ORIGINAL ARTICLE Combined 99m Tc-methoxyisobutylisonitrile scintigraphy and fine-needle aspiration cytology offers an accurate and potentially cost-effective investigative strategy for the assessment of solitary or dominant thyroid nodules Anita Wale & Kenneth A. Miles & Barnaby Young & Charles Zammit & Anthony Williams & John Quin & Sabina Dizdarevic Received: 2 April 2013 /Accepted: 14 August 2013 /Published online: 13 September 2013 # Springer-Verlag Berlin Heidelberg 2013 Abstract Purpose Fine-needle aspiration (FNA) has revolutionised the care of patients with thyroid nodules and is the initial inves- tigation of choice. However, as a result of nondiagnostic (Thy1) and nonneoplastic (Thy2) specimens, it remains an imperfect sole solution with a range of sensitivities and a high inadequate ratio. Therefore the British Thyroid Association (BTA) guidelines recommend a second FNA immediately for Thy1 specimens and 3–6 months later for Thy2 specimens. Patients must be followed up to exclude malignancy. In this study we assessed the performance of MIBI scintigraphy for diagnosing thyroid malignancy and the cost-effectiveness of a combined FNA/MIBI investigative strategy for the manage- ment of thyroid nodules. Methods The diagnostic performance of MIBI scintigraphy was calculated from a retrospective review of local data com- bined with a meta-analysis of the published literature. Deci- sion tree analysis was used to calculate the cost-effectiveness of a combined FNA/MIBI investigative strategy compared to the BTA guidelines. Results From 712 patients, the sensitivity, specificity, PPV and NPVof MIBI scintigraphy for the diagnosis of malignan- cy were 96 %, 46 %, 34 % and 97 %, respectively. MIBI- based strategies were more accurate and associated with lower cost per patient (£1,855/€2,125 vs. £2,445/€2,801) and lower cost per cancer diagnosed (£1,902/€2,179 vs. £2,469/€2,828) with negligible change in life expectancy. Conclusion Due to its high NPV, MIBI scintigraphy can usefully exclude malignancy for Thy1 and Thy2 lesions. Its low specificity means MIBI scintigraphy cannot be recom- mended as a first-line investigation, but as a second-line investigation MIBI scintigraphy may lead to a lower rate of unnecessary thyroidectomies. Combined FNA/MIBI strate- gies are potentially cost-effective in the management of solitary or dominant thyroid nodules. Keywords Thyroid cancer . MIBI . FNA Introduction The incidence of thyroid cancer is increasing, but the early diagnosis of thyroid cancer is challenging. Detecting thyroid carcinomas at an early histological stage—before significant spread outside the thyroid parenchyma—improves 5-year A. Wale : S. Dizdarevic Department of Nuclear Medicine, Brighton and Sussex University Hospitals NHS Trust, Brighton, UK K. A. Miles University College London, London, UK B. Young Tan Tock Seng Hospital, 11 Jalan Tan Tock Seng, Novena, Singapore C. Zammit Department of Surgery, Brighton and Sussex University Hospitals NHS Trust, Brighton, UK A. Williams Department of Pathology, Brighton and Sussex University Hospitals NHS Trust, Brighton, UK J. Quin Department of Endocrinology and Diabetes, Brighton and Sussex University Hospitals NHS Trust, Brighton, UK A. Wale (*) Department of Nuclear Medicine, Royal Sussex County Hospital, Eastern Road, Brighton BN2 5BE, UK e-mail: [email protected]Eur J Nucl Med Mol Imaging (2014) 41:105–115 DOI 10.1007/s00259-013-2546-0
Transcript
ORIGINAL ARTICLE
Combined 99mTc-methoxyisobutylisonitrilescintigraphy and fine-needle aspiration cytology offersan accurate and potentially cost-effective investigative strategyfor the assessment of solitary or dominant thyroid nodules
Anita Wale & Kenneth A. Miles & Barnaby Young &
Charles Zammit & Anthony Williams & John Quin &
Sabina Dizdarevic
Received: 2 April 2013 /Accepted: 14 August 2013 /Published online: 13 September 2013# Springer-Verlag Berlin Heidelberg 2013
AbstractPurpose Fine-needle aspiration (FNA) has revolutionised thecare of patients with thyroid nodules and is the initial inves-tigation of choice. However, as a result of nondiagnostic(Thy1) and nonneoplastic (Thy2) specimens, it remains animperfect sole solution with a range of sensitivities and a highinadequate ratio. Therefore the British Thyroid Association(BTA) guidelines recommend a second FNA immediately forThy1 specimens and 3–6 months later for Thy2 specimens.Patients must be followed up to exclude malignancy. In thisstudy we assessed the performance of MIBI scintigraphy for
diagnosing thyroid malignancy and the cost-effectiveness of acombined FNA/MIBI investigative strategy for the manage-ment of thyroid nodules.Methods The diagnostic performance of MIBI scintigraphywas calculated from a retrospective review of local data com-bined with a meta-analysis of the published literature. Deci-sion tree analysis was used to calculate the cost-effectivenessof a combined FNA/MIBI investigative strategy compared tothe BTA guidelines.Results From 712 patients, the sensitivity, specificity, PPVand NPVof MIBI scintigraphy for the diagnosis of malignan-cy were 96 %, 46 %, 34 % and 97 %, respectively. MIBI-based strategies were more accurate and associated with lowercost per patient (£1,855/€2,125 vs. £2,445/€2,801) and lowercost per cancer diagnosed (£1,902/€2,179 vs. £2,469/€2,828)with negligible change in life expectancy.Conclusion Due to its high NPV, MIBI scintigraphy canusefully exclude malignancy for Thy1 and Thy2 lesions. Itslow specificity means MIBI scintigraphy cannot be recom-mended as a first-line investigation, but as a second-lineinvestigation MIBI scintigraphy may lead to a lower rate ofunnecessary thyroidectomies. Combined FNA/MIBI strate-gies are potentially cost-effective in the management ofsolitary or dominant thyroid nodules.
