council for Behavioral Health
Medicare Access and CHIP
Reauthorization Act (MACRA) of
2015
• Repeals the Sustainable
Growth Rate formula
• Creates a new Quality
Payment Program by
streamlining existing programs
What is MACRA?
The Big Picture
Clinicians can choose either:
• The Merit-Based Incentive
Payment System (MIPS), which
streamlines multiple quality
programs
• An Advanced Alternative
Payment Model (APM), which
provides bonus payments for
participation
Two Paths to Payment:
MACRA’s New Quality Payment Program
• Require participants to use certified EHR technology • Require participants to bear “more than nominal
financial risk” …therefore not an option for most providers
– Comprehensive ESRD Care (CEC) - Two-Sided Risk– Comprehensive Primary Care Plus (CPC+)– Next Generation ACO Model– Shared Savings Program - Track 2– Shared Savings Program - Track 3– Oncology Care Model (OCM) - Two-Sided Risk– Comprehensive Care for Joint Replacement (CJR) Payment Model (Track
1- CEHRT)– Vermont Medicare ACO Initiative (as part of the Vermont All-Payer ACO
• An individual clinician is defined as a single National Provider Identifier (NPI) tied to a single Tax Identification Number (TIN)
• A clinician group is defined as a set of 2+ clinicians, identified by their NPIs, who share a common TIN—regardless of the specialty or practice site
Individuals vs. Groups
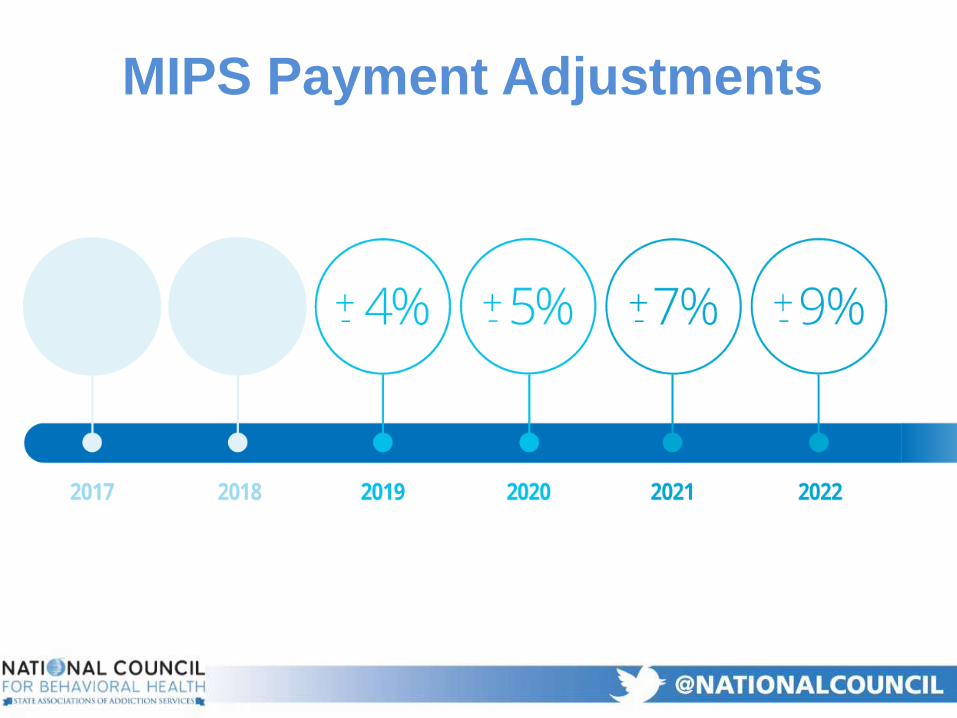
MIPS Payment Adjustments
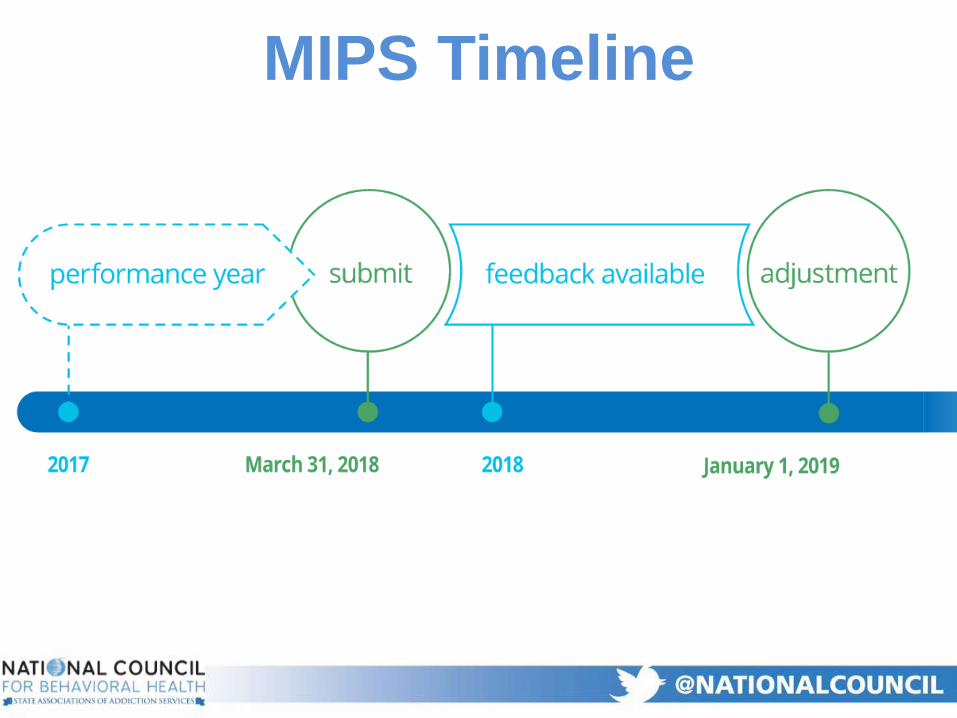
MIPS Timeline
“Pick Your Pace” Reporting Options
in 2017 to Avoid 2019 Penalties
MIPS Scoring
• CMS will factor in four weighted performance categories to calculate a final MIPS score
• Payment adjustments in 2019 may be negative, neutral or positive based on CMS-established threshold (3/100)
Quality Improvement
Activities
Advancing Care
Information Cost
Final Score
PQRS Value-based Modifier
Meaningful Use
• Requires providers to report six quality
measures for a minimum of 90 consecutive
days
• Emphasis on outcome/high priority measures:
– Appropriate use
– Care coordination
– Patient experience
– Patient safety
• Option to use behavioral/mental health
specialty measure set (25 measures)
Quality (60%)
• Quality measure data will be compared to CMS
benchmarks to determine your Quality score
• If there is no benchmark for a measure, clinicians /
groups will receive three points
• CMS will publish benchmarks prior to the start of each
performance year
