Centre of Excellence for Early Childhood Development 1 What Do We Know About Center-Based Programs for Infants and Toddlers? Effective Programs for Early Child Development: Linking Research to Policy and Practice Banff, Canada, March 16 – 19, 2003 Donna Spiker, Ph.D.
Transcript
Centre of Excellence for Early Childhood Development
1
What Do We Know About Center-Based Programs for
Infants and Toddlers?
Effective Programs for Early Child Development: Linking Research to Policy and Practice
Banff, Canada, March 16 – 19, 2003Donna Spiker, Ph.D.
Centre of Excellence for Early Childhood Development
2
Selected Programs for Infants & Toddlers
• Abecedarian Project• Project CARE• Chicago Child-Parent Center• Syracuse Family Development
Research Program • Infant Health and Development
Program
Source: Karoly et al. (1998), Investing in our children.
Centre of Excellence for Early Childhood Development
3
Rationale for IHDP Study
• Neonatal intensive care was saving more and more LBW infants
• LBW infants at risk for delays• When LBW is combined with social risk,
greater chance for delays• Previous intervention research with high
risk samples suggested benefits
Centre of Excellence for Early Childhood Development
4
Areas of Risk for LBW Infants
Centre of Excellence for Early Childhood Development
SOURCE: Klein, N, Hack, M, Gallagher, J., Fanaroff, AA. (1985) Pediatrics.
Centre of Excellence for Early Childhood Development
8
Behavior ProblemsIdentified By Teachers
• Difficulty Attending to Tasks• Difficulty Working Independently• Difficulty Following Directions• Socially Withdrawn• Passive Behavior
SOURCE: Klein NK. (1988). Journal of Special Education
Centre of Excellence for Early Childhood Development
9
Early Intervention Programs for LBW Infants
• Nursery• Home-Based• Combined Nursery and Home-Based
Some Reported Short-term Benefits• Weight Gain at Faster Rate• Reduced Apnea• Enhanced Mother-Child Interaction• Higher Bayley MDI Scores at 6 Months,
1 and 2 Years
Centre of Excellence for Early Childhood Development
10
Preschool Program For NBW, At Risk Children
• Head Start• Perry Preschool Program• Syracuse Family Program• Abecedarian Project• Project CARE