Keywords Thyroid cancer . MIBI . FNA
Introduction
The incidence of thyroid cancer is increasing, but the earlydiagnosis of thyroid cancer is challenging. Detecting thyroidcarcinomas at an early histological stage—before significantspread outside the thyroid parenchyma—improves 5-year
A. Wale : S. DizdarevicDepartment of Nuclear Medicine, Brighton and Sussex UniversityHospitals NHS Trust, Brighton, UK
K. A. MilesUniversity College London, London, UK
B. YoungTan Tock SengHospital, 11 Jalan Tan Tock Seng, Novena, Singapore
C. ZammitDepartment of Surgery, Brighton and Sussex University HospitalsNHS Trust, Brighton, UK
A. WilliamsDepartment of Pathology, Brighton and Sussex University HospitalsNHS Trust, Brighton, UK
J. QuinDepartment of Endocrinology and Diabetes, Brighton and SussexUniversity Hospitals NHS Trust, Brighton, UK
A. Wale (*)Department of Nuclear Medicine, Royal Sussex County Hospital,Eastern Road, Brighton BN2 5BE, UKe-mail: [email protected]
Eur J Nucl Med Mol Imaging (2014) 41:105–115DOI 10.1007/s00259-013-2546-0
relative survival rate (from about 50–51 % at stage IV to near100 % at stage I for papillary and follicular thyroid cancer [1])with excision and radioiodine therapy [1, 2]. Such tumoursmost commonly present as a solitary palpable nodule in aeuthyroid patient. However, determining which nodules con-tain malignancy is difficult: solitary palpable nodules arepresent in 5–7 % of the population, and only less than 5 %of these contain malignancy [3].
Fine needle aspiration (FNA) cytology is the first-lineinvestigation of choice, with further management determinedaccording to the Thy 1–5 staging system as recommendedby the British Thyroid Association (BTA) guidelines [4]. Inthe UK the Thy 1–5 staging system is used to classify thefindings of the FNA cytology for the sample in terms of itsadequacy and nature, i.e. how likely it is that the sample isbenign or malignant [3]. The categories are summarized inTable 1.
Management of patients with Thy3 – Thy5 lesions isclear, as with the high rate of malignancy patients shouldall proceed to resection. However, patients with Thy1 orThy2 (nondiagnostic or nonneoplastic) lesions pose a diag-nostic challenge. Others have found up to 20 % of Thy1lesions and up to 10 % of Thy2 lesions are malignant [5], andthus the BTA guidelines recommend repeat FNA as shown inTable 1. Furthermore, if a confident diagnosis is not reachedafter repeat FNA, the BTA guidelines recommend resectionof the thyroid nodule [4]. This strategy of repeat FNA andthe possibility of resection have potential patient and costimplications.
Functional imaging of the thyroid has traditionally beenused in clinical practice as part of the assessment of thyroidnodules, A number of radiochemicals have been investigatedincluding 99mTc-pertechnetate [6], 99mTc-methoxyisobuty-lisonitrile (MIBI), radioiodine, 210Tl [7], tetrofosmin [8] and18F-FDG [9]. In practice 99mTc-pertechnetate is useful forimaging thyrotoxic patients and identifying toxic nodules;however by itself, it has a very low specificity for malignancy
[10]. Of the tumour-seeking radiopharmaceuticals, MIBI hasbeen considered most useful as it is readily available, offerslow radiation exposure of the patient and a high tumour tobackground ratio due to accumulation in the mitochondriaof metabolically active cells [11, 12]. MIBI uptake has beenreported as highly sensitive for thyroid neoplasia, but itsroutine use is hampered by low specificity [13]. Morerecently others have investigated the potential role of MIBIscintigraphy in combination with FNA cytology to detectmalignancy in patients with nondiagnostic FNA cytology.In this situation MIBI scintigraphy has been shown to havea high negative predictive value (NPV) for excluding ma-lignancy. In addition, the potential role of MIBI scintigra-phy as a second-line investigation after FNA cytology toexclude rather than confirm malignancy may avoid theproblem of the low specificity of MIBI scintigraphy formalignancy.
A combined FNA/MIBI investigative strategy has beenused in our centre for the investigation of solitary and domi-nant thyroid nodules. In this study:
1. We reviewed our UK institutional experience with MIBIscintigraphy and correlated the results of MIBI scintigra-phy with histology to determine the sensitivity, specificity,positive predictive value (PPV) and NPV of MIBI scin-tigraphy in the investigation of patients with a solitary ordominant palpable thyroid nodule without compressivesymptoms.
2. We performed a meta-analysis of the published studiescombined with our local experience, reviewing the sensi-tivity, specificity, PPV and NPV of MIBI scintigraphy todetermine the role for MIBI scintigraphy in excludingmalignancy.
3. We assessed whether a combined FNA/MIBI investiga-tive strategy is more cost-effective than the FNA-onlystrategy outlined in the BTA guidelines in the investiga-tion of patients with thyroid nodules.
