50
Bringing Combat Medicine to the “Streets of EMS” MAJ Will Smith MD, EMT-P US Army www.wildernessdoc.com June 11, 2010 CSEC Telluride, CO
| Date post: | 14-Apr-2016 |
| Category: |
Documents |
| Upload: | john-alexander-gallin |
| View: | 8 times |
| Download: | 0 times |
BringingCombat Medicine
to the “Streets of EMS”
MAJ Will Smith MD, EMT-P
US Army www.wildernessdoc.com
June 11, 2010CSEC
Telluride, CO

Disclaimers
• No financial conflicts to disclose
• Board of Advisors for Chinook Med
• Volunteer Position - sample products
• This presentation is NOT an official position or endorsement from the United States Department of Defense/US Army

Objectives
• Briefly describe military tactical combat casualty care (TCCC)
• How to apply what we learn between austere environments (EMS?)
• Discuss products and protocols that should be adopted into EMS patient care

My Experience
• EMT - Basic 1990
• EMT- Intermediate 1992
• EMT - Paramedic 2005
• MD - 2001
• Emergency Medicine - 2004

My Experience
• Joined Army Reserve - Sept 27, 2001
• Deployments
• Iraq - Dec 2005 to Mar 2006
• Egypt - Oct 2007 to Nov 2007
• Iraq - Oct 2008 to Jan 2009
• El Salvador - Sept 2009
• Panama - April 2010

• Before: ‘Streets of EMS’ to Combat• Now: Combat to ‘Streets of EMS’

TCCC
Butler, et. al. Military Medicine 2006
• Tactical Combat Casualty Care - 1996
“Conventional civilian medicine was not appropriate for optimizing casualty care within the tactical environment.”

TCCC• American College of Surgeons (PHTLS)

Levels of Combat Care
• Self Aid
• Buddy Aid
First Aid Kit - All Soldiers

Levels of Combat Care
• Combat Life Saver
EMR

Levels of Combat Care
• Combat Lifesaver Skills (CLS)
• Rapid casualty assessment (Triage)
• Control hemorrhage
• Treat penetrating chest trauma
• Maintain BLS airway
• Initiate saline lock and IVF (Removing?)
• Package casualty for transport

Levels of Combat Care
• Combat Medic
• 91 Whisky
• Special Forces Medic
• 18 Delta
EMT or Paramedic

Levels of Combat Care
• Medical Treatment Facilities (MTF)
• Level 1 - BAS
• Level 5 - CONUS
Rural Clinic to Trauma Center

TCCC
• 3 Phases
• Care under fire
• Tactical field care
• Tactical Evacuation Care

Care Under Fire
• Return fire
• Provide basic care
• Stop bleeding (TQ)
• Move patient to CCP (if safe)
Scene Safety

Tactical Field Care
• No longer under direct fire
• AVPU
• Airway, Breathing
• NPA
• Recovery position (on side)
• Rescue breaths
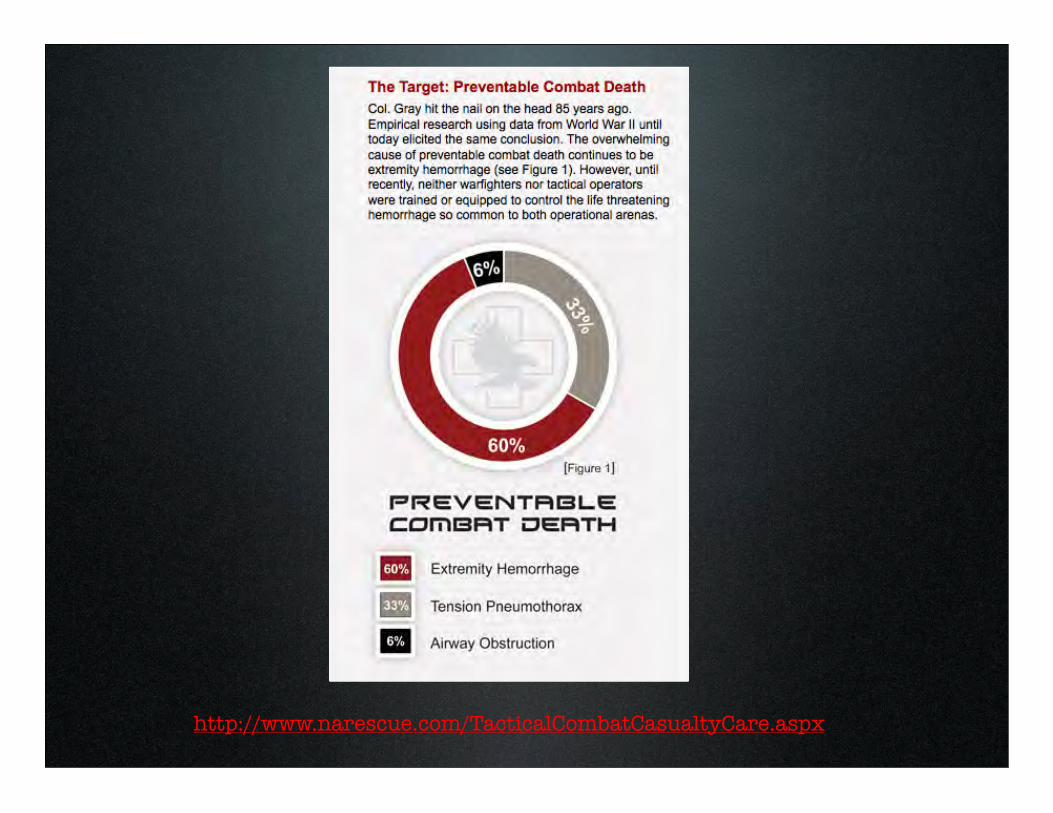
http://www.narescue.com/TacticalCombatCasualtyCare.aspx