Some Long-term Benefits:• Higher Academic Achievement• Lower Grade Retention• Lower School Drop-out• Reduced Juvenile Delinquency• Increased Employment
Centre of Excellence for Early Childhood Development
11
Rationale for the IHDP
• LBW at risk for health and developmental dysfunction.
• Early intervention studies for NBW at risk children demonstrate positive, long-term effects.
Centre of Excellence for Early Childhood Development
12
However…at the time…..
• Results from these single site studies are not generalizable;
• Biologic constraints of LBW infants might limit their response to intervention;
• The effect of exposure to infections in group care is unknown in LBW infants.
Centre of Excellence for Early Childhood Development
13
A National, Multisite, Randomized Clinical Trial
Purpose: To evaluate a comprehensive intervention designed to improve the health and development of LBW, premature infants.
Program Components:» Early Child Development Services» Family Support Services» Pediatric Follow-up Services
SOURCE: IHDP. (1990). Journal of the American Medical Association. Gross, Spiker & Haynes. (1997). Helping premature, low birth weight babies.
Centre of Excellence for Early Childhood Development
14
Organization of the IHDP
THE ROBERT WOOD JOHNSON FOUNDATON
NATIONAL ADVISORY COMMITTEE
NATIONAL STUDY OFFICE
OFFICE FOR PROGRAM DEVELOPMENT
RESEARCH STEERING COMMITTEE
8 PARTICIPATING UNIVERSITIES
Centre of Excellence for Early Childhood Development
15
Participating Sites
• University of Arkansas for Medical Sciences (ARK)• Albert Einstein College of Medicine (EIN)• Harvard University of Medical School (HAR)• University of Miami School of Medicine (MIA)• University of Pennsylvania School of Medicine (PEN)• University of Texas Health Sciences Center (TEX)• University of Washington School of Medicine (WAS)• Yale University School of Medicine (YAL)
Centre of Excellence for Early Childhood Development
16
Target Sample Size Per Site
Intervention Group (1/3 of total sample)
Follow-up Group(2/3 of total sample)
Total
LighterBirth Weight Group(2/3 of total sample)
30
15
60
30
90
45HeavierBirth Weight Group(1/3 of total sample)
