West Virginia’s Coaches Asthma Clipboard You can make a positive difference in the health of a child with asthma Cynthia Keely, BA, RRT, LRTR Manager WV Asthma Education and Prevention Program www.wvasthma.org
Transcript
West Virginia’s Coaches Asthma Clipboard
You can make a positive difference in the health of a child with asthma
Cynthia Keely, BA, RRT, LRTR Manager
WV Asthma Education and Prevention Program www.wvasthma.org
• Funded by the Centers for Disease Control and Prevention through a cooperative grant agreement with the WV Department of Health and Human Resources.
• One of 36 states, tribes, and territories funded for asthma activities. Provides funds for the operation of a statewide asthma coalition (WVAC), asthma education initiatives and interventions, and data surveillance.
Website:
www.wvasthma.org
Learning Objectives
• The scope of asthma
• Common asthma symptoms
• Potential asthma triggers
• The difference between quick-relief and controller medications for asthma
• How to manage an asthma episode
• How to respond to an asthma emergency
• The importance and components of an Asthma Action Plan
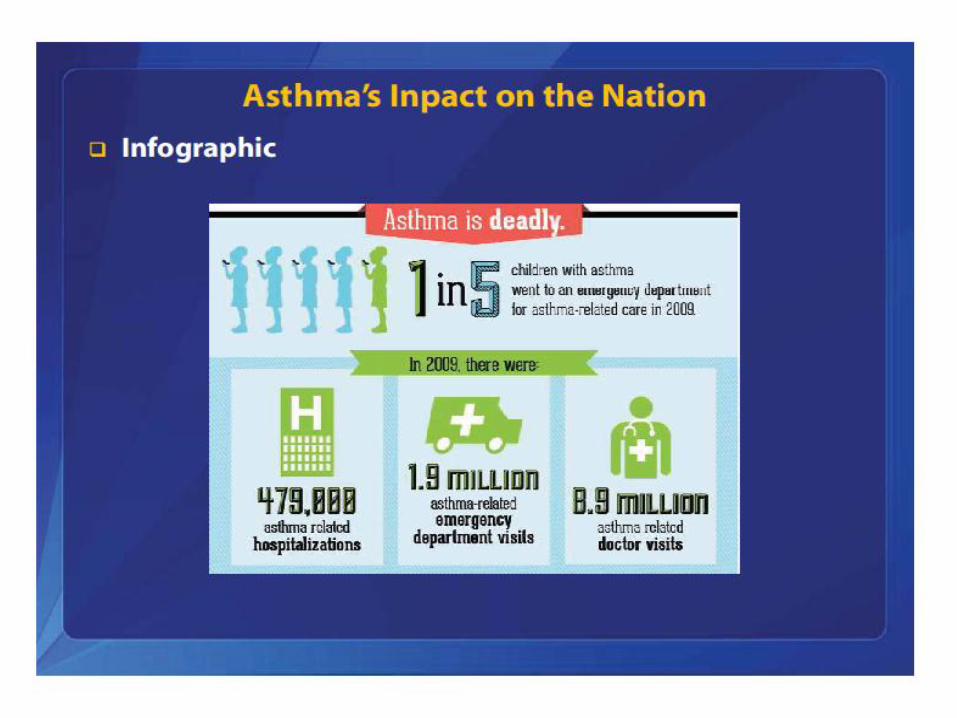
How Many People Have Asthma?
25 Million people in the U.S. have asthma • 18.7 Million adults have asthma.
– That’s equal to 1 in 12 adults.
• 7 Million children have asthma. – That’s equal to 1 in 11 children.
• Approximately 5,000 people die each year from asthma in the U.S.
In 2008, • an estimated 44,000 children in WV had asthma
• 14.7% of children had lifetime asthma
• 11.5% of children had current asthma
• Boys (<18years) are more like to have asthma than girls
On average 27 West Virginians die from asthma each year.
