58
The Human Brain: The Human Brain: Anatomy, Anatomy, Functions, Functions,
| Date post: | 20-Oct-2015 |
| Category: |
Documents |
| Upload: | badr-diham |
| View: | 18 times |
| Download: | 0 times |

The Human Brain:The Human Brain:Anatomy,Anatomy,Functions,Functions,

Main MenuMain Menu
• Brain Anatomy• Brain Functions

Brain Anatomy MenuBrain Anatomy MenuSkull AnatomyInterior Skull SurfaceBlood Vessels of the BrainArteries of the BrainThe NeuronThe MeningesExternal Brain StructuresThe CerebrumThe Cerebrum – The CortexThe NeocortexLobes of the Cerebrum
Frontal LobeTemporal LobeParietal LobeOccipital LobeLimbic Lobe
The Limbic SystemCerebellumThalamusHypothalamusThe Medulla OblongataThe PonsThe VentriclesCerebrospinal FluidThe BrainstemBrainstem ComponentsBrainstem DivisionsThe Cranial Nerves

Skull AnatomySkull Anatomy
The skull is a rounded layer of bone designed to protect the brain from penetrating injuries.
Blood Vessels of the Skull
Rough Interior of Skull

Interior Skull SurfaceInterior Skull SurfaceThe base of the skull is rough, with many bony protuberances.
These ridges can result in injury to the temporal lobe of the brain during rapid acceleration.
Bony ridges
Injury from contact with skull
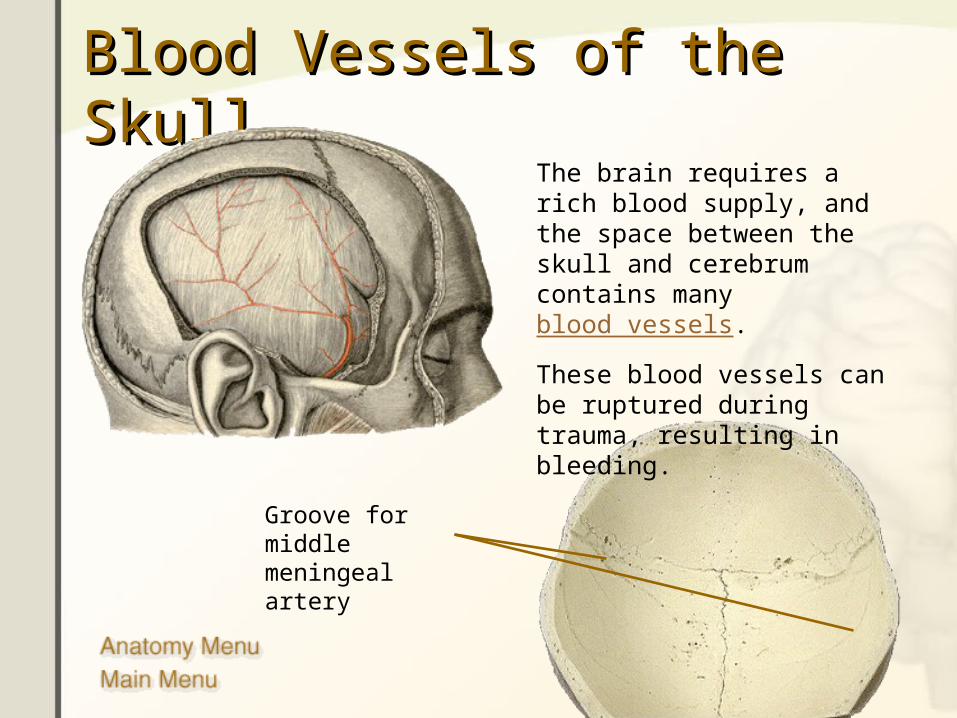
Blood Vessels of the SkullBlood Vessels of the SkullThe brain requires a rich blood supply, and the space between the skull and cerebrum contains many blood vessels.
These blood vessels can be ruptured during trauma, resulting in bleeding.
Groove for middle meningeal artery

Arteries of the BrainArteries of the Brain
The human brain requires a constant supply of oxygen. A lack of oxygen of just a few minutes results in irreversible damage to the brain.
The NeuronThe Neuron
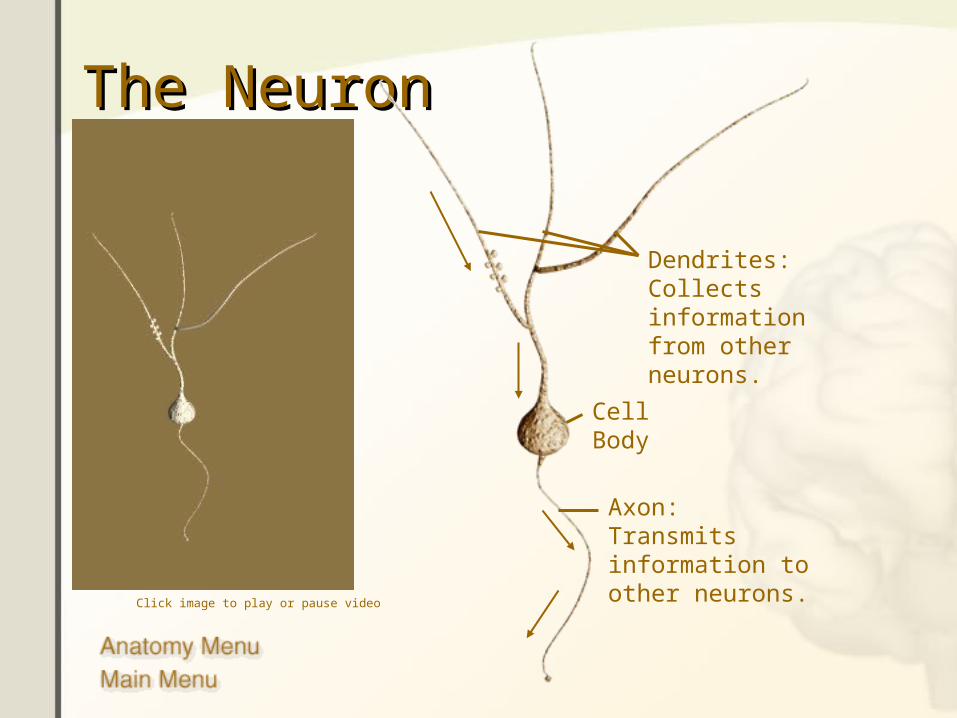
Dendrites:Collects information from other neurons.
Cell Body
Axon:Transmits information to other neurons.
Click image to play or pause video