45 90 135Total
Lighter Birth Weight Group = <2000 grams
Heavier Birth Weight Group = 2001-2500 grams
Centre of Excellence for Early Childhood Development
17
IHDP Study Enrollment
Screened for EligibilityProtocol exclusions
Eligible for RecruitmentRefused consent
RandomizedWithdrawn
Primary Analysis Group
4511-3249
1302- 274
1028- 43
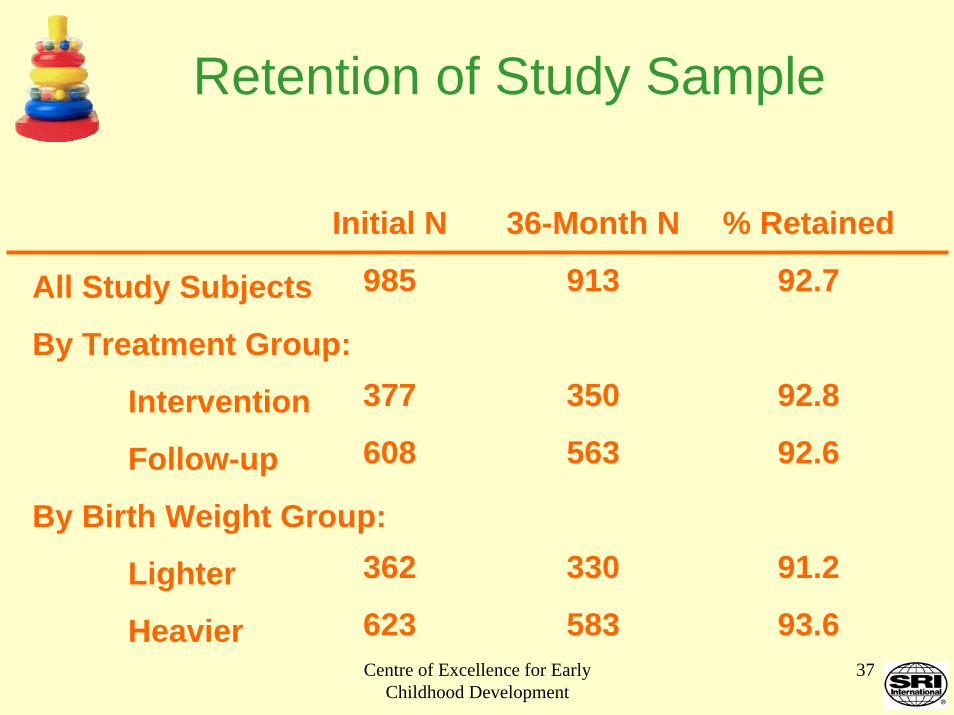
985
Centre of Excellence for Early Childhood Development
18
Reasons for ExclusionExcluded Infants = 3249
Infant death:7%
Resided outside of catchment area:
47%
Other exclusions:20%
Infant medical or maternal exclusion:
7%
Gestational age >37 weeks:
19%
Centre of Excellence for Early Childhood Development
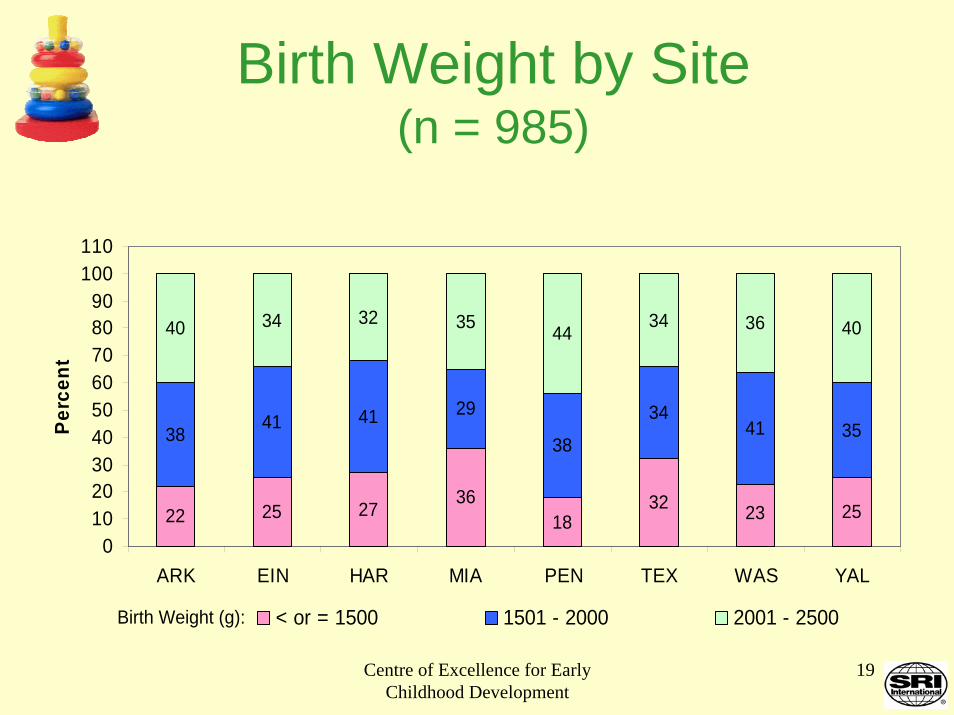
19
Birth Weight by Site(n = 985)
22 25 2736
1832 25
3841 41 29
38
3441 35
40 34 32 35 4434 36 40
23
0102030405060708090
100110
ARK EIN HAR MIA PEN TEX WAS YAL
Birth Weight (g):
Perc
ent
< or = 1500 1501 - 2000 2001 - 2500
Centre of Excellence for Early Childhood Development
20
Maternal Race/Ethnicity by Site(n = 985)
53 4533
7895
71
1738
40
7
131446
15
60
9 15
8159
1
1
2
3
4
0102030405060708090
100110
ARK EIN HAR MIA PEN TEX WAS YAL
Perc
ent
Black Hispanic White, other
Centre of Excellence for Early Childhood Development
21
Maternal Education By Site(n = 985)
3852
16
6444
58
27 21
3318
27
23
33
35
2829
29 30
57
1323
7
45 50
0102030405060708090
100110
ARK EIN HAR MIA PEN TEX WAS YAL
Perc
ent
<12th grade High school graduate Some college
Centre of Excellence for Early Childhood Development
22
Maternal Age By Site(n = 985)
7 11 618 16 20
7
18 117
16 1325
7 9
6457
56
5757
48
5861
1121
319 14 7
31 23
40102030405060708090
100110
ARK EIN HAR MIA PEN TEX WAS YAL
Age in Years:
Perc
ent
< 18 18 & 19 20 - 30 > 30
Centre of Excellence for Early Childhood Development
Centre of Excellence for Early Childhood Development
54
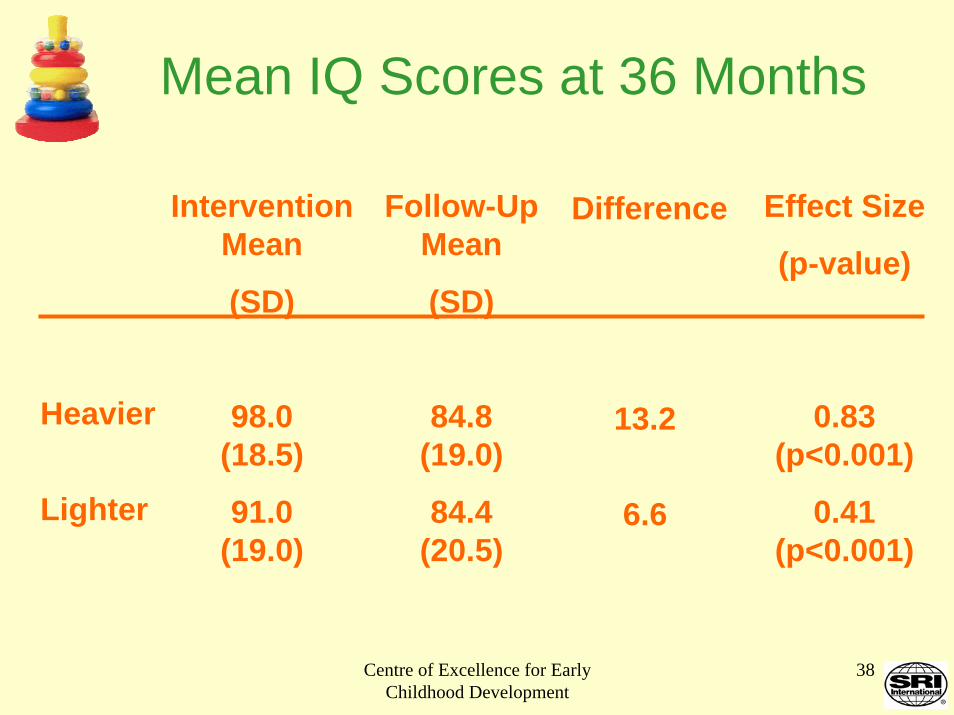
Summary of 36 Month IHDP Results
For Intervention Group Children:
Cognitive Development. Higher IQ scores.Behavioral Competence. Lower maternal report of behavior problemsHealth Status. Higher maternal report of minor illnesses for Lighter group only.