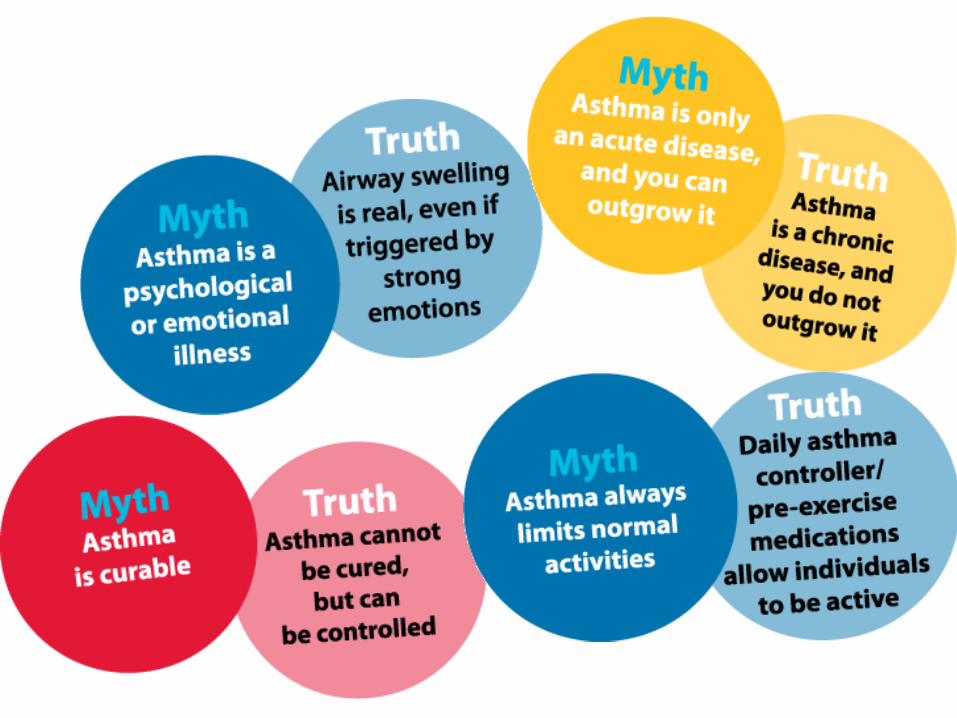
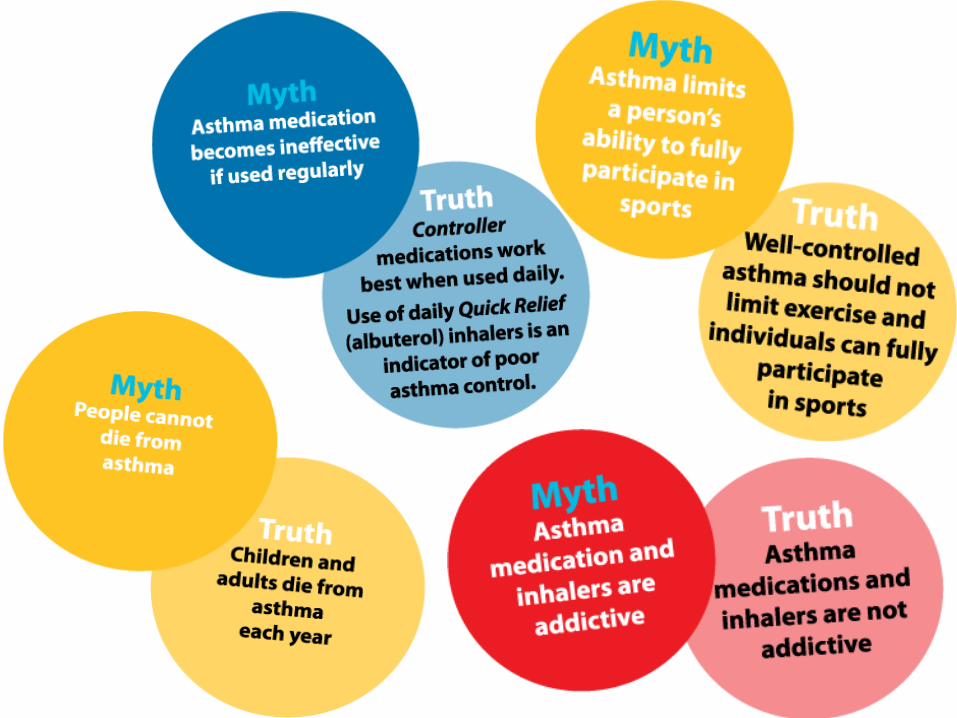
The Good News
Asthma can be controlled!
Children with asthma are just like any other child!
Children with asthma can play sports and compete just like everyone else!
The Goal of Asthma Management
• “Children should live happy, healthy, physically active lives, without asthma symptoms slowing them down”
What is Asthma?
A chronic disease that causes obstruction:
Tightening of the muscles surrounding the airways.
Swelling of the lining of small airways in the lungs.
Airways that are overly sensitive to allergen and irritant triggers.
Over production of sticky mucus clogging the airways.