The MeningesThe MeningesThe meninges are layers of tissue that separate the skull and the brain.
Skull
Dura mater
Arachnoid Layer
Pia Mater
Brain

External Brain StructuresExternal Brain Structures

The CerebrumThe Cerebrum
The largest portion of the brain is the cerebrum. It consists of two hemispheres that are connected together at the corpus callosum.
The cerebrum is often divided into five lobes that are responsible for different brain functions.
Corpus callosum
The CerebrumThe Cerebrum
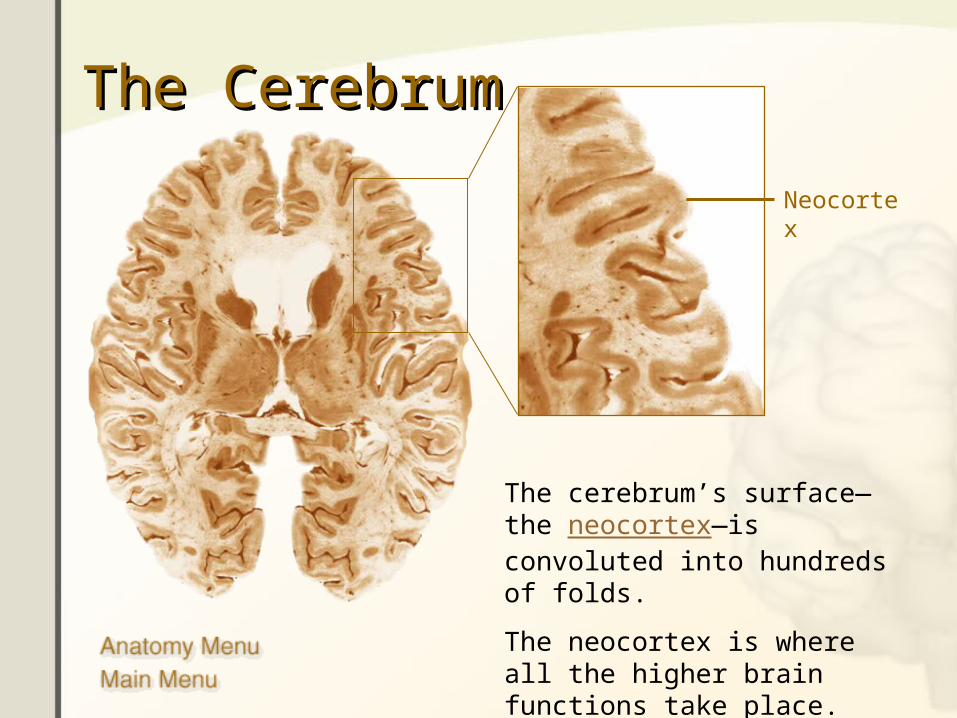
The cerebrum’s surface—the neocortex—is convoluted into hundreds of folds.
The neocortex is where all the higher brain functions take place.
Neocortex
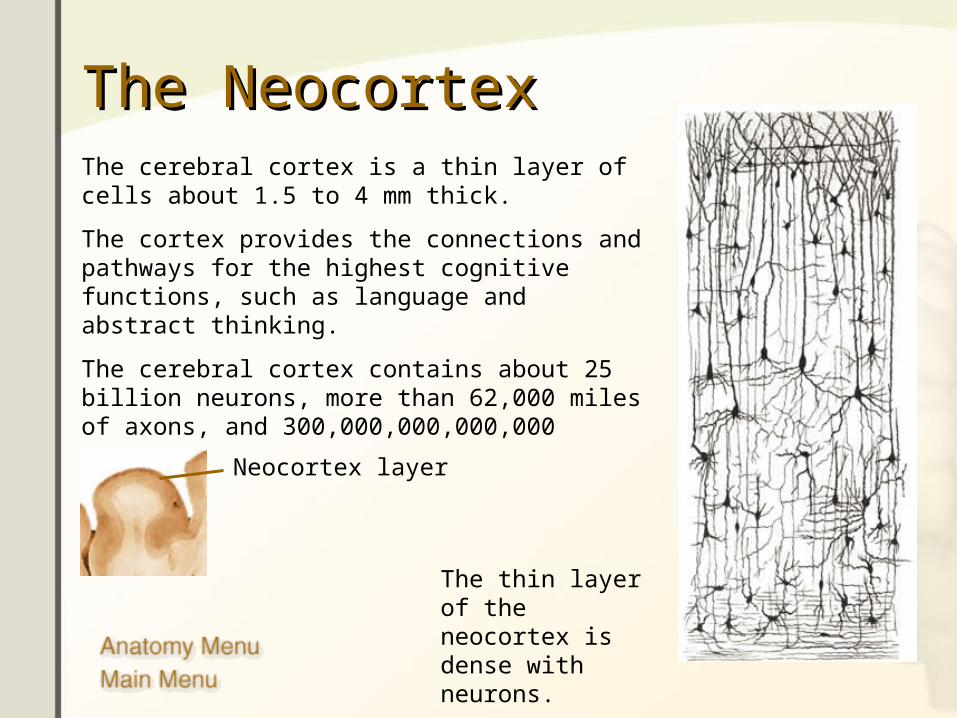
The NeocortexThe NeocortexThe cerebral cortex is a thin layer of cells about 1.5 to 4 mm thick.
The cortex provides the connections and pathways for the highest cognitive functions, such as language and abstract thinking.
The cerebral cortex contains about 25 billion neurons, more than 62,000 miles of axons, and 300,000,000,000,000 synapses.
Neocortex layer
The thin layer of the neocortex is dense with neurons.

Lobes of the CerebrumLobes of the Cerebrum
Parietal Lobe
Temporal Lobe
Frontal Lobe
Limbic Lobe
Occipital Lobe

Frontal LobeFrontal LobeThe frontal lobe is the area of the brain responsible for higher cognitive functions.
These include:
• Problem solving• Spontaneity• Memory• Language• Motivation• Judgment• Impulse control• Social and sexual behavior.