Table 1 Diagnostic categories for FNA cytology of the thyroid from the BTA guidelines [4]
Thy4 Suspicious for malignancy (but not diagnostic) Multidisciplinary discussion
Repeat FNAwith or without surgical intervention
Thy5 Diagnostic of malignancy Multidisciplinary discussion
Differentiated and medullary thyroid cancer: surgical intervention
Anaplastic, lymphoma or metastatic cancer: further investigation,radiotherapy with or without chemotherapy
106 Eur J Nucl Med Mol Imaging (2014) 41:105–115
Materials and methods
Institutional (local) data
A retrospective review was undertaken of patients who wereseen in a multidisciplinary clinic for the assessment of apalpable thyroid nodule between 2002 and 2010. Patientswere entered into this study if they had a solitary or dominantcold thyroid nodule on 99mTc-pertechnetate scintigraphy, didnot have compressive symptoms and then underwentthyroidectomy.
Radionuclide imaging
Our local institutional practice uses both FNA and radionu-clide imaging to assess patients with a palpable thyroid nodule.A combination of the FNA cytology results, in line with theBTA guidelines, and MIBI scintigraphy results is used todecide on a patient’s management. Initial 99mTc-pertechnetatescintigraphy is performed with 80 MBq of 99mTc-pertechne-tate (Administration of Radioactive Substances AdvisoryCommittee UK-ARSAC diagnostic reference level) adminis-tered intravenously with imaging performed 20 min afterinjection. If a cold nodule is seen on 99mTc-pertechnetateimaging, MIBI scintigraphy is performed on the sameday with 400 MBq of 99mTc-MIBI administered intrave-nously with imaging performed 20 min after injection. De-layed views are not routinely obtained.
The images were visually reported for areas of mismatcheduptake by S.D. (nuclear medicine physician with 18 yearsexperience in nuclear medicine), and each study was scoredas “negative” or “positive” based on the MIBI scintigraphyfindings. A positive studywas a studywithMIBI–pertechnetatemismatch indicating neoplasia (Fig. 1) and a negative studywasa study with no MIBI–pertechnetate mismatch indicating be-nign pathology (Fig. 2).
FNA cytology data were collected and each sample wasgradedThy1 toThy5 according to theBTAguidelines (Table 1).A combination of the FNA cytology data and imaging resultswas used to decide on a patient’s further management. Histo-logical data were collected retrospectively, and each samplewas scored as “benign” or “malignant” from the pathologyreport. The sensitivity, specificity, PPVand NPV for the detec-tion of malignancy by MIBI scintigraphy compared to histolo-gy as the gold standard were then calculated.
MIBI meta-analysis
Search strategy
The MEDLINE database on PubMed was searched on 14September 2010 (1950 – present) using the following searchterms: “MIBI”, “sestaMIBI”, “thyroid”, "nodule" 'NOT'
"parathyroid" combined with the Boolean operators ‘AND’and ‘NOT’ “parathyroid”. The titles were initially scanned andabstracts of interest were reviewed. The reference lists of allarticles reviewed and included in the studywere scanned and thestudies found were included in the study if they met the inclu-sion criteria.
Inclusion criteria
To be included in the review: (1) the study had to havecorrelated MIBI scintigraphy results with histology from thy-roidectomy, (2) the study had to have had a similar MIBIacquisition to our local practice, and (3) the article had to reportthe raw data required to calculate the prevalence, sensitivity,specificity, PPVand NPV.
Exclusion criteria
The following criteria were used to exclude studies from thereview: (1) if semiquantification methods were used in thereporting ofMIBI scintigraphy, (2) if the histological data werenot extractable for each case, (3) if the studywas in animals, (4)
Fig. 1 Positive MIBI study with mismatch between the 99mTc-pertechnetate (99mTcO4
−) study (a) that shows a dominant cold nodulein the right lower pole and the 99mTc-MIBI study (b)
Eur J Nucl Med Mol Imaging (2014) 41:105–115 107
if the study was in humans under the age of 18 years, and (5) ifthe article was a conference abstract, editorial, commentary/letter or review.
Data extraction
Two authors (A.W., B.Y.) independently collected and tabu-lated the data into an electronic spreadsheet. Any differencesin collated data between the two authors were discussed andagreement was reached by consensus. The specific itemscollected were the following: first author, year of publication,study sample size, 99mTc-pertechnetate andMIBI scintigraphyimaging protocol and reporting methods.
Cost-effectiveness analysis
Decision tree analysis was used to compare the cost-effectivenessof the FNA-only strategy outlined in the BTA guidelines (Fig. 3)with a combined FNA/MIBI investigative strategy (Fig. 4). TheBTA guidelines advise that Thy2 nodules receive a repeat aspi-ration 3–6 months after the initial FNA cytology result and thatThy1 samples are re-aspirated immediately. All patients with
Thy3 – Thy5 lesions proceed to thyroidectomy due to the highrisk of malignancy. As per our local clinical practice, Fig. 4outlines the combined FNA/MIBI investigative strategy whichincorporates MIBI scintigraphy into the BTA guidelines. Thy1and Thy2 lesions are investigated with MIBI scintigraphy.MIBI–pertechnetate matched cold nodules are not investigatedfurther, and any MIBI–pertechnetate mismatch requires repeataspiration.
Model input assumptions
An audit of FNA cytology was also performed over the sameperiod of time for patients attending the multidisciplinarythyroid clinic in order to calculate inadequacy ratios and theinput assumptions for the cost-effectiveness analysis.
