49
Cochrane Rapid Response: Accelerating Knowledge Translation for Decision- Makers Chantelle Garritty Ottawa Hospital Research Institute and Catherine Gallagher George Mason University
| Date post: | 29-Dec-2015 |
| Category: |
Documents |
| Upload: | lawrence-mccormick |
| View: | 223 times |
| Download: | 1 times |

Cochrane Rapid Response: Accelerating Knowledge Translation for Decision-Makers
Chantelle GarrittyOttawa Hospital Research Institute
and Catherine Gallagher
George Mason University

Overview
Knowledge translationEvidence synthesis and knowledge translation: inseparableDecision-making dilemmas
Requirement of high rigor evidenceLack of timeMultiple restrictionsFallacies
Cochrane’s approach Rapid Response: Borrowed heavily from KTA Canada
Impact on translationDecision-making outcomes
Rapid response v. Traditional systematic reviewTradesImpactsEvaluation

Rapid reviews in context…and as a precursor to translation
Evidence needs arise… • Both organically and purposively• Within a system with static and dynamic operational parameters• At any level: Locally, nationally and globally• Always within limited resource structures
Rapid reviews should…• Make the very best use of limited resources• Provide a gauge of the distance between status quo and optimum interventions or systems•Have clear implications for practice and for outcomes• Lead to implementation and assessment of impact
Rapid reviews align perfectly with “habits of high value health care organizations”…• Specification and planning – criteria based decision making for clinical and operations•Deliberate design and management of resources for all systems and for sub-population•Measurement and oversight•Self-study (Bohmer, 2011 NEJM)
Here we discuss tools and methods to…• Enhance, automate, and accelerate processes• Limit biases of narrative input, increase transparency, and facilitate investment• Place the rapid review in its larger context of clinical and systems utility• More specifically , understand the relationship between acceleration and dissemination
*Recognize the limitations of current depth and breadth of evidence pool –Bohmer, 2011 NEJM

Part I: Knowledge translation
What is it?
CIHR (2000) “the exchange, synthesis and ethically sound application of knowledge – within a complex system of
interactions among researchers and users – to accelerate the capture of the benefits of research for the public through improved health, more effective services and products, and a strengthened health care system”

Emerged alongside Evidence-based Practice Movement:
“process of moving what we learned through research to the actual applications…
….in a variety of practice settings and circumstances…...the interest in KT appears to coincide with the growing
engagement in the EBP approach in which…
…practitioners make practice decisions based on the integration of the research evidence with clinical expertise and the patient’s unique values and circumstances.”
Straus, Richardson, Glasziou, & Haynes, 2005

Coinciding with knowledge translation movement
Increased:• rigor and standardization of all elements of the scientific process• burden of proof of utility of investigation• investigation into communication methods (dissemination sciences)• open access tools to summarize knowledge base, manage references • move publicly funded research to the public• stakeholder involvement• joint decision making
It is impossible to separate knowledge translation from knowledge generation and synthesis

Why we need evidence synthesis and knowledge translation
1. To make sense of knowledge proliferation– 10,000 new trials each year in MEDLINE– 350,000 new trials each year in Cochrane
2. Public is not benefiting from evidence
30-40% of patients do not receive care according to present scientific evidence20-25% of care provided is not needed or potentially harmful
Grol & Grimshaw (2003) Lancet
3. Current publication practices do not speak language or format of decision makers (both societal and individual)

Why we need evidence synthesis and knowledge translation
4. Calibrate traditional academic model to meet practice needs
Investigator interest versus Social utilityTimeliness versus ExhaustivenessSimplicity of design versus Complexity of social worldGeneralizability versus Local acceptabilityAcademic freedom versus Costs to publicIncreases in standardization versus Loss of natural variationQuantity of publications versus Quality of
reconciliation

What does it look like?
There are many models of the KT process
Commonalities across models include:1. Early and consistent stakeholder engagement2. Standardization of reporting requirements to maximize benefits of research efforts3. Concern with content delivery to public4. Iterative processes