Temporal LobeTemporal LobeThe temporal lobe plays a role in emotions, and is also responsible for smelling, tasting, perception, memory, understanding music, aggressiveness, and sexual behavior.
The temporal lobe also contains the language area of the brain.

Parietal LobeParietal LobeThe parietal lobe plays a role in our sensations of touch, smell, and taste. It also processes sensory and spatial awareness, and is a key component in eye-hand co-ordination and arm movement.
The parietal lobe also contains a specialized area called Wernicke’s area that is responsible for matching written words with the sound of spoken speech.
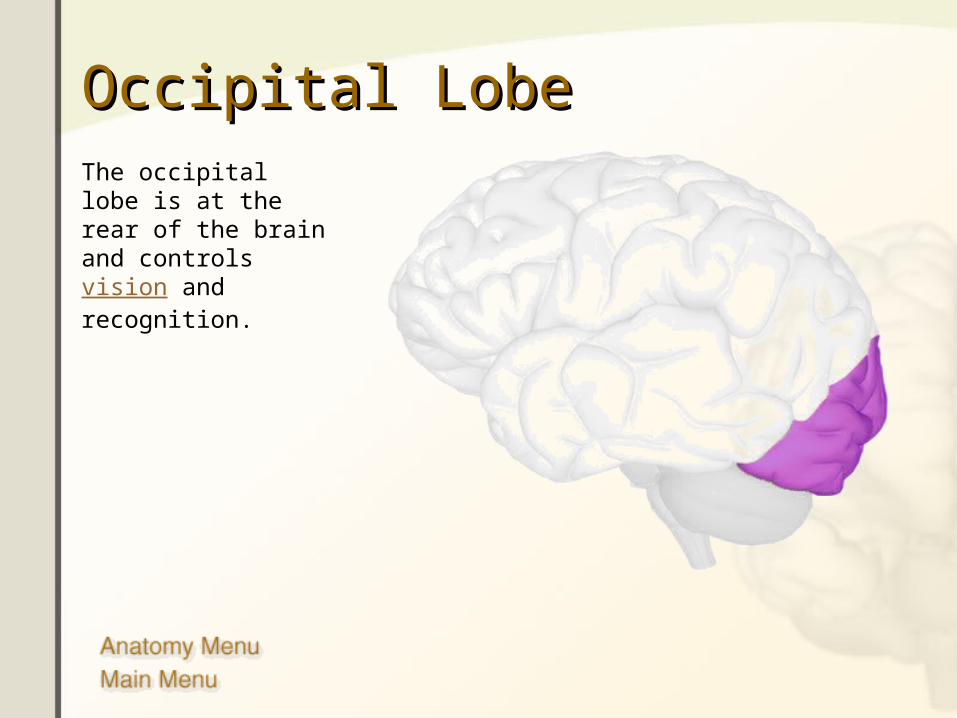
Occipital LobeOccipital LobeThe occipital lobe is at the rear of the brain and controls vision and recognition.

Limbic LobeLimbic LobeThe limbic lobe is located deep in the brain, and makes up the limbic system.

The Limbic SystemThe Limbic System
A. Cingulate gyrusB. FornixC. Anterior thalamic
nucleiD. HypothalamusE. Amygdaloid nucleusF. Hippocampus
The limbic system is the area of the brain that regulates emotion and memory. It directly connects the lower and higher brain functions.

CerebellumCerebellumThe cerebellum is connected to the brainstem, and is the center for body movement and balance.
Click image to play or pause video

ThalamusThalamusThalamus means “inner room” in Greek, as it sits deep in the brain at the top of the brainstem.
The thalamus is called the gateway to the cerebral cortex, as nearly all sensory inputs pass through it to the higher levels of the brain.

HypothalamusHypothalamus
The hypothalamus sits under the thalamus at the top of the brainstem. Although the hypothalamus is small, it controls many critical bodily functions:
• Controls autonomic nervous system
• Center for emotional response and behavior
• Regulates body temperature
• Regulates food intake
• Regulates water balance and thirst
• Controls sleep-wake cycles
• Controls endocrine system
The hypothalamus is shaded blue. The pituitary gland extends from the hypothalamus.

The Medulla OblongataThe Medulla Oblongata
The medulla oblongata merges seamlessly with the spinal cord and creates the base of the brainstem.
The medulla is primarily a control center for vital involuntary reflexes such as swallowing, vomiting, sneezing, coughing, and regulation of cardiovascular and respiratory activity.
The medulla is also the origin of many cranial nerves.

The PonsThe Pons
The pons is the rounded brainstem region between the midbrain and the medulla oblongata. In fact, pons means “bridge” in Latin.
The main function of the pons is to connect the cerebellum to the rest of the brain and to modify the respiratory output of the medulla.
The pons is the origin of several cranial nerves.
The VentriclesThe Ventricles
Click image to play or pause video
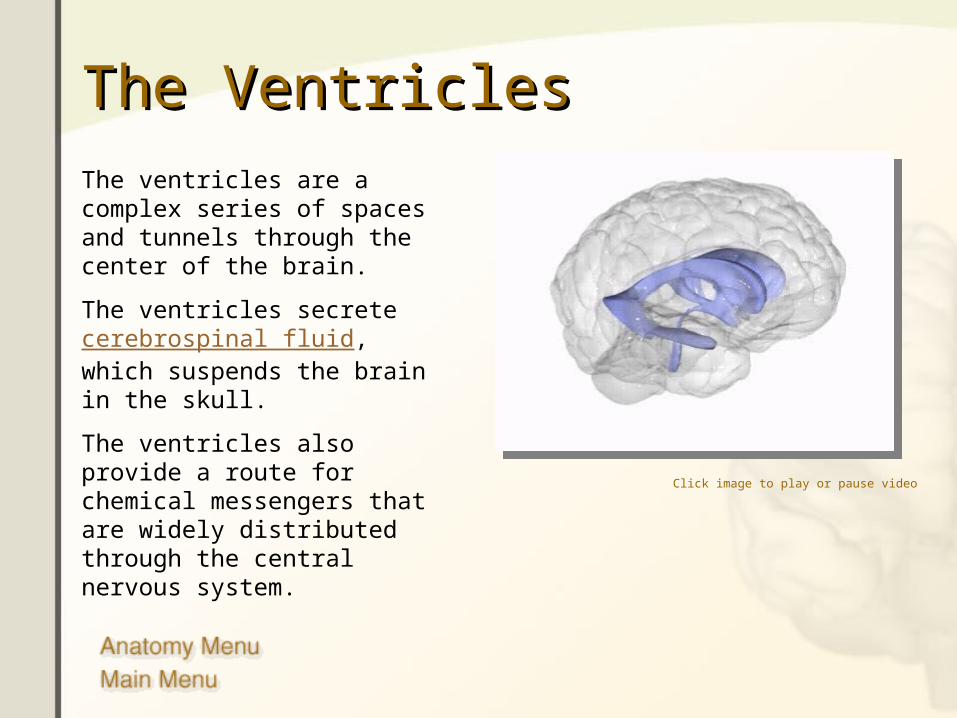
The ventricles are a complex series of spaces and tunnels through the center of the brain.
The ventricles secrete cerebrospinal fluid, which suspends the brain in the skull.
The ventricles also provide a route for chemical messengers that are widely distributed through the central nervous system.