Quality Benchmark Comparisons
• CMS plans to increase the number of required outcome
measures through future rulemaking, as more outcome
measures become available
• CMS will increase emphasis on measures related to:
– Appropriate use
– Patient experience
– Safety
– Care coordination
• CMS will update/add quality measures annually based
on clinician input
Future Quality Measures
• Requires MIPS eligible clinicians to use certified EHR
technology (CEHRT)
• Two measure sets in 2017 for reporting based on EHR
edition:
1. Advancing Care Information Objectives and
Measures
2. Advancing Care Information Transition Objectives
and Measures (2017)
Advancing Care Information (25%)
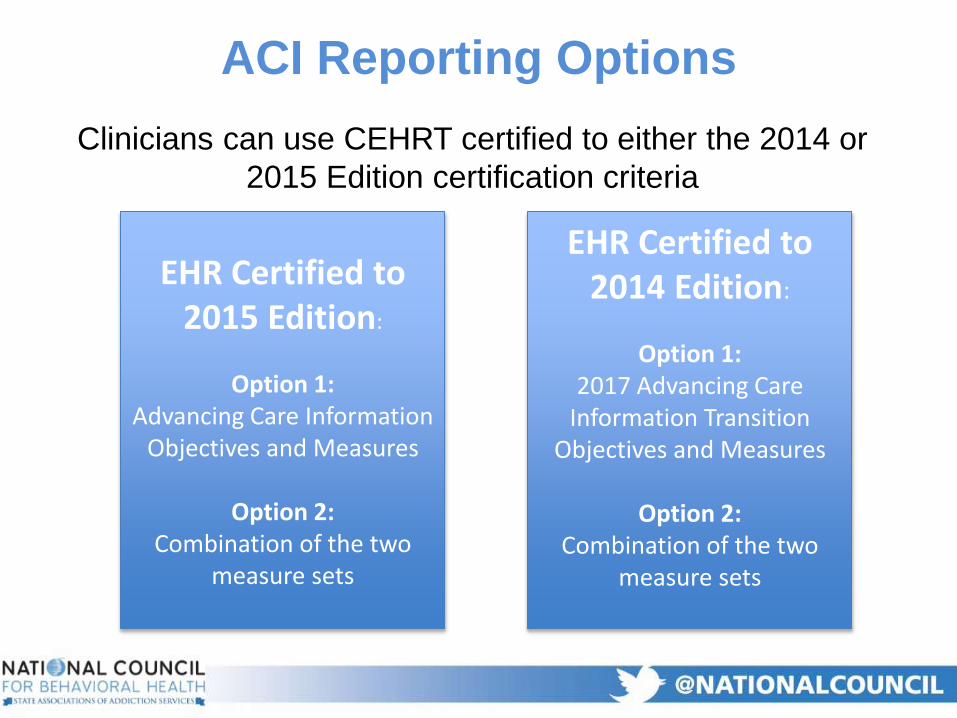
Clinicians can use CEHRT certified to either the 2014 or
2015 Edition certification criteria
ACI Reporting Options
EHR Certified to 2015 Edition:
Option 1: Advancing Care Information
Objectives and Measures
Option 2: Combination of the two
measure sets
EHR Certified to 2014 Edition:
Option 1: 2017 Advancing Care
Information Transition Objectives and Measures
Option 2: Combination of the two
measure sets
Clinicians must submit a numerator/ denominator
OR yes/no combination for each of the following
measures:
Protect patient health information
Electronic prescribing
Patient electronic access
Health Information Exchange: Send summary of care
Health Information Exchange: Request/accept
summary of care
Advancing Care Information:
Base Score
• Based on a MIPS eligible clinician’s
performance rate for each measure reported
• Nine measures
– Patient Electronic Access
– Coordination of Care through Patient Engagement
– Health Information Exchange
Advancing Care Information:
Performance Score
• Clinicians/clinician groups may be eligible for
a hardship exemption in the Advancing Care
Information performance category
• Category weight would be applied to Quality
category
• Participate anyway! 75% of your 2017 MIPS
score is based on Quality and Improvement
Activities!
What if I don’t have an EHR?
• Clinicians do NOT select cost measures
– CMS will apply measures to clinicians and determine
score based on Medicare Part B claims analysis
– No independent reporting required
• Cost analysis based on:
– Total per capita cost for all attributed beneficiaries
– Medicare spending per beneficiary (MSPB)
– Episode of care measures (not yet finalized; may be
implemented in 2019)
Cost (0%)
• Cost category weight will increase to 30
