Page 1
DOI:10.4158/EP13460.OR © 2013 AACE.
ENDOCRINE PRACTICE Rapid Electronic Article in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited, typeset and finalized. This version of the manuscript will be replaced with the final, published version after it has been published in the print edition of the journal. The final, published version may differ from this proof. DOI:10.4158/EP13460.OR © 2013 AACE. Original Article EP13460.OR
A DIAGNOSTIC SCORING SYSTEM FOR MYXEDEMA COMA
Running title: Diagnostic Scoring for Myxedema Coma
Geanina Popoveniuc, MD1, 2, Tanu Chandra, MD3, 4, Anchal Sud, MD1, Meeta Sharma, MD1, Marc R. Blackman, MD 2, 4, 5, Kenneth D. Burman, MD1, Mihriye Mete,
PhD 6,7 , Sameer Desale, MS 6,7 , Leonard Wartofsky, MD1
From: 1Division of Endocrinology, Department of Medicine, MedStar Washington Hospital Center, Washington DC; 2Division of Endocrinology, Department of Medicine, Georgetown University Hospital, Washington DC; 3Division of Endocrinology, Department of Medicine, Veterans Affairs Medical Center, Washington DC; 4Division of Endocrinology, Department of Medicine, George Washington University Hospital, Washington, DC; 5Research Service (151), Veterans Affairs Medical Center, Washington DC; 6 Department of Biostatistics and Bioinformatics, Medstar Health Research Institute, Hyattsville, MD; 7 Georgetown-Howard Universities Center for Clinical and Translational Sciences, Washington, DC (GHUCCTS-CTSA)
Correspondence address: Geanina Popoveniuc MD, address: 110 Irving Street NW, 2A72, Washington, DC, 20010-2975. Email: [email protected]
Page 2
DOI:10.4158/EP13460.OR © 2013 AACE.
Keywords: myxedema coma; hypothyroidism; diagnosis; scoring system.
Abstract
Objective: To develop diagnostic criteria for myxedema coma (MC), a decompensated state
of extreme hypothyroidism with a high mortality rate if untreated, in order to facilitate its
early recognition and treatment.
Methods: The frequencies of characteristics associated with MC were assessed
retrospectively in patients from our institutions, in order to derive a semiquantitative
diagnostic point scale that was further applied on selected patients from literature. Logistic
regression analysis was used to test the predictive power of the score. Receiver operating
characteristic (ROC) curve analysis was performed to test the discriminative power of the
score.
Results: Of the 21 patients, 7 were re-classified as not having MC (non-MC), and they were
used as controls. The scoring system included a composite of alterations of thermoregulatory,
central nervous, cardiovascular, gastrointestinal, and metabolic systems, and presence or
absence of a precipitating event. All our 14 MC patients had a score of ≥ 60, whereas 6/7 non-
MC patients had scores of 25-50. Sixteen of 22 MC patients from literature had a score ≥ 60,
and 6/22 scored between 45 - 55. The odds ratio per each score unit increase as a continuum
was 1.09 (95% CI, 1.01-1.16; p =0.019); a score of 60 identified coma with an odds ratio of
Page 3
DOI:10.4158/EP13460.OR © 2013 AACE.
1.22.The area under the ROC curve was 0.88 (95% CI, 0.65-1.00), and the score of 60 had
100% sensitivity, and 85.71% specificity.
Conclusions: The scoring system proposed indicates a score of ≥ 60 potentially diagnosing
MC, whereas scores between 45-59 could classify patients at risk for MC.
Abbreviations: MC = myxedema coma; ROC = receiver operating characteristic; TSH = thyroid stimulating hormone; T4 = thyroxine; T3 = triiodothyronine; GCS = Glasgow Coma Scale APACHE II = Acute Physiology and Chronic Health Evaluation; SOFA = Sequential Organ Failure Assessment; SD = standard deviation; MWHC = Medstar Washington Hospital Center; VAMC = Veterans Affair Medical Center.
Introduction
Myxedema coma is a rare form of extreme hypothyroidism with a mortality rate that may
approach 60% [1]. The condition represents a state of decompensated hypothyroidism that
usually occurs after a period of longstanding, unrecognized or poorly controlled thyroid
hypofunction and is often precipitated by a superimposed systemic illness. Such precipitating
or exacerbating factors include infection, trauma, certain medications, hypothermia,
cerebrovascular accident, congestive heart failure, metabolic disturbances, and electrolyte
abnormalities [1-3]. If left untreated, the clinical course is one of multi-organ dysfunction with
characteristic lethargy progressing to altered sensorium (stupor, delirium, and coma).
Hypothermia is a key early manifestation in most patients and may be quite profound (less
than 26° C). Respiratory depression leading to hypoventilation and hypercapnia may
Page 4
DOI:10.4158/EP13460.OR © 2013 AACE.
necessitate intubation and mechanical ventilation. Decreased cardiac contractility,
bradycardia, cardiomegaly, and arrhythmias may lead to hypoperfusion and cardiogenic
shock. Other common abnormalities seen in patients with myxedema coma include
gastrointestinal dysfunction, renal impairment, hyponatremia, hypoglycemia, hypoxemia and
anemia [1].
The diagnosis of myxedema coma is usually based on clinical manifestations, a history of
moderate to severe hypothyroidism, and is confirmed by laboratory testing, with elevated
serum thyrotropin (TSH), and decreased total and free thyroxine (T4), and triiodothyronine
(T3). Early diagnosis, supportive care, and treatment with intravenous thyroxine have been
shown to improve outcomes [4]. Recent reports including prospective studies [2, 3, 5] have
focused on establishing predictors of poor outcome in patients with myxedema coma.
Coma on admission, lower GCS (Glasgow Coma Scale) score and an APACHE II (Acute
Physiology and Chronic Health Evaluation) score of < 20 were demonstrated to be reliable
predictors of higher mortality in the prospective study of Rodriquez et al. [2] of 11 patients
with myxedema coma. They also noted that the mean age of survivors was lower than that of
non-survivors, albeit not statistically significantly. Heart rate, body temperature, mean free
T4, and mean TSH did not differ between survivors and non-survivors. Dutta et al [3], in a
report of 23 patients with myxedema coma, found hypotension and bradycardia on admission,
need for mechanical ventilation, hypothermia unresponsive to treatment, sepsis, intake of
sedative drugs, lower GCS score, and high APACHE II and SOFA (Sequential Organ Failure
Assessment) scores highly predictive of a poor outcome. Results from a Medline search of 82
Page 5
DOI:10.4158/EP13460.OR © 2013 AACE.
cases of myxedema coma [5] revealed that older age, cardiac complications, such as
hypotension and sinus bradycardia with low voltage QRS, and high dose thyroid hormone
replacement during treatment for myxedema coma were associated with a fatal outcome after
1 month of therapy. There was no significant difference in mortality based upon the APACHE
II score and the presence of pulmonary complications.
The diagnosis of myxedema coma is mainly clinical, with no clear cut criteria that might
distinguish either hypothyroidism alone or coma of other etiologies from true myxedema
coma. In view of the high morbidity and mortality of myxedema coma [2], the development
and application of criteria for its identification could allow earlier diagnosis and treatment that
may have a salutary effect on prognosis for recovery and outcome. [4]
Materials and Methods
Study population
Our study population was based on all patients age 18 years and older who presented to
MedStar Washington Hospital Center (MWHC), Washington DC and Veterans Affair (VA)
Medical Center, Washington DC from 1989 to 2009, with an admitting or discharge diagnosis
of myxedema coma.
Definitions
The following definitions and grading systems were employed: hypothermia was defined as a
temperature lower than 35°C. Bradycardia was defined as heart rate less or equal to 60 beats
per minute and hypotension as blood pressure less than 90/60 mmHg, or a mean arterial
Page 6
DOI:10.4158/EP13460.OR © 2013 AACE.
pressure less than 70. Neurological findings were graded based on the severity of mental
status changes, from somnolence to obtundation, stupor and coma. Obtundation was defined
as less than full mental capacity, but still easy arousable with persistence of alertness for brief
periods of time [1]. Stupor was applied to the state of lack of critical cognitive function and
level of consciousness, responsiveness only to painful stimuli, while coma was considered to
be the state of complete lack of responsiveness. Hypoglycemia was defined as a blood glucose
level < 60 mg/dL and hyponatremia was classified as a serum sodium < 135 mEq/L . To
define hypoxemia we used a threshold for oxygen saturation at room temperature of less than
88% or pO2 less than 55 mmHg, while hypercapnia was indicated by a pCO2 level of 50
mmHg or greater. The diagnosis of primary hypothyroidism was based on levels of total or
free thyroxine (T4) below the reference range together with an elevated serum TSH.
Reference ranges were as follows: total T3 71-180 ng/dL, total T4 4.5 -12 ug/dL, free T4 0.8 -
1.7 ng/dL, and TSH 0.45 – 4.5 mIU/L.