LTC McManus, USAISR

LTC McManus, USAISR

Tactical Field Care• “Tourniquet First” for
extremity bleeding
• Use other methods as needed
• Direct pressure
• Pressure bandages
• Hemostatic agents
• Forget Pressure Points and Elevation!
Last Resort or First Choice?

Tactical Field Care
• Chest injuries
• Cover sucking chest wounds
• Needle decompression

Combat Medic
• Additional Skills
• Surgical Criocthyroidotomy
Tracheal Hook
Cuffed Tube

King Airway

Tactical Field Care
• IV Fluids
• Radial pulse - Saline Lock
• No Radial - 500 ml Hextend
• 30 min - No Radial - 500 ml Hextend
Limited Resources
Tactical Field Care
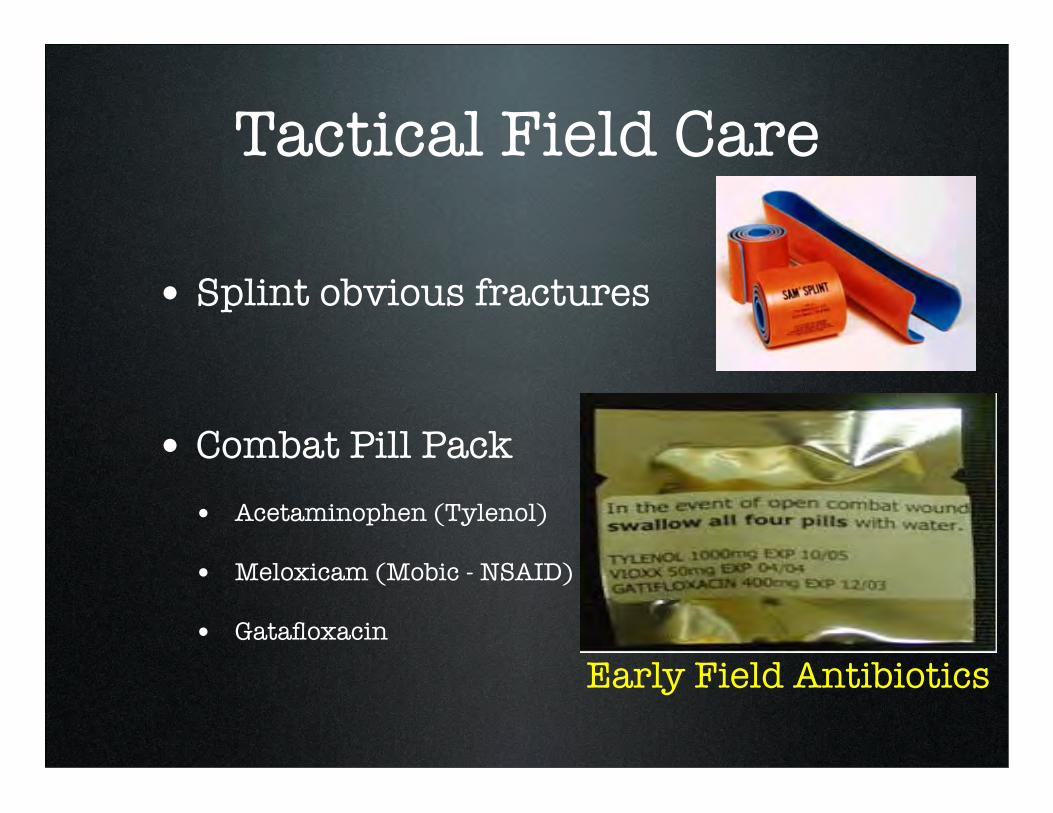
• Splint obvious fractures
• Combat Pill Pack• Acetaminophen (Tylenol)
• Meloxicam (Mobic - NSAID)
• Gatafloxacin
Early Field Antibiotics

Combat TACEVAC
• TACEVAC - Tactical Evacuation
• CASEVAC - Casualty Evacuation
• MEDEVAC - Medical Evacuation
!