Centre of Excellence for Early Childhood Development
55
Summary of 36 Month IHDP Results (cont’d)
For intervention Group Children:
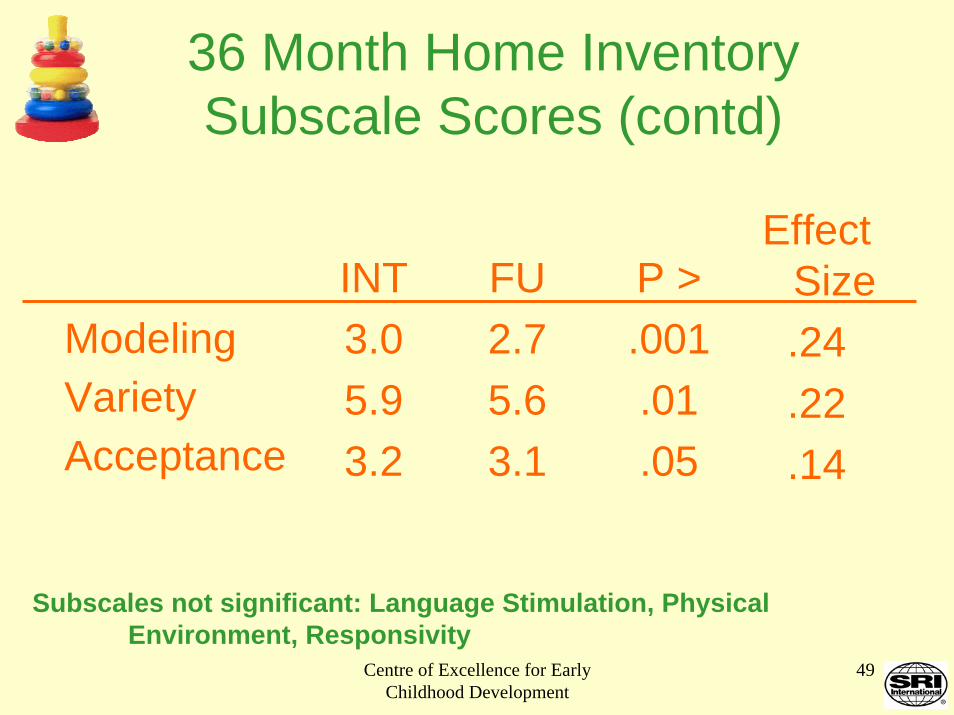
Small, but significant, improvements in:Mother-child interactionChild social competence and task persistenceQuality of home environment
Centre of Excellence for Early Childhood Development
56
Summary of 36 Month IHDP Results (cont’d)
Positive INT effects greatest for:Heavier weight infants
Most disadvantaged infants (lower maternal education, lower family income)
Those with higher levels of participation in the intervention
Positive effects at 7 of 8 sites shows replicability across diverse communities
Centre of Excellence for Early Childhood Development
57
Implications of the IHDP Study:Birth to Age 3
Largest multi-site RCT to evaluate an intervention with LBW infants and toddlers.Site diversity allows generalization of results.Definitive evidence of efficacy of early intervention for LBW premature infants.Greatest effects with those at social risk.Group care feasible for biologically vulnerable infants.Relevance to eligibility issues for early intervention.
Centre of Excellence for Early Childhood Development
58
IHDP Phase II Follow-up
Follow-up of Study Cohort To Determine Long-Term Significance
At Age 5 and Age 8 years
Centre of Excellence for Early Childhood Development
59
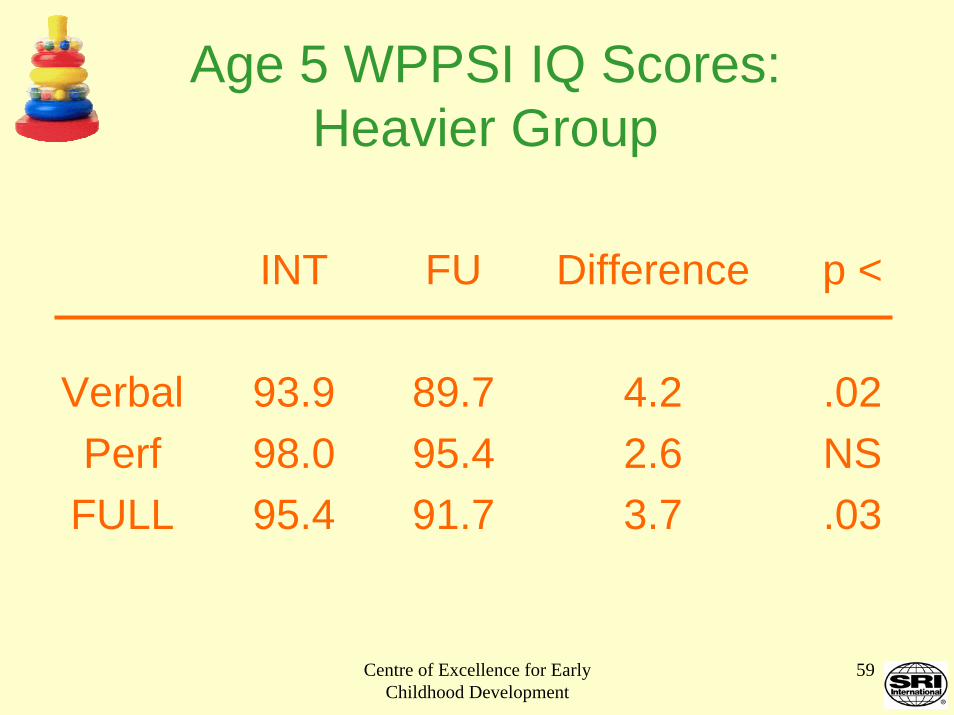
Age 5 WPPSI IQ Scores: Heavier Group
INT
93.998.095.4
FU
89.795.491.7
Difference
4.22.63.7
p <
.02NS.03
VerbalPerf
FULL
Centre of Excellence for Early Childhood Development
60
Age 5 WPPSI IQ Scores: Lighter Group
VerbalPerf
FULL
INT
88.892.689.8
FU
89.594.791.3
Difference
-0.7-2.1-1.5
p <
NSNSNS
Centre of Excellence for Early Childhood Development
61
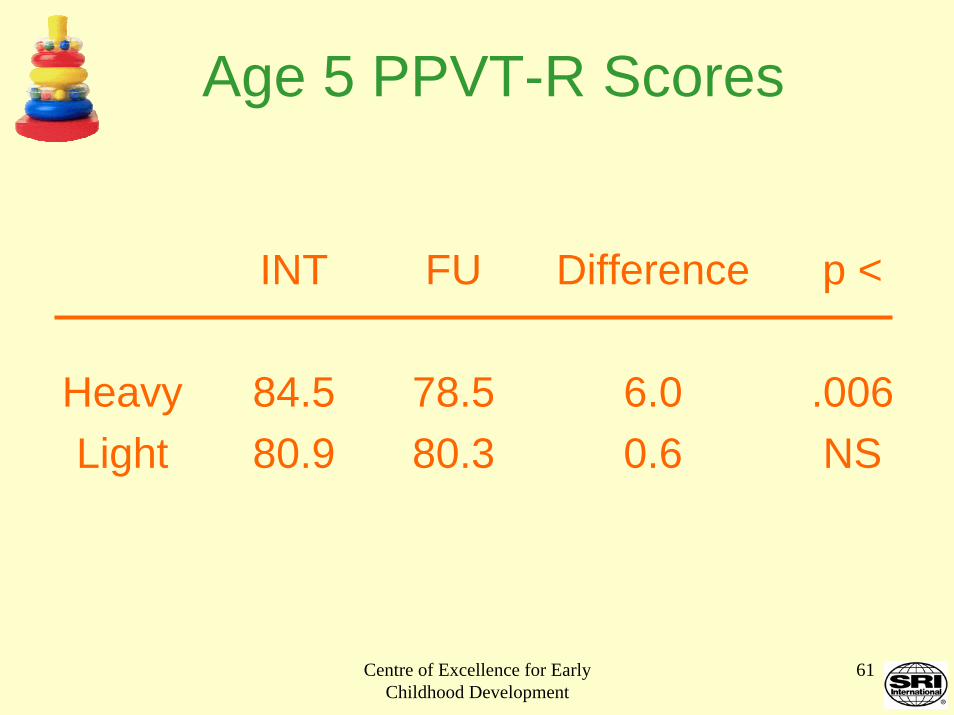
Age 5 PPVT-R Scores
INT
84.580.9
FU
78.580.3
Difference
6.00.6
p <
.006NS
HeavyLight