Methodology
Each chart was retrospectively reviewed (by GP and TC) to note patient demographics and the
clinical manifestations of myxedema coma in each patient on presentation. The following
characteristics were recorded for each patient: demographics (gender, age, race, past medical
history, to include history of hypothyroidism, or thyroid surgery, medications, medication
non-compliance), vital signs at the time of MC diagnosis (temperature, heart rate, respiratory
rate, blood pressure, oxygen saturation), respiratory status (supplemental oxygen, mechanical
ventilation), neurological status (somnolence, lethargy, obtundation, stupor, coma, seizures),
gastrointestinal manifestations (anorexia, abdominal pain, constipation, decreased/absent
intestinal motility), laboratory findings (complete metabolic panel, TSH, free T4 and total T3,
Page 7
DOI:10.4158/EP13460.OR © 2013 AACE.
blood cultures, urine cultures), electrocardiographic findings, chest X Ray reports, and history
of precipitating insults, if present.
The frequency of various factors distinguishing myxedema coma from hypothyroidism
without coma or non-thyroidal causes of coma was assessed and weighted to further develop a
diagnostic point scale in order to enable a semiquantitative distinction between uncomplicated
hypothyroidism, severe hypothyroidism and myxedema coma. The potential utility of the
diagnostic scoring system was assessed by application to selected patients reported in the
literature.
Statistical analysis
Microsoft excel spreadsheet software was used to note the frequency of clinical events.
Baseline characteristics between the two groups (MC vs. non-MC) were compared by using
Fisher’s exact test for categorical variables and two sample t-test for continuous variables. A
p- value of <0.05 was considered to be statistically significant. Logistic regression analysis
was used to test the predictive power of the score for myxedema coma. Results were
expressed using odds ratio and 95% confidence interval. Further, receiver operating
characteristic (ROC) curve analysis was performed to test the discriminative power of the
score. The discriminative power was measured by using area under ROC curve. Sensitivities
and specificities were calculated for all values of the score and the cutoff point was identified
with left topmost point on ROC curve (representing the highest sensitivity and specificity).
Statistical analyses were performed in SAS 9.3, SAS Institute Inc., Cary, NC, USA.
The study protocol was approved by the Institutional Review Boards of MWHC and VAMC.
Results
Page 8
DOI:10.4158/EP13460.OR © 2013 AACE.
Chart review identified twenty one patients who had been diagnosed with myxedema coma by
an endocrinologist. We re-classified seven patients as non-myxedema coma (non-MC) as we
believed they were misdiagnosed with myxedema coma, and we used them as a control group
(Table 3). Reasons for re-classification included normal free T4 levels and only marginally
elevated serum TSH (patients 1, 2, 4, 7), or absence of any degree of mental status changes
(patients 3, 5 and 6), since mental status alteration was a criteria historically used to diagnose
myxedema coma in patients with hypothyroidism.
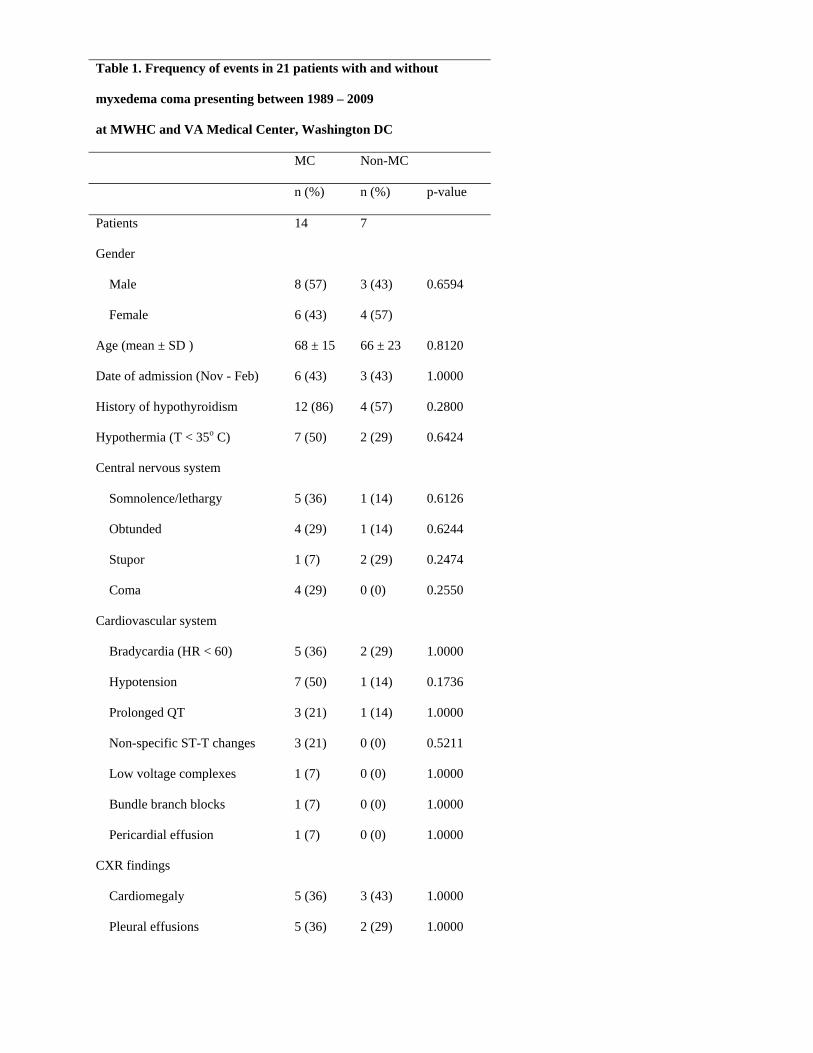
The frequency of demographics and clinical characteristics of the patients in each group is
presented in Table 1 and a summary of the patients clinical characteristics is detailed in Tables
2 and 3 (page 1 and 2). As noted in Table 1, there were no statistical significant differences
between the two groups in terms of patient clinical characteristics, to distinguish patients with
myxedema coma, from those with other forms of hypothyroidism. The age (mean ± SD) at
presentation was 68 ± 15 years in MC group vs. 66 ± 23 years in non-MC group (p = 0.81),
with 57% of men in MC group vs. 43% in non-MC group (p = 0.66). The distribution of the
neurological alterations in MC group was relatively similar throughout the entire spectrum of
neurocognitive dysfunction, with 36% of the patients described as somnolent or lethargic, and
with coma being present in 29% of the subjects (Table 1).The most common clinical
manifestations in MC patients were hypothermia (50% in MC vs. 29% in non-MC, p = 0.64)
and hypotension (50% in MC vs. 14% in non-MC, p = 0.17). A wide spectrum of EKG
alterations was noted in patients with MC, with bradycardia present in 36% of the cases.
Myxedema coma patients had more frequent and wider distribution of EKG alterations,
metabolic disturbances and gastrointestinal manifestations, than non-MC patients, although
Page 9
DOI:10.4158/EP13460.OR © 2013 AACE.
none reaching statistical significance (Table 1). Each patient was noted to have had one or
more identifiable precipitating events.
Based on the above findings, we constructed a diagnostic scoring system to enable a
semiquantitative distinction between uncomplicated hypothyroidism, severe hypothyroidism
and myxedema coma (Table 4). The lack of statistically significant difference between all the
clinical characteristics of the two groups, combined with the wide and relatively similar
distribution of events in each category led to the construction of a comprehensive
multisystemic diagnostic scale, in which points were assigned using a stratified approach
based on the severity of each condition in a particular system. The highest weighted
description applicable in each category was considered and scores were totalled. When a
given descriptive characteristic was encountered in more than one category (i.e., precipitating
event and metabolic disturbance), the condition was counted once.
When applied to the fourteen patients with MC, a score of 60 or higher (60 - 120) was
calculated to be diagnostic of myxedema coma (Table 2, page 2). Six of the seven patients
with non-MC had scores ranging between 25 and 50 (Table 3, page 2). A single patient from
this latter cohort had a score of 110, but he was excluded because of a normal free T4 of 1.14
ng/dL and an only mild TSH elevation.
Logistic regression univariate analysis identified the score as a continuum to be predictive of
the outcome with an odds ratio of 1.09 per unit of the score (95% CI, 1.01-1.16; p =0.019). A
score of 45 predicted coma with a probability of 0.27 and an odds ratio of 0.37, respectively,
Page 10
DOI:10.4158/EP13460.OR © 2013 AACE.
whereas a score of 60 had a predictive probability of 0.55, with an odds ratio of 1.22. The
model overall was significant (Chi-square test p-value = 0.0006).
The area under the ROC curve of the prediction score was 0.88 (95% CI, 0.65 – 1.00) (Fig 1).