The Ottawa Model of Research Use


Decision-maker dilemmas impacting:evidence synthesis, knowledge translation and implementation
Legislative and funding require use of high rigor evidence for programs and practiceNew burden on practitioners to acquire, interpret, and apply evidenceBeyond skill and resourcesEvidence pool is often underdeveloped
Additional obstacles to evidence incorporation, chief among them:Timepolicy time does not coincide with research timeResourcesfundingavailable qualified labor poolvaluesCultureclinical, organizational, experiential, consensus on values that impact the reception of evidence
Common fallacies in evidence incorporationLocality effect “findings weren’t generate in my district with my people”Experience “we know it works”

Overcoming decision-maker dilemmas
Knowledge translation is designed to reduce the burden to decision-makersBut it is only as good as the preceding steps…
While it is recognized that each step from question formation through dissemination is integral to knowledge translation, we have less progress in the earlier phases
In a word:
Early phases of the knowledge generation and synthesis process must always consider:a. the desired dissemination, translation and implementation goals andb. decision-maker obstacles

Evidence synthesis and knowledge translation are inseparable
Question Refinement Synthesis DecisionTranslation
and Implementation
Socio-political context

Remainder….How do we adapt earlier phases so that knowledge translation reaches the right
people, at the right time, with the right message.?For Cochrane that means can and how can we adapt Cochrane Review methodologies
to increase the likelihood of successful dissemination?
In a word: is there is a viable alternative to the gold standard systematic review

The systematic review dilemma
1. The methodologies that make systematic reviews authoritative take time
…in years… not months, weeks, days or hours
2. Decision-makers often have trouble with evidence importation
…global evidence viewed skeptically…preference for local samples, data, evaluations
3. This leaves knowledge translation and decision-makers with unattractive options to proceed
….without high rigor information, …with a non-representative
sample of high rigor evidence, ….with low rigor evidence.

Cochrane’s Response
Adapts rapid review methodsRelies on KTA’s work on rapid evidence reviewsCreates new protocol that defines processes from question
development to implementation

IDEALLY
The rapid review is a mixed-method, interdisciplinary examination of evidence that directly addresses the “pull” needs of decision makers.
Findings of rapid reviews provide a compass to understand current practice and to set the course for outcome improvements in a specific environment.
Rapid reviews are tailored, fast, and implicitly designed to address implementation decisions.
Error, biases, and wasted time are threats to the value of a rapid review.
INCORPORATIONS TO IMPROVE EFFICIENCIES and IMPACT:
Knowledge management frameworksDiagnosing true knowledge gapsPrioritization criteria
Mixed methods and fieldsSurvey methods research and cognitive interviewingDecision makingUnderstanding of risk and probabilitySimulation research Implementation and evaluation researchPublic health and systems research
Business Lean knowledge workTeamingWork place 360°evaluations

Through our 2-year CIHR KTA research grant, we began to dive into the
realm of ‘rapid reviews.’
Modifying KTA to Cochrane Culture

Local Partnership – KTA Champlain LHIN needed assistance in developing
knowledge capacity Wanted energies directed to “push” activities;
primarily knowledge intelligence services as they required expedient evidence-based answers to help direct policy, implementation, and practice decisions
“Evidence Summaries” – a form of rapid review – was developed and was iteratively refined
A series of evidence summaries (n=19) were produced (~4-6wks each) in response to clinical and health services questions developed with LHIN managers and stakeholders

Scoping Exercise of Rapid Reviews (Ganann et al 2010)
Findings from 70 studies that authors looked at:
•RRs employ a variety of methodologies;
• Variety of different labels (rapid reviews, HTAs; evidence summaries; ultra rapid reviews)
• Seem to vary in depth of description of methods used to abbreviate the process
• Few discussed limitations (what was lost) or what bias was potentially introduced by using RR methods

No universally accepted definition of rapid review
• Closest we’ve come to a definition:– Rapid review (RR) is a type of literature review
produced using accelerated and streamlined systematic review (SR) methods• Using various means to short circuit the
system