Cerebrospinal FluidCerebrospinal Fluid
Cerebrospinal fluid is a colorless liquid that bathes the brain and spine.
It is formed within the ventricles of the brain, and it circulates throughout the central nervous system.
Cerebrospinal fluid fills the ventricles and meninges, allowing the brain to “float” within the skull.
Click image to play or pause video

The BrainstemThe BrainstemThe brainstem is the most primitive part of the brain and controls the basic functions of life: breathing, heart rate, swallowing, reflexes to sight or sound, sweating, blood pressure, sleep, and balance.
The brainstem can be divided into three major sections.
Detailed brainstem anatomy.
Click image to play or pause video

Brainstem Components Brainstem Components
Front
RearMore Information:MedullaThalamusPons

Brainstem DivisionsBrainstem Divisions
Midbrain
Pons
Medulla Oblongata
The Cranial NervesThe Cranial Nerves
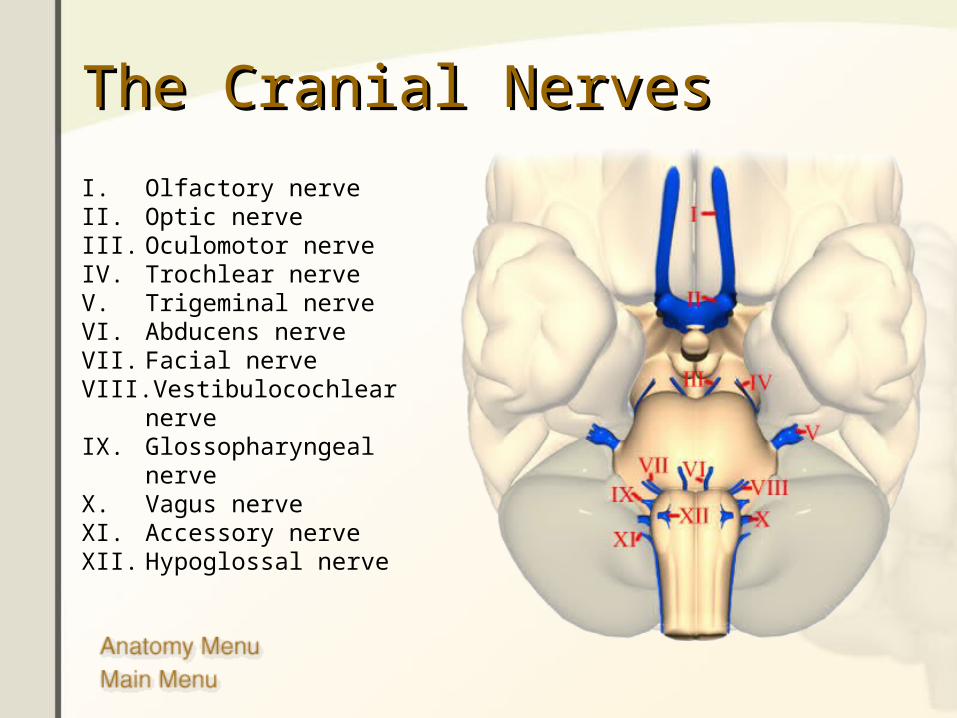
I. Olfactory nerveII. Optic nerveIII. Oculomotor nerveIV. Trochlear nerveV. Trigeminal nerveVI. Abducens nerveVII. Facial nerveVIII. Vestibulocochlear nerveIX. Glossopharyngeal nerveX. Vagus nerveXI. Accessory nerveXII. Hypoglossal nerve
TasteTaste
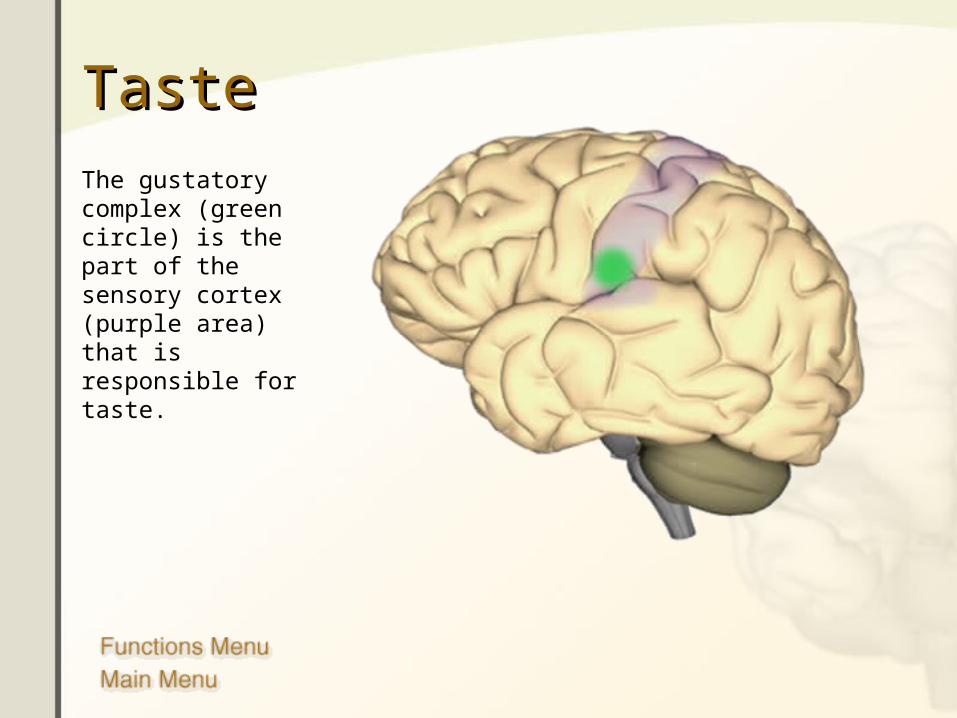
The gustatory complex (green circle) is the part of the sensory cortex (purple area) that is responsible for taste.