Centre of Excellence for Early Childhood Development
62
Age 5 Child Behavior Checklist Scores
INT
29.233.131.9
FU
33.332.833.0
Difference
-4.10.4
-1.1
p <
.06NSNS
HeavyLight
TOTAL
Centre of Excellence for Early Childhood Development
63
Age 5 Health Measures
No significant treatment differences for:
• Morbidity Index• Hospitalizations
Centre of Excellence for Early Childhood Development
64
What can we say about key components of high-quality center-based programs for
infants and toddlers?
Centre of Excellence for Early Childhood Development
65
Key Program Characteristics
• Small group size• High teacher-child ratio• High health & safety standards• Appropriate facilities and play materials• Well-trained teachers• Transportation to center (if needed)
Centre of Excellence for Early Childhood Development
66
Key Program Characteristics (contd)
• Consultation with health providers and social workers
• Attention to parent-center communication and alliance via:– Parent groups – Home visits– Parent-teacher communication (notes,
visits to center)
Centre of Excellence for Early Childhood Development
67
Key Program Characteristics (contd)
• Developmentally-appropriate curriculum:– Play-based– Has affective and cognitive focus
• Ongoing monitoring and training to assure implementation of educational curriculum
Centre of Excellence for Early Childhood Development
68
Essential Features of Curriculum• Encourage exploration• Mentor in basic skills• Celebrate developmental advances• Guided rehearsal & extension of new
skills• Protect from inappropriate disapproval,
teasing, or punishment• Provide a rich & responsive language
Centre of Excellence for Early Childhood Development
73
References
Blair, C., Ramey, C. T., & Hardin, J. (1995). Early intervention for low birth-weight, premature infants: Participation and intellectual development. American Journal on Mental
Retardation, 99, 542-554.