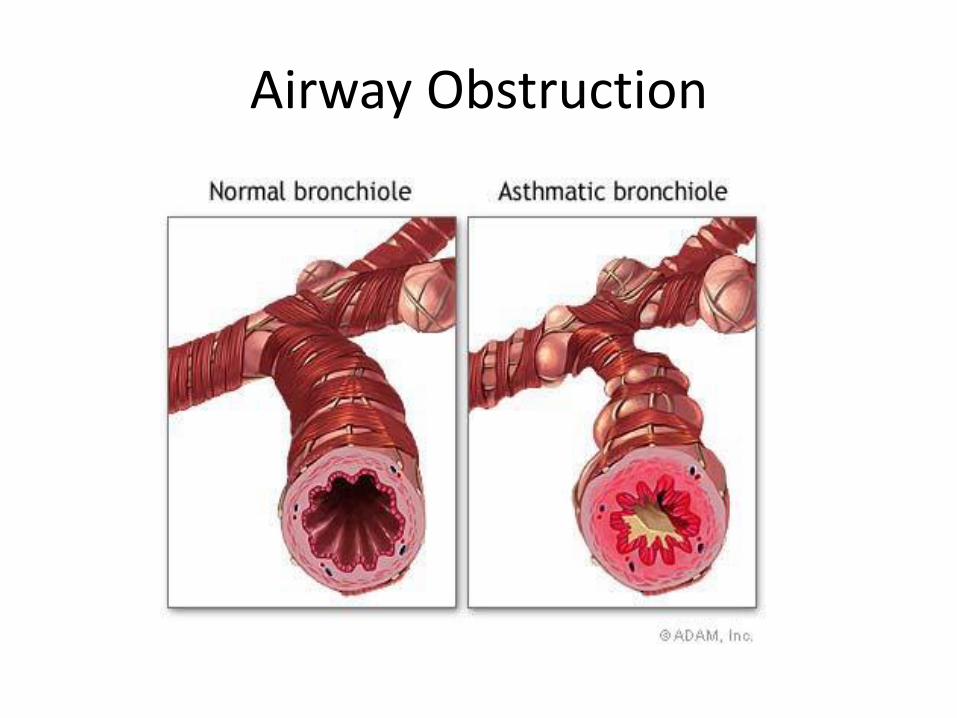
Airway Obstruction
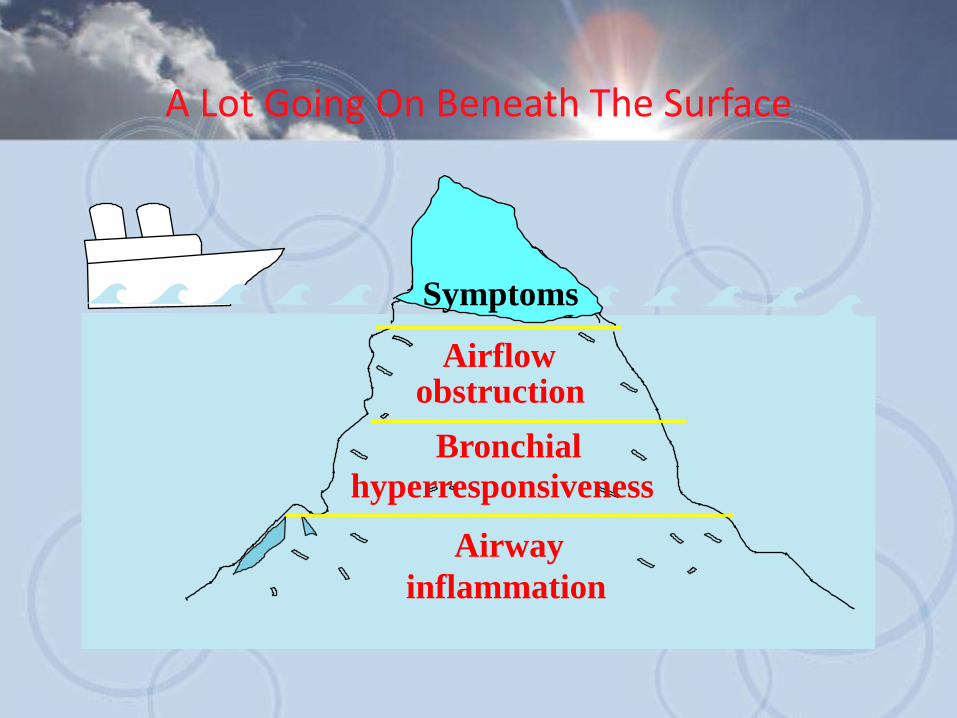
Symptoms
A Lot Going On Beneath The Surface
Airflow obstruction
Bronchial
hyperresponsiveness
Airway
inflammation
Common Symptoms of Asthma
Frequent cough, especially at night
Shortness of breath or rapid breathing
Chest Tightness
Chest pain
Wheezing
Fatigue (not associated with exercise)
Behavior changes
Asthma Triggers
Triggers cause asthma symptoms to begin or get worse.