CognitionCognition
The prefrontal cortex is involved with intellect, complex learning, and personality.
Injuries to the front lobe can cause mental and personality changes.
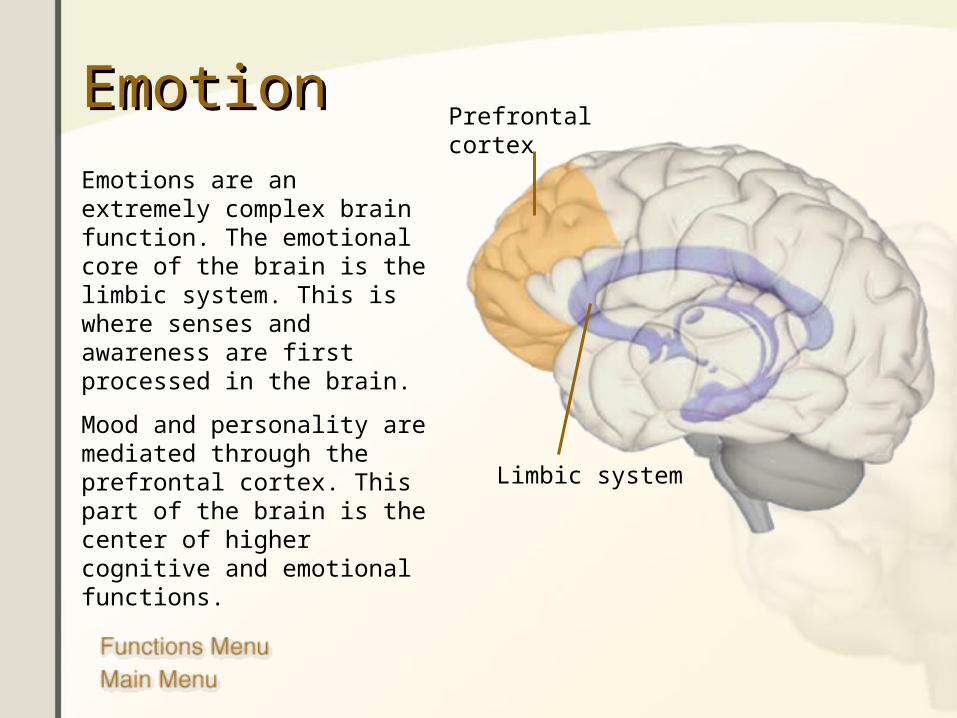
EmotionEmotion
Emotions are an extremely complex brain function. The emotional core of the brain is the limbic system. This is where senses and awareness are first processed in the brain.
Mood and personality are mediated through the prefrontal cortex. This part of the brain is the center of higher cognitive and emotional functions.
Prefrontal cortex
Limbic system
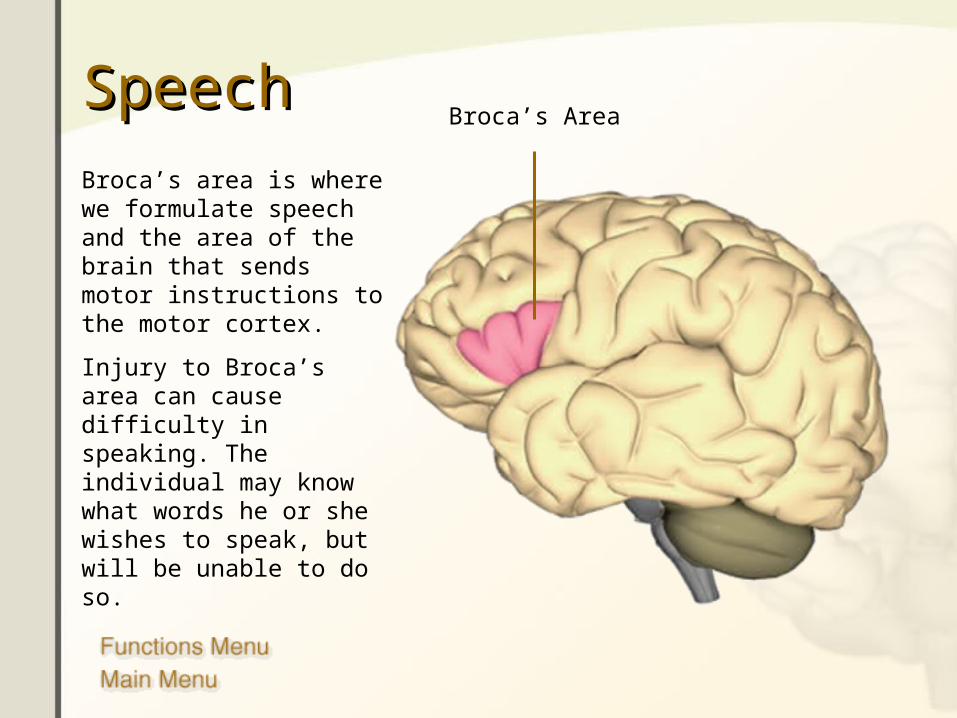
SpeechSpeech
Broca’s area is where we formulate speech and the area of the brain that sends motor instructions to the motor cortex.
Injury to Broca’s area can cause difficulty in speaking. The individual may know what words he or she wishes to speak, but will be unable to do so.
Broca’s Area
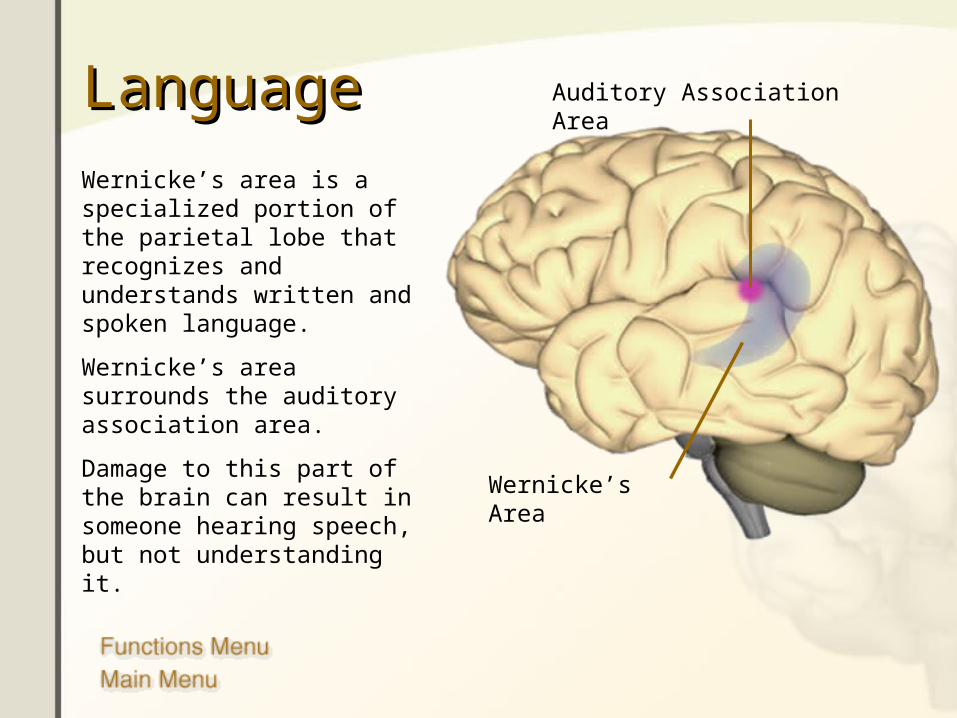
LanguageLanguage
Wernicke’s area is a specialized portion of the parietal lobe that recognizes and understands written and spoken language.
Wernicke’s area surrounds the auditory association area.
Damage to this part of the brain can result in someone hearing speech, but not understanding it. Wernicke’s Area
Auditory Association Area