FNA cytology was performed according to best practiceguidelines, with a multidisciplinary approach, ultrasound guid-ance and on-site cytology support for immediate adequacyassessment. Any Thy1 FNA cytology samples were regardedas inadequate. In order to calculate sensitivity and specificity forFNA cytology, patient results were grouped into “nondiagnosticor nonneoplastic” (Thy1 or Thy2), or “malignant/likely malig-nant” (Thy3 – Thy5). Histological data were collected for thesepatients and the sensitivity and specificity of FNA cytology indetecting malignancy compared to histology as the gold stan-dard was then calculated. The sensitivity and specificity of FNAcytology were assumed to be the same when used as the first-line investigation of palpable thyroid nodules, when used afterMIBI scintigraphy, and when used on Thy1 samples. However,the inadequate fraction was estimated as double the baseline forrepeat FNA cytology [14].
The diagnostic performance of MIBI scintigraphy wasderived from the meta-analysis and the baseline prevalenceof malignancy in thyroid nodules was 5 %, in keeping withtypical clinical populations [3]. Mortality from hemithy-roidectomy was modelled at 0.2 % due to postoperativehaematomas [15]. Life expectancy (LE) was modelled at34.5 years in patients with diagnosed thyroid cancer,34.5 years in those with a benign thyroid lesion and 20.7 yearsin those with undiagnosed thyroid cancer [16].
Unit costs for MIBI scintigraphy and FNA cytology wereestimated from pricing structures at the hospital. The cost ofthyroidectomy was obtained from the Healthcare ResourceGroups version 3.5 (HRG3.5) National Health Service (NHS)Casemix service.
Model outputs and cost-effectiveness analysis
The model outputs for each strategy were (a) the proportion ofnodules correctly diagnosed, (b) the proportion of cancersdetected, (c) average LE, (d) cost per patient, and (e) costper cancer detected. Cost-effectiveness of the FNA/MIBIinvestigative strategy was expressed as net monetary benefit
Fig. 2 Negative MIBI study with no mismatch between the 99mTc-pertechnetate (99mTcO4
−) study (a) and the 99mTc-MIBI study (b) whichhave similar appearances
108 Eur J Nucl Med Mol Imaging (2014) 41:105–115
(NMB) based on a value of £30,000/€34,372 for a year oflife, as adopted by the National Institute for Health and
Clinical Excellence (NICE) and calculated from the follow-ing equation:
NMB Uð Þ ¼ 30; 000� LE FNA=MIBI strategy−LE BTA strategyð Þ− Cost of FNA=MIBI strategy−Cost of BTA Strategyð Þ
The FNA/MIBI investigative strategy is cost-effective ifthe NMB is positive.
Sensitivity analysis
The impact of variations in the input assumptions of NMBwas assessed by varying the input assumptions as shown inTable 5. The limits of the diagnostic performance of FNA andMIBI scintigraphy are represented by the 95th percentiles ofthe respective values. The operative mortality was reduced to0 in keeping with local experience.
Results
Local study
The inclusion criteria for entry into the study were met by 108patients, each with a solitary or dominant thyroid nodule
without compressive symptoms. The imaging and histologyof each of these patients was reviewed and scored. A total of17 malignancies were diagnosed on histology, and thus theprevalence of malignancy was 16 %.
FNA cytology was performed in 91 of the 108 patients. Inthose patients who underwent FNA cytology 20 of 91 of thenodules were Thy1, 45 were Thy2, 21 were Thy3, 4 wereThy4 and 1 was Thy5. In 17 patients malignancy was diag-nosed histologically from thyroidectomy, and 16 of thesepatients had corresponding FNA cytology results. In 13 ofthese 16 patients, the lesion was correctly identified by FNAcytology as follicular or malignant (Thy3 – Thy5), in 2 pa-tients the result was falsely negative (Thy2), and in 1 FNAcytology was nondiagnostic (Thy1).
MIBI scintigraphy was positive in 81 of 108 patients(75 %) and was positive in each patient with histolog-ically confirmed malignancy; therefore the sensitivity ofMIBI scintigraphy was 100 %. MIBI scintigraphy wasnegative in only 27 of 108 patients (25 %) resulting in
Fig. 3 Decision tree. BTA guidelines as the baseline strategy
Eur J Nucl Med Mol Imaging (2014) 41:105–115 109
a specificity of only 30 %. The PPV was 21 % and theNPV was 100 %.
Meta-analysis
Study selection
A total of 38 citations including references were found. Ab-stracts were reviewed to exclude review articles, case reports,and other irrelevant papers—leaving 16 articles. From the fullpapers, nine of these were considered suitable for the meta-analysis, excluding those in which histological data were notextractable for each case or semiquantification methods wereused, and one article that was unobtainable [17].