KTA Project with the Champlain LHIN

Rapid Review Methods Essentially developed an abbreviated & accelerated
version of current SR methods Borrowing from Cochrane but having to make
certain concessions compared to a traditional SR to accommodate expedited turnaround time (4-6 weeks)
Out of which emerged an 8-step rapid review process developed iteratively across development of 19 ‘Evidence Summaries’ within a 24-month span

Rapid reviews: From start to finishit was an 8-stage approach…
1. Needs assessment (with stakeholders)2. Question development and refinement (PICO/TS)3. Protocol development and approval4. Systematic literature search (with limits)5. Screening and selection of studies (with limits)6. Narrative synthesis of included studies (no meta-analysis)7. Report production phase8. Ongoing follow-up with end users
Objective: high rigour, transparency, and usability

Rapid Reviews vs. Traditional Systematic Review
General Differences- Condensed timeline - Limits set on inclusion criteria of the
search including how grey literature is dealt with
- Post-hoc rethinking of eligibility criteria depending on volume and applicability of evidence
- Heavy reliance on systematic review evidence vs. Inclusion of primary studies (e.g., RCTs or observational studies)
General Similarities- Retains core values of being
transparent to facilitate replication- Adoption of standards to assess
quality of included studies- Share preference for highest
quality studies

Overview of our reports:• Conducted a total of 19 rapid evidence summaries to
date• 13 – focused on clinical initiatives
– 9 across the field of obstetrics/gynaecology• Better Outcomes Registry & Network Ontario (BORN Ontario) –
an initiative to increase capacity to plan and deliver improved maternal-child services
– 6 – focused on health systems/ health services initiatives• Effectiveness of Antimicrobial Stewardship Programs in Hospitals
– Requests came from various stakeholders (n=9)

• Snapshot of Rapid Review report
KTA Interviews – Knowledge Users’ Impressions of Rapid Reviews Approach
Stakeholders(CHAMPLAIN LHIN, BORN ONTARIO, OTTAWA HOSPITAL RESEARCH INSTITUTE
(OHRI), THE OTTAWA HOSPITAL (TOH))• Scientific Director of Performance Measurement – TOH• Chief Information Officer, Champlain LHIN • Former CEO, Champlain LHIN• Clinician, transport nurse, educator, and lactation consultant, BORN ONTARIO• Scientific Manager, BORN ONTARIO• Division Chief, Endocrinology and Metabolism, TOH• Clinical Investigator (MD), Clinical Epidemiology, OHRI, TOH• Senior Health Planning & Engagement Specialist at Champlain LHIN

Knowledge Users’ FeedbackUtility• Structure/ format of summaries is important – eyes
being drawn to key messages (capture reader’s attention)• Thought to be incredibly useful to have evidence at your
fingertips and summarized as it was• Format was user-friendly for non-researcher decisions makers
and clinicians• Format increased level of comfort with data for non-clinicians,
and validated that decisions are made based in part on the evidence provided

Knowledge Users’ Feedback-2• Notion that rapid reviews assists with
having wide group of stakeholders from various backgrounds to get on the same page in terms of understanding what the latest evidence is and what it means (levels out playing field in decision-making so process less prone to group think scenarios)
• Directly influenced practice change in local delivery of care (Example: summaries are being used to move forward on the regional plan on delivering diabetes care)

Knowledge Users’ Feedback-3
• Approach has helped build relationships between those creating the summaries and the implementers - key ingredient to ensure ongoing dialogue
• Notion that the evidence is coming from an “objective, third party” lens – and not from one particular angle/clinical slant, made the findings of the rapid reviews seem more credible
• Rapid reviews were used to help set the context for LHIN discussions, and were key to planning
• Also, used to lay the groundwork as part of a broader environmental scans; ultimately helping with prioritizing of LHIN projects
Knowledge Users’ Feedback-4Barriers• Policy and practice implementation difficult – taking general
evidence and applying it locally found to be challenging• System issues provide obstacles (for example, such as sites where
they only have OR times for 1-day/ week which then controls when surgeries can happen –even though that might not match with when it should be done)
• Unfavourable attitudes towards evidence requires behaviour change efforts (interventions difficult to implement)
• Taking the scientific evidence and translating it into a user-friendly format for a variety of end-users (dissemination science applied)