The cutoff point on ROC curve corresponded to the score of 60, which had the highest
sensitivity (100%) and specificity (85.71%), with a positive likelihood ratio of 7.0 and
negative likelihood ratio of 0.0. The score of 45 had 100% sensitivity, but a lower specificity
of 42.86%, whereas a score of less than 25 had 0% specificity (Fig 1).
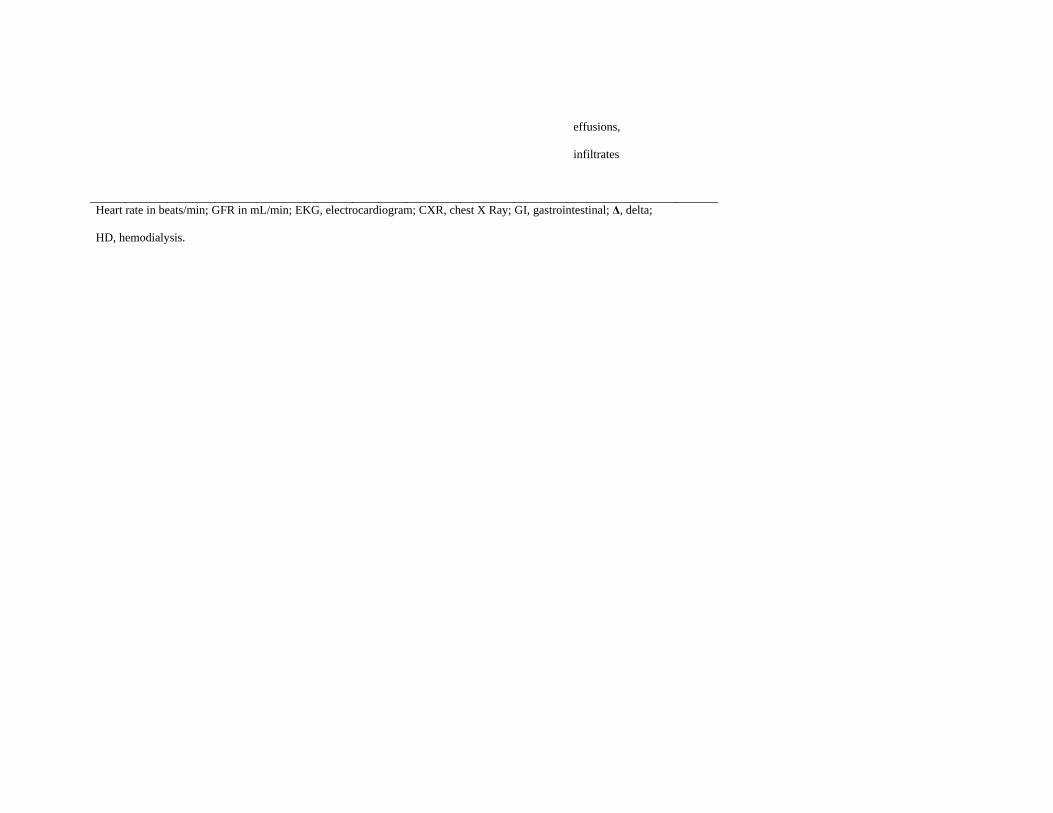
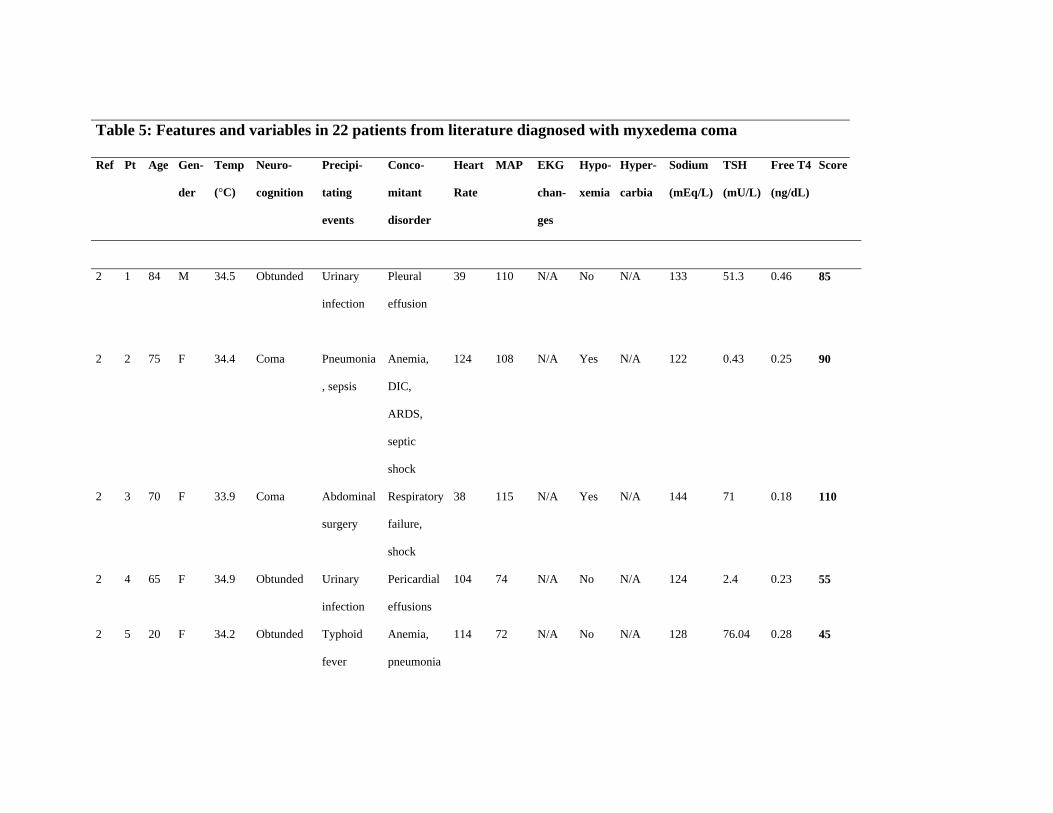
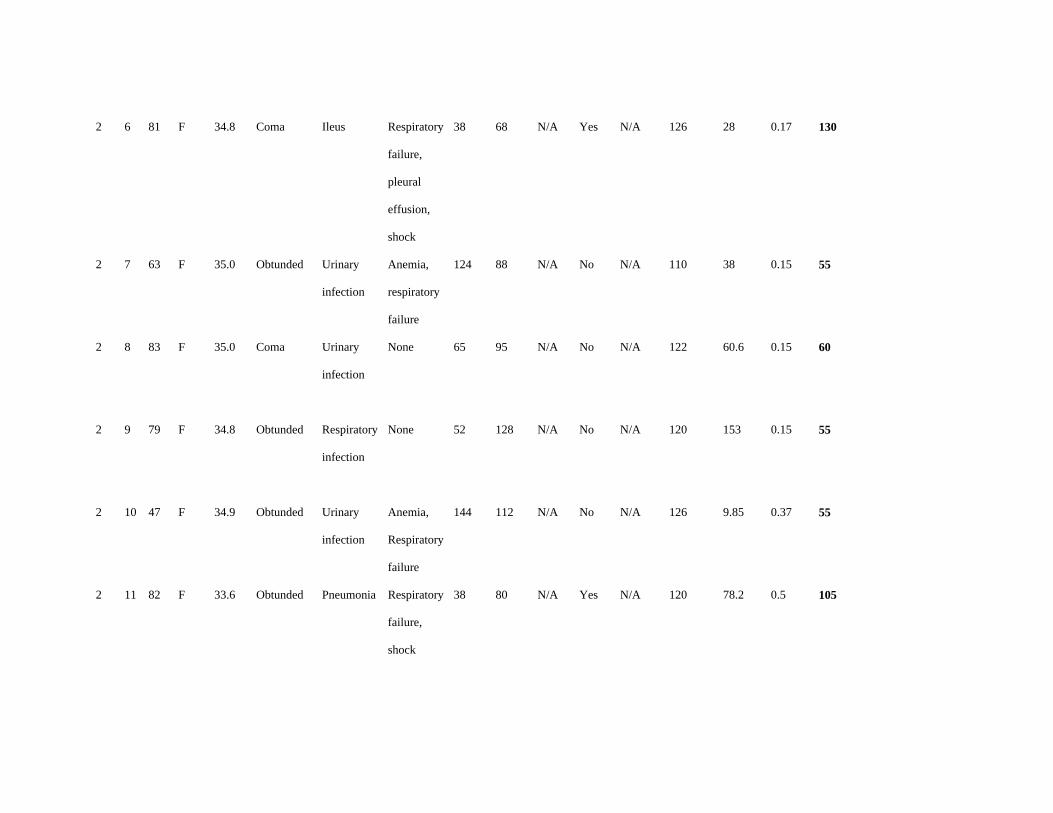
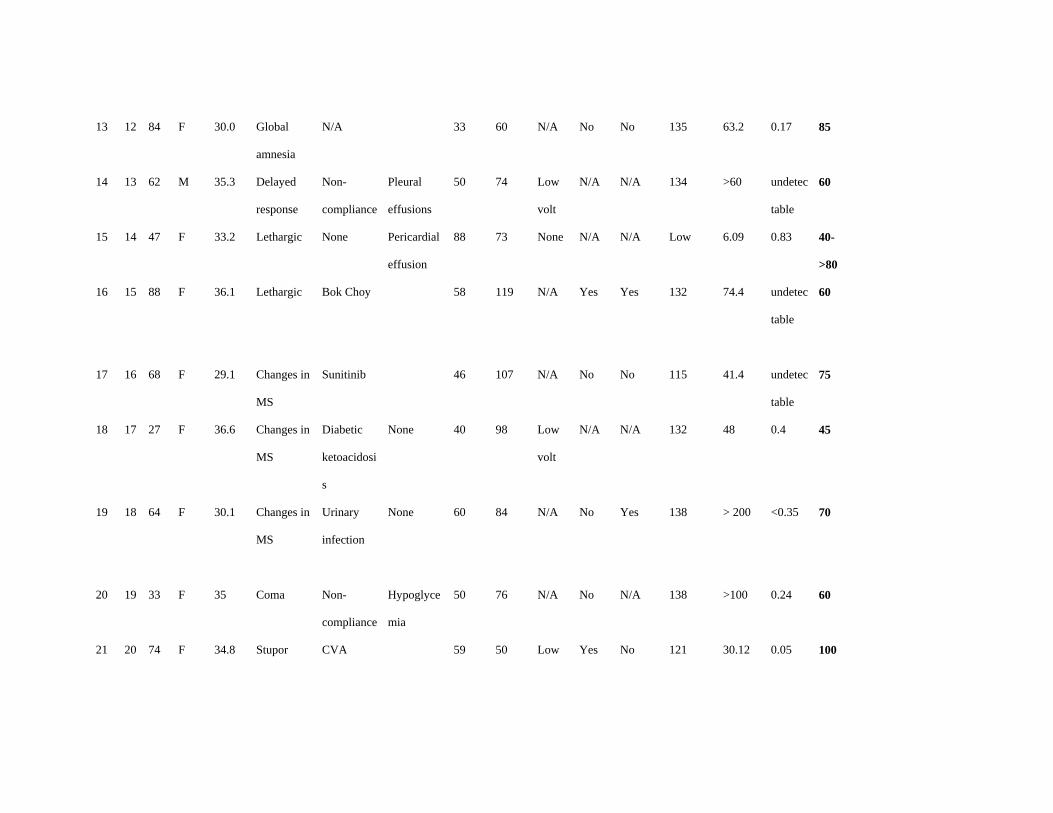
When applied to patients in the literature for whom enough clinical data were available, the
diagnostic scoring system identified 16 out of 22 patients as having myxedema coma (score ≥
60) (Table 5). The remaining six patients would have been classified as being at risk for
myxedema coma (scores ranged between 45 - 55), but did not quite meet the criteria for a
diagnosis of myxedema coma. None of the twenty two patients had scores at presentation that
qualified them as unlikely to have myxedema coma.
Discussion
Although it is generally accepted that the diagnosis of myxedema coma should rely on some
degree of mental status alteration, impaired thermoregulatory response and the presence of a
precipitating event [6], clear cut diagnostic criteria to define myxedema coma have not been
established. Moreover, uncertainty of diagnosis is suggested by the numerous hypothyroid
patients with presumed myxedema coma reported in the literature in whom at least one of
these features was minor or absent.
Page 11
DOI:10.4158/EP13460.OR © 2013 AACE.
Although altered mental status was a prominent aspect of the presenting clinical picture in all
our patients, it would be tenuous to base a diagnosis on this alone. There may be innumerable
etiologies for mental status change, but it is through combination with other signs and
symptoms of our scoring system, along with thyroid function test results, that the mental
status changes allow a more precise focus on the diagnosis of myxedema coma.
To our knowledge, there have been no previous reports of clinical algorithms to define
diagnostic criteria for myxedema coma, likely due to the paucity of cases and consequent
lack of studies to address this issue. Accordingly, we have developed a diagnostic scoring
system for myxedema coma, and assessed its potential utility in a cohort of patients from our
two institutions, as well as applying it to selected patients identified in the literature [2, 13-
23]. Our hope is that this scoring system will enable earlier diagnosis and treatment of
patients with myxedema coma.
Importantly, most of the patients whom we evaluated from the literature were likely
“underscored” due to limited clinical data availability. Thus, an assigned score of 60 could
easily have been achieved with one or two more variables being present, such as the lacking
details of metabolic abnormalities, EKG changes, and/or gastrointestinal manifestations.
Patient 14 [Table 5] [15] was of particular interest, as she initially presented to the hospital
with biochemical evidence of subclinical hypothyroidism, and clinical features that would not
have diagnosed her with myxedema coma, given a score of 40. Shortly after admission, her
clinical status deteriorated and she was diagnosed with myxedema coma, achieving a score of
80, based on our diagnostic scale. Of note, the patient’s biochemical markers continued to
reflect a state of subclinical hypothyroidism throughout her hospitalization, showing that a
reliance on thyroid function tests alone could have potentially missed the development of