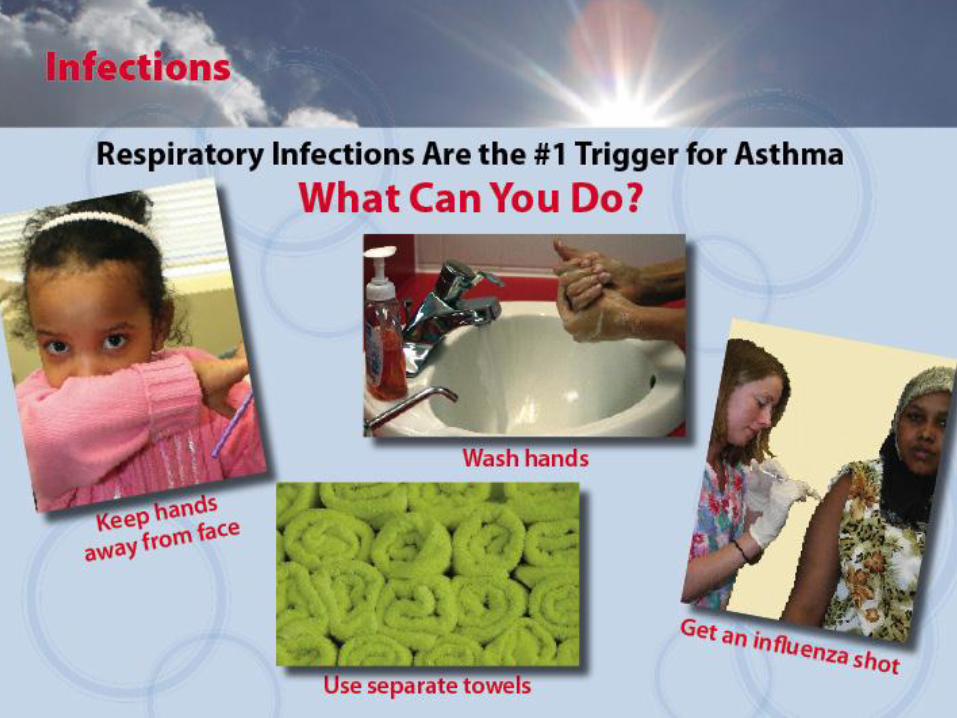
• Infections
• Allergens
• Irritants
• Behaviors
If you avoid asthma triggers, you may prevent asthma episodes and may require less medication to keep your asthma under
control.
Every Child is Unique!
Wheezing and coughing are the most common symptoms -but-
No two children will have the exact same symptoms or the same trigger.
Every child who has a diagnosis of asthma should have access to a quick-relief inhaler!
Every child who has asthma should have an asthma action plan (AAP).
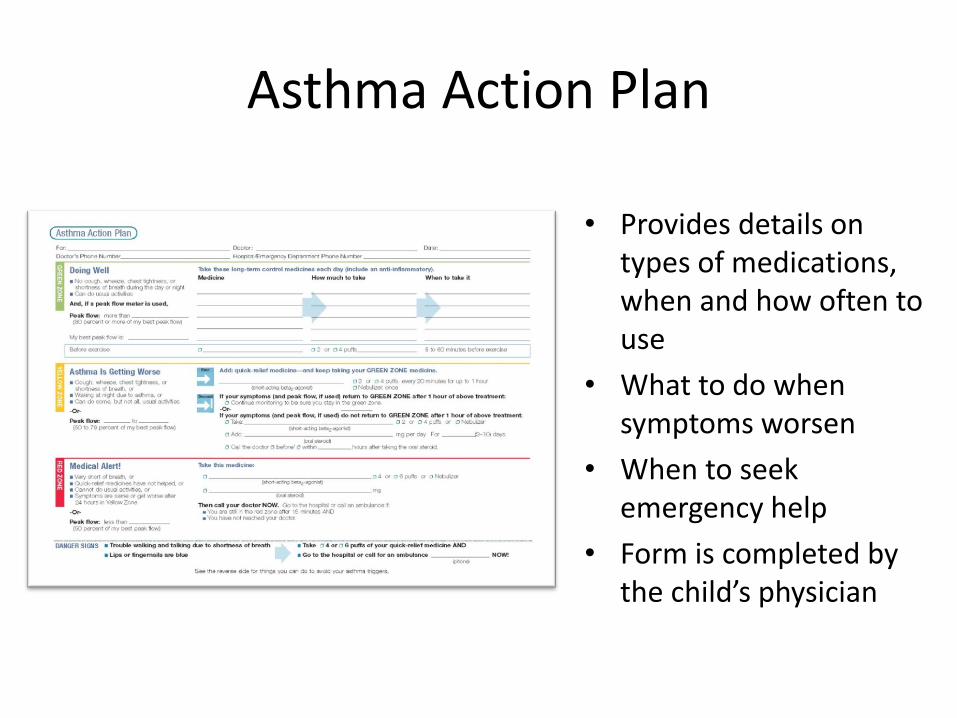
Asthma Action Plan
• Provides details on types of medications, when and how often to use
• What to do when symptoms worsen
• When to seek emergency help
• Form is completed by the child’s physician
Asthma Attacks and Episodes
What is an “ Asthma Episode”?