HearingHearingThere are two auditory areas of the brain:
• The primary auditory area (brown circle) is what detects sounds that are transmitted from the ear. It is located in the sensory cortex.
• The auditory association area (purple circle) is the part of the brain that is used to recognize the sounds as speech, music, or noise.
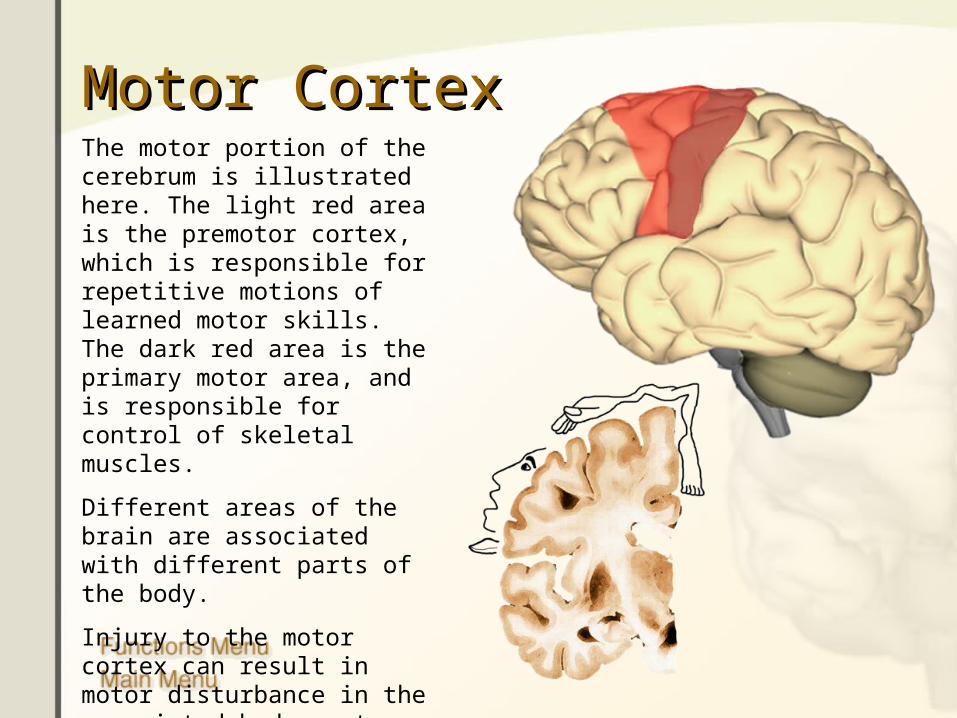
Motor CortexMotor CortexThe motor portion of the cerebrum is illustrated here. The light red area is the premotor cortex, which is responsible for repetitive motions of learned motor skills. The dark red area is the primary motor area, and is responsible for control of skeletal muscles.
Different areas of the brain are associated with different parts of the body.
Injury to the motor cortex can result in motor disturbance in the associated body part.

Sensory CortexSensory CortexThe sensory portion of the cerebrum is illustrated here.
Different areas of the brain are associated with different parts of the body, as can be seen below.
Injury to the sensory cortex can result in sensory disturbance in the associated body part.

Autonomic FunctionsAutonomic FunctionsThe brainstem controls the basic functions of life. Damage to these areas of the brain are usually fatal:
•The pons plays a critical role in respiration.
•The medulla oblongata is responsible for respiration and cardiovascular functions. Pons
Medulla Oblongata
INVESTIGATION OF INVESTIGATION OF NEUROLOGICAL DISEASE NEUROLOGICAL DISEASE TESTS OF FUNCTION (CLINICAL NEUROPHYSIOLOGY) In the investigation of neurological disease, tests of function have a somewhat more restricted application than tests of structure (i.e. imaging). Nevertheless, recording of electrical activity over the brain and assessment of nerve and muscle function are essential in certain conditions. The major tests are electroencephalography (EEG), evoked potentials (EPs) and nerve conduction studies/electromyography (NCS/EMG).
Electroencephalography Electrical activity arising in the cerebral cortex can be detected using electrodes placed on the scalp, although this is estimated to detect only 0.1-1% of the brain's electrical activity at any one time. An array of electrodes provides spatial information. Rhythmical waveforms can be detected and are distinguished by their frequency. When the eyes are shut, the most obvious frequency over the occipital cortex is 8-13/s; this is known as alpha rhythm, and disappears when the eyes are opened. Other frequency bands seen over different parts of the brain in different circumstances are beta (faster than 13/s), theta (4-8/s) and delta (slower than 4/s). Lower frequencies predominate in the very young and during sleep. Various diseases result in abnormalities of the EEG. These may be continuous or episodic, focal or diffuse. Examples of continuous abnormalities include a global increase in fast frequencies (beta) seen with sedating drugs (e.g. benzodiazepines), or marked slowing seen over a structural lesion such as a tumour or an infarct. With the advent of modern neuro-imaging, EEG has lost its use in localising lesions, except in the management of epilepsy (see below and \). However, it is still useful in the management of patients who have disturbance of consciousness or disorders of sleep, in the diagnosis of cerebral diseases such as encephalitis, and in certain dementias (e.g. sporadic Creutzfeldt-Jakob disease).