Bradley, R. H., Whiteside, L., Caldwell, B. M., Casey, P. H., Kelleher, K. H., & Pope, S. (1993). Maternal IQ, the home environment, and child IQ in low-birth-weight, premature
children. International Journal of Behavioral Development, 16, 61-74.
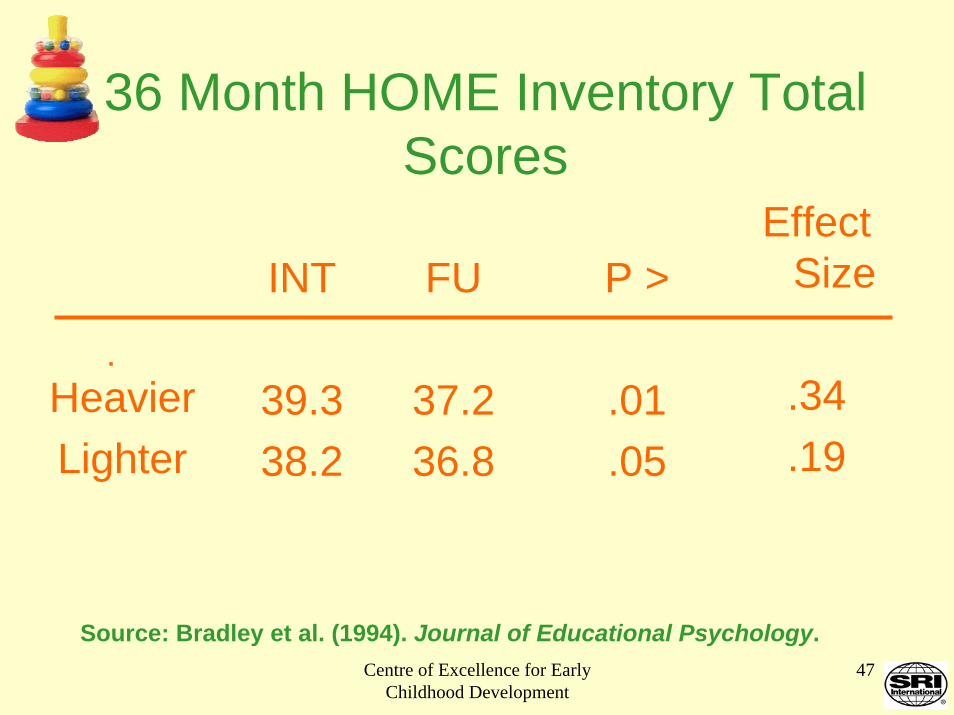
Bradley, R. H., Whiteside, L., Mundfrom, D. J., Casey, P. H., Caldwell, B. M., & Barrett, K. (1994). Impact of the Infant Health and Development Program (IHDP) on the home
environments of infants born prematurely and with low birth-weight. Journal of Educational Psychology, 86, 531-541.
Bradley, R. H., Whiteside, L., Caldwell, B. M., Casey, P. H., Kelleher, K., Pope, S., Swanson, M., & Barrett, K. (1994). Maternal IQ, the home environment, and child IQ in low birthweight, premature children. International Journal of Behavioral Development, 16, 61-
74
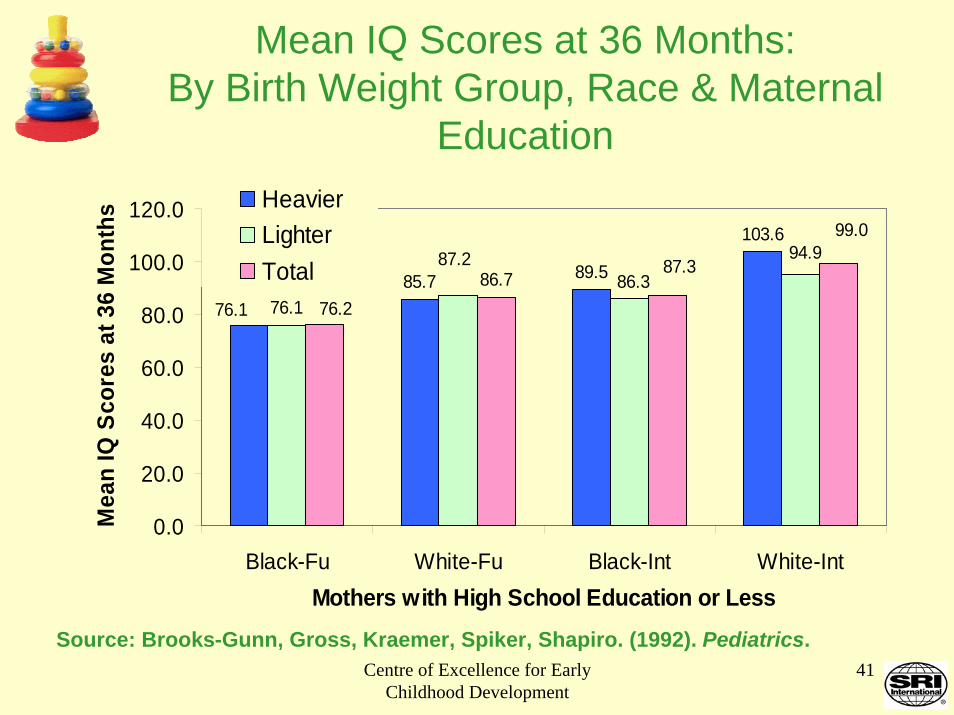
Brooks-Gunn, J., Gross, R., Kraemer, H. C., Spiker, D., & Shapiro, S. (1992). Enhancing the cognitive outcomes of low-birth-weight, premature infants: For whom is the intervention
most effective? Pediatrics, 89, 1209-1215.