Page 12
DOI:10.4158/EP13460.OR © 2013 AACE.
myxedema coma, thereby delaying diagnosis and treatment of this patient.
The predictive power of the score as a continuum showed an odds ratio of 1.09 (95% CI, 1.01-
1.16; p =0.019) suggesting that with each unit increase in the score within the range of
available data, the odds of myxedema coma increases by a factor of 1.09, or by 9%. For
instance, a change in score from 50 to 51 would change the predictive probability of coma
from 0.35 to 0.37, or from odds ratio of 0.54 to odds ratio of 0.58. The score of 60 represented
a turning point and predicted coma with a high accuracy, given its predicted probability of
0.55, which conferred an odds ratio of 1.22. The odds of coma for a score of 45 was
approximately 1/3 (0.37), which corresponded to a predicted probability of 0.27.
The discriminative power of the scoring system was high, with area under the ROC curve of
0.88 (95% CI, 0.65 – 1.00). The score of 60 had the highest sensitivity (100%), and specificity
(85.71%) of the scores calculated which makes it a good screening tool given the highest
sensitivity and the relatively high specificity. The score of 45 had 100% sensitivity, but a
lower specificity of 42.86%. Given the above considerations, we propose that with application
of the recommended scoring system, a score of 60 or higher will be highly suggestive of
myxedema coma, a score between 45 and 59 will represent risk for myxedema coma, and that
a score of less than 45 is unlikely to indicate myxedema coma. Given the small sample size,
our model was not capable of producing a threshold score for patients at risk for myxedema
coma, therefore the scores between 45-59 are only our suggestion of representing patients in
this category, based on the given probabilities.
Neurocognitive dysfunction in patients with myxedema coma may vary from disorientation
Page 13
DOI:10.4158/EP13460.OR © 2013 AACE.
and lethargy to slow mentation, confusion, cognitive dysfunction, minimal responsiveness, or
coma. The decompensated neurologic state may be primary, such as from a cerebrovascular
event or due to a drug overdose with sedatives or hypnotics; whereas sepsis, hyponatremia, or
other metabolic disturbances are secondary events, which may worsen the cognitive function.
Homeostatic dysfunction resulting from thyroid hormone deficiency is generally insufficient
to cause myxedema coma, as the body can compensate through neurovascular mechanisms. A
triggering event is usually required to overcome the compensatory mechanisms in a
hypothyroid patient. [7] Infection, cerebrovascular or cardiovascular events, cold temperature
exposure, medications such as amiodarone, beta blockers, lithium, narcotics, sedatives,
diuretics, and metabolic derangements are several examples of such insults. [2, 3] Each
patient had at least one identifiable precipitating event and the frequency of these events was
in concordance with the findings reported in other studies. [3]
Prolonged untreated hypothyroidism coupled with a triggering event may lead to
cardiovascular collapse and shock which may not be responsive to vasopressor therapy alone,
until thyroid hormone also is administered [8]. Electrocardiographic abnormalities such as
bradycardia, low voltage, nonspecific ST wave inversion, QT prolongation, as well as rhythm
abormalities may be seen [9]. Hypotension was commonly seen in our myxedema coma cases,
and the frequency of electrocardiographic abnormalities was similar to that reported in the
literature [3].
Page 14
DOI:10.4158/EP13460.OR © 2013 AACE.