Evoked potentials If a stimulus is provided-for example, to the eye-it would normally be impossible to detect the small EEG response evoked over the occipital cortex as the signal would be lost in background noise. However, if the EEG data from 100-1000 repeated stimuli are averaged electronically, this noise is removed and an evoked potential recorded whose latency (the time interval between stimulus onset and the maximum positive value of the evoked potential, P100) and amplitude can be measured. Evoked potentials can be measured following visual, auditory or somatosensory stimuli if electrodes are appropriately positioned, although visual evoked potentials are by far the most commonly used). Abnormalities of the evoked potential indicate damage to the relevant pathway, either in the form of a conduction delay (increased latency) or reduced amplitude, or both. With the advent of magnetic resonance imaging (MRI), the use of evoked potentials is becoming restricted to specialised indications, such as providing a semi-objective measure of visual function.
Nerve conduction studies and Nerve conduction studies and electromyography electromyography The principal use of nerve conduction studies is to identify damage to peripheral nerves, and to determine whether the pathological process is focal or diffuse, and whether the damage is principally axonal or demyelinating. It is also possible to obtain some information about nerve roots by more sophisticated analysis of responses to impulses initially conducted antidromically (i.e. the 'wrong' way) back up to the spinal cord, and then returning orthodromically (the 'right'
way) down to the stimulation point ('F waves') .Fine concentric needle electrodes can be inserted into muscle bellies themselves and the potentials from individual motor units recorded. It is possible to record abnormal spontaneous activity arising from muscles at rest, such as fibrillations (a sign of denervation) or myotonic discharges. Abnormalities in the shape and size of muscle potentials can help in the differential diagnosis of denervation and structural muscle diseases. Myopathies caused by metabolic abnormalities (causing electromechanical dissociation rather than loss of fibre structure) show no changes on
needle EMG .Electromyography can also be used to investigate the neuromuscular junction. Repetitive stimulation of a nerve with trains of electrical impulses at 3-15/s does not normally result in a significant fall-off in the amplitude of the resulting muscle action potential. However, such a decrement is seen in myasthenia gravis (p. 1252) and provides one of the key diagnostic features. Augmentation of the response to repetitive stimulation is seen in the Lambert-Eaton myasthenic
syndrome, though usually at higher stimulation frequencies .


Electromyography can also be used to investigate the neuromuscular junction. Repetitive stimulation of a nerve with trains of electrical impulses at 3-15/s does not normally result in a significant fall-off in the amplitude of the resulting muscle action potential. However, such a decrement is seen in myasthenia gravis) and provides one of the key diagnostic features. Augmentation of the response to repetitive stimulation is seen in the Lambert-Eaton myasthenic syndrome, though usually at higher stimulation frequencies. IMAGINGImaging is crucial to the identification of lesions of the nervous system in disease. There are various techniques, based on the use of X-rays (plain X-rays, computed tomography (CT), myelography and angiography), magnetic resonance (MR imaging-MRI, or MR angiography-MRA), ultrasound (Doppler imaging of blood vessels), and radioisotopes (single photon emission computed tomography-SPECT, and positron emission tomography-PET). The indications, usefulness and limits of each technique are listed in The choice of technique depends upon the area of the neuraxis that is being investigated
Head and orbit The use of plain skull X-rays is largely restricted to the diagnosis of fractures and sinus disease. CT or MRI is needed to image pathology inside the skull. Which is used depends on what information is being sought and, to some extent, how urgently it is required, as CT is often more easily available than MRI. CT will show bone and calcium well, and will easily image collections of blood. It will also detect abnormalities of the brain and ventricles, such as atrophy, tumours, cysts, abscesses, vascular lesions and hydrocephalus. Diagnostic yield is often improved by the use of intravenous contrast and spiral CT methods. It is, however, limited in its ability to image the posterior fossa (because of the surrounding bone density), and it is poor at detecting
abnormalities of white matter and at allowing detailed analysis of grey matter .MRI is much more useful in the investigation of posterior fossa disease as it is not affected by the surrounding bone. It is much more sensitive than CT to abnormalities of white and grey matter and is therefore useful in the investigation of inflammatory conditions such as multiple sclerosis, and in investigating epilepsy. MRI can also provide additional information about structural brain lesions, which may complement that available from CT. It is also useful in imaging the orbits, where special imaging sequences can be used to compensate for orbital fat and thereby allow clear views of extraocular
muscles, optic nerve and other orbital structures .Standard isotope brain scans are of little value in assessing structure if other imaging facilities are available. However, the blood flow and function of the
cerebral hemispheres can be assessed by using either SPECT or PET .
Neck Plain X-rays of the neck are useful in the investigation of structural damage to vertebrae, such as that resulting from trauma or inflammatory damage (e.g. rheumatoid arthritis). They can also provide implicit information about intervertebral disc disease, but not detailed information about the cervical cord or nerve roots, for
which myelography or MRI is needed .Myelography is invasive. Potential complications include headache, seizures and meningitis. With the advent of MRI its use is declining. Nevertheless, it is still of value if MRI is not available or the patient cannot tolerate lying within an MRI scanner. Radio-opaque contrast is injected into the lumbar theca and then moved up to the cervical region by tilting the patient. The contrast outlines the nerve roots and spinal cord, thereby providing information about abnormal structure. Examples of the neck imaged by plain X-rays, myelography and MRI are
shown in .