Occurs when a child or person with asthma is exposed to a trigger or irritant and their asthma symptoms start to appear.
This can occur suddenly without a lot of warning, or build up for several days before the symptoms begin.
Episodes are preventable by avoiding exposure to triggers and taking daily controller medications (inhaled or by pill medication, if prescribed).
How Do I Handle An Asthma Episode On The Field/Gym?
1. Remain calm and re-assure the child.
2. Check the child's asthma action plan or emergency card for actions.
3. Give “quick-relief” medication if ordered and available.
4. Children may carry and self-administer their own asthma inhalers per WV State Code §18522b.*
Handling An Episode cont..
4. Have the child sit up and breathe slowly --
-in through the nose, and out through pursed lips slowly.
5. Have the child sip room temperature water.
6. Contact the parent/guardian as necessary - AND-
7. DO NOT leave the child unattended.
CALL 911 if...
Lips or nail beds are bluish.
Child has difficulty talking, walking or drinking.
Quick relief medication (albuterol) is ineffective or not available.
Neck, throat, or chest muscles are pulling in (retracting).
Nostrils flare out when trying to breathe.
Obvious distress.
Altered level of consciousness/confusion.
Rapidly deteriorating condition.
Exercise Induced Bronchospasm
Formerly Called Exercise Induced Asthma
What Is Exercise Induced Bronchospasm (EIB)?
Formerly referred to as Exercise Induced Asthma
Tightening of the muscles around the airways.
Distinct from other types of asthma because it only happens with aerobic type exercise.
Can be prevented by taking pre-exercise medication and by warming up/cooling down.
About 10% of the general population without asthma, have EIB when they exercise. 1
1. Ohio State University Medical Center www.sportsmedicine.osu.edu/Clinical_Care/asthma.htm
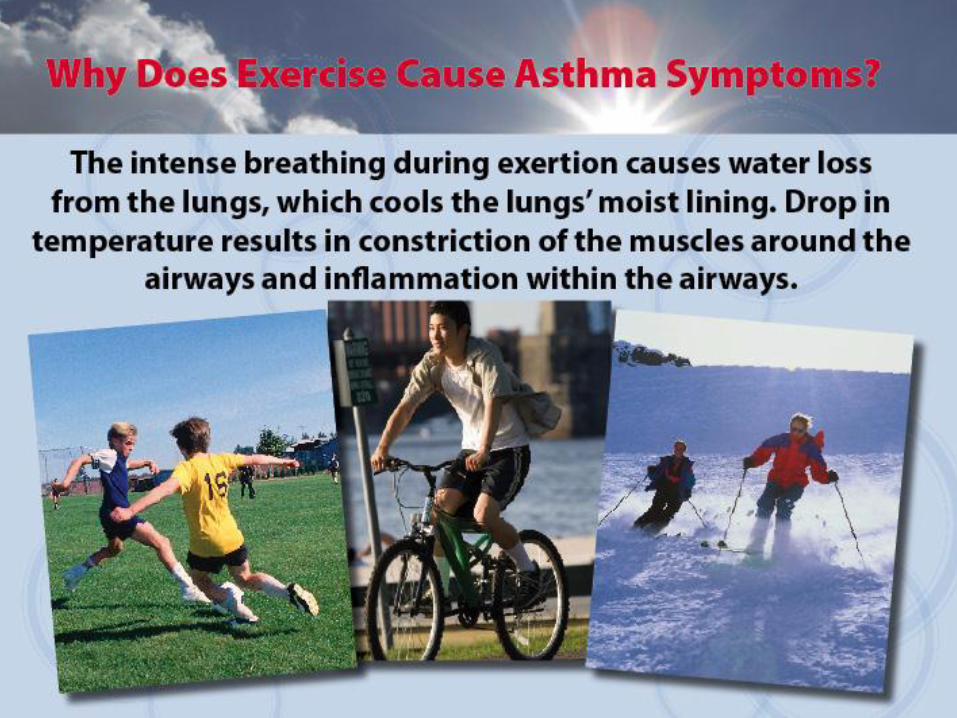
EIB - What Happens?
Symptoms include coughing, wheezing, chest tightness (pressure) and shortness of breath.
Symptoms may begin during exercise and can be worse 5 to 10 minutes after exercise.
EIB can spontaneously resolve 20 to 30 minutes after starting.
Can be avoided by doing the following:
Preventing EIB
Get an Asthma Action Plan from each child/student athlete with asthma - Keep it with you on a clipboard.
Athletes should use quick-relief inhaled medication (Albuterol) 15 -30 minutes before strenuous activity begins.