An impaired ventilatory response and a need for mechanical ventilation are common
manifestations in patients with myxedema coma. Decreased respiratory center sensitivity to
hypercarbia and hypoxemia may lead to hypoventilation, which may be aggravated further by
impaired respiratory muscle function, obesity, and other obstructive processes of the airway
such as macroglossia, myxedema of the larynx and nasopharynx, intrinsic processes such as
pneumonia, reduced lung volumes, or extrinsic compressive processes such as pleural
effusions [1, 10, 11].
Reduced glomerular filtration rate (GFR) in hypothyroid patients is a result of decreased renal
plasma flow withwater retention and hyponatremia usually being concomitant findings in
these patients [12]. Fluid extravasation, resulting from altered vascular permeability, may
present as effusions, nonpitting edema and anasarca. Effects of profound thyroid hormone
deficiency on the gastrointestinal system may include decreased intestinal motility with
constipation and may progress to paralytic ileus with a quiet and distended abdomen,
anorexia, nausea and abdominal pain [23]. In our patients, the metabolic abnormalities
occurred with relative equal frequencies but independent of each other, suggesting the
importance of appreciation of the multisystemic basis for development of myxedema coma.
The ultimate diagnosis of myxedema coma should be made with biochemical evidence of low
levels of serum free T4 and T3, and elevated TSH in patients with primary hypothyroidism,
whereas in secondary hypothyroidism the biochemical diagnosis should rely on low, or
normal TSH, and low free T4 and total T3 hormone levels and evidence of pituitary
dysfunction. None of our patients had biochemical evidence of secondary hypothyroidism.
Page 15
DOI:10.4158/EP13460.OR © 2013 AACE.
Particular attention should be given to patients with biochemical evidence of secondary
hypothyroidism that could be difficult to distinguish from the “sick euthyroid” state. The latter
entity represents a physiologic adaptive response of the thyrotropic feedback control to severe
illness, and is reflected by biochemical evidence of normal, low, or slightly elevated TSH,
depending of the severity of the illness, and low free T4 and T3. Therefore, in order to avoid
misclassifying patients with “sick euthyroid” syndrome as having myxedema coma in the
setting of commonly present multiorgan dysfunction, we suggest that appropriate diagnosis of
secondary hypothyroidism should be done first, either from history of hypothalamic-pituitary
dysfunction, or through imaging studies reflecting organic hypothalamic, or pituitary disease.
This study is limited by virtue of its retrospective design and relatively small sample size,
which precluded accurate comparison between groups due to lack of statistical power. Also,
due to insufficient published data in all the case reports of myxedema coma assessed from
literature, it was not possible to fully validate the scoring system. However, the score
demonstrated to have positive predictive value and a high discriminative power.
In conclusion, considering the complex, multisystemic manifestations of hypothyroidism in
patients with myxedema coma and the high mortality associated with delays in therapy, a
practical guide to earlier diagnosis could be of value. We propose a diagnostic scoring system
for myxedema coma based upon data from restrospective cases diagnosed at our institutions,
as well as from selected case reports culled from the literature. This scoring system assessed
an array of the diagnostic features associated with myxedema coma and found a similar
frequency of findings in our cohort of patients as in those assessed from the literature [2, 3, 5].
Page 16
DOI:10.4158/EP13460.OR © 2013 AACE.
This scoring system should be considered in the clinical context of the patient. Further large
prospective, well controlled studies are needed to confirm the current findings, and to inform
whether such a diagnostic approach to patients with myxedema coma will enable earlier
recognition and more effective treatment of this potentially fatal endocrine emergency.
Disclosure Summary: The authors have nothing to disclose.
References:
1. Klubo-Gwiezdzinska J, Wartofsky L. Thyroid emergencies. Endocrinol Metab Clin
North Am. 2012; 96:385-403.
2. Rodriguez I, Fluiters E, Pérez-Méndez LF, Luna R, Páramo C, García-Mayor RV.
Factors associated with mortality of patients with myxoedema coma: prospective study in
11 cases treated in a single institution. J Endocrinol. 2004;180:347-350.
3. Dutta P, Bhansali A, Masoodi SR, Bhadada S, Sharma N, Rajput R. Predictors of
outcome in myxoedema coma: a study from a tertiary care center. Crit Care. 2008; 12:R1
4. Jordan RM. Myxedema coma. Pathophysiology, therapy, and factors affecting
prognosis. Med Clin North Am. 1995;79:185-194
5. Yamamoto T, Fukuyama J, Fujiyoshi A. Factors associated with mortality of
myxedema coma: report of eight cases and literature survey. Thyroid. 1999; 9:1167-1174
6. Nicoloff JT. Thyroid storm and myxedema coma. Med Clin North Am. 1985;69:1005-
1017
Page 17
DOI:10.4158/EP13460.OR © 2013 AACE.
7. Fliers E, Wiersinga WM. Myxedema coma. Rev Endocr Metab Disord. 2003;4:137-141
8. Gardner DG. “Endocrine emergencies”, in D.G. Gardner and D. Shoback, eds.
Greenspan’s Basic and Clinical Endocrinology, McGraw-Hill, New York, NY, USA, 8th
edition, 2007.
9. Polikar R, Burger AG, Scherrer U, Nicod P. The thyroid and heart. Circulation. 1993;
87:1435-1441
10. Zwillich CW, Pierson DJ, Hofeldt FD, Lufkin EG, Weil JV. Ventilatory control in
myxedema and hypothyroidism. N Engl J Med. 1975;292:662-665
11. Ladenson PW, Goldenheim PD, Ridgway EC. Prediction and reversal of blunted
ventilatory responsiveness in patients with hypothyroidism. Am J Med. 1988;84:877-883
12. Montenegro J, Gonzalez O, Saracho R, Aguirre R, Martinez I. Changes in renal
function in primary hypothyroidism. Am J Kidney Dis. 1996;27:195-198
13. Kogan A, Kassif Y, Shadel M, Shwarz Y, Lavee J, Or J, Raanani E. Severe
hypothermia in myxoedema coma: a rewarming by extracorporeal circulation. Emerg
Med Australas. 2011; 23:773-775
14. G Pearse S, D Dahdal M, Grocott-Mason R, W Dubrey S. Myxoedematous pre-coma
and heart failure. Br J Hosp Med (Lond). 2011;72:52-53
15. Mallipedhi A, Vali H, Okosieme O. Myxedema coma in a patient with subclinical
hypothyroidism. Thyroid. 2011;21:87-89
16. Chu M, Seltzer TF. Myxedema coma induced by ingestion of raw bok choy. N Engl J
Med. 2010; 362:1945-1946
17. Chen SY, Kao PC, Lin ZZ, Chiang WC, Fang CC. Sunitinib-induced myxedema
coma. Am J Emerg Med. 2009;27:370.e1-370.e3
Page 18
DOI:10.4158/EP13460.OR © 2013 AACE.
18. Cappelli C, Stanga B, Paini A, Gandossi E, Cumetti D, Castellano M, et al.
Myxoedema coma precipitated by diabetic ketoacidosis and neuroleptic drugs: case
report in an intensive care unit. Intern Emerg Med. 2007;2:147-149
19. Sheu CC, Cheng MH, Tsai JR, Hwang JJ. Myxedema coma: a well-known but
unfamiliar medical emergency. Thyroid. 2007;17:371-372
20. Yu CH, Stovel R, Fox S. Chorea--an unusual manifestation in a woman recovering from
myxedema coma. Endocr Pract. 2012;18:e43-e48
21. Ahn JY, Kwon HS, Ahn HC, Sohn YD. A case of myxedema coma presenting as a
brain stem infarct in a 74-year-old Korean woman. J Korean Med Sci. 2010;25:1394-
1397
22. Kargili A, Turgut FH, Karakurt F, Kasapoglu B, Kanbay M, Akcay A. A forgotten
but important risk factor for severe hyponatremia: myxedema coma. Clinics (Sao Paulo).