KTA Dissemination
• Reviews are disseminated on our website (www.ohri.ca/kta), to end-users directly, and when possible, through publication

KTA Publications
Most highly cited article in J of SRs
since published in February 2012;
5237 views/downloads

KTA Teaching & Training
• To date, we have delivered several workshops

Local Program DevelopmentThe Ottawa Hospital Technology Assessment Program (TOHTAP)• Hospital-based knowledge support
service with focus on rapid reviews• Knowledge synthesis + local data +
economical evaluation• Inaugural year with possible long-
term funding commitment (OHRI, TOH Performance Management & Patient Safety groups)


Cochrane Rapid Response....

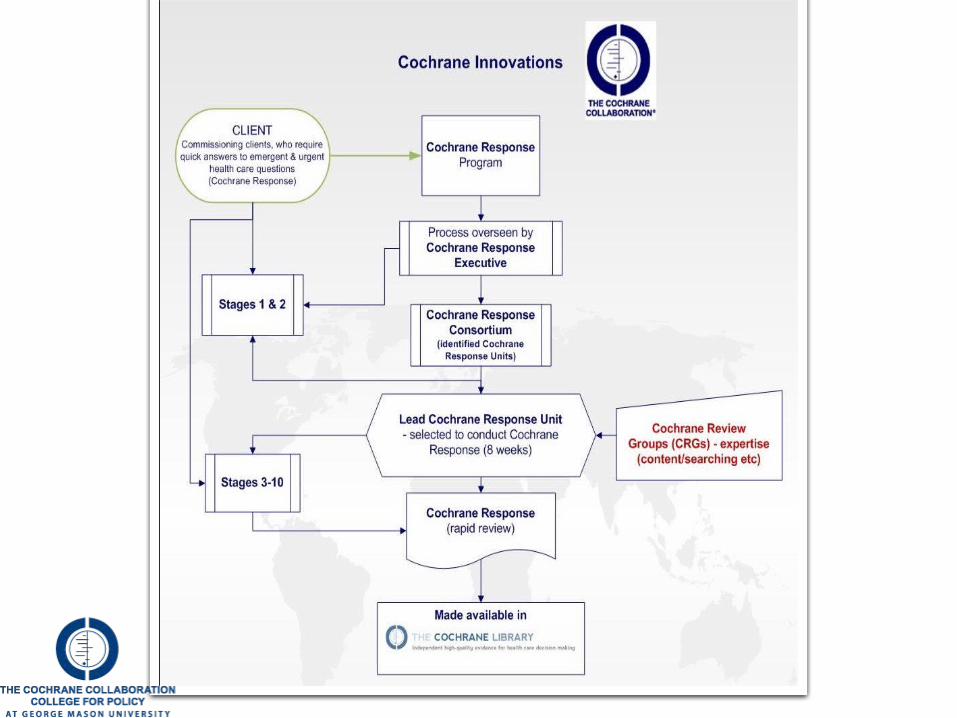
International Program DevelopmentCochrane Innovations• Newly established program by
Cochrane Collaboration with primary goal of providing a mechanism by which Collaboration can respond to requests for commissioned reviews

Cochrane Response
• Rapid reviews are one type of commissioned review, for which the Cochrane version is referred to as “Cochrane Response”
• Currently, small global consortium has been assembled to develop materials to assist in the conduct of Cochrane Responses – to date relied heavily on our KTA approach
• Authors will be experienced Cochrane authors and active members of the Cochrane Response Consortium