Imaging methodology
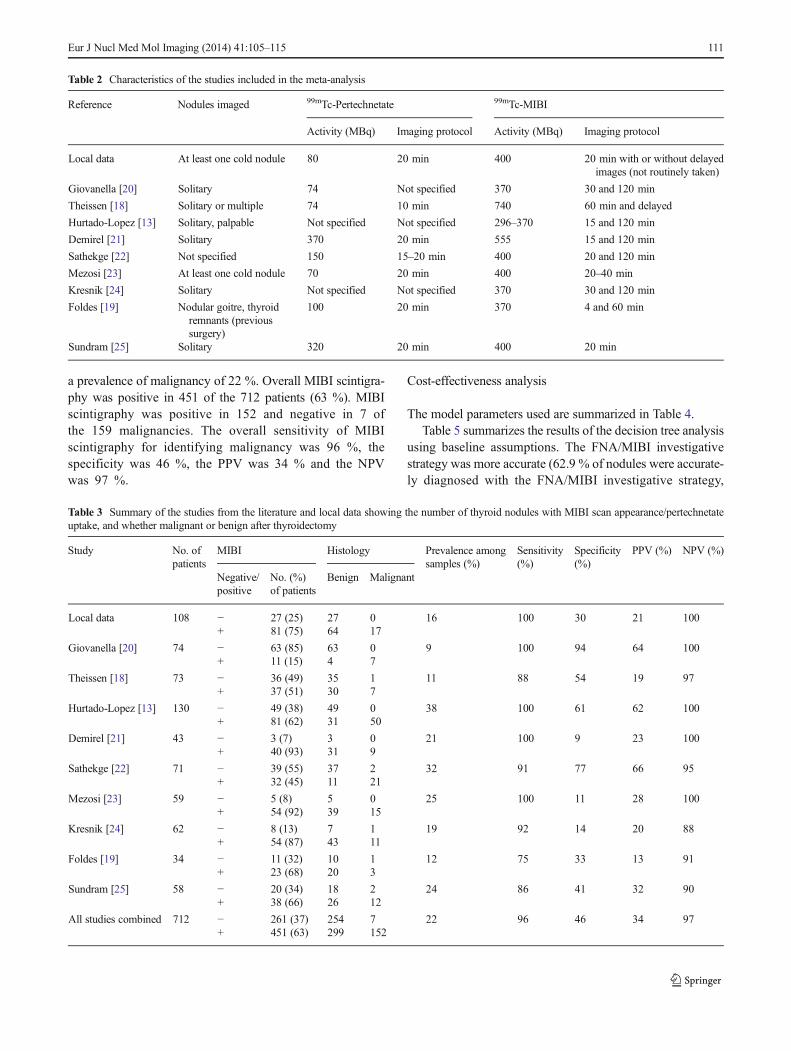
The acquisition and interpretation methods in each study aresummarized in Table 2.
All but two studies in the analysis used static imaging 15–20 min after intravenous injection of 300–600 MBq of 99mTc-MIBI. Theissen et al. imaged with 740 MBq of MIBI 60 min
after injection [18] and Foldes et al. imaged with 370 MBq ofMIBI 4 min and 60 min after injection [19]. Interpretation ofall images relied on visual inspection and scoring as A, B or C(where A is cold, B is warm, and C is hot) or as 0, 1, 2 or 3(where 0 is no significant uptake, 1 is increased uptake, butless than normal thyroid, 2 is uptake equal to normal thyroid,and 3 is uptake greater than normal thyroid).
The results with the most conservative regimen, in whichany MIBI uptake (i.e. MIBI–pertechnetate mismatch) indicat-ed neoplasia (i.e. scores of B or C, or 1, 2 or 3) and no MIBI–pertechnetate mismatch indicated benign pathology, weresummed and compared with the histological data. The highprevalence of malignancy among these samples reflects theretrospective nature of the studies in which patients hadfulfilled additional selection criteria for surgery, be itFNA or clinical.
Results
The results from each of the nine studies and our local data aresummarized in Table 3. The studies included a total of 712patients with 159 malignancies diagnosed histologically with
a prevalence of malignancy of 22 %. Overall MIBI scintigra-phy was positive in 451 of the 712 patients (63 %). MIBIscintigraphy was positive in 152 and negative in 7 ofthe 159 malignancies. The overall sensitivity of MIBIscintigraphy for identifying malignancy was 96 %, thespecificity was 46 %, the PPV was 34 % and the NPVwas 97 %.
Cost-effectiveness analysis
The model parameters used are summarized in Table 4.Table 5 summarizes the results of the decision tree analysis
using baseline assumptions. The FNA/MIBI investigativestrategy was more accurate (62.9 % of nodules were accurate-ly diagnosed with the FNA/MIBI investigative strategy,
Table 2 Characteristics of the studies included in the meta-analysis
Table 3 Summary of the studies from the literature and local data showing the number of thyroid nodules with MIBI scan appearance/pertechnetateuptake, and whether malignant or benign after thyroidectomy
Study No. ofpatients
MIBI Histology Prevalence amongsamples (%)
Sensitivity(%)
Specificity(%)
PPV (%) NPV (%)
Negative/positive
No. (%)of patients
Benign Malignant
Local data 108 − 27 (25) 27 0 16 100 30 21 100+ 81 (75) 64 17
compared with 37.8 % with the BTA strategy), but the FNA/MIBI investigative strategy detected a slightly lower propor-tion of cancers (97.5 %, compared with 99 % with the BTAstrategy). The cost per patient and cost per cancer detectedwere lower for the FNA/MIBI investigative strategy with amarginally longer LE (2.6 days). The NMB for baselineconditions was £800/€917.
The results of the sensitivity analysis are shown in Table 6.The NMB was most sensitive to prevalence of malignancy,falling below £0/€0 if the prevalence value was 16 % orabove. The NMB remained positive for variations in all otherparameters.
Discussion
The use of FNA cytology for the diagnosis of thyroid cancerin thyroid nodules is an imperfect sole test: our local datashowed that 16 out of 17 histologically proven malignancies
had FNA cytology, but FNA cytology correctly identifiedonly 13 of these 16 nodules as malignant. To the best of ourknowledge our study is the first to quantify the impact of theuse of MIBI scintigraphy through cost-effectivenessanalysis and the first to consider the potential impactof MIBI scintigraphy on BTA guidelines. There hasbeen one previously published editorial which correlatedMIBI uptake with histology in a meta-analysis of ninestudies (448 patients) in which MIBI scintigraphy was used inpatients with hypofunctioning thyroid nodules. This publica-tion found that the NPVof a negativeMIBI scan was 100 % inpatients with differentiated and medullary thyroid cancer [26].We found a NPVof 97 %.