Centre of Excellence for Early Childhood Development
74
Brooks-Gunn, J., Kelbanov, P. K., Liaw, F., & Spiker, D. (1993). Enhancing the development of low-birth-weight, premature infants: Changes in cognition and behavior over the first three years.
Child Development, 64, 736-753.
Brooks-Gunn, J., McCarton, C. M., Casey, P. H., McCormick, M. C., Bauer, C. R., Bernbaum, J. C., et al. (1994). Early intervention in low-birth-weight premature infants: Results through age 5
years from the Infant Health and Development Program. Journal of the American Medical Association, 272, 1257-1262.
Brooks-Gunn, J., McCormick, M. C., Shapiro, S., Benasich, A., & Black, G. W. (1994). The effects of early education intervention on maternal employment, public assistance, and health
insurance: The Infant Health and Development Program. American Journal of Public Health, 84, 924-931.
Burchinal, M., Roberts, J.E., Nabors, L.A., & Bryant, D.M. (1996). Quality of center child care and infant cognitive and language development. Child Development, 67, 606-620.
Burchinal, M. , Roberts, J.E., Riggins, R, Jr., Zeisel, S.A., Neebe, E., & Bryant, D.M. (2000). Relating quality of center-based child care to early cognitive and language development
longitudinally. Child Development, 71, 338-357.
Campbell, F. A., & Ramey, C. T. (1994). Effects of early intervention on intellectual and academic achievement: A follow-up study of children from low-income families. Child
Development, 65, 684-698.
Centre of Excellence for Early Childhood Development
75
Campbell, F. A, Pungello, E.P., Miller-Johnson, S., Burchinal, & M. Ramey, C.T. (2001). The development of cognitive and academic abilities: Growth curves from an early childhood
Duncan, G. J., Brooks-Gunn, J., & Klebanov, P. (1994). Economic deprivation and early childhood development. Child Development, 65, 296-318.
Gross, R., Brooks-Gunn, J., & Spiker, D. S. L. Friedman & M. Sigman (Eds.). (1992). The psychological development of low- birth-weight children., Annual Advances in Applied
Developmental Psychology, (Vol. 6, pp. 411-433). Norwood, New Jersey: ABLEX Publishing Corporation.
Gross, R. T., Spiker, D., & Haynes, C. W. (Eds.). (1997). Helping low birth weight, premature babies: The Infant Health and Development Program. Stanford, CA. Stanford University Press.
Guralnick, M. J. (1998). Effectiveness of early intervention for vulnerable children: A developmental perspective. American Journal on Mental Retardation, 102, 319-345.
Hollomon, H. A., & Scott, K. G. (1998). Influence of birth-weight on educational outcomes at age 9: The Miami site of the Infant Health and Development Program. Journal of
Developmental and Behavioral Pediatrics, 19, 404-410.
Centre of Excellence for Early Childhood Development
76
Howes, C., Phillips, D.A., & Whitebook, M. (1992). Thresholds of quality: Implications for the social development of children in center-based child care. Child Development, 63, 449-460.
Infant Health and Development Program. (1990). Enhancing the outcomes of low-birth-weight, premature infants: A multi-site, randomized trial. Journal of the American Medical Association,
263, 3035-3042.
Infant Health and Development Program. (1997). Results at age 8 years of early intervention for low-birth--weight premature infants. Journal of the American Medical Association, 277, 126-132.