Do warm-up (5-15 minutes) and cool-down exercises before and after activities.
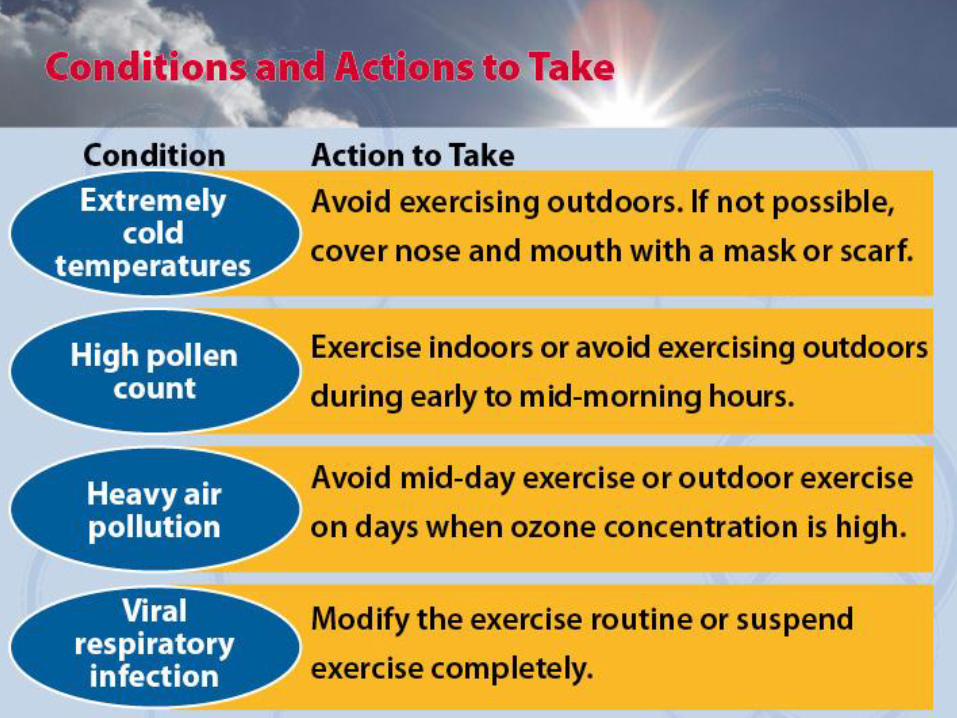
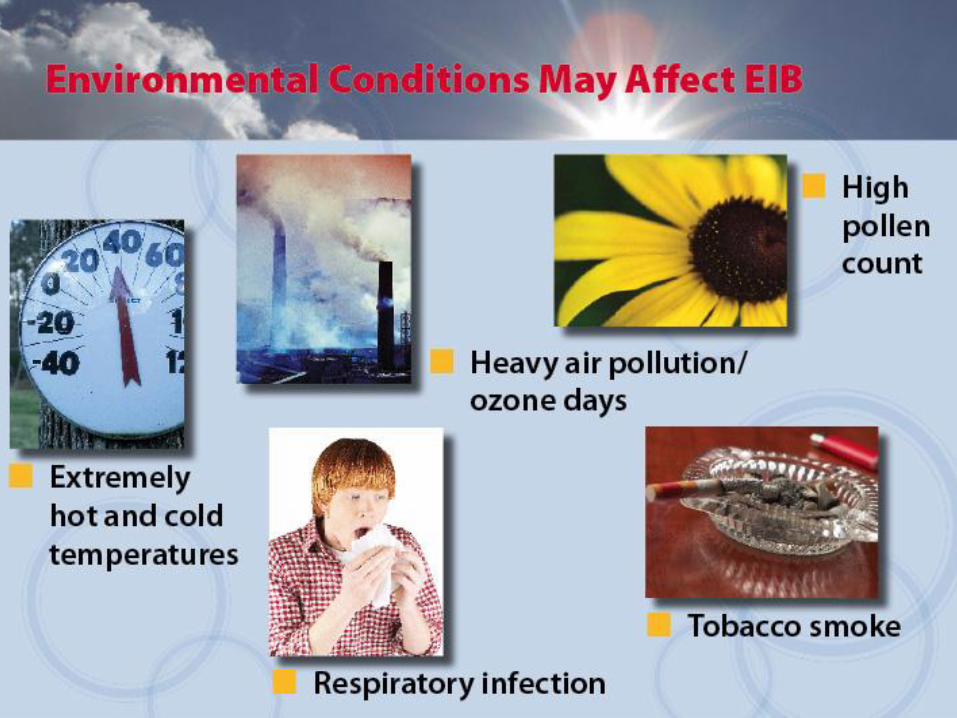
Check outdoor ozone/air quality levels - the local forecast and http://airnow.gov/.