• Each requires at least two reviewers, one information retrieval specialist, content expertise, and the necessary input of the client
• Process adds in 24-hour peer review periods with access to input from across the many content and methods experts that make up the collaboration (Cochrane’s 55 Review Groups, 14 Fields, and 12 Methods Groups)
• Each Response is placed on an 8-week schedule and has intermediate deliverables scheduled throughout this period
• There is an intention to publish these rapid reviews through the Cochrane Library, making them available for other decision-makers
Cochrane Response

11-stage process developed based on Cochrane principles, and a review timeline of 8-weeks
Cochrane Response Process
1. Topic Refinement 2. Contracts 3. Problem
Statement4. Protocol
Development
5. Literature Search
6. Screening & Study Selection
7. Data Mining & Extraction 8. Synthesis
9. Report Contruction
10. Contingency Phase
11. Additional Products or
Services

In SummaryIDEALLY
The rapid review is a mixed-method, interdisciplinary examination of evidence that directly addresses the “pull” needs of decision makers.
Findings of rapid reviews provide a compass to understand current practice and to set the course for outcome improvements in a specific environment.
Rapid reviews are tailored, fast, and implicitly designed to address implementation decisions.
Error, biases, and wasted time are threats to the value of a rapid review.
INCORPORATIONS TO IMPROVE EFFICIENCIES and IMPACT:
Knowledge management frameworksDiagnosing true knowledge gapsPrioritization criteria
Mixed methods and fieldsSurvey methods research and cognitive interviewingDecision makingUnderstanding of risk and probabilitySimulation research Implementation and evaluation researchPublic health and systems research
Business Lean knowledge workTeamingWork place 360°evaluations

Evidence and decisions: variables at play
Decision maker characteristics: Goals, Position, Agency, Beliefs, Experiences
Type of decision:•Funding•Service•Refinement or change of practice
Processes used to refine PICO/ST
Resources for evidence synthesis:• Qualified labor•Training integrity•time•funding•Generalizability•Local context
Distance between evidence and current practice
Access and Management of
stakeholder groups
Consensus on utility of question
Question Refinement Synthesis Decision Translation and Implementation
Socio-political context
Diversity of Stakeholder group
Competing priorities:Introduce funding
Do nothing
Translation activities windows missed

US Representative: VA 11th District
Connelly
Cochrane Collaboration
Cochrane Innovations
Targeted patient population within Northern Virginia’s 11th District
US CONGRESS
Ottawa Hospital Research Institute:
uOttawa EPCKnowledge to Action Canada
Extensions of sustainable relationship into Virginia’s 8th and 10th Districts
Congressman Moran
VA 8th District
Congressman Wolf
VA 10th District
INOVA Health Systems
G e o r g e M a s o n U n i v e r s i t y
Chief Medical Officer CMO’s hospitals and Care Centers
I N O V A H E A L T H S Y S T E M S
Cochrane Policy College
Dept of Medicine
Core EDD team
AHRQEffective care
programEPCs, DEcIDE

Rigor requirements needed for all aspects of knowledge generation, rapid review, and dissemination
Empirical assessment of outcome improvementDo those receiving intervention perform better
Retain knowledgeChange practiceShare information
Are practices influencedAre systems refinedIs money saved
How do moderators at each stage affect reception of knowledge
What happens when you manipulate conditionsAssert funding unto schemeIntroduce alternative therapySkip one or more of the steps
What is the best format of findings display (see Dr. Probability next)
Encourage use of limited resources for high utility questions
Does partnership and ongoing delivery encourage change over inserting external evidence?
Decision making trainingDo decision makers understand evidence?Are they able to use it in light of competing priorities? Can they use evidence to ensure greatest clinical, fiscal, social utility?Did change happen?Are outcomes betterAre decisions
Next steps: parsing the variables and assessing their impact so that knowledge translation is truly calibrated for:Type of decisionType of consumerCurrent contextual factors (local vs. global)
Manipulate parametersConduct random assignment to knowledge productsConduct implementation and outcome evaluation
Mixed methods

But what about the medicalisation of
1000 people?

