2010; 65:447-448
23. Yanamandra U, Kotwal N, Menon A, Nair V. Ogilvie’s syndrome in a case of
myxedema coma. Indian J. Endocrinol Metab. 2012;16:447-449
Page 19
Table 1. Frequency of events in 21 patients with and without
myxedema coma presenting between 1989 – 2009
at MWHC and VA Medical Center, Washington DC
MC Non-MC
n (%) n (%) p-value
Patients 14 7
Gender
Male 8 (57) 3 (43) 0.6594
Female 6 (43) 4 (57)
Age (mean ± SD ) 68 ± 15 66 ± 23 0.8120
Date of admission (Nov - Feb) 6 (43) 3 (43) 1.0000
History of hypothyroidism 12 (86) 4 (57) 0.2800
Hypothermia (T < 35o C) 7 (50) 2 (29) 0.6424
Central nervous system
Somnolence/lethargy 5 (36) 1 (14) 0.6126
Obtunded 4 (29) 1 (14) 0.6244
Stupor 1 (7) 2 (29) 0.2474
Coma 4 (29) 0 (0) 0.2550
Cardiovascular system
Bradycardia (HR < 60) 5 (36) 2 (29) 1.0000
Hypotension 7 (50) 1 (14) 0.1736
Prolonged QT 3 (21) 1 (14) 1.0000
Non-specific ST-T changes 3 (21) 0 (0) 0.5211
Low voltage complexes 1 (7) 0 (0) 1.0000
Bundle branch blocks 1 (7) 0 (0) 1.0000
Pericardial effusion 1 (7) 0 (0) 1.0000
CXR findings
Cardiomegaly 5 (36) 3 (43) 1.0000
Pleural effusions 5 (36) 2 (29) 1.0000
Page 20
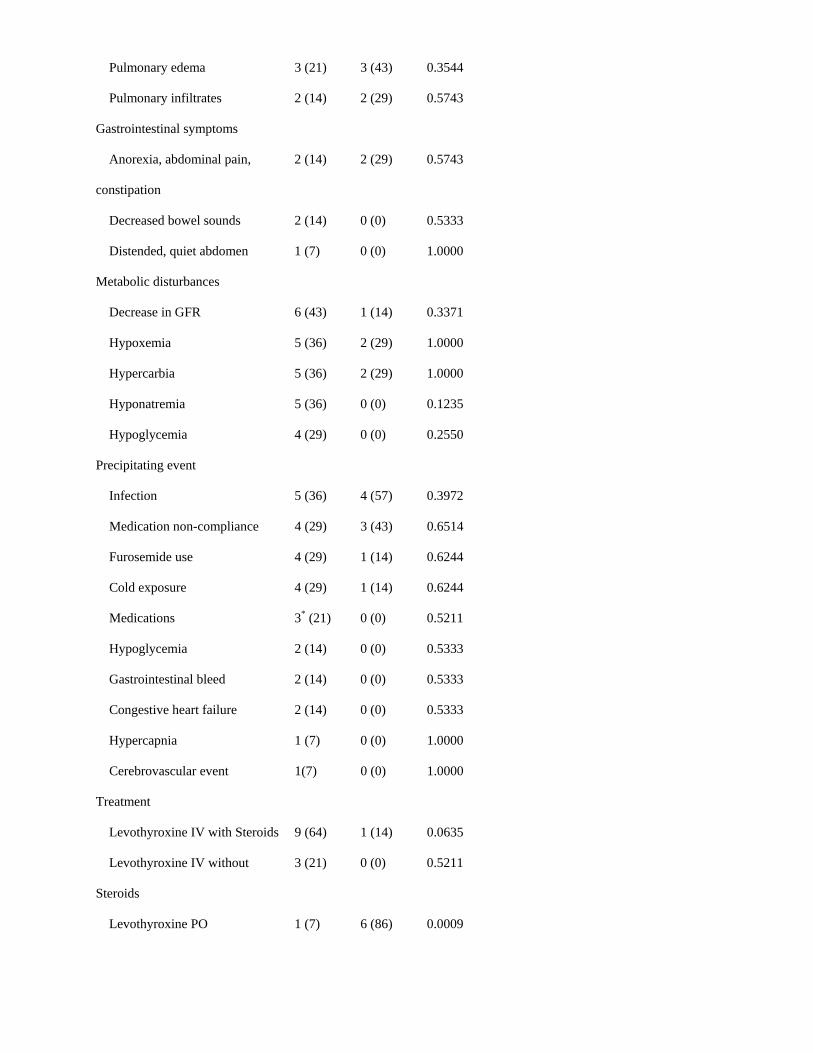
Pulmonary edema 3 (21) 3 (43) 0.3544
Pulmonary infiltrates 2 (14) 2 (29) 0.5743
Gastrointestinal symptoms
Anorexia, abdominal pain,
constipation
2 (14) 2 (29) 0.5743
Decreased bowel sounds 2 (14) 0 (0) 0.5333
Distended, quiet abdomen 1 (7) 0 (0) 1.0000
Metabolic disturbances
Decrease in GFR 6 (43) 1 (14) 0.3371
Hypoxemia 5 (36) 2 (29) 1.0000
Hypercarbia 5 (36) 2 (29) 1.0000
Hyponatremia 5 (36) 0 (0) 0.1235
Hypoglycemia 4 (29) 0 (0) 0.2550
Precipitating event
Infection 5 (36) 4 (57) 0.3972
Medication non-compliance 4 (29) 3 (43) 0.6514
Furosemide use 4 (29) 1 (14) 0.6244
Cold exposure 4 (29) 1 (14) 0.6244
Medications 3* (21) 0 (0) 0.5211
Hypoglycemia 2 (14) 0 (0) 0.5333
Gastrointestinal bleed 2 (14) 0 (0) 0.5333
Congestive heart failure 2 (14) 0 (0) 0.5333
Hypercapnia 1 (7) 0 (0) 1.0000
Cerebrovascular event 1(7) 0 (0) 1.0000
Treatment
Levothyroxine IV with Steroids 9 (64) 1 (14) 0.0635
Levothyroxine IV without
Steroids
3 (21) 0 (0) 0.5211
Levothyroxine PO 1 (7) 6 (86) 0.0009
Page 21
*Amiodarone (n=2), Amitriptyline (n=1)
SD, standard deviation; T, temperature; HR, heart rate; CXR, chest X Ray; GFR, glomerular
filtration rate.
Page 22
Table 2: Features and variables in 14 patients with myxedema coma (page 1/2)
Pa-
tient
Age Gen-
der
History
of hypo-
thyro-
idism
Cold
season
(Nov-
Feb)
Tempera
-ture (°C)
Neuro-
cognition
Precipitating
events
TSH
(mU/L)
Free T4
(ng/dL)
Total T3
(ng/dL)
1 49 M Yes Yes 33.3 Obtunded Hypoglycemia
Cold exposure
53.4 0.68 50.6
2 67 F Yes No 36.4 Coma Infection (PNA)
Hypercarbia
28.6 0.59 56.3
3 84 M Yes No 33.6 Coma Infection (UTI)
GI bleed
125 < 0.3
4 41 F Yes No 36.4 Lethargic Amitriptyline 122 0.56
5 76 M No Yes 36.2 Obtunded Infection (UTI)
Amiodarone
Cold exposure
170 0.49 66.3
6 82 F Yes No 36.3 Lethargic Infection (UTI) 71 < 0.2 < 40
7 67 F Yes Yes 36.3 Obtunded Hypoglycemia 326 0.39 < 40
8 49 F Yes Yes 37 Lethargic GI bleed
Furosemide
57 0.42 < 40
9 74 M Yes Yes 34.4 Coma Amiodarone 45 0.2