Stay hydrated! Dehydration can exacerbate the issue.
No Bullying! Do not allow other athletes to tease or berate the athlete having asthma symptoms.
Typically taken at home prior to school or sporting activities
Quick Relief Rescue Medications
Taken only when needed to relieve symptoms.
Taken before exercise to prevent exercise induced bronchospasm (EIB) from developing.
Inhaled Meds Include: Albuterol (Proventil, Ventolin, ProAir), and Levalbuterol (Xopenex)
Quick Relief Rescue Medications
Should be taken 10-15 minutes before strenuous or aerobic activity begins.
Taken when needed to relieve symptoms.
Should be immediately and easily accessible at every sporting event.
Coaching staff must be aware that an athlete is using this medication and ready to assist.
Should be taken using a spacer or holding chamber (with the inhaler).
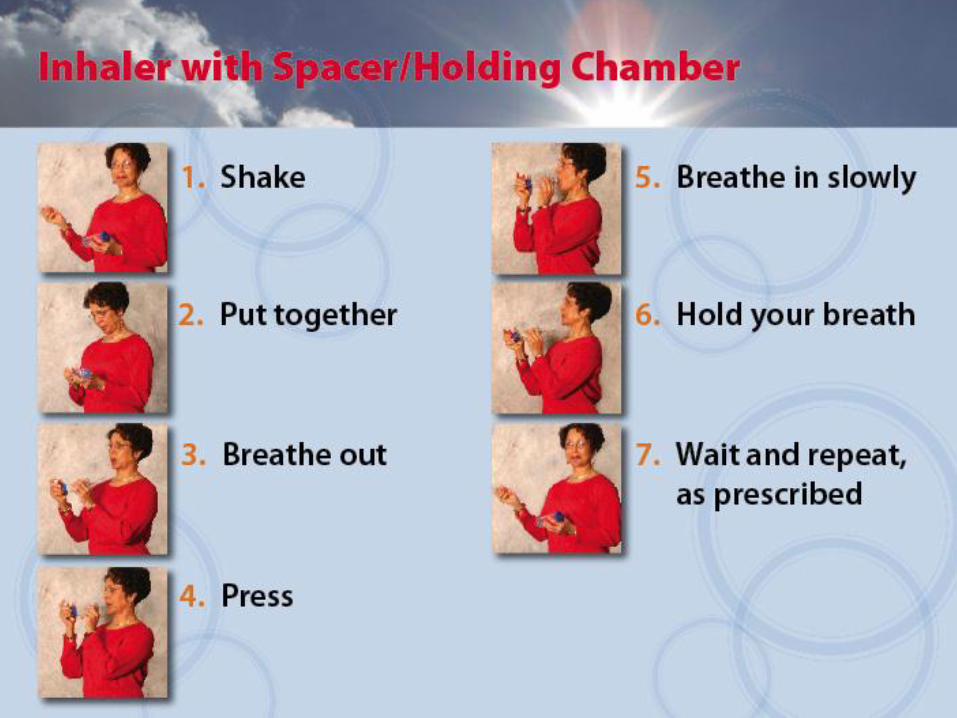
What is a Holding Chamber (spacer) and why should it be used?
WHAT IS A HOLDING CHAMBER • A holding chamber is a 4 - 8 inch long tube that fits on the end of the inhaler mouthpiece.
BENEFITS TO USING A SPACER • Helps the person using it to breathe at their own pace, improving coordination.
• Allows more medicine to reach deep into the lungs.
• Prevents medicine from escaping into the air.
• To be used with people of all ages (holding chambers/spacers with masks for young children are also available).
• The name spacer and holding chamber have been used interchangeably. However, a true Holding Chamber has a one-way valve inside that prevents the medicine from escaping once you have pressed down on the inhaler canister (it also prevents the person from blowing/breathing into the device). Both types, either spacer or valved holding chamber, are used with an inhaler to increase the amount of medicine reaching deep into the lungs. Some inhalers cannot or should not be used with a holding chamber/spacer – these include Maxair, Qvar, any dry powdered inhaler, and other devices. Consult the physician or pharmacist for more information.