Combat Medic
• Narcotics
• Morphine Auto-Injectors (5-10 mg)
• ACTIQ - ‘Fentanyl Pop’
• Intranasal Ketamine
• Narcan, Fentanyl
• Versed, Glucagon

Combat Medic
• Intraosseous (IO)
Bleeding Control
• Direct Pressure
• Elevation (above heart)
• Pressure Points
• Tourniquet (LAST RESORT)
Old Algorithm

“Hemorrhage due to penetrating trauma is the leading cause of preventable death during military operations” Butler, JEMS 2008

Tourniquets
• Risk vs. Benefit
• Appropriately applied
• Limited application time

Tourniquets
C-A-T Tourniquet

What makes a good TQ?
• Width >1”, Mechanical arm (cam)
• Easily application (<60 sec)
• Self-applied, adjustable, non-slip

Ideal Pneumatic Cuff
Delphi Tourniquet

Compression Bandages
• Direct Pressure = Stop Bleeding

Compression Bandages

PPE
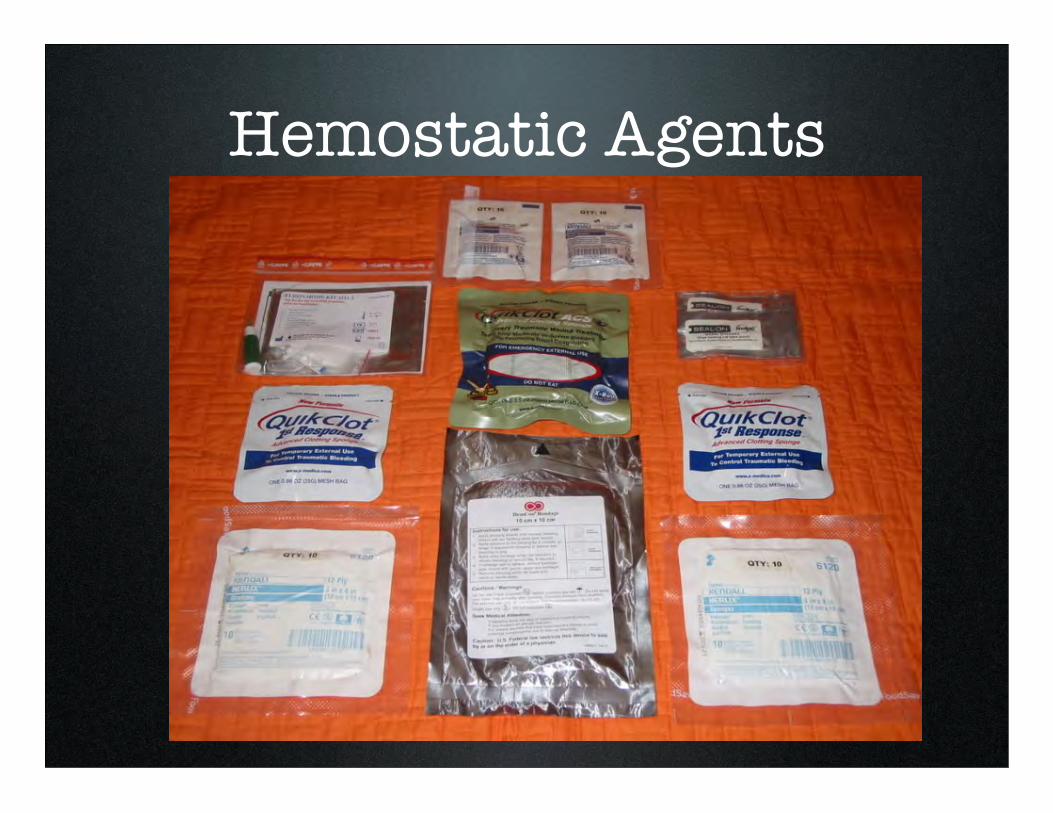
Hemostatic Agents

Hemostatic Agents
• Stop bleeding in areas where TQ don’t work
• TCCC Top agent:
• Combat Guaze

Other Agents

Harmful effects of Granular Clotting Agents
• Kheirabadi, J Trauma 2009
• Exothermic local effect of complete vessel occlusions (injured and surrounding)
• Embolic events (PE/Stroke)

Hypothermia Prevention

Hypothermia Kills
• Even in Iraq, 18% of pts arrived T<36C (96.8F)
• Temps in critical trauma pts < 34C (93F) = near 100% mortality

HPMK - Hypothermia Kit

Warmed Fluid (blood)

Exposure to other things

Summary
• “Tourniquet First” for severe extremity bleeding
• Adapted protocols for EMS and Tactical Settings

References
• The War on Trauma, Lessons Learned from a Decade of Conflict. Supplement to JEMS October 2008, sponsored by North American Rescue, Inc. Download at: www.NARescue.com
• War Surgery in Afghanistan and Iraq. A series of cases, 2003-2007. Ed. Nessen, et. al. 2008. Office of the Surgeon General.

References
• Combat Lifesaver Course: Student Self-Study Guide. Subcourse IS0871, Edition B. Army Institute for Professional Development. Ft. Sam Houston, TX.

Questions?
www.wildernessdoc.com

