Lumbo-sacral region Imaging of this region is similar to imaging the neck, and plain X-rays are of limited use. Contrast can be injected into the lumbar thecal space and used to outline the lower nerve roots only (radiculography), or it can be run up to outline the conus and spinal cord (myelography). The information obtained may be enhanced by the additional use of CT following myelography (contrast CT). Non-contrast CT of the lumbar spine can only be used to image the vertebrae and discs. As with the cervical spine, MRI provides a non-invasive way of obtaining high-resolution images of both
the vertebral column and the relevant neural structures .Blood vessels
Various techniques are available to investigate extracranial and intracranial blood vessels. The least invasive is ultrasound (Doppler or duplex scanning), which is used to investigate the carotid and the vertebral arteries in the neck, usually as part of the investigation of stroke. In skilled hands, reliable information can be provided about the degree of arterial stenosis, and the technique often gives useful anatomical information, e.g. whether there is an ulcerated plaque. Information concerning the blood flow in the intracerebral vessels is also becoming increasingly possible to obtain using transcranial Doppler. While the anatomical resolution of Doppler imaging is limited, this is improving with increased experience and many centres no longer require formal angiography before performing carotid endarterectomy. This has the advantage of eliminating the small but significant risk of stroke or even death
associated with catheter angiography .
SPECIAL TESTS Blood tests
Many systemic conditions affect the nervous system and these can often be diagnosed with the help of blood tests: for example, confusion due to hypothyroidism, a stroke due to systemic lupus erythematosus, ataxia due to vitamin B12 deficiency, or myelopathy due to syphilis. The blood tests relating to general medical conditions which affect the nervous system are dealt with in the sections
dealing with the conditions themselves .There are, however, a number of blood tests which are used in investigating specific neurological diseases. These include haematological tests (e.g. looking for acanthocytes to diagnose neuroacanthocytosis), biochemical tests (e.g. creatine kinase in muscle diseases, copper studies to diagnose Wilson's disease) or tests to help diagnose innumerable infections of the nervous system. In addition, there are a number of specific antibodies that are useful diagnostically. These include antibodies to acetylcholine receptors and muscle-specific tyrosine kinase (MuSK), seen in myasthenia gravis, and to voltage-gated calcium channels in Lambert-Eaton myasthenic syndrome. Antibodies to different types of ganglioside (glycoproteins expressed on nerve membranes) can be seen in various types of neuropathy including multifocal motor neuronopathy, and the Guillain-Barré syndrome (particularly the Miller-Fisher variant). Also, antineuronal antibodies provide markers of paraneoplastic cerebellar or neuropathic syndromes. Antibodies to basal
ganglia neurons are found in Sydenham's chorea and encephalitis lethargica .An increasing number of inherited neurological conditions can now be diagnosed by DNA analysis (p. 50). These include diseases caused by increased numbers of trinucleotide repeats, such as Huntington's disease, myotonic dystrophy and some types of spinocerebellar ataxia. Also, defects of mitochondrial DNA can be detected in many conditions including Leber's hereditary optic neuropathy, and some syndromes causing epilepsy or stroke-like syndromes
Lumbar puncture Lumbar puncture
Lumbar puncture is indicated in the investigation of infections (e.g. meningitis or encephalitis), subarachnoid haemorrhage, inflammatory conditions (e.g. multiple sclerosis, sarcoidosis and cerebral lupus) and some neurological malignancies (e.g. carcinomatous meningitis, lymphoma and leukaemia), and to measure CSF pressure (e.g. in idiopathic intracranial hypertension). It is, of course, part of the procedure of myelography, and can be used in therapeutic procedures, either to lower CSF pressure or to administer drugs

If there is a space-occupying lesion in the head, lumbar puncture can result in a shift of intracerebral contents downwards, towards and into the spinal canal. This process is known as coning, and is potentially fatal . Consequently, lumbar puncture is contraindicated if there is any suggestion of raised intracranial pressure (e.g. papilloedema), depressed level of consciousness, or focal neurological signs suggesting a cerebral lesion, until imaging of the head (by CT or MRI) has excluded a space-occupying lesion or hydrocephalus. It is also contraindicated if the patient is likely to bleed, as in thrombocytopenia, disseminated intravascular coagulation or warfarin therapy, unless specific measures are taken to compensate for the clotting deficit on a temporary basis. Lumbar puncture is not contraindicated in those on aspirin
About 30% of lumbar punctures are followed by low-pressure headache, which can be severe. Other minor complications involve transient radiular pain during the procedure, and pain over the lumbar region. Provided the test is performed under sterile conditions, infections such as meningitis are extremely rar



Biopsies Nerve and muscle are occasionally biopsied to assist in the diagnosis and management of a number of neurological conditions. Likewise, it is occasionally
necessary to biopsy brain or meninges .Nerve is sometimes biopsied as part of the investigation of peripheral neuropathies. Usually, the sural nerve is sampled at the ankle or the radial nerve at the wrist. Histology can help identify underlying causes in demyelinating neuropathies (e.g. vasculitic) or, occasionally, infiltration with abnormal substances such as amyloid. However, nerve biopsy is not performed unless it is reasonably likely to diagnose a potentially treatable condition such as an inflammatory neuropathy,
since there is an appreciable morbidity .

Skeletal muscle biopsy is performed more frequently. The quadriceps muscle is often sampled, although this depends somewhat on which muscles are affected. Indications include the investigation of primary muscle disease, as muscle histology can be used to distinguish neurogenic wasting, myositis and myopathy, which may be difficult to distinguish clinically. Histology and enzyme histochemistry can also be helpful in the diagnosis of more widespread metabolic disorders, such as mitochondrial and some storage diseases. Although pain and infection can follow the procedure, these are much less of a
problem than after nerve biopsy .The nature of lesions demonstrated by brain imaging can often be inferred from the appearances as well as the history, examination and other, less invasive, investigations. However, there are situations in which the nature of lesions is not clear, and it is important to obtain tissue for histological examination. Likewise, it is sometimes necessary to biopsy the brain parenchyma itself in unexplained degenerative diseases (e.g. unusual dementias) so as
not to miss potentially treatable disease .Brain biopsy used to require full craniotomy. However, owing to the increased availability and sophistication of cerebral imaging, it is now possible to biopsy most lesions stereotactically through a burrhole in the skull. The complication rate of such stereotactic biopsies is much lower than that of open craniotomy, but haemorrhage, infection and death still occur. Hence, brain biopsy is only considered if a diagnosis cannot be reached in any other way

