Our findings indicate that a combined FNA/MIBIinvestigative strategy is more accurate and has a loweraverage cost per patient. Cost per cancer detected alsofell, with no significant adverse effect on mortality. Fora typical prevalence of malignancy within the thyroidnodules of 5 %, combining MIBI with the BTA guide-lines is likely to be more cost-effective than the BTAstrategy alone with a NMB of £800/€917 per patient. Todate studies have only suggested the possibility thatincorporating MIBI scintigraphy into the diagnosticstrategy may be cost-effective [27], but no cost-effectiveness analysis has been conducted. However,sensitivity analysis suggests that for a prevalence valueabove 16 %, the BTA strategy may be more cost-effective than the combined FNA/MIBI investigativestrategy. However, patients with such a high prior prob-ability of malignancy may be considered suitable forthyroidectomy irrespective of the FNA result as a con-sequence of significant risk factors for malignancy ornodule size. Immediate thyroidectomy with no imagingwould cost £2,341/€2,682 per patient with a LE of34.43 years (allowing for operative mortality) andwould therefore be more cost-effective than the BTAstrategy (i.e. positive NMB) for a prevalence of malig-nancy of 14 % and above.
A number of simplifications were necessary to develop thismodel. It was not possible to predict how clinical experienceand preparatory investigations—for example thyroid functiontests and 99mTc-pertechnetate scans—influence selection ofthyroid nodules for FNA. In addition, the best strategy forthe follow up of repeatedly inadequate FNA specimens is notclear. A similar sensitivity and specificity for FNA whenrepeated on nodules with an initially inadequate biopsy prob-ably overestimates the performance of FNA, and thus intro-duces a bias towards the baseline strategy. The assumptionthat the inadequacy rate doubles for a repeat FNA is based onthe observation that cystic nodules often produce inadequatesamples as a result of low cellularity [14]. The exact rate isunknown, as is the probability of malignancy in these thyroidnodules. For example, occasional cystic nodules with an
Table 4 Summary of base model parameters, and ranges used for sensi-tivity analysis
Parameter Value
Prevalence of malignancy 5 % (5–20 %)
FNA (from local audit) Sensitivity: 87 % (54.8–99.7 %)
Table 5 Results of decision tree analysis using baseline assumptions
BTA strategy MIBI strategy
Proportion of nodules accuratelydiagnosed (%)
37.8 62.9
Proportion of cancers detected (%) 99.0 97.5
Average life expectancy (years) 34.45 34.46
Cost per patient £2,445/€2,801 £1,855/€2,125
Cost per cancer detected £2,469/€2,828 £1,902/ €2179
112 Eur J Nucl Med Mol Imaging (2014) 41:105–115
inadequate staging cytology for satisfactory diagnosis, receivetherapeutic FNA cytology and may not require follow up.This was not factored into to the calculations.
For the MIBI meta-analysis, we determined diagnosticsensitivity and specificity values assuming that sampling errorwas the only source of variation among the studies identified.However, when performing a meta-analysis and incorporatinga meta-analysis of diagnostic studies into economic models, itis important to consider other causes of variation amongstudies [28]. There is a potential issue when averaging sensi-tivities and specificities across a dataset, and in order to do thiswe must assume that the diagnostic threshold is the same foreach study in order to reduce the heterogeneity of the data[28]. To minimize the heterogeneity of the data, the inclusioncriteria used in our meta-analysis limited us to studies whichused MIBI scintigraphy in a comparable way to our own data,so minimizing potential variations in image acquisition andinterpretation which would have introduced heterogeneityinto the data. However, other sources of variation suchas differences in preselection of patients for surgery andimprovements in technology over the intervening yearsmay have unknown effects on the model’s performance.In addition there was variability in the sensitivity andPPV between the studies included in this meta-analysiswhich cannot be explained by variability in the preva-lence of thyroid malignancy; a cause for this variabilitycannot be identified. Nevertheless, sensitivity analysishas shown that over a wide range of parameters, theuse of MIBI scintigraphy remains cost-effective, andthus further clinical validation is warranted.
Finally, one-third of the tumours not detected by MIBIscintigraphy in this meta-analysis were anaplastic carcino-mas—a tumour associated with expression of the multidrugresistance protein (MRP1), of which MIBI is a substrate [29]
resulting in quick clearance ofMIBI from cells and potentiallycausing false-negative results. Interestingly, the presence ofMRP1 in non-oncocytic lesions is more frequently related tobenign pathology, while oncocytic lesions tend to show no orlowMRP1 expression resulting inMIBI retention and delayedwashout on delayed scans when dual-phase MIBI thyroidscintigraphy is performed [30].
The potential use of MIBI scintigraphy for inadequate FNAsamples has been discussed, but less than 80% of malignancieswere identified in our model by even the baseline strategy, theprimary source of loss being from nonneoplastic Thy2 results.There has thus been some debate regarding the benefit ofrepeating the FNA of nodules with initially nonneoplastic sam-ples; some authors recommend re-aspiration only on the basisof clinical criteria [31], whilst others have noted a significantnumber of missed malignancies without re-aspiration within 3–6 months [32]. Whilst the need to repeat the FNA in Thy1 andThy2 lesions is disputed by some authors, the BTA guidelinesrecommend repeat FNA in Thy1 nodules immediately and inThy2 nodules 3–6 months after the first FNA, and dischargefrom follow-up only with two Thy2 FNA results 3–6 monthsapart, particularly if there is clinical concern, to exclude neo-plasia [4]. This would be expected to increase the chance ofdetectingmalignancy, with amuch lower inadequacy rate, but itis also associated with considerable additional costs.