percent in the 2019 performance year / 2021
payment year
Cost Scoring
MIPS eligible clinicians can choose from a list of 90+
activities (updated annually) under nine sub-categories:
Improvement Activities (15%)
• Depression screening
• Diabetes screening
• EHR Enhancements for Behavioral Health Data Capture
• Implementation of co-location of primary care and mental health services
• Implementation of integrated Primary Care Behavioral Health model
• Major depressive disorder prevention and treatment interventions
• Tobacco use
• Unhealthy alcohol use
Improvement Activities: Behavioral
and Mental Health
Improvement Activity Scoring
• Activity weight for most
clinicians: Attest to completing up
to four activities for at least 90
days
• Activity weights for
small/rural/HPSA practices:
Attest to completing up to two
activities for at least 90 days
• Full credit for clinicians in a
patient-centered medical home,
Medical Home Model or similar
specialty practice
Individual Group
Defined as a single National Provider Identifier (NPI) tied to a single Tax Identification Number (TIN)
Defined as a set of 2+ clinicians, identified by their NPIs, who share a common TIN regardless of the specialty or practice site
Low volume threshold determined at individual level
Low volume threshold determined for entire group
Payment adjustment based on individual clinician’s performance
Groups are assessed as a group across all performance categories and receive one payment adjustment based on the group’s performance
Have the option to report via Medicare claims
Have the option to report via CMS Web Interface (groups 25+ only)
Individual vs. Group Reporting
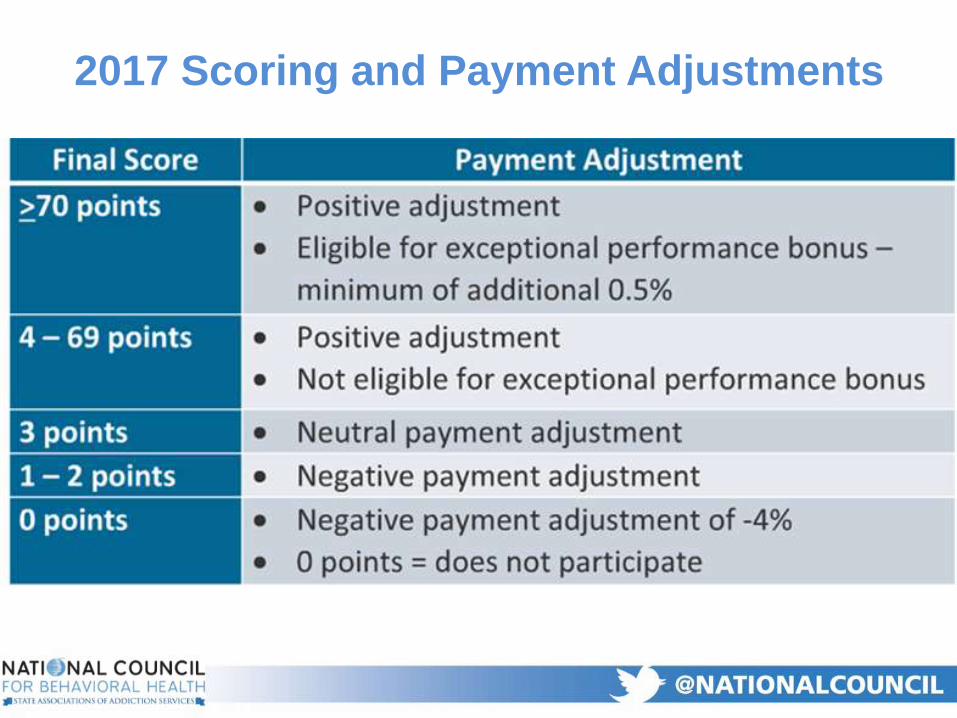
2017 Scoring and Payment Adjustments
Success in MIPS Depends
on Everyone.
• Do they know how they’re doing on applicable quality metrics?
• Do they know how they compare to their peers?
• Do they have regular access to data and means to implement plan-do-study-act cycles to continuously improve performance?
• Are they consistently following appropriate care pathways/protocols?
How Do Clinicians Demonstrate
Quality of Care?
• Do they understand their patients’ total cost of care?
• Do they understand how their costs compare to your competitors?
• Do they understand their role in increasing efficiency and reducing costs?– Using evidence-based practices to reduce the risk
of relapse, emergency room utilization and hospital readmission