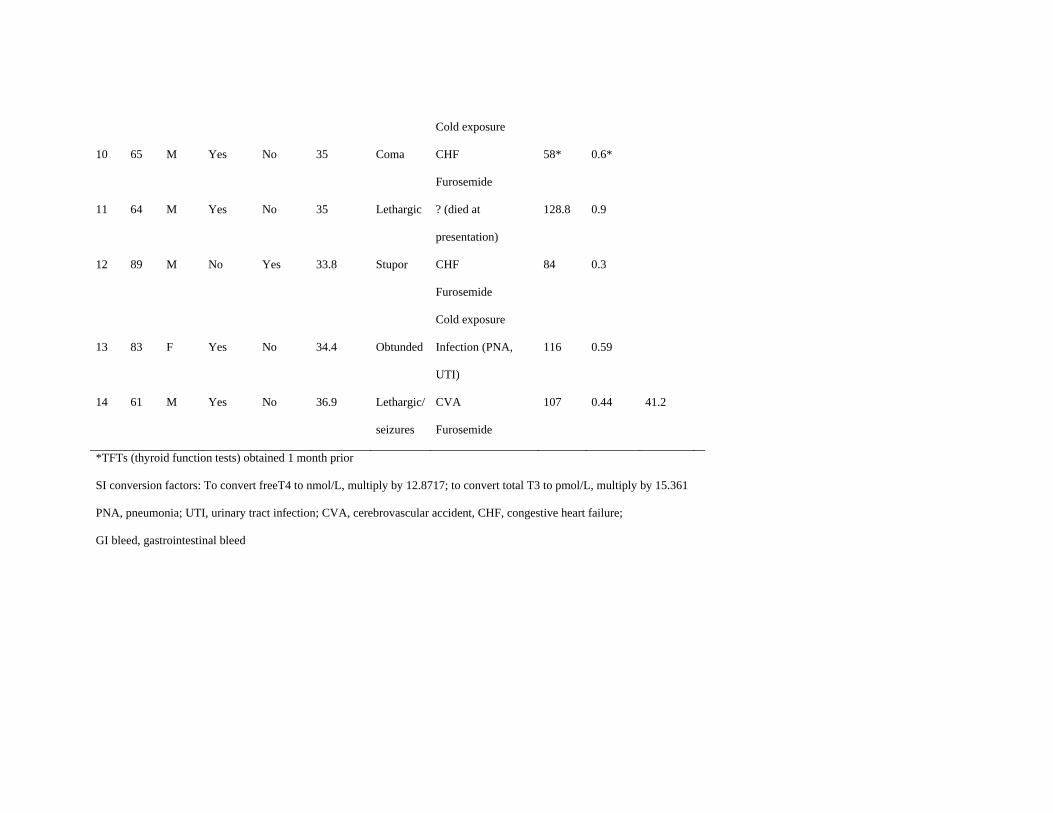
Page 23
Cold exposure
10 65 M Yes No 35 Coma CHF
Furosemide
58* 0.6*
11 64 M Yes No 35 Lethargic ? (died at
presentation)
128.8 0.9
12 89 M No Yes 33.8 Stupor CHF
Furosemide
Cold exposure
84 0.3
13 83 F Yes No 34.4 Obtunded Infection (PNA,
UTI)
116 0.59
14 61 M Yes No 36.9 Lethargic/
seizures
CVA
Furosemide
107 0.44 41.2
*TFTs (thyroid function tests) obtained 1 month prior
SI conversion factors: To convert freeT4 to nmol/L, multiply by 12.8717; to convert total T3 to pmol/L, multiply by 15.361
PNA, pneumonia; UTI, urinary tract infection; CVA, cerebrovascular accident, CHF, congestive heart failure;
GI bleed, gastrointestinal bleed
Page 24
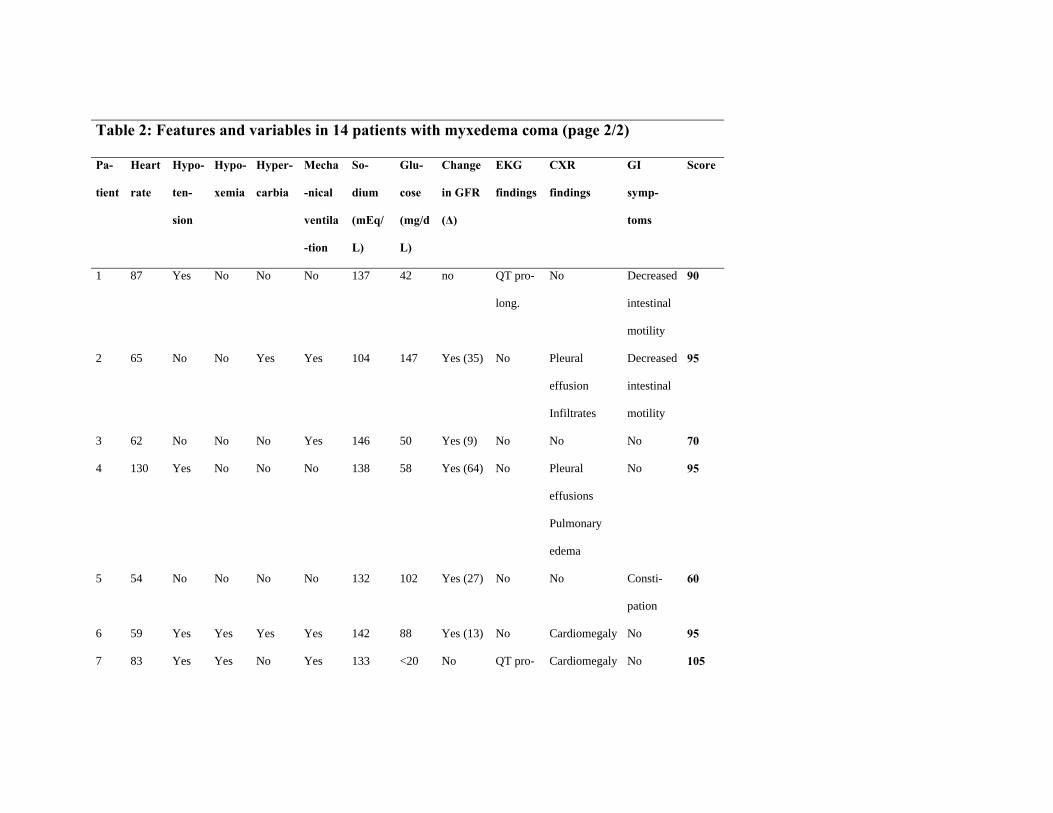
Table 2: Features and variables in 14 patients with myxedema coma (page 2/2)
Pa-
tient
Heart
rate
Hypo-
ten-
sion
Hypo-
xemia
Hyper-
carbia
Mecha
-nical
ventila
-tion
So-
dium
(mEq/
L)
Glu-
cose
(mg/d
L)
Change
in GFR
(Δ)
EKG
findings
CXR
findings
GI
symp-
toms
Score
1 87 Yes No
No No 137 42 no QT pro-
long.
No Decreased
intestinal
motility
90
2 65 No No Yes Yes 104 147 Yes (35) No Pleural
effusion
Infiltrates
Decreased
intestinal
motility
95
3 62 No No No Yes 146 50 Yes (9) No No No 70
4 130 Yes No No No 138 58 Yes (64) No Pleural
effusions
Pulmonary
edema
No 95
5 54 No No No No 132 102 Yes (27) No No Consti-
pation
60
6 59 Yes Yes Yes Yes 142 88 Yes (13) No Cardiomegaly No 95
7 83 Yes Yes No Yes 133 <20 No QT pro- Cardiomegaly No 105
Page 25
long. Pulmonary
edema
8 61 No No No No 133 81 Yes (19) No Cardiomegaly
Pleural
effusions
No 65
9 70 Yes Yes No No 135 109 N/A No cardiomegaly Abdomin
al pain
100
10 56 No No No Yes 136 135 N/A No No Ileus 90
11 46 Yes No No Yes 133 71 N/A No No No 80
12 61 No No Yes No 156 128 N/A No Pleural
effusions
No 60
13 67 Yes Yes Yes Yes 145 175 Yes (15) QT pro-
long.
Pleural
effusions
Pulmonary
edema
Infiltrates
No 120
14 56 No No No No 138 145 No No Cardiomegaly No 75
GFR, glomerular filtration rate; CXR, chest X Ray
Heart rate in beats/min; GFR in mL/min.
Page 27
Table 3: Features and variables in 7 patients without myxedema coma (page 1/2)
Pa-
tient
Age Gen-
der
History
of hypo-
thyro-
idism
Cold
season
(Nov-
Feb)
Tempe
-rature
(°C)
Neuro-
cognitio
n
Precipitating
events
TSH
(mU/L)
Free T4
(ng/dL)
Total T3
(ng/dL)
1 32 M No Yes 31.3 Lethargic Infecion
(bacteremia)
5.67 0.62 56.2
2 73 M No No 36.8 Stupor Infection (PNA) 5.83 1.06
3 52 F Yes Yes 37 Normal Non-compliance 80.6 0.39
4 77 F Yes No 37 Obtunded Non-compliance 9.0 1.3
5 94 F Yes No 36.6 Normal Infection (UTI) 7.2 2.03
6 45 F Yes No 36.6 Normal Non-compliance 145 0.28
7 90 M No Yes 34.4 Stupor Infection (PNA)
Cold exposure
Furosemide
11.9 1.4 70.8
PNA, pneumonia; UTI, urinary tract infection
Page 28
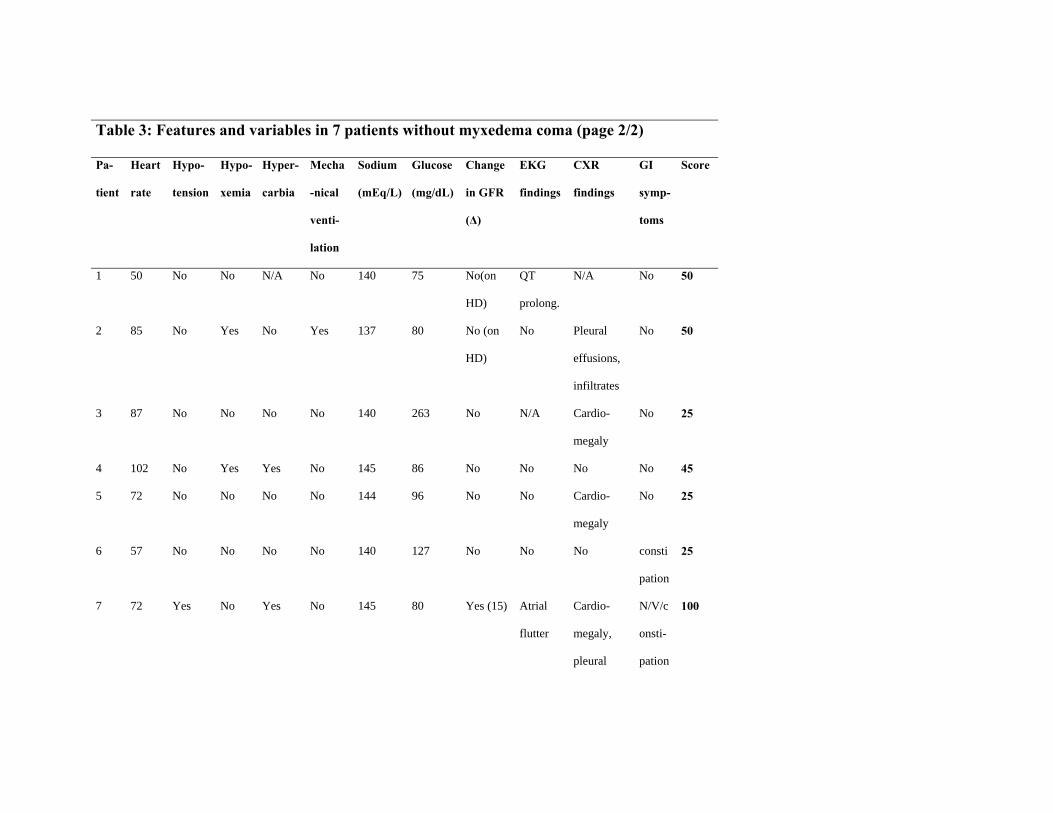
Table 3: Features and variables in 7 patients without myxedema coma (page 2/2)
Pa-
tient
Heart
rate
Hypo-
tension
Hypo-
xemia
Hyper-
carbia
Mecha
-nical
venti-
lation
Sodium
(mEq/L)
Glucose
(mg/dL)
Change
in GFR
(Δ)
EKG
findings
CXR
findings
GI
symp-
toms
Score
1 50 No No N/A No 140 75 No(on
HD)
QT
prolong.