Assuming a consistent sensitivity of 96 % and a specificityof 46 %, a subsequent MIBI scan may thus form a prudentstrategy in determining re-aspiration in only those patientswith mismatched pertechnetate/MIBI uptake. Some patientsmay also be excluded by clinical criteria from further investi-gation—for example where aspiration reveals a cyst, which isaspirated to dryness.
This meta-analysis of 712 patients showing a very highNPVof 97% whenMIBI scintigraphy is incorporated into the
Table 6 Results of sensitivityanalysis Range Net monetary benefit
Prevalence 5–20 % £800–£−310/€917–€−355FNA
Sensitivity 54.8–99.7 % £669–£869/€766–€996
Specificity 83.1–92.9 % £798–£923/€914–€1,057
Indeterminate fraction
First FNA 20–31 % £655–£964/€750–€1,104
Second FNA 25–50 % £407–£800/€466–€916
MIBI
Sensitivity 90.8–98.1 % £465–£976/€533–€1,118
Specificity 42.2–50.7 % £682–£922/€781–€1,056
Operative mortality 0–0.2 % £278–£800/€318–€916
Costs
MIBI £150–£350/€172–€401 £689–£867/€789–€993
FNA £200–£600/€229–€687 £692–£874/€793–€1,001
Surgery £1,500–£4,000/€1,718–€4,582 £588–£2,439/€674–€2,794
Eur J Nucl Med Mol Imaging (2014) 41:105–115 113
diagnostic strategy indicates that MIBI scintigraphy can use-fully exclude malignancy when FNA is nondiagnostic ornonneoplastic (Thy1 or Thy2). Excluding malignancy withMIBI scintigraphy avoids unnecessary thyroidectomy andthus the proposed FNA/MIBI investigative strategy is cost-effective by saving these patients from unnecessary thyroid-ectomy and repeat FNA. Given this and the facts that up to20 % of Thy1 (nondiagnostic) aspirates may ultimately bemalignant [5] and 3.5 % of Thy2 specimens may be malignant[33], and that the false-negative rate of FNA may be up to11.5 % or even 17. 1 % [32], there is an important role forMIBI scintigraphy in the investigation of thyroid nodules.
Due to its high NPV, MIBI scintigraphy can usefully ex-clude malignancy when FNA of the thyroid is nondiagnostic(Thy1) and may provide further reassurance when FNA sug-gests benignity (Thy2). MIBI scintigraphy has a low specific-ity and therefore cannot be recommended as a first-line inves-tigation in the assessment of solitary or dominant thyroidnodules. However, the use of MIBI scintigraphy as a second-line investigation after FNA has the potential to reduce the rateof unnecessary thyroidectomies, and therefore combined FNA/MIBI strategies are potentially cost-effective in the manage-ment of thyroid nodules.
Acknowledgments The project was partially sponsored by Bristol-Myers Squibb.
Conflicts of interest None.
References
1. American Cancer Society. Thyroid cancer survival by type and stage.2013. http://www.cancer.org/cancer/thyroidcancer/detailedguide/thyroid-cancer-survival-rates. Accessed 30 August 2013.
2. Sant M, Aareleid T, Berrino F, Bielska Lasota M, Carli PM, Faivre J,et al. EUROCARE-3: survival of cancer patients diagnosed1990-94 – results and commentary. Ann Oncol. 2003;14 Suppl 5:v61–118.
4. British Thyroid Association, Royal College of Physicians. Guide-lines for the management of thyroid cancer (Perros P, editor), 2nd ed.Report of the Thyroid Cancer Guidelines Update Group. London:Royal College of Physicians; 2007.
5. Renshaw AA. Significance of repeatedly nondiagnostic thyroid fine-needle aspirations. Am J Clin Pathol. 2011;135(5):750–2.
6. Prakash R, Narayanan RV, Shankar LR, Kakar A. Radionuclideangiography in evaluation of cold solitary thyroid nodules. Improveddiagnostic accuracy using flow and washout analysis. Clin NuclMed. 1995;20(10):878–83.
7. Okumura Y, Takeda Y, Sato S, Komatsu M, Nakagawa T, Akaki S,et al. Comparison of differential diagnostic capabilities of 201Tlscintigraphy and fine-needle aspiration of thyroid nodules. J NuclMed. 1999;40(12):1971–7.
8. Kanmaz B, Erdil TY, Yardi OF, Sayman HB, Kabasakal L,Sonmezoglu K, et al. The role of 99Tcm-tetrofosmin in the evalua-tion of thyroid nodules. Nucl Med Commun. 2000;21(4):333–9.
9. Mitchell JC, Grant F, Evenson AR, Parker JA, Hasselgren PO,Parangi S. Preoperative evaluation of thyroid nodules with 18FDG-PET/CT. Surgery. 2005;138(6):1166–74; discussion 74–5.
10. Lumachi F, Varotto L, Borsato S, Tregnaghi A, Zucchetta P, MarzolaMC, et al. Usefulness of 99mTc-pertechnetate scintigraphy and fine-needle aspiration cytology in patients with solitary thyroid nodulesand thyroid cancer. Anticancer Res. 2004;24(4):2531–4.