– Coordinating care for complex medical co-morbidities
How Do Clinicians Reduce Costs?
How Do Clinicians Continuously
Improve Quality of Care?
• Achieving health equity
• Behavioral / mental health
• Beneficiary engagement
• Care coordination
• Emergency response & preparedness
• Expanded practice access
• Patient safety & Practice Assessment
• Population management
• Determine which Quality measures to report
• Determine which Improvement Activities to
focus on, and how to measure and document
participation
• Ensure appropriate IT systems are in place to
allow for near-real time data analysis and
reporting
• Ensure that there are appropriate care
pathways/protocols in place for staff to follow
The Administrator’s Role
• Do staff understand that transformation is everyone’s job?
• Do staff at all levels have job descriptions that reflect their role in practice transformation and quality improvement?
• Do staff have access to the data they need to identify areas for improvement and track progress over time?
• Do staff feel comfortable identifying challenges and pitching new ideas?
• Do staff feel valued and respected?
The Administrator’s Role
How to Prepare
QPP.CMS.GOV
Determine Quality Payment Program eligibility (see qpp.cms.gov clinician NPI look up tool)
“Pick Your Pace” for 2017
Review applicable quality measures and improvement activities
Make sure your EHR is certified by the Office of the National Coordinator for Health Information Technology; review applicable measures
If you do NOT have access to CEHRT, check to see if you’re eligible for a hardship exemption
Patient & family engagement Team-based relationships Population management Practice as a community partnerCoordinated care delivery Organized, evidence-based careEnhanced access
Continuous, Data-Driven Quality Improvement
Engaged and committed leadership QI strategy supporting a culture of quality and safety Transparent measurement and monitoringOptimal use of HIT
Sustainable Business Operations
Strategic use of practice revenue Staff vitality and joy in work Capability to analyze and document value Efficiency of operation
• Free, customized technical assistance is available
for small practices with 15 or fewer clinicians
• Priority is given to those small practices:
– Located in a rural area
– Located in designated health professional shortage
areas (HPSAs)
– Located in designated medically underserved areas