N/A No 50
2 85 No Yes No Yes 137 80 No (on
HD)
No Pleural
effusions,
infiltrates
No 50
3 87 No No No No 140 263 No N/A Cardio-
megaly
No 25
4 102 No Yes Yes No 145 86 No No No No 45
5 72 No No No No 144 96 No No Cardio-
megaly
No 25
6 57 No No No No 140 127 No No No consti
pation
25
7 72 Yes No Yes No 145 80 Yes (15) Atrial
flutter
Cardio-
megaly,
pleural
N/V/c
onsti-
pation
100
Page 29
effusions,
infiltrates
Heart rate in beats/min; GFR in mL/min; EKG, electrocardiogram; CXR, chest X Ray; GI, gastrointestinal; Δ, delta;
HD, hemodialysis.
Page 31
Table 4. Diagnostic Scoring System for Myxedema Coma
Termoregulatory dysfunction (Temperature, oC) Cardiovascular dysfunction
>35 0 Bradycardia
32-35 10 Absent 0
<32 20 50-59 10
Central Nervous System Effects 40-49 20
Absent 0 <40 30
Somnolent/Lethargy 10 Other EKG changes* 10
Obtunded 15 Pericardial/pleural effusions 10
Stupor 20 Pulmonary edema 15
Coma/Seizures 30 Cardiomegaly 15
Gatrointestinal findings Hypotension 20
Anorexia/abdominal pain/constipation 5 Metabolic disturbances
Decreased intestinal motility 15 Hyponatremia 10
Paralytic ileus 20 Hypoglycemia 10
Precipitating event Hypoxemia 10
Absent 0 Hypercarbia 10
Present 10 Decrease in GFR 10
*Other EKG changes: QT prolongation, or low voltage complexes, or bundle branch blocks, or non-specific ST-T
changes, or heart blocks.
A score of 60 or higher is highly suggestive/diagnostic of myxedema coma; a score of 25 -59 is suggestive of risk
for myxedema coma, and a score below 25 is unlikely to represent myxedema coma.
Page 32
Table 5: Features and variables in 22 patients from literature diagnosed with myxedema coma
Ref Pt Age Gen-
der
Temp
(°C)
Neuro-
cognition
Precipi-
tating
events
Conco-
mitant
disorder
Heart
Rate
MAP EKG
chan-
ges
Hypo-
xemia
Hyper-
carbia
Sodium
(mEq/L)
TSH
(mU/L)
Free T4
(ng/dL)
Score
2 1 84 M 34.5 Obtunded Urinary
infection
Pleural
effusion
39 110 N/A No N/A 133 51.3 0.46 85
2 2 75 F 34.4 Coma Pneumonia
, sepsis
Anemia,
DIC,
ARDS,
septic
shock
124 108 N/A Yes N/A 122 0.43 0.25 90
2 3 70 F 33.9 Coma Abdominal
surgery
Respiratory
failure,
shock
38 115 N/A Yes N/A 144 71 0.18 110
2 4 65 F 34.9 Obtunded Urinary
infection
Pericardial
effusions
104 74 N/A No N/A 124 2.4 0.23 55
2 5 20 F 34.2 Obtunded Typhoid
fever
Anemia,
pneumonia
114 72 N/A No N/A 128 76.04 0.28 45
Page 33
2 6 81 F 34.8 Coma Ileus Respiratory
failure,
pleural
effusion,
shock
38 68 N/A Yes N/A 126 28 0.17 130
2 7 63 F 35.0 Obtunded Urinary
infection
Anemia,
respiratory
failure
124 88 N/A No N/A 110
38 0.15 55
2 8 83 F 35.0 Coma Urinary
infection
None 65 95 N/A No N/A 122 60.6 0.15 60
2 9 79 F 34.8 Obtunded Respiratory
infection
None 52 128 N/A No N/A 120 153 0.15 55
2 10 47 F 34.9 Obtunded Urinary
infection
Anemia,
Respiratory
failure
144 112 N/A No N/A 126 9.85 0.37 55
2 11 82 F 33.6 Obtunded Pneumonia Respiratory
failure,
shock
38 80 N/A Yes N/A 120 78.2 0.5 105
Page 34
13 12 84 F 30.0 Global
amnesia
N/A 33 60 N/A No No 135 63.2 0.17 85
14 13 62 M 35.3 Delayed
response
Non-
compliance
Pleural
effusions
50 74 Low
volt
N/A N/A 134 >60 undetec
table
60
15 14 47 F 33.2 Lethargic None Pericardial
effusion
88 73 None N/A N/A Low 6.09 0.83 40-
>80
16 15 88 F 36.1 Lethargic Bok Choy 58 119 N/A Yes Yes 132 74.4 undetec
table
60
17 16 68 F 29.1 Changes in
MS
Sunitinib 46 107 N/A No No 115 41.4 undetec
table
75
18 17 27 F 36.6 Changes in
MS
Diabetic
ketoacidosi
s
None 40 98 Low
volt
N/A N/A 132 48 0.4 45
19 18 64 F 30.1 Changes in
MS
Urinary
infection
None 60 84 N/A No Yes 138 > 200 <0.35 70
20 19 33 F 35 Coma Non-
compliance
Hypoglyce
mia
50 76 N/A No N/A 138 >100 0.24 60
21 20 74 F 34.8 Stupor CVA 59 50 Low Yes No 121 30.12 0.05 100
Page 35
volt
Prol
QT
22 21 78 M 35.5 Coma N/A Hypoactive
BS
52 70 N/A N/A Yes 106 61.24 <0.3 75
23 22 60 F 37.7 Altered
sensorium
(obtunded)
sepsis Ogilvie’s
syndrome
(ileus)
bradic 125 Juncti
onal
rythm
N/A N/A 122 341.57 1.6* 75
Ref, reference; Pt, patient; Temp, temperature; MAP, mean arterial pressure; EKG, electrocardiogram; N/A, not available.
DIC, disseminated intravascular coagulation; ARDS, acute respiratory distress syndrome; MS, mental status;
CVA, cerebrovascular accident; BS, bowel sounds; Heart rate in beats/min.
*Total T4: 1.6 ug/dL (5.6 – 13.7ug/dL)
Page 36
a
Figure 1. ROC curve of the scoring system for myxedema coma
0.00
0.25
0.50
0.75
1.00
Sen
sitiv
ity
0.00 0.25 0.50 0.75 1.001 - Specificity
Area under ROC curve = 0.8827
≥60
≥65
≥70
≥75
≥80
≥105
≥120
>120
≥90
≥95
≥100
≥25 ≥50 ≥45



























![Long-term Behavioral Problems in Children With Severe …pediatrics.aappublications.org/content/pediatrics/138/5/...consciousness (Blantyre coma score [BCS] ≤2) and Plasmodium falciparum](https://static.documents.pub/doc/80x56/5ac1a5947f8b9a5a4e8d6456/long-term-behavioral-problems-in-children-with-severe-blantyre-coma-score-bcs.jpg)