11. Casara D, Rubello D, Saladini G. Role of scintigraphy with tumor-seeking agents in the diagnosis and preoperative staging of malignantthyroid nodules. Biomed Pharmacother. 2000;54(6):334–6.
12. Maffioli L, Steens J, Pauwels E, Bombardieri E. Applications of99mTc-sestamibi in oncology. Tumori. 1996;82(1):12–21.
13. Hurtado-Lopez LM, Arellano-Montano S, Torres-Acosta EM,Zaldivar-Ramirez FR, Duarte-Torres RM, Alonso-De-Ruiz P, et al.Combined use of fine-needle aspiration biopsy, MIBI scans andfrozen section biopsy offers the best diagnostic accuracy in theassessment of the hypofunctioning solitary thyroid nodule. Eur JNucl Med Mol Imaging. 2004;31(9):1273–9.
14. Nguyen GK, LeeMW, Ginsberg J, Wragg T, Bilodeau D. Fine-needleaspiration of the thyroid: an overview. Cytojournal. 2005;2(1):12.
15. Shrime MG, Goldstein DP, Seaberg RM, Sawka AM, Rotstein L,Freeman JL, et al. Cost-effective management of low-risk papillarythyroid carcinoma. Arch Otolaryngol Head Neck Surg. 2007;133(12):1245–53.
16. Links TP, van Tol KM, Jager PL, Plukker JT, Piers DA, Boezen HM,et al. Life expectancy in differentiated thyroid cancer: a novel ap-proach to survival analysis. Endocr Relat Cancer. 2005;12(2):273–80.
17. Sehgal AK, Sathekge MM, Mageza RB, Modiba MC. TC99mMIBIscintigraphy in well-differentiated thyroid carcinoma. Cent Afr JMed. 2001;47(4):97–102.
18. Theissen P, Schmidt M, Ivanova T, Dietlein M, Schicha H. MIBIscintigraphy in hypofunctioning thyroid nodules – can it predict thedignity of the lesion? Nuklearmedizin. 2009;48(4):144–52.
19. Foldes I, Levay A, Stotz G. Comparative scanning of thyroid noduleswith technetium-99m pertechnetate and technetium-99mmethoxyisobutylisonitrile. Eur J Nucl Med. 1993;20(4):330–3.
20. Giovanella L, Suriano S, Maffioli M, Ceriani L, Spriano G.(99m)Tc-sestamibi scanning in thyroid nodules with nondiagnosticcytology. Head Neck. 2010;32(5):607–11.
21. Demirel K, Kapucu O, Yucel C, Ozdemir H, Ayvaz G, Taneri F. Acomparison of radionuclide thyroid angiography, (99m)Tc-MIBIscintigraphy and power Doppler ultrasonography in the differentialdiagnosis of solitary cold thyroid nodules. Eur J Nucl Med MolImaging. 2003;30(5):642–50.
22. Sathekge MM, Mageza RB, Muthuphei MN, Modiba MC,Clauss RC. Evaluation of thyroid nodules with technetium-99m MIBI and technetium-99m pertechnetate. Head Neck.2001;23(4):305–10.
23. Mezosi E, Bajnok L, Gyory F, Varga J, Sztojka I, Szabo J et al. Therole of technetium-99mmethoxyisobutylisonitrile scintigraphy in thedifferential diagnosis of cold thyroid nodules. Eur J Nucl Med.1999;26(8):798–803.
24. Kresnik E, Gallowitsch HJ, Mikosch P, Gomez I, Lind P. Techne-tium-99m-MIBI scintigraphy of thyroid nodules in an endemic goiterarea. J Nucl Med. 1997;38(1):62–5.
25. Sundram FX, Mack P. Evaluation of thyroid nodules for malignancyusing 99Tcmsestamibi. Nucl Med Commun. 1995;16(8):687–93.
26. Hurtado-Lopez LM, Martinez-Duncker C. Negative MIBI thyroidscans exclude differentiated and medullary thyroid cancer in 100% ofpatients with hypofunctioning thyroid nodules. Eur J Nucl Med MolImaging. 2007;34(10):1701–3.
27. Polyzos SA, Kita M, Avramidis A. Thyroid nodules – stepwisediagnosis and management. Hormones (Athens). 2007;6(2):101–19.
28. Sutton AJ, Cooper NJ, Goodacre S, Stevenson M. Integration ofmeta-analysis and economic decision modeling for evaluating diag-nostic tests. Med Decis Making. 2008;28(5):650–67.
29. Sugawara I, Masunaga A, Itoyama S, Sumizawa T, AkiyamaS, Yamashita T. Expression of multidrug resistance-associatedprotein (MRP) in thyroid cancers. Cancer Lett. 1995;95(1-2):135–8.
30. Saggiorato E, Angusti T, Rosas R, Martinese M, Finessi M,Arecco F, et al. 99mTc-MIBI Imaging in the presurgicalcharacterization of thyroid follicular neoplasms: relationshipto multidrug resistance protein expression. J Nucl Med.2009;50(11):1785–93.
31. Merchant SH, Izquierdo R, Khurana KK. Is repeated fine-needleaspiration cytology useful in the management of patients with benignnodular thyroid disease? Thyroid. 2000;10(6):489–92.
32. Flanagan MB, Ohori NP, Carty SE, Hunt JL. Repeat thyroid nodulefine-needle aspiration in patients with initial benign cytologic results.Am J Clin Pathol. 2006;125(5):698–702.
33. RenshawA. An estimate of risk of malignancy for a benign diagnosisin thyroid fine-needle aspirates. Cancer Cytopathol. 2010;118(4):190–5.