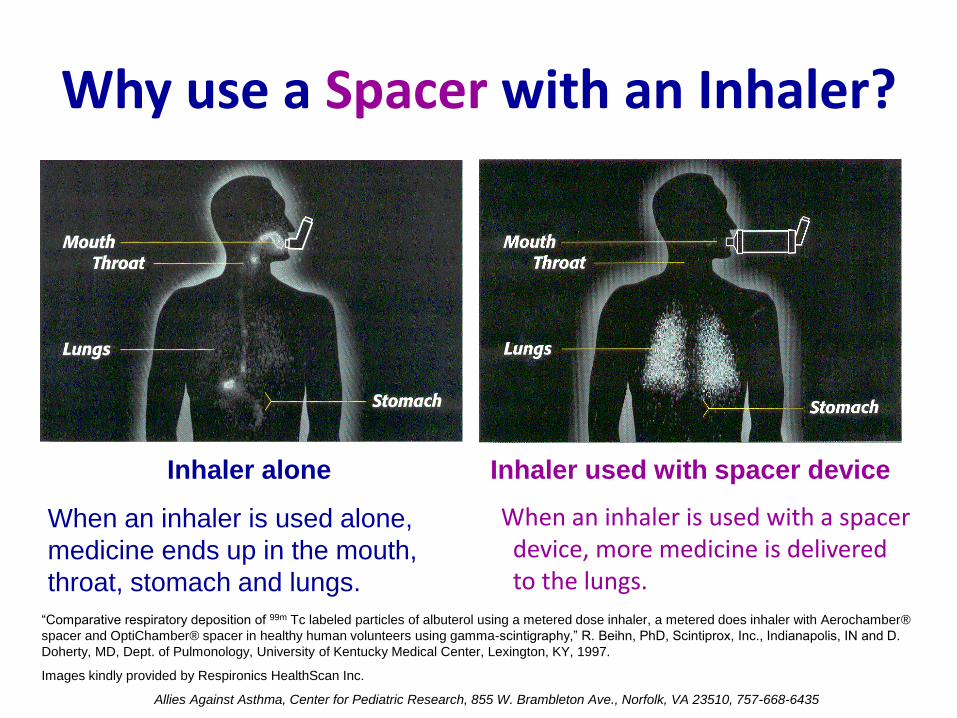
When an inhaler is used alone,
medicine ends up in the mouth,
throat, stomach and lungs.
Inhaler alone
Why use a Spacer with an Inhaler?
Inhaler used with spacer device
When an inhaler is used with a spacer device, more medicine is delivered to the lungs.
“Comparative respiratory deposition of 99m Tc labeled particles of albuterol using a metered dose inhaler, a metered does inhaler with Aerochamber®
spacer and OptiChamber® spacer in healthy human volunteers using gamma-scintigraphy,” R. Beihn, PhD, Scintiprox, Inc., Indianapolis, IN and D.
Doherty, MD, Dept. of Pulmonology, University of Kentucky Medical Center, Lexington, KY, 1997.
Images kindly provided by Respironics HealthScan Inc.
Allies Against Asthma, Center for Pediatric Research, 855 W. Brambleton Ave., Norfolk, VA 23510, 757-668-6435
Devices
Athletes, Keep Asthma in Good Control
Get and use an Asthma Action Plan
Know symptoms and Peak Flow readings for each of the green-yellow-red zones.
Take “controller” medicine daily.
Avoid exposure to triggers.
Find a healthcare provider you trust and go in for asthma check-ups at least twice a year.
Tell your coach and teammates about your asthma.
Take Home Messages
Athletes with asthma can participate in exercise and sports without restrictions.
If an athlete is having trouble participating, their asthma may not be in good control.
Athletes having difficulty should be allowed to rest.
If athletes are having asthma symptoms with activity, encourage them to use quick-relief inhaler 15-30 minutes before the activity or event.
If you have a concern about an athlete, talk with the child and the parents.
Encourage flu shots annually and regular asthma check-ups with their healthcare provider.
Rules You Should Know
• Epi Pen Bill becomes Law 2013
– For undiagnosed anaphylaxis use for allergic reactions
• Existing Laws, Policy, and Rules:
– Inhaler Law – students right to carry and self-administer (2004)
– “No-Idling” – policy for all buses and vehicles over 10,001 lbs. not to idle near schools or school function areas (exceptions noted for weather). Fine of $300 for those who do.
New Asthma Initiative for 2013
• A new project to reduce school absenteeism by students with asthma
• 6,700 each of holding chambers/spacers and peak flow meters purchased. A joint effort with WVDE, WVAEPP, and the Office of Maternal Child & Family Health
• Project to begin dispensing these devices to students diagnosed with asthma in WV Schools beginning the 2013-2014 school year
• School Nurses will be the point of contact at each school.
Everyone Wins When An Athlete Plays Their Game To The Fullest!
Cynthia Keely, BA, RRT, LRTR
Manager
West Virginia Asthma Education and Prevention Program







![[MS-RDPECLIP]: Remote Desktop Protocol: Clipboard … · Remote Desktop Protocol: Clipboard Virtual Channel ... Remote Desktop Protocol: Clipboard Virtual ... Remote Desktop Protocol:](https://static.documents.pub/doc/80x56/5ae3205b7f8b9a097a8dc1a3/ms-rdpeclip-remote-desktop-protocol-clipboard-desktop-protocol-clipboard.jpg)