Karoly, L. A., Greenwood, P. W., Everingham, S. S., Hoube, J., Kilburn, M. R., Rydell, C. P., Sanders, & M., Chiesa, J. (1998). Investing in our children: What we know and don't know about
the costs and benefits of early childhood interventions. Santa Monica, CA: Rand Corporation.
Knitzer, J. (2001). Federal and state efforts to improve care for infants and toddlers. Future of Children, 11, 78-97.
Liaw, F. R., & Brooks-Gunn, J. (1993). Patterns of low-birth-weight children's cognitive development. Developmental Psychology, 29, 1024-1035.
Leventhal, T., Brooks-Gunn, J., McCormick, M.C., & McCarton, C.M. (2000). Patterns of service use in preschool children: Correlates, consequences, and the role of early intervention. Child
Development, 71, 802-819.
Centre of Excellence for Early Childhood Development
77
McCarton, C, Brooks-Gunn, J., Wallace, I., Bauer, C. R., Bennett, F. C., Bernbaum, J. C., Broyles, S., Casey, P., McCormick, M., Scott, D., Tyson, J., Tonascia, J. & Meinert, C. (1997). Results at age 8 years of early intervention for low-birth-weight premature infants: The Infant
Health and Development Program. Journal of the American Medical Association, 277, 126-132.
McCormick, M. C., Brooks-Gunn, J., Shapiro, S., Benasich, A., Black, G. W., & Gross, R. (1991). Health care use among young children in day care. Journal of the American Medical Association,
265, 2212-2217.
McCormick, M., McCarton, C., Brooks-Gunn, J., Belt, P., & Gross, R. (1998). The Infant Health and Development Program: Interim summary. Journal of Developmental and Behavioral
Pediatrics, 19, 359-370.
McCormick, M.,McCarton, C.,Brooks-Gunn, J.Belt, P., & Gross, R. (1998). The Infant Health and Development Corporation: Interim summary. Journal of Developmental & Behavioral Pediatrics,
19, 359-370.
Ramey, C.T., Ramey, S.L.(1992). Effective early intervention. American Journal on Mental Retardation, 30,337-345.
Ramey, C. T., Bryant, D., Wasik, B. H., Sparling, J., Fendt, K., & LaVange, L. M. (1992). Infant Health and Development Program for low birth weight, premature infants: Program elements,
family participation, and child intelligence. Pediatrics, 89, 454-465.
Centre of Excellence for Early Childhood Development
78
Ramey, C. T., Campbell, F. A., Burchinal, M., Bryant, D., Wasik, B. H., Skinner, M. L., & Gardner, D.M. (1999). Early learning, later success: The Abecedarian Study. Available from
the Frank Porter Graham Child Development Institute at: [email protected]
Reynolds, A. J. (1994). Effects of a preschool plus follow-on intervention for children at risk. Developmental Psychology, 30, 787-804.
Reynolds, A. J. (1998). Developing early childhood programs for children and families at risk: Research-based principles to promote long-term effectiveness. Children & Youth Services
Review,20,503-523.
Reynolds, A. J., & Temple, J. A. (1998). Extended early childhood intervention and school achievement: Age thirteen findings from the Chicago Longitudinal Study. Child Development,
69, 231-246.
Reynolds, A. J., Chang, H., & Temple, J. A. (1998). Early childhood intervention and juvenile delinquency: An exploratory analysis of the Chicago Child-Parent Centers. Evaluation
Review, 22, 341-372.
Reynolds, A. J. (1999). Educational success in high-risk settings: Contributions of the Chicago Longitudinal Study. Journal of School Psychology, 37, 345-354.
Reynolds, A. J., Temple, J. A., Robertson, D. L., & Mann, E. A. (2001). Long-term effects of an early childhood intervention on educational achievement and juvenile arrest: A 15-year
follow-up of low-income children in public schools. Journal of the American Medical Association, 285, 2339-2378.
Centre of Excellence for Early Childhood Development
79
Sparling, J., Lewis, I., Ramey, C. T., Wasik, B. H., Bryant, D., & LaVange, L. M. (1991). Partners: A curriculum to help premature, low birth-weight infants get off to a good start.
Topics in Early Childhood Special Education, 11, 36-55.
Spiker, D., Kraemer, H. C., Scott, D. T., & Gross, R. T. (1991). Design issues in a randomized clinical trial of a behavioral intervention: Insights from the Infant Health and
Development Program. Journal of Developmental and Behavioral Pediatrics, 12, 386-393.
Spiker, D., Ferguson, J., & Brooks-Gunn, J. (1993). Enhancing maternal interactive behavior and child social competence in low-birth-weight, premature infants. Child
Development, 64, 754-768.
Wasik, B.H., Ramey, C.T., Bryant, D.M., & Sparling, J.J. (1990). A longitudinal study of two early intervention strategies: Project CARE. Child Development, 61,1682-1